
Improved Organizational Design of the Diagnostic and Therapeutic
Process in Ovarian and Lung Cancer
Ewa Okoń-Horodyńska
1a
, Tomasz Sierotowicz
1b
and Agnieszka Sznyk
2
1
Jagiellonian University, Faculty of Management and Social Communication,
Institute of Economics, Finance and Management, Department of Economics and Innovation,
Prof. Lojasiewicza 4, 30-348, Krakow, Poland
2
Institute of Innovation and Responsible Development, INNOWO, Warsaw, Poland
Keywords: Health Care and Well-being, Improvement of Diagnostic Process, Modeling and Simulation of Diagnostic
Processes, Use ICT in Improved Diagnostic Process.
Abstract: A disease in each single patient can be one of a kind and an individual approach is needed. Tumors are in this
case particularly risky. The main research problem, as a case study, was to demonstrate the length and com-
position of the current Polish diagnostic process for two most risky conditions: ovarian carcinoma and lung
cancer, as well as to determine the causes for this. The main goal was to create a new, innovative model for
time-improved diagnostic processes of ovarian and lung cancer. In order to achieve aims of this research, the
BPMN and CPM were used. The main result of this study is a model of treatment processes in the indicated
cases with organizational changes, encompassing all possible types of contact between the patient and the
healthcare system. The entire diagnostic time for lung and ovarian cancer was shortened about 50%, which
significantly increases the chances of quick diagnosis and effective treatment. The newly designed and pre-
sented in the text model is an example of organizational innovation where implementation of ICT solutions,
allows to achieve and even improve an optimal path leading to the development of personalized medicine.
1 INTRODUCTION
A disease in each single patient can be one of a kind
and an individual approach is therefore needed. The
proper treatment is undertaken with considerable de-
lay. This delay can be divided into three types. The
first concerns delay in diagnosis caused by too late
first visit at the primary care physician (PCP) or in-
sufficient knowledge of the PCP to notice certain
symptoms. The second group of delay results from
lengthy and rigid workup procedures (overlapping
delay loop) and introduction of appropriate treatment
due to accurate decisions. Finally, the third type of
delay is associated with the reaction of the organism
to therapy. The economic dimension of these types of
delay and barriers in treatment cannot be left unno-
ticed. Damage to health caused by neoplasms renders
the vast human potential, mainly the professional one,
unexploited, and the costs of treatment and care over
patients leave a mark in economies, which might
a
https://orcid.org/0000-0002-2548-254X
b
https://orcid.org/0000-0002-1462-8267
threaten the future stability of public finances and
cause a decrease in Gross National Product (GNP),
not only in Poland. According to the Polish National
Cancer Registry (Didkowska et al., 2015), there were
156.5 thousand new cases of malignancies and 94
thousand deaths due to such diseases in 2013. The in-
cidence had increased by approximately 4 thousand.
Malignant tumors constitute the second cause of mor-
tality in Poland. In 2013, these diseases accounted for
26% of deaths among males and almost 23% among
females. Malignant tumors are the principal cause of
premature death (before the age of 65). This phenom-
enon is particularly evident in the female population:
33% of death in the group of young women and nearly
49% among middle-aged ones (Didkowska et al.,
2015). In Poland, lung cancer (ICD10: C34) accounts
for 1/3 of all deaths due to malignant cancers among
males and 15% among females. Ovarian carcinoma
(ICD10: C56), in turn, is a cause of 6.2% of all deaths
due to malignant cancers among Polish women. In
154
Oko
´
n-Horody
´
nska, E., Sierotowicz, T. and Sznyk, A.
Improved Organizational Design of the Diagnostic and Therapeutic Process in Ovarian and Lung Cancer.
DOI: 10.5220/0007950801540163
In Proceedings of the 16th International Joint Conference on e-Business and Telecommunications (ICETE 2019), pages 154-163
ISBN: 978-989-758-378-0
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

2000–2002, one-year survival rates reached 71.9%.
This value remained similar in 2003–2005 (70.8%) as
though global innovations could not reach Poland.
According to the EUROCARE-5 study (Eurocare,
2014), Poland, with 5-year survival among ovarian
cancer patients of 34.5%, falls below the European
value, i.e. 37.6%. Is this not the highest time for the
implementation of personalized model of treatment in
these cases? However, in order to do this properly and
effectively, it is necessary to first review the existing
process paths in the diagnosis and treatment of these
diseases. The critical point in the treatment of these
diseases is the moment of initiation of proper inpa-
tient treatment as well as selection and application of
individualized therapies. In order to perfect the entire
process, one must first improve the diagnostic process
because the moment of initiation and duration of
proper treatment depends upon the efficiency and ef-
ficacy of diagnosis. This paper, describes a design of
a processes, starting with the first contact up to the
conclusion of personalized therapy and a return to so-
cial and economic functioning. The process includes
the main scheme up to a detailed and complex hospi-
tal treatment. The main research problem was to
demonstrate the length and composition of the current
Polish diagnostic process for two most risky condi-
tions, i.e. ovarian carcinoma and lung cancer, as well
as to determine the causes for this. The results of this
application study are models of the treatment process
in the indicated cases with organizational changes,
encompassing all possible types of contact between
the patient and the healthcare system. These models
are a pilot undertaking that ought to be popularized if
the results described in the conclusions, which depict
an optimal development path for Polish personalized
medicine, are desired.
2 LITERATURE REVIEW
An optimal diagnostic process, i.e. a process which is
as short as possible and leads to establishing an accu-
rate diagnosis, is an important factor, not only for the
time of recovery and re-initiation of professional ac-
tivity, which lowers losses for the economy, but also
for the efficacy of subsequent treatment (Rivera et al.,
2013). Diagnosis, proper inpatient treatment and in-
dividualized post-hospital therapy are subprocesses
that comprise one diagnostic and therapeutic process
of a given disease, occurring in certain specified con-
ditions of the healthcare system in a given country.
The diversification of processes in terms of their du-
ration results from both the type of disease and its
stage of progression. That is why optimization must
be conducted for a given process that encompasses
the subprocesses of diagnosis and treatment proper
for a given disease. Diseases that pose the greatest
challenge in establishing a rapid diagnosis include
ovarian carcinoma and lung cancer. In these cases,
improvement of time needed to make a diagnosis
seems to be of fundamental significance due to the
fact that initial symptoms are not necessarily specific,
and the efficacy of the proper treatment strongly de-
pends on the time of its initiation (Havrileskya et al.,
2009). The issue of optimizing the diagnostic process
in ovarian and lung cancers is not new (Evans et al.,
2007; Collins et al., 2007). Good practice concerning
optimal organization of the diagnostic process in
terms of its duration and establishing an accurate di-
agnosis vary depending on a country. This results
from the diversity of healthcare systems. They can be
helpful in identifying the major barriers on the way to
proper diagnosis and treatment. Obviously, they can-
not eliminate all barriers and are not ready instru-
ments for optimal solutions in other healthcare sys-
tems (Evans et. al., 2007).
3 MATERIALS AND METHODS
In real environments, it is common to deal with pro-
cess characterized by incremental development, fol-
lowed by agile approaches and time improved meth-
ods such as Critical Path Method (CPM). For this rea-
son, the processes under research have to be consid-
ered to be continuous (Kunze et al., 2016). This iter-
ative approach to the process re-thinking along with
organizational change of both the structure and the
outcomes of a process is often referred to as process
re-engineering. In the presented solution, the process
will be change in order to time-improvement all steps
of diagnostic part of process. As a result, the treat-
ment can be start at earliest opportunity with using the
same medical assets.
3.1 Conceptual Framework and
Assumptions
Improvement of the diagnostic and therapeutic pro-
cess requires an individual approach to the process
that consists of various consecutive events. This study
is an attempt to identify and design organizational
changes aiming at shortening the duration of diagnos-
ing ovarian and lung cancers using existing material
and non-material resources, on the basis of the opti-
mization of current treatment processes of these dis-
eases. Therapy in ovarian and lung cancers consists
of three subprocesses: diagnosis, hospital treatment
Improved Organizational Design of the Diagnostic and Therapeutic Process in Ovarian and Lung Cancer
155

and individual post-hospital therapy. Since the main
aim of the study is to optimize the duration of the di-
agnostic subprocess, it was necessary to obtain de-
tailed data concerning this subprocess, which is a part
of the patient treatment process.
3.2 Data
In the Polish healthcare system, the therapeutic pro-
cess is different for each patient (which considerably
prolongs the diagnostic process and treatment proper)
instead of creating certain specific disease-and pa-
tient-based groups. Thus, data collected for the study
were collected from two sources: the Polish
healthcare system and patients participating in the
therapeutic process for ovarian and lung cancers.
These data allow to identify all possible events that
could occur depending on: the type of physician
whom patients consult initially, symptoms that are
identified and the number of specialists that can take
part in the diagnostic process. At the same time, the
minimum and maximum time periods associated with
awaiting individual actions were distinguished.
3.3 Methods
Management sciences currently have at their disposal
computer tools for process management. These make
use of standards enabling description of various pro-
cesses characterized by variable complexity (Ouyang
et al., 2008; Grosskopf et al., 2009). The application
of these tools is not limited to business processes
only. In particular, the Business Process Management
Notation (BPMN) standard can be used for descrip-
tion, simulation and optimization of diagnostic and
therapeutic processes (Allweyer, 2008; White, Bock,
2011). Process optimization and its associated modi-
fication not only allow to identify bottlenecks, but al-
lows the entire process to be accelerated, but also give
opportunities to obtain clues aiming at process recon-
figuration in accordance with the value-driven ap-
proach (Thomas et al., 2010; Bollen, 2016, Combi et
al., 2017). The application of this method entailed the
performance of the following actions in successive
sequences. 1. Based on the data obtained, three ther-
apeutic processes were modeled in the dedicated soft-
ware: for ovarian carcinoma treatment if the patient
initially consulted a PCP; for ovarian carcinoma treat-
ment if the patient initially consulted a gynecologist;
and for lung cancer treatment when the patient re-
ported to a PCP. The models consisted of all events
and time delays of their performance in the diagnostic
subprocess. The remaining subprocesses (treatment
proper and individualized post-hospital therapy) were
presented in the models in the global form, as envis-
aged by the standard adopted. 2. Each process was
then simulated in each possible variant according to
minimum and maximum time that lapse from the ini-
tial patient appointment up to the moment of referring
to hospital for treatment, which is equivalent to spec-
ifying a point for establishing a diagnosis. 3. The di-
agnostic subprocess was improved for each model of
the treatment process. 4. The model of improved di-
agnosis for all three treatment processes was designed
and verified. The obtained models of treatment pro-
cesses and results of conducted optimization served
for forming final conclusions and indicating the need
for further research.
4 RESULTS
Each of the models encompasses all possible types of
patient-healthcare system contact, organized in the
form of events in accordance with the BPMN stand-
ard in swimlane diagrams (Ryan, et al., 2009; White
et al., 2011; Scheuerlein et at., 2012, Combi et al.,
2017), starting with the initial visit up to the conclu-
sion of post-hospital individual treatment and a return
to effective professional activity. The following sub-
sections present individual models for three processes
dedicated to treatment of ovarian and lung cancers.
4.1 Model of Ovarian Cancer
Treatment Process – The First Visit
at a PCP Office
The first model (Figure 1) presents possible paths of
contact between an ovarian cancer patient and the
healthcare system assuming that her first visit in the
diagnostic subprocess took place in a PCP office.
Solid lines denote a typical course of events (connec-
tion between events). Dashed lines, however, show
the flow of information concerning test results. After
each medical consultation with any type of doctor, al-
ternative decisions that the doctor could make are pre-
sented. The remaining subprocesses, being a part of
the treatment process but not the subject of investiga-
tion, are marked and described as follows:
1. Treatment of other diseases – both the PCP and
any specialist (apart from geneticist) can diagnose
diseases other than ovarian cancer and initiate a
subprocess of treatment at any stage of the pro-
cess.
2. Inpatient treatment – each of the doctors partici-
pating in the diagnostic process (apart from
geneticist) can diagnose ovarian cancer based on
ICE-B 2019 - 16th International Conference on e-Business
156
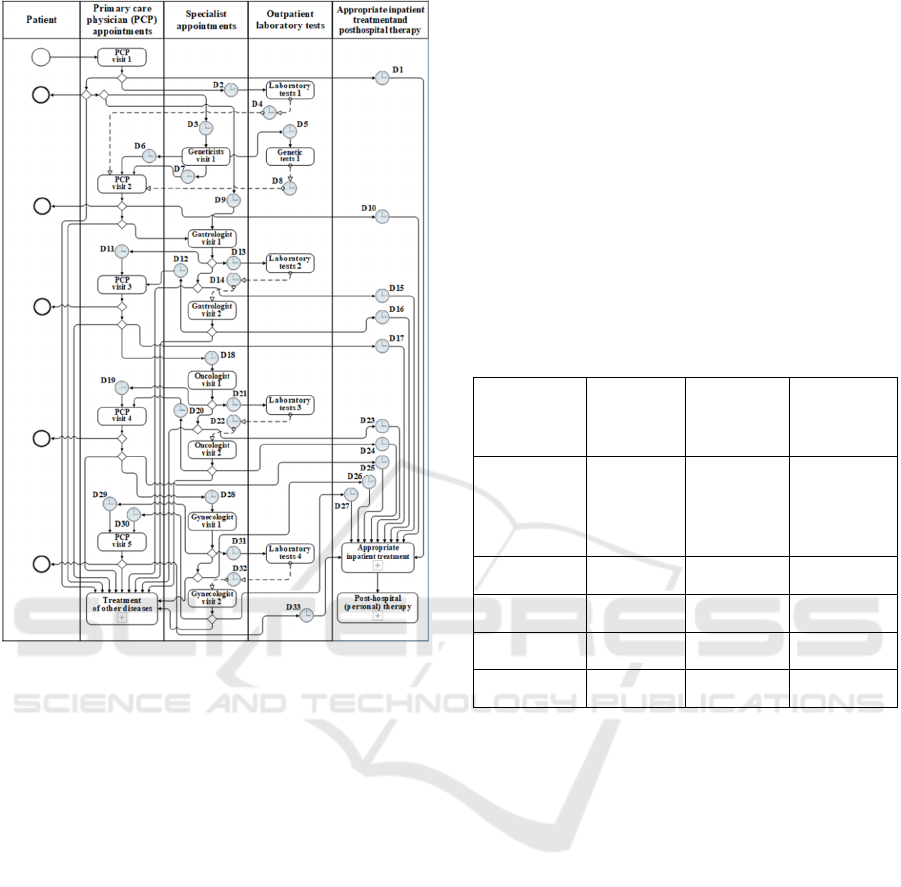
Figure 1: Model of ovarian cancer treatment process – the
first visit at a PCP office.
data achieved or obtained in examinations and refer
patients to hospital for proper inpatient treatment. 3.
Post-hospital personal therapy – it is a subprocess of
individual post-hospital treatment after the conclu-
sion of the inpatient ovarian cancer treatment. The in-
dividual stages of the diagnostic process involve time
delay, marked as D. As the model suggests, 33 maxi-
mum delays, which may negatively affect effective
treatment, were identified. The model contains the
maximum number of possible events in the diagnostic
subprocess. The stages of specialist consultations can
be repeated and their number depends on the number
of specialists engaged in the diagnostic process.
Events in the form of specialist appointments as con-
secutively referred by a PCP are therefore possible.
Moreover, each specialist can repeatedly refer the pa-
tient for specialist tests proper for that doctor’s spe-
cialty, according to their qualifications. This entails
multiple events in terms of laboratory testing. A re-
ferral for specialist examinations entails another spe-
cialist visit upon receipt of test results. If there are no
signs of a disease belonging to the field of expertise
of a given specialist, the patient is again referred to a
PCP who, in turn, refers her for further examinations
(in the case of issuing a referral to hospital, all exam-
inations are conducted there). The delay in this model
strictly depends on the events in the process and con-
cern the periods of awaiting: appointments with indi-
vidual physicians; performance of examinations; ob-
taining test results and admission to hospital. The
model (Figure 1) contains a description of actions
conducted by four specialists to whom the patient
may be referred by a PCP: geneticist, gastrologist, on-
cologist and gynecologist. Minimum and maximum
delay values, based on obtained data and simulations,
are presented in Table 1.
Table 1: Delay in waiting for doctor appointments- ovarian
cancer treatment - first visit at a PCP office.
Specialist
Wait time
for visit-
min (days)
Wait time
for visit-
max (days)
Delay time
PCP 1 7
D6, D7,
D11, D12,
D19, D20,
D29, D30
Gastrologist 90 120 D9
Geneticist 30 180 D3
Oncologist 14 90 D18
Gynecologist 2 14 D28
As indicated by the data and calculations presented in
Table 1, the shortest period of awaiting a visit con-
cerns a PCP – 1 day. The longest period of waiting
for an appointment with a specialist among the mini-
mum waiting periods concerns a gastrologist: 90
days. The longest possible time of awaiting consulta-
tion concerns a geneticist and may reach even 180
days. The shortest and the fastest treatment path in
terms of the number of events occurs when the patient
is referred to hospital during the first PCP appoint-
ment. Such situations are nearly non-existent in prac-
tice since this disease does not produce specific signs
in early stages. The longest treatment path involves
subsequent referrals to all specialists engaged in the
treatment process. If the patient is referred by a spe-
cialist for further examinations, the second appoint-
ment with this specialist is delayed at least by the time
of awaiting test results. Specialist examinations are
another source of delay. This concerns both the date
of their performance and awaiting results. Table 2
presents delay periods for each patient’s appointment.
Improved Organizational Design of the Diagnostic and Therapeutic Process in Ovarian and Lung Cancer
157
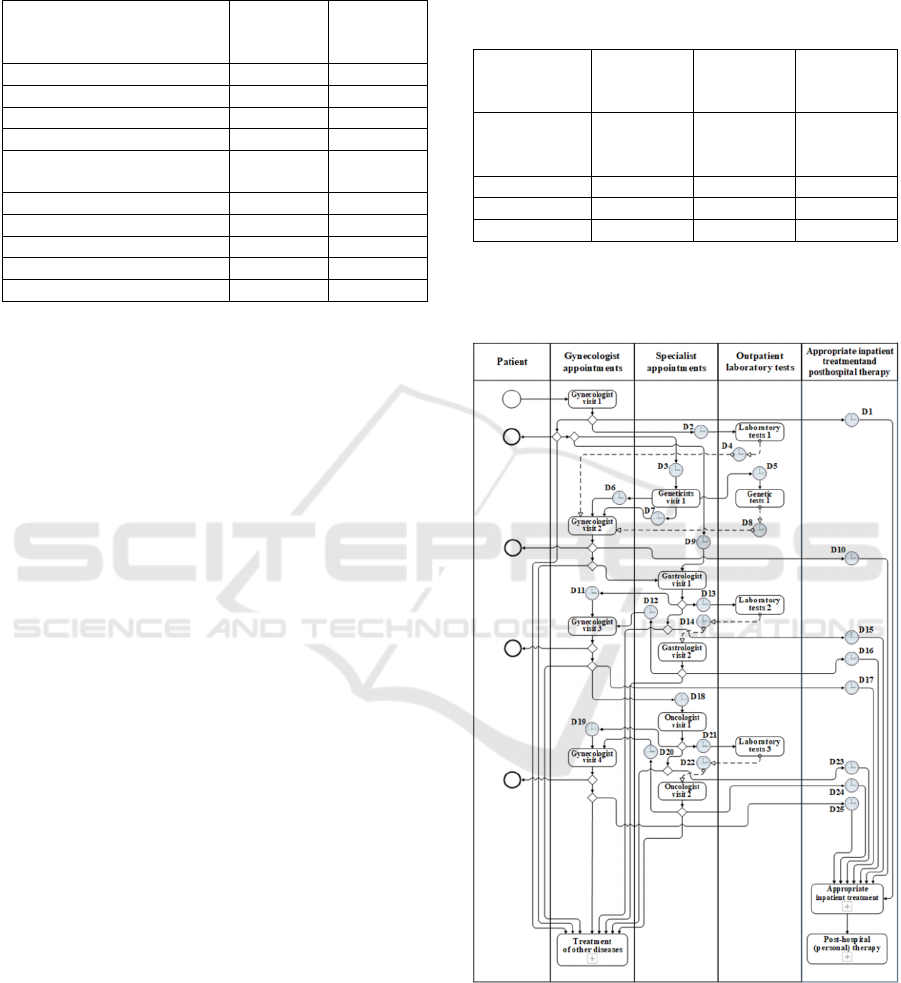
Table 2: Delay in awaiting tests and results in the model of
ovarian cancer diagnosis and treatment – the first visit at a
PCP office.
Referring physician appoint-
ment
Result –
min (days)
Result –
max
(days)
PCP or Gynecologist 1 2
Oncologist or Gynecologist 7 14
PCP or Gynecologist 14 28
PCP or Gynecologist 1 2
PCP or Gynecologist or On-
cologist
5 10
PCP or Gynecologist 1 7
Oncologist or Gynecologist 30 120
Oncologist or Gynecologist 30 180
Gastrologist or Oncologist 30 180
Geneticist 180 180
The delay time contains time delay points marked as
“D” included in the first model (Figure 1) for duration
of waiting for examinations and test results, respec-
tively. The duration of delays ends with the duration
of waiting for hospital admission. Since a referral to
hospital can be issued by any physician, this delay can
occur at various points during the diagnostic subpro-
cess. They are identified as: D1, D10, D15, D16, D17,
D23, D24, D25, D26, D27, D33. These delays will
certainly occur only once in the diagnostic process.
The time of awaiting hospital admission ranges from
1 to 14 days. Moreover, during each visit a PCP,
based on test results, may decide that: 1) there are no
signs of a severe disease that would require further
processes in the healthcare system; 2) there is a need
to initiate a different treatment subprocess; 3) there is
a need for hospital treatment.
4.2 Model of Ovarian Cancer
Treatment Process – The First Visit
at a Gynecologist Office
Figure 2 presents a model of ovarian cancer diagnos-
tic and therapeutic process when the patient first re-
ports to a gynecologist. The second model (Figure 2)
was drawn up based on the approach adopted in Fig-
ure 1. As the model suggests, if the patient reports
first to a gynecologist, the number of specialists to
whom she can be referred is lower. This also means
that the number of possible laboratory examinations
is lower, but the number of tests remains unchanged.
In the entire diagnostic subprocess, 25 delays were
noted. This number is lower by 8 compared with the
previous model. Table 3 presents delay in awaiting
doctor appointment in the model of ovarian cancer di-
agnosis and treatment when the first visit took place
at a gynecologist office. The longest period of waiting
for an appointment among the cases with the lowest
time periods concerns a gastrologist: 90 days.
Table 3: Delay in waiting for doctor appointments- ovarian
cancer treatment - the first visit at a gynecologist office.
Specialist
Wait time
for visit-
min (days)
Wait time
for visit-
max (days)
Delay time
Gynecologist 2 14
D6, D7,
D11, D12,
D19, D20
Gastrologist 90 120 D9
Geneticist 30 180 D3
Oncologist 14 90 D18
As indicated by the data and calculations presented in
Table 3, the shortest period of awaiting a visit con-
cerns a gynecologist: 2 days.
Figure 2: Model of ovarian cancer treatment process – the
first visit at a gynecologist office.
The longest possible time of awaiting consultation
concerns a geneticist and may reach even 180 days.
Compared with the model shown in Figure 1 (the first
visit – PCP), the range of delay did not change con-
siderably, but the entire diagnostic subprocess is
ICE-B 2019 - 16th International Conference on e-Business
158
shorter by one gynecological consultation, which
saves 2 to 180 days. This results from the possibility
of being referred for specialist examinations as soon
as during the very first visit (by a gynecologist). The
remaining delays in other segments of this process
still lower chances for effective treatment. The short-
est path in terms of the number of events and, at the
same time, the fastest treatment route takes place
when a gynecologist refers the patient to hospital at
the very first visit. Such situations are rare in practice
because symptoms of ovarian cancer would then in-
dicate advanced disease, the treatment of which is
poorly effective. The longest treatment path involves
subsequent referrals to all specialists engaged in the
treatment process. As in the previous model, if the pa-
tient is referred for further examinations by a special-
ist, the second appointment with this specialist is de-
layed at least by the time of awaiting test results. Spe-
cialist examinations are another source of delay. This
concerns both the date of their performance and
awaiting results. Table 4 presents delay periods for
each patient’s appointment. The delay time contains
time delay points marked as “D” included in the sec-
ond model (Figure 2) for duration of waiting for ex-
aminations and test results, respectively. The total de-
lay ends with the duration of waiting for hospital ad-
mission. Since a referral to hospital can be issued by
any physician, this delay can occur at various points
during the diagnostic subprocess. They are marked
as: D1, D10, D15, D16, D17, D23, D24, D25.
Table 4: Delay in awaiting tests and results in the model of
ovarian cancer diagnosis and treatment – the first visit at a
gynecologist office.
Referring physician appoint-
ment
Result-
min (days)
Result-
max
(days)
Gynecologist 1 2
Gynecologist or Oncologist 7 14
Gynecologist 14 28
Gynecologist 1 2
Gynecologist or Oncologist 5 10
Gynecologist 1 7
Gynecologist or Oncologist 30 120
Gynecologist or Oncologist 30 180
Gastrologist or Oncologist 30 180
Geneticist 180 180
These delays will certainly occur only once in the di-
agnostic process. As in the previous model, the time
of awaiting hospital admission ranges from 1 to 14
days. Moreover, during each visit a gynecologist,
based on test results, may decide that there are no
signs of a severe disease that would require further
processes in the healthcare system, there is a need to
initiate a different treatment subprocess or that there
is a need for hospital treatment.
4.3 Model of Lung Cancer Treatment
Process
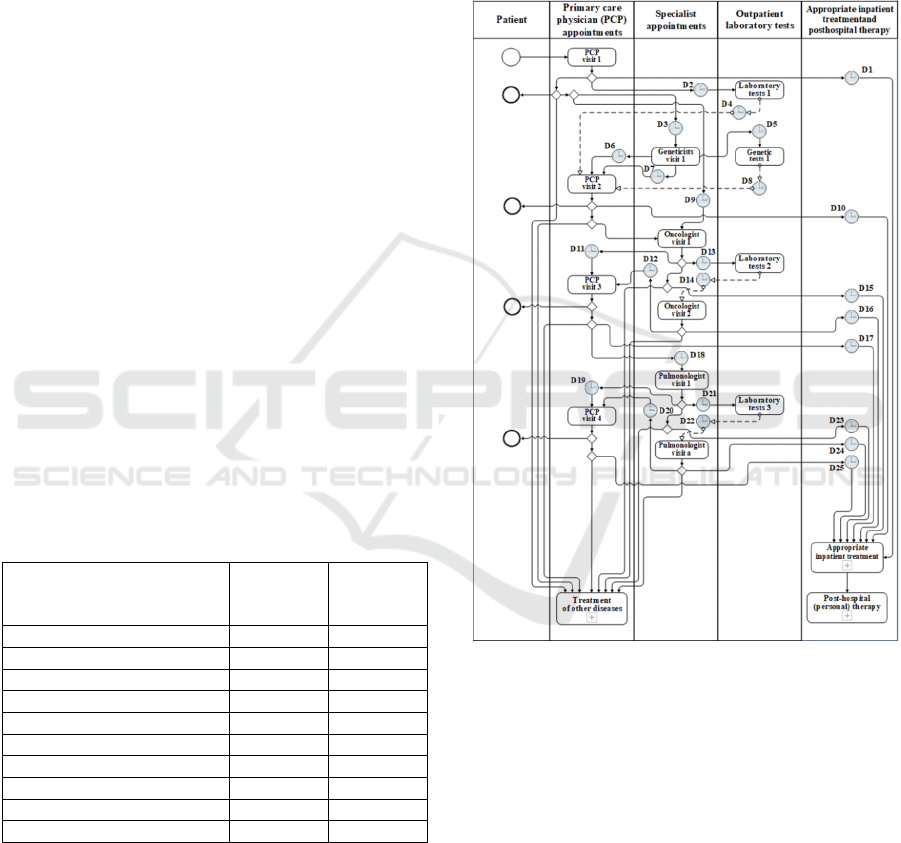
Figure 3 presents a model of lung cancer diagnostic
and therapeutic process. The third model (Figure 3) is
also based on Figure 1 (first visit at a PCP office).
Figure 3: Model of lung cancer diagnostic and therapeutic
process.
It is characterized by a lower number of specialists to
whom patients may be referred. This also means that
the number of possible laboratory examinations is
lower, but the number of tests remains unchanged. In
the entire diagnostic process, 25 delays were noted.
This number is lower by 8 compared with the previ-
ous model (Figure 1). Table 5 presents delay in await-
ing doctor appointment in the model of lung cancer
diagnosis and treatment. As indicated by the data and
calculations presented in Table 5, the shortest period
of awaiting a visit concerns a PCP: 1 day. The shortest
and the fastest treatment path in terms of the number
Improved Organizational Design of the Diagnostic and Therapeutic Process in Ovarian and Lung Cancer
159
of events occurs when the patient is referred to hospi-
tal during the first PCP appointment. Such situations
are rare in practice because first symptoms of lung
cancer are non-specific and require additional, some-
times numerous, examinations.
Table 5: Delay in awaiting doctor appointment in the model
of lung cancer diagnosis and treatment.
Specialist
Wait time
for visit-
min (days)
Wait time
for visit-
max (days)
Delay time
PCP 1 7
D6, D7,
D11, D12,
D19, D20
Geneticist 30 180 D3
Oncologist 14 90 D9
Pulmonologist 14 120 D18
The longest period of waiting for an appointment
among the events with the shortest time periods con-
cerns a geneticist: 30 days. The longest possible time
of awaiting consultation also concerns a geneticist
and may reach even 180 days. The longest treatment
path involves subsequent referrals to all specialists
engaged in the treatment process. As in the previous
models, if the patient is referred for further examina-
tions by a specialist, the second appointment with this
specialist is delayed at least by the time of awaiting
test results. Specialist examinations are another
source of delays. This concerns both the date of their
performance and awaiting results. Table 6 presents
types of examinations and delay periods that they en-
tail.
Table 6: Delay in awaiting tests and results in the model of
lung cancer diagnosis and treatment.
Referring physician appoint-
ment
Result –
min
(days)
Result –
max
(days)
PCP 1 2
PCP 14 28
PCP or Oncologist 1 7
PCP or Oncologist or Pul-
monologist
30 120
Oncologist or Pulmonologist 1 7
Oncologist or Pulmonologist 31 62
Pulmonologist 30 180
Pulmonologist 7 14
Geneticist 180 180
The delay time contains time delay points marked as
“D” included in the second model (Figure 3) for du-
ration of waiting for the examination and test results,
respectively. The delay ends with the duration of
waiting for hospital admission. They are marked as:
D1, D10, D15, D16, D17, D23, D24, D25. The time
of awaiting hospital admission occurs only once and
ranges from 1 to 14 days. During each visit, a PCP,
based on test results, may decide that there is a need
to initiate a different treatment subprocess or that
there is a need for hospital treatment. The PCP can
also diagnose a minor disease or prescribe certain
medications, after which the patient leaves the
healthcare system.
4.4 Improved Model of Ovarian and
Lung Cancer Treatment
The model simulations yielded results presented in
Table 7. It was assumed that all necessary examina-
tions will be conducted in an optimal way, i.e. without
extending the waiting period associated with their
performance and receiving results. That is why the
delay ranges from 1 to 180 days in each of the ana-
lyzed models. Also, delay associated with the initial
PCP or gynecological visit are not taken into consid-
eration in the simulation since, in this case, the patient
makes decisions irrespective of the system in which
treatment is conducted. As simulations suggest (Table
7), the longest delay is generated by repeatable loops
of appointments with specialists. A question arises:
Can the duration of the diagnostic process in ovarian
and lung cancer be shortened significantly using the
present resources of the healthcare system? The sim-
ulations indicate that two organizational changes may
be performed: 1. Broadening the scope of PCP quali-
fications in terms of referring patients for specialist
examinations, involving oncological, gynecologic
and gastrological tests. 2. Organizing online medical
conferences with specialists that would have access to
all data that a PCP has obtained from the patient and
to results of tests from within their fields of expertise.
Following such a conference, a PCP can inform the
patient about the results of the conference and refer
them to hospital for treatment even during the second
visit. These two organizational changes served for de-
signing an improved model of ovarian and lung can-
cer treatment (Figure 4). First of all, the scope of PCP
and gynecologist qualifications must be broadened so
that patients could be referred for examinations dur-
ing the first appointments. The range of tests should
include the most significant tests conducted by an on-
cologist, gastrologist, geneticist and pulmonologist.
The PCP should have the power to refer patients for
gynecological examinations if symptoms suggest
ovarian cancer. When all tests have been conducted
in accordance with the initial diagnosis of ovarian or
lung cancer it is necessary to organize an online med-
ical conference without the need for the patient pres-
ence. Physicians that must take part in the conference
ICE-B 2019 - 16th International Conference on e-Business
160
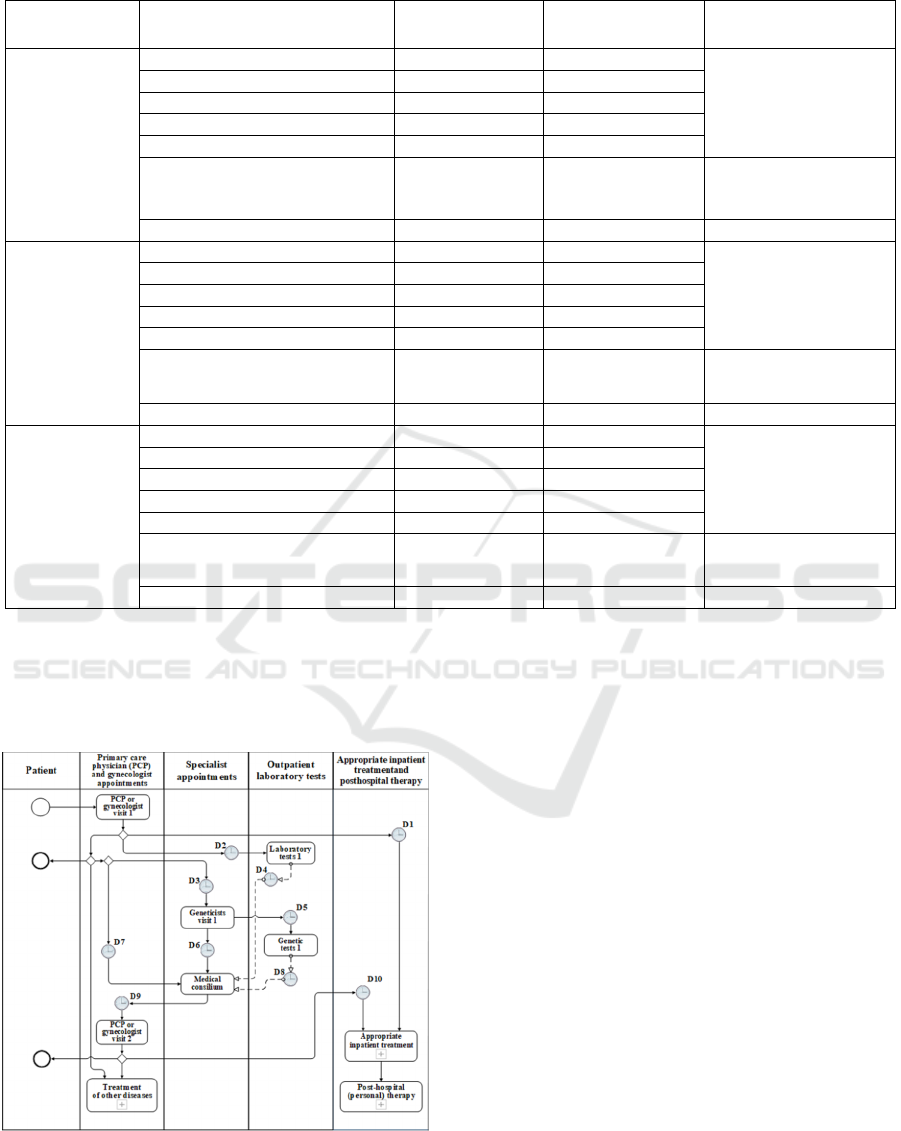
Table 7: Simulations of ovarian and lung cancer treatment model.
Model Event
Wait time for
visit- min (days)
Wait time for visit -
max (days)
Designation
Model of ovar-
ian cancer treat-
ment process –
the first visit at
a PCP office
4 PCP visits 4 28
Delay concerning visits
is presented in Table 1
1
st
visits to 4 specialists 136 404
2
n
d
visits to 4 specialists 136 404
Admission to hospital 1 14
Total 277 940
Perform and obtain test results 1 180
Delay concerning tests
is presented in Table 2
Total visits and examinations 278 1120
N/A
Model of ovar-
ian cancer treat-
ment process –
the first visit at
a gynecologist
office
4 visits to the gynecologist 8 72
Delay concerning visits
is presented in Table 3
1
st
visits to 3 specialists 134 390
2
n
d
visits to 3 specialists 134 390
Admission to hospital 1 14
Total 267 866
Perform and obtain test results 1 180
Delay concerning tests
is presented in Table 4
Total visits and examinations 268 1046
N/A
Model of lung
cancer treat-
ment process –
the first visit al-
ways takes
place at a PCP
office
4 PCP visits 4 28
Delay concerning visits
is presented in Table 5
1
st
visits to 3 specialists 58 390
2
n
d
visits to 3 specialists 58 390
Admission to hospital 1 14
Total 121 822
Perform and obtain test results 1 180
Delay concerning tests
is presented in Table 6
Total visits and examinations 122 1002
N/A
include: a PCP, oncologist and, depending on the sus-
pected disease: gynecologist and gastrologist for
ovarian cancer, or pulmonologist and thoracic sur-
geon for lung cancer
Figure 4: Improved model of ovarian and lung cancer diag-
nostic and therapeutic process.
Doctors taking part in such an online medical confer-
ence have access to all data collected by the PCP dur-
ing the first visit and to all test results. The conference
can be organized using standard and generally avail-
able tools for a video conference. Eventually, such
conferences will be held regularly as the work on
computerization of the health system progresses will
continue with application of appropriate security
measures. Doctors can make the following decisions:
1. The patient is healthy; 2. Admission to hospital; 3.
Depending on the diagnosis, initiation of treatment
for diseases other than ovarian or lung cancer. The
application of the proposed solution to the treatment
process of lung and ovarian cancer will reduce the
time of awaiting appointments with specialists. The
simulations of the optimal model of ovarian and lung
cancer diagnostic and therapeutic process yielded re-
sults presented in Table 8. For the simulation condi-
tions to be identical to those in the previous models,
it was assumed that all necessary examinations will
be conducted in the optimal way, i.e. without extend-
ing the waiting period associated with their perfor-
mance and receiving results. That is why the delay
ranges from 1 to 180 days in each of the analyzed
models. Delay associated with the initial PCP visit are
Improved Organizational Design of the Diagnostic and Therapeutic Process in Ovarian and Lung Cancer
161
Table 8: Results of simulations of the optimal model of ovarian and lung cancer diagnosis and treatment.
Disease Event
Wait time for
visit-min (days)
Wait time for visit-
max (days)
Designation
Improved model of
ovarian cancer treat-
ment process – the
first visit at a PCP
office
One PCP visit 1 7 D9
One visit with a geneticist 30 180 D3
Medical conference 106 224 D6, D7
Admission to hospital 1 14 D1, D10
Total 138 425
N/A
Perform and receive test results 1 180
D2, D4, D5,
D8
Total visits and examinations 139 605
N/A
Improved model of
ovarian cancer treat-
ment process – the
first visit at a gyne-
cologist office
One visit to a gynecologist 2 14 D9
One visit to a geneticist 30 180 D3
Medical conference 104 210 D6, D7
Admission to hospital 1 14 D1, D10
Total 137 404
N/A
Perform and receive test results 1 180
D2, D4, D5,
D8
Total visits and examinations 138 584
N/A
Improved model of
lung cancer treatment
process – the first
visit always takes
place at a PCP office
One PCA visit 1 7 D9
One visit to a geneticist 30 180 D3
Medical conference 28 210 D6, D7
Admission to hospital 1 14 D1, D10
Total 60 411
N/A
Perform and receive test results 1 180
D2, D4, D5,
D8
Total visits and examinations 61 591
N/A
not taken into consideration in the simulation since,
in this case, the patient makes decisions irrespective
of the system in which treatment is conducted. When
conducting the simulation, all data concerning delay
calculated in all models for doctor appointments, per-
formance of examinations and obtaining test results
as well as admission to hospital were used.
5 DISCUSSION AND
CONCLUSIONS
The work presented in this paper demonstrates that
organizational changes could reduce the number of
delays in the diagnostic and therapeutic process of
ovarian and lung cancer from 33 and 25, respectively,
to 10 in both cases with using the same number of
specialists and other medical staff. Moreover, it al-
lowed the application of one standardized diagnostic
subprocess where the difference between diseases
only involves different sets of specialist examinations
and a different team of physicians taking part in the
medical conference. Upon the introduction of
changes, the improved model preserves the shortest
possible diagnostic path by the possibility of issuing
a referral to hospital even during the first visit. The
simulation of the improved model for ovarian cancer
diagnosis and treatment with the first visit at a PCP
office indicates that the minimum time was reduced
from 278 to 139 days, and the longest possible time
of staying within the healthcare system – from 1120
to 605 days. This means reductions in the time from
the first PCP visit to hospital admission by 50% and
46%, respectively. In the case of the first patient visit
at a gynecologist office, the minimum time was re-
duced from 268 to 138 days, and the maximum time
– from 1046 to 584 days. This means reductions in
the time from the first appointment with a gynecol-
ogist to hospital admission by 48.5% and 44.17%, re-
spectively. As for the simulation of the optimal model
for lung cancer diagnosis and treatment, the minimum
time was reduced from 122 to 61 days, and the longest
possible time – from 1002 to 591 days. This means
reductions in the time from the first PCP visit to hos-
pital admission by 50% and 41%, respectively. Con-
sidering the results reported above, it can be stated
that introducing organizational changes (for now
without making investments in the fixed assets and
equipment), in the form of broadening the scope of
PCP and gynecologist qualifications in terms of issu-
ing referrals for specialist examinations as well as or-
ICE-B 2019 - 16th International Conference on e-Business
162

ganizing regular medical conferences online depend-
ing on the type of symptoms and initial PCP diagno-
sis, helps save approximately 50% of time in the sub-
process of ovarian and lung cancer diagnosis. These
results enable earlier decisions about referring pa-
tients for proper personalized treatment. Organizing
online medical conferences without the need for the
patient presence will reduce lines to specialists since
in many cases, decisions will be made during the con-
ference. Reductions in the time that would otherwise
be devoted to awaiting appointments with specialists
is another long-term effect of the aforementioned or-
ganizational innovation. Essential investments must
be made within the Information and Communication
Technologies (ICT) (rapid communication, online
conferences). It is an example of how the ICT can be
used in the process of diagnostic and treatment in or-
der to reduce time for diagnostic and start personal-
ized therapy as soon as possible. Without additional
investments in specialists and medical staff, a sub-
stantial time-optimization of process brings about
50% of diagnostic time reduction.
6 FUTURE RESEARCH
The subsequent stage of improvement management
should involve the performance of preliminary re-
search and making a selection of facilities that per-
form specialist laboratory tests in order to shorten
procedures and examinations, as well as reduce the
time of waiting for test results (they should be avail-
able instantaneously). Another challenge for the pre-
sent healthcare system is the introduction of an inte-
grated database in which patient data and their entire
medical histories could be stored. The issues pre-
sented above should constitute new research and im-
plementation projects that need to be undertaken as
soon as possible.
REFERENCES
Allweyer, T., 2008. Business Process Modeling Notation-
Einführung in den Standard für die Geschäftsprozess-
modellierung. Books on Demand GmbH. Norderstedt.
Bollen, P., 2016. Business Process Model Semantics in
BPMN. Springer-Verlag. Berlin.
Collins, L., Haines, Ch., Perkel, R., Enck, R., 2007. Lung
Cancer: Diagnosis and Management. American Family
Physician. 75(1), 56-63.
Combi, C., Oliboni, B., Zardini, A., Zerbato, F., 2017. A
Methodological Framework for the Integrated Design
of Decision-Intensive Care Pathways – an Application
to the Management of COPD Patients. Journal of
Healthcare Informatics Research. 12(1), 157-217.
Didkowska, J, Wojciechowska, U., 2015. Nowotwory
złośliwe w Polsce w 2013 roku. Zakład Epidemiologii
KRN. Warszawa.
Evans, J., Ziebland, S., McPherson, A., 2007. Minimizing
delays in ovarian cancer diagnosis: an expansion of An-
dersen’s model of “total patient delay”. Family Prac-
tice. 24(2), 48-55.
Grosskopf, A, Decker, G, Weske, M., 2009. The Process:
Business Process Modeling using BPMN. Meghan
Kiffer Press. New York.
Havrileskya, L., Broadwatere, G., Davisa, D., Noltea, K.,
Barnetta, J., Myersb, E., Kulasingamb, S., 2009. Deter-
mination of quality of life-related utilities for health
states relevant to ovarian cancer diagnosis and treat-
ment. Gynecologic Oncology. 113(2), 216-220.
Kunze, M, Weske, M., 2016. Behavioural Models: From
modelling finite automata to analyzing business pro-
cesses. Springer-Verlag. Berlin.
Ouyang, C., Dumas, M., Ter Hofstede, H., Van Der Aalst,
M., 2008. Pattern-based translation of BPMN process
models to BPEL web services. International Journal of
Web Services Research. 5: 42-61.
Rivera, M., Mehta, A., Wahidi, M., 2013. Establishing the
Diagnosis of Lung Cancer: Diagnosis and Management
of Lung Cancer. American College of Chest Physicians
Evidence-Based Clinical Practice Guidelines. 143(5),
10-40.
Ryan K. L., Lee, S., Lee, W., 2009. Business process man-
agement (BPM) standards: a survey. Business Process
Management Journal. 15(5), 744-791.
Scheuerlein, H., Rauchfuss, F., Dittmar, Y., Molle, R., Leh-
mann, T., Pienkos, N., Settmacher, U., 2012. New
methods for clinical pathways—Business Process Mod-
eling Notation (BPMN) and Tangible Business Process
Modeling BPM. Langenbeck's Archives of Surgery.
397(5), 755-761.
Steward, R. W., Wild, C. P., 2015. WHO, World Cancer
Report 2014. International Agency for Research on
Cancer Publishers. London.
The EUROCARE-5 Working Group-5., 2014. Cancer sur-
vival in Europe 1999–2007 by country and age: results
of EUROCARE-5 – a population-based study. The Lan-
cet Oncology. 15(1), 23-34.
Thomas, O., Vom Brocke, J., 2010. A value-driven ap-
proach to the design of service-oriented information
systems - making use of conceptual models. Infor-
mation Systems and e-Business Management. 8(1), 67-
97.
White, SA, Bock, C., 2011. BPMN 2.0 Handbook Second
Edition: Methods, Concepts, Case Studies and Stand-
ards in Business Process Management Notation. Future
Strategies Inc. New York.
Improved Organizational Design of the Diagnostic and Therapeutic Process in Ovarian and Lung Cancer
163
