
A Systematic Review on the Use of Educational Technologies for Medical
Education
Dalmaris Lima
1
, Victor Sotero
1
, Diego Dermeval
1,2 a
, Jorge Artur
1,2
and Francisco Passos
2
1
Center of Excellence for Social Technologies (NEES), Computing Institute, Federal University of Alagoas (UFAL),
Av. Lourival Melo Mota, S/N, Tabuleiro do Martins, Macei
´
o-AL, Brazil
2
Faculty of Medicine, Federal University of Alagoas (UFAL), Av. Lourival Melo Mota, S/N,
francisco passos01@hotmail.com
Keywords:
Educational Technologies, Medical Education, Computers and Medical Education.
Abstract:
Educational technologies have been increasingly used in medical education to promote innovative pedagogical
strategies in classroom. However, the medical scientific community still lacks a comprehensive understanding
on how educational technologies are used in medical education. The objective of this work is to explore
what types of technologies are employed in medical education, aiming to identify in which domains they
have been applied and the reported evidence of using educational technologies in medical education. We
conducted a Systematic Literature Review (SLR) to identify the primary studies on the use of educational
technologies in medical education, following a pre-defined review protocol. One hundred sixty-eight papers
were selected, covering nine types of education technologies, which were applied in more than 40 medical
domains. Moreover, our SLR results also show that most of the papers included in this SLR reported positive
evidence about the benefits of using these technologies in medical domain.
1 INTRODUCTION
The evolution of medical education has been taking
place rapidly. Students enter in the medical school
with a high level of technological skills and high ex-
pectation regarding innovative ways of learning. As
such, many researchers and medical schools have
been investigating how to apply new educational tech-
nologies in medical education. These technologies
may be, for instance, adaptive platforms, educational
games, gamification, mobile learning applications,
simulated virtual patients, and so on (Jabbar et al.,
2016; Ellaway and Masters, 2008) . Despite the ex-
istence of many works which rely on the use of ed-
ucational technologies in medical education, it is not
known to what extent there is evidence to state that
the use of educational technologies, indeed, benefits
medical education. Moreover, it is also important to
understand: i) what are the main types of educational
technologies that have been used in medical educa-
tion; and ii) on which medical domains these tech-
nologies have been applied.
There are some works that investigated the appli-
a
https://orcid.org/0000-0002-8415-6955
cation of educational technologies in health education
(Kalaian and Kasim, 2017) and, specifically, its us-
age in medical education (Ellaway and Masters, 2008;
Taveira-Gomes et al., 2016). However, these stud-
ies did not capture all the aspects and evidences that
we are interested. We are interested in finding how
promising educational technologies (e.g., ITS, CSCL,
mobile learning, gamification, and so on) have been
used in medical education.
In this article, we used the Systematic Review of
Literature (SLR) method (Kitchenham and Charters,
2007) to identify, evaluate, interpret, and synthesize
available studies to address specific research ques-
tions on the use and effectiveness of educational tech-
nologies in medical education settings and to estab-
lish evidence status with in-depth analysis. Thus, the
objective of this systematic review is to better under-
stand how these educational technologies are being
developed, applied and evaluated, as well as to iden-
tify in what way these technologies have been applied
to medical education. This paper presents the results
of a SLR on studies published from 1986 to Septem-
ber 2017 and was conducted following a pre-defined
review protocol, as will be further explained. The re-
mainder of this paper is organized as follows. Section
Lima, D., Sotero, V., Dermeval, D., Artur, J. and Passos, F.
A Systematic Review on the Use of Educational Technologies for Medical Education.
DOI: 10.5220/0007678501530160
In Proceedings of the 11th International Conference on Computer Supported Education (CSEDU 2019), pages 153-160
ISBN: 978-989-758-367-4
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
153

2 describes the SLR method used in this review. Sec-
tion 3 presents the results of the quality assessment
and an overview the papers. Then, it reports the find-
ings of the review along with an analysis and discus-
sion for each research question. Finally, Section V
presents conclusions, limitations and future works.
2 METHOD
A Systematic Literature Review (SLR) is a means of
identifying, evaluating and interpreting the available
research findings related to a research question, topic
area, or phenomenon. The main purpose of conduct-
ing a systematic review is to gather evidence on which
to base conclusion (Kitchenham and Charters, 2007).
Our SLR was structured based on the guide-
lines for conducting systematic reviews proposed by
(Kitchenham and Charters, 2007). The SLR was di-
vided into three main processes: SLR planning, con-
ducting the SLR, and reporting the SLR. Following
the steps: i) identification of the need for a system-
atic review; ii) formulation of a focused review ques-
tion; iii) a comprehensive and thorough search of pri-
mary studies; iv) evaluation of the quality of included
studies; v) identification of the data needed to answer
the research question; vi) extraction of data; vii) sum-
mary and summary of study results; viii) interpreta-
tion of results to determine their applicability; and ix)
reporting.
2.1 Research Question
The main objective of this SLR is to identify and
map the existing studies in the literature that use ed-
ucational technologies to promote medical education.
Based on this main objective, specific questions were
raised to identify the existing works in the area. The
questions along with their respective descriptions and
motivations are described below.
RQ1: What types of educational technologies
have been used in medical education? This question
aims to identify the main types of educational tech-
nologies (e.g., intelligent tutoring systems, computer-
supported collaborative learning, learning manage-
ment systems, and so on) used to support medical ed-
ucation;
RQ2: Which medical education domains have
been supported by educational technologies? This
question aims to identify the main domains, in the
medical field, that make use of the technologies
for educational support. It is important support re-
searchers in future developments of educational tools
to aid medical education;
RQ3: Are there evidences to state that using ed-
ucational technologies benefits medical education?
This question intends to analyze if such studies pro-
vide some evidence that the use of educational tech-
nologies benefits medical education considering its
domains. Evidence should consider positive and neg-
ative results including empirical and non-empirical
evaluation. They are important since they form a
knowledge base about the use of educational tech-
nologies for medical education.
2.2 Inclusion and Exclusion Criteria
The definition of the inclusion and exclusion crite-
ria is directly linked to the research objective. We
defined the following inclusion criteria based on our
research questions: (i) primary studies; (ii) peer-
reviewed studies, and (iii) studies evaluating or using
educational technologies in medical education. The
exclusion criteria of this review are: (i) duplicated pa-
pers; (ii) gray literature; (iii) non-English papers; (iv)
non-peer-reviewed studies; (v) position papers; (vi)
redundant article authored by the same researcher;
(vii) secondary studies; and (viii) short papers. We
also excluded (ix) papers that use educational tech-
nologies for other health areas (e.g.,nursing, physio-
therapy) and papers that received a score less than
50% of quality after conducting the quality assess-
ment step of the review, as further explained in Sec-
tion 2.4. Note that a primary study is a paper that
presents any new contribution to a field (Kitchenham
and Charters, 2007) and secondary studies are review
papers, such as systematic reviews, meta-analysis or
surveys.
2.3 Source Selection and Search
The search was performed only in electronic
databases, the following electronic databases were
searched: ACM Digital, EI Compendex, IEEE Digital
Library, ISI Web of Science, Lilacs, PubMed, Science
@ Direct, Scopus and Springer Link. The systematic
review process is described in Figure 1 as well as the
number of studies analyzed per step.
In step 1, the studies were obtained from the elec-
tronic databases using the following string: ((”Med-
ical education” OR ”medical teaching” OR ”med-
ical school”) AND (”authoring tool” OR ”author-
ing system” OR ”intelligent authoring” OR ”learning
management system” OR ”m-learning” OR ”mobile
learning” OR ”collaborative learning” OR ”computer
supported collaborative learning” OR ”intelligent tu-
toring system” OR ”intelligent educational systems”
OR ”massive open on line courses” OR ”adaptive ed-
CSEDU 2019 - 11th International Conference on Computer Supported Education
154
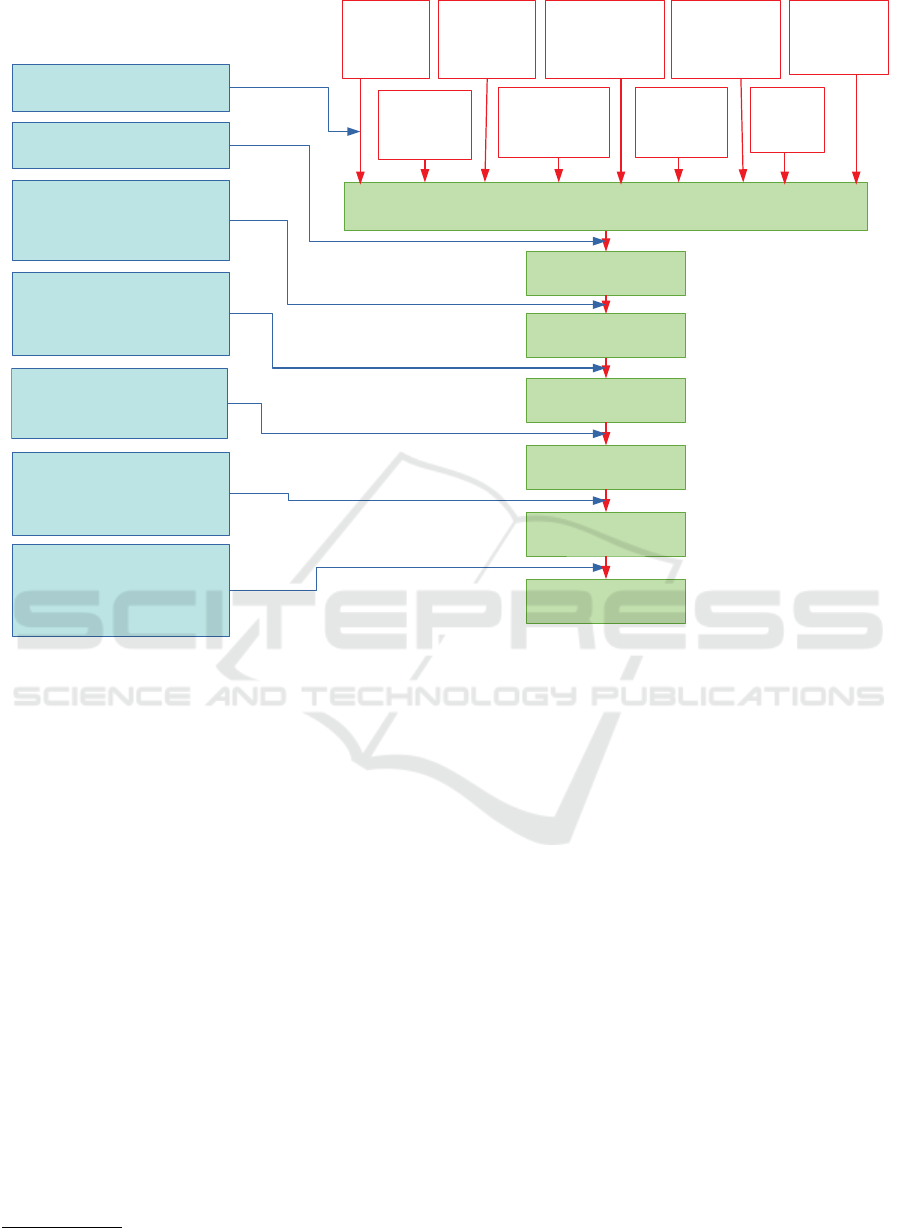
Step 1: Identify and organize studies
retrieved from the electronic base.
Step 2: automatic removal of
duplicated papers using Parsifal tool
Step 3: reviewers reviewed the
titles, keywords, and publication
local and excluded those that did
not attend the inclusion criteria. If
there was insufficient data, the
a paper was left for the next step.
Step 4: reviewers analyzed the
the paper’s abstracts and excluded
those which did not attend the
inclusion criteria. If there was
insufficient data, the paper was left
for next step
Step 5: the complete text from the
papers selected at step 4 were
retrieved and reviewed and those
that attended the inclusion criteria
were selected
Step 6: Revised studies that aimed
to assess the use of technology in
healthcare education,
in general, were rejected,
the other studies met the
inclusion criteria for the next step.
Step 7: the studies reviewed with
Scores in the evaluation of quality
of less than 4.5, or less than 50% of
total quality assessment scores were
excluded, as well as closing the
studies selection stage
ACM Digital:
18 titles
EI Compendex:
145 titles
PubMed:
881 titles
ISI Web Science:
266 titles
Scopus:
578 titles
Springer Link:
999 titles
Science@Direct:
1129 titles
IEEE Digital Libary:
79 titles
Lilacs:
5 titles
4,100
titles
281
titles
291
titles
1,168
titles
2,153
titles
3,159
titles
168
titles
Figure 1: Research questions and motivations.
ucational systems” OR ”adaptive learning systems”
OR ”artificial intelligence in education” OR ”gamifi-
cation”)).
The results for the string search (4100 papers)
were automatically downloaded and organized with
the help of the Parsifal tool
1
. In Figure 1 we describe
the selection stages, as well as the number of studies
in each stage. In the end the selection process, 168
papers remained and were included in the review.
2.4 Quality Assessment
The quality assessment (QA) of the selected studies
was based on a scoring technique to evaluate the cred-
ibility, integrity, and relevance of the selected papers.
All the papers were submitted to a set of 9 quality
criteria. Nine questions are adapted to quality assess-
ments of studies in the literature. Table 1 presents the
evaluation tool. All quality criteria were taken from
the literature. The main basis for structuring the qual-
ity assessment questionnaire was the Systematic Re-
view of the Literature conducted by (Dermeval et al.,
1
http://parsif.al
2017).
We used a technique of score between 3 possible
answers, Yes = 1,0, No = 0,0 and Maybe = 0,5. In
questions Q6 and Q9, it would be possible only a di-
rect answer (Yes / No), where Q6 was asked if the
study was evaluated with some empirical method, al-
ready in Q9 is questioned if the study can be put in
an industrial environment. In question Q5 brings the
question of whether these tools would be available for
download on the web, being scored with 1.0 if the tool
is present and it is available for download on the web,
0.5 if only the tool is presented, but it’s unavailable for
download and has received score 0,0 those who did
not present any type of tool. In the other questions,
this line follows, taking into account the requirement
of the question totally received 1.0, partially attend-
ing 0.5 and not meeting the requirements of question
received 0.0.
Note that, in the selection steps, authors evaluated
the studies separately to discuss disagreement regard-
ing classification. Studies were organized in a spread-
sheet, separated per retrieved papers over electronic
databases. After this analysis, there was a cross-
referencing of the data and a discussion of the diver-
A Systematic Review on the Use of Educational Technologies for Medical Education
155
gences between the evaluations, reaching agreement
on the issues.
2.5 Data Extraction and Synthesis
The data extraction was performed through the read-
ing of the 168 articles selected in the previous steps.
During this stage, the data was extracted by complet-
ing the extraction form (Table 2). All search, selec-
tion, and extraction were done with the aid of the Par-
sifal tool.
3 RESULTS AND ANALYSIS
A total of 168 papers met the inclusion criteria and
their data were extracted. Prior to presenting the re-
sults and analysis for each research question, we re-
view the quality assessment results and give a short
overview of the general characteristics of the studies.
The quality assessment on the selected papers is
useful to increase the accuracy of the data extraction
results. This evaluation helped to determine the va-
lidity of the inferences conducted and in ascertaining
the credibility and coherent of the synthesis of results.
For the sake of space, the quality assessment results
as well as the list of the 168 papers included in this
review are available at Google drive
2
:
The scores of all papers are no less than 50% and
the average score is 74,46%. We chose the minimum
of 50% quality with the aim to establish an accept-
able quality threshold for the articles. Taken together,
these 9 criteria provided a measure of the extent to
which we could be confident that a particular study’s
findings could make a valuable contribution to this re-
view.
3.1 Overview of the Studies
In the following sections, we depict in detail publica-
tions years, local and type of paper, research methods,
and application context information.
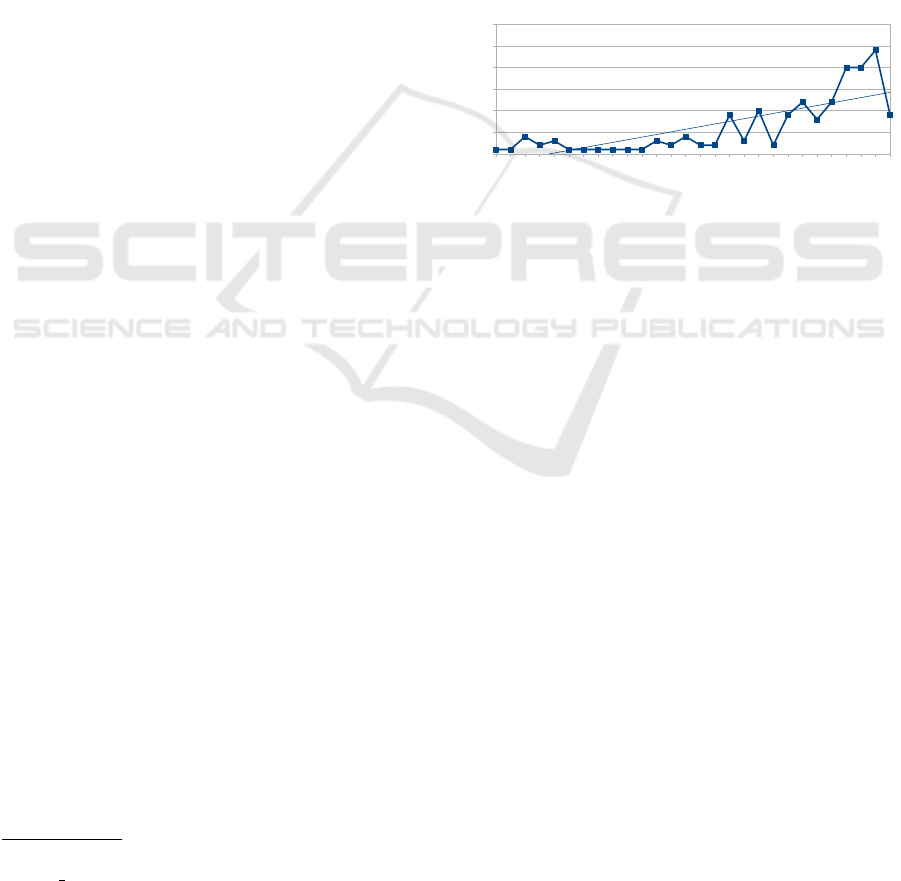
3.1.1 Publication Year
The reviewed papers were published between 1986
and 2017. From a temporal point of view (Figure 2),
an increasing number of publications in the context of
this review is observed since 2006. 2016 (24;14.12%)
is the year with most publications, followed by 2014
and 2015 (each with 20 papers;11.76%), 2011 (12;
2
https://drive.google.com/file/d/1MXBbYq97z-
2euqCk Fg5e6eJda9x43v7/view?usp=sharing
7.06%), 2013 (12; 7.06%), 2008 (10; 5.88%), 2006,
2010 and 2017 (each with 9 papers; 5.29%), 2012 (8;
4.71%), 2002 and 1990 (each with 4 papers; 2.35%),
2007, 2000, and 1992 (each with 3 papers; 1.76%),
2009, 2005, 2004, 2001, and 1991 (each with 2 pa-
pers; 1.18%). There is only one paper published in
each of the following years: 1999, 1997, 1996, 1995,
1994, 1993, 1988, and 1986.
Note that there is an increasing interesting in the
publications on the use of educational technologies
in medical since 2006. It is also worth noting that,
as the search process of this review was performed
in September 2017, a slight decrease in the number of
publications would be expected in 2017 because some
papers might be in press.
1986
1988
1990
1991
1992
1993
1994
1995
1996
1997
1999
2000
2001
2002
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
0
5
10
15
20
25
30
1 1
4
2
3
1 1 1 1 1 1
3
2
4
2 2
9
3
10
2
9
12
8
12
20 20
24
9
Number of Publication per Year
Figure 2: Number of publications per year.
3.1.2 Articles Types
The types of sources could be journal, conference,
or book chapters. The majority of the articles are
the journal papers (63.53%, 108 studies), followed
by chapter books (20%, 34 studies), and conferences
(15.29%, 26 studies).
The venues with more contributions are: BMC
Medical Education (29 publications), Advances in
Health Sciences Education (5 publications), Medical
Science Educator and Lecture Notes in Computer Sci-
ence (including subsections in Artificial Intelligence
and Lecture Notes in Bioinformatics)(each one with 4
papers), and Medical Teacher (2 publications). How-
ever, one might note that several sources from edu-
cational technology, medicine and computer science
have been considered as possible venues for publica-
tion, which may suggest that scientific communities
are interested in this interdisciplinary field.
3.1.3 Research Method
The classification of the publications was based
on the categories (i.e.,controlled experiment, quasi-
experiment, case study, survey research, ethnography
and action research) defined by (Easterbrook et al.,
2008). However, we have defined two extra categories
to classify papers that did not fit in those categories:
CSEDU 2019 - 11th International Conference on Computer Supported Education
156

Table 1: Study quality assessment criteria. These criteria are adapted from (Dermeval et al., 2017). Y=Yes,N=No, and
M=Maybe.
# Questions Possible answers
Q1 Is there a rationale for why the study was undertaken? Y=1,0 ,N=0,0 ,M=0,5
Q2 Is there a clear statement of the goals of the research? Y=1,0 ,N=0,0 ,M=0,5
Q3 Is the proposed technique properly described? Y=1,0 ,N=0,0 ,M=0,5
Q4 Is there an adequate description of the context (industry,
laboratory setting, products used and so on) in which the
research was carried out?
Y=1,0 ,N=0,0 ,M=0,5
Q5 Does the study provide or use a tool? If so, is the tool
available for download on the internet?
Y=1,0 ,N=0,0 ,M=0,5
Q6 Was the study empiricaly evaluated? Y=1,0 ,N=0,0
Q7 Is there a discussion about the results of the study? Y=1,0 ,N=0,0 ,M=0,5
Q8 Are the limitations of this study explicitly discussed? Y=1,0 ,N=0,0 ,M=0,5
Q9 Does the study also evaluate the proposal in industrial
settings?
Y=1,0 ,N=0,0
Table 2: Extraction form.
# Study data Description RQ
1 Study Identifier Unique id for the study Overview
2 Author(s) Overview
3 Type of article Book chapter, Conference, Journal, Workshop Overview
4 Article Source Overview
5 Application context Industrial, academic Overview
6 Year Overview
7 Title Overview
8 Country Overview
9 Researchers genders Female, Male, Other Overview
10 Research Method Action research, Case study, Controlled experiment, Ethnography, Il-
lustrative Scenario, Not applicable, Survey
Overview
11 Type of educational
technologies
CSCL, Educational Game, Gamified, Environment, ITS, LMS, M-
learning, MOOC, Simulation, T-learning
RQ1
12 Medical education do-
mains supported
RQ2
13 Evidence Negative argumentation, Negative with empirical evaluation,Positive
argumentation, Positive with empirical evaluation
RQ3
illustrative scenario and not applicable. The first is
appropriate for papers that just explain their contribu-
tions using small examples or argumentation. The lat-
ter refers to the papers that do not present any kind of
research method or explanation of using the proposal.
Case Study (41.18%; 70 studies) constitute the
majority of the studies, followed by Not applica-
ble (20%; 34 studies), Survey (17.85%; 30 studies),
Controlled experiment (10.59%; 18 studies), illustra-
tive scenario (5.29%; 9 studies) and action research
(3.53%; 6 studies). It is worth noting that 118 studies
(70.23%) are concerned in conducting empirical stud-
ies (i.e., controlled experiment, case study, and sur-
vey) on evaluating or creating technologies for medi-
cal education. There were no ethnography and action
research papers in our classification.
3.1.4 Application Context
The paper settings were categorized as industry and
academic. The majority of them (93.45%; 157 pa-
pers) are in the academic category, whereas, 19 papers
(11.30%) belong to the industry category
3.2 RQ1: Types of Educational
Technologies
The purpose of this research question was to iden-
tify the main educational technologies used to support
medical education.
3.2.1 Results
The technologies were categorized into nine differ-
ent types, Computer-supported collaborative learning
(CSCL), Gamified environment, Educational Game,
learning management system (LMS), Simulation,
mobile-learning, intelligent tutoring system (ITS),
massive open online course (MOOC), tv-learning.
As seen in Table 3, the predominant type of ed-
ucational technology used in medical education is
A Systematic Review on the Use of Educational Technologies for Medical Education
157

Table 3: Studies over Technologies used.
Types of educational Tech-
nologies
Studies Freq %
LMS S11, S46, S58, S59, S91, S167, S125, S154, S88, S140, S168,
S1,S13, S16, S21, S32, S35, S36, 38, S48, S55, S56, S61, S62, S63,
S65, S66, S68, S69, S70, S71, S72, S74, S75, S77, S81, 83, S90,
S92, S94, S96, S97, S99, S102, S103, S104, S105, S108, S109,
S110, S114, S121, S124, S130, S132, S138, S139, S141, S143,
S144, S145, S148, S149, S150, S152, S157, S164, S14, S20, S127,
S158, S159, S5, S34, S19
75 44.12%
M-Learning S125, S8, S14, S20, S127, S158, S15, S22, S27, S28, S31, S67, S79,
S82, S89, S106, S107, S112, S116, S117, S119, S120, S128, S129,
S137, S142, S156, S163, S133, S165, S118
31 18.24%
Simulation S50, S101, S53, S134, S169, S5, S34, S2, S3, S7, S17, S18, S23,
S24, S39, S40, S42, S44, S54, S60, S76, S78, S87, S126, S136,
S161, S162, S166, S95
31 18.24%
ITS S10, S12, S25, S26, S29, S33, S37, S41, S47, S49, S64, S80, S93,
S100, S115, S135, S147, S151, S153, S155, S170, S140, S168,
S134, S169
25 14.71%
CSCL S4, S43, S45, S52, S73, S131, S146, S160, S85, S11, S46, S58, S59,
S91, S167, S125, S50
17 10%
Educational Game S6, S8, S30, S53, S84, S101, S154 7 4.12%
Gamified Environment S85, S84, S101, S86, S98, S88 6 3.53%
T-learning S19, S118, S95, S57, S123 5 2.94%
MOOC S159, S111, S122 3 1.76%
LMS (44.12%;75 studies), followed by Simulation
(18.24%;31 studies), M-learning (18.24%;31 stud-
ies), ITS (14.71%;25 studies), CSCL (10%; 17 stud-
ies), educational games (4.11%;7 studies), gamified
environment (3.52%;6 studies), t-learning (2.94%;5
studies) and MOOC (1.76%;3 studies). It is worth
noting that a publication could have used more than
one educational technology of the RE process. Thus,
the sum of the percentage is greater than 100%
3.2.2 Analysis and Discussion
In summary, we could note that several distinct types
of educational technologies have been used in medi-
cal education, showing the demand for different types
of educational technologies to target different medical
education needs. It is worth noting that most of the
papers (44.12%) are using LMS, which could suggest
that the studies are more focused on content reposi-
tories for medical education rather than on adaptive-
intensive educational systems (e.g., ITS). An interest-
ing result that we might mention is the frequent use
of mobile technologies for medical education, this re-
sults could indicate that mobile devices may be well-
accepted by medicine students. Moreover, educa-
tional technologies based on simulation are also fre-
quently used, which is expected since medical school
curricula uses lots of practical activities.
We also could note that some promising educa-
tional technologies might be underexplored in medi-
cal education. For example, educational games and
gamification could be more used along with other
types of educational games to target achieving more
engagement of medicine students.
3.3 RQ2: Medical Education Domains
The purpose of this research question was to main
medical domains where educational technologies
have been used.
3.3.1 Results
The classification of the medical domains was per-
formed after the data extraction step, that is, during
the extraction of data to answer this research question.
We identified 47 different medical domains where
these technologies were applied. Educational tech-
nologies have been used in several domains, for ex-
ample, for pediatric learning support (4.71 %, 8 stud-
ies), followed by anatomy study (4.12 %, 7 studies).
These areas are followed by teaching and practice
surgeries (3.53 %, 6 studies), diagnosis of diseases
(1.18 %, 2 studies), cardiology (3 studies, 1.76 %).
Note that a study could have targeted more than one
domain, so the sum of the percentage may be greater
than 100 %.
CSEDU 2019 - 11th International Conference on Computer Supported Education
158

Table 4: Medical education domains.
Medical Education
Domains
Studies Freq %
Anatomy S11, S17,S28 7 4.12%
Anesthesia S44 1 0.59%
Antimicrobia pre-
scribing
S8 1 0.59%
Atheromatosis S93 1 0.59%
Cardio-respiratory S132 1 0.59%
Cardiology S26, S47, S75 4 2.35%
Cardiopulmonary S142 1 0.59%
Cardiovascular Phys-
iology
S64 1 0.59%
Clinical education S102 1 0.59%
Cryosurgery S135 1 0.59%
Cytopathology S57 1 0.59%
Dental S150, S156 2 1.18%
Dermatology S76 1 0.59%
Chiropractic S151 1 0.59%
Diagnostic S151 2 1.18%
Emergency S50 1 0.59%
Endocrinology S77, S161 2 1.18%
Forensic medicine S24 1 0.59%
General practitioners S32 1 0.59%
Gynecologic S25 1 0.59%
Histology S158, S83 3 1.76%
Human Anatomy S35, S53, S165, S28 4 2.35%
Human Genetics S2 1 0.59%
Laparoscopy S54 1 0.59%
Microscopy S71 1 0.59%
Neurology S21 1 0.59%
Neuroradiology S69 1 0.59%
Oncology S13, S99, S134 3 1.76%
Operating S101 1 0.59%
Orthopedy S38, S90 2 1.18%
Pediatric S109, S23, S143, S154, S96,
S107, S133, S127
8 4.71%
Pathology S83 5 2.94%
Pharmacology S162, S28 2 1.18%
Physiology S29 1 0.59%
Pneumology S94 1 0.59%
Psychiatric S97, S124 2 1.18%
Radiology S19, S152 2 1.18%
Surgery S88, S123, S136 3 1.76%
Thoracic Surgery S87 1 0.59%
Traumatology S90 1 0.59%
Urology S30, S62, S159 3 1.76%
Venereology S76 1 0.59%
3.3.2 Analysis and Discussion
In fact, the great majority of the papers are not target-
ing any particular medical domain. This results might
suggest that researchers have been proposing generic
educational technologies not tied to specific medical
domains. However, it is worth noting that educational
technologies have been applied in a plenty of medical
domains, illustrating the need for research and devel-
opment for solutions in several areas. Another inter-
esting point that we can raise is that some technolo-
gies could be more amenable to be used in particular
domains. For example, it is expected that simulation
technologies might be more frequently use in surgery
domain that in psychiatric. As such, it would be also
interesting to investigate if there are some kind of cor-
relation between medical domains and the types of
educational technologies used.
3.4 RQ3: Supportive Evidence
The purpose of this research question was to gather
and classify evidences to state that using educational
technologies benefits or not medical education.
3.4.1 Results
The classification of the papers was defined accord-
ing to the presence or absence of empirical evaluation
in the paper and by the positive or negative indication
that using educational technologies benefits medical
education. The defined categories are: positive with
empirical evaluation, positive without empirical eval-
uation, negative with empirical evaluation and nega-
tive without empirical evaluation (see Table 5). As
shown in Table 5, 45.29% (77 studies) of the studies
reported positive evidence after conducting empirical
evaluation and 44.29% of studies (76 studies) only
presented positive argumentation about the benefits of
educational technologies. In addition, 4.71% (8 stud-
ies) presented negative evidence after running empiri-
cal evaluation and 3.53% (6 studies) argued about the
negative implications of using educational technolo-
gies in medical education.
Table 5: Supportive evidence.
Types of evidence Studies Freq %
Positive argumentation S1, S2, S7, S8, S12, S16, S20, S21, S23, S24, S25,
S26, S28, S33, S39, S40, S42, S43, S44, S45, S46,
S47, S48, S49, S50, S53, S56, S57, S58, S59, S60,
S61, S67, S69, S70, S77, S78, S80, S81, S83, S84,
S85, S88, S91, S93, S98, S100, S101, S103, S105,
S106, S107, S109, S110, S111, S112, S117, S120,
S121, S125, S130, S131, S136, S145, S147, S148,
S150, S152, S155, S159, S160, S162, S164, S165,
S167, S170
77 45,29%
Positive with empirical evaluation S3, S4, S5, S6, S9, S10, S11, S13, S14, S15, S18,
S22, S27, S29, S30, S31, S34, S36, S37, S38, S41,
S52, S54, S62, S63, S65, S66, S68, S74, S75, S76,
S79, S82, S86, S87, S89, S90, S92, S94, S95, S99,
S102, S104, S108, S115, S116, S118, S119, S122,
S123, S124, S126, S127, S128, S129, S132 ,S133,
S134, S137, S138, S139, S140, S142, S144, S146,
S149, S151, S153, S154, S156, S157, S158, S161,
S163, S166, S168,S169
78 45,88%
Negative argumentation S17, S19, S32, S64, S72, S114, S143 8 4.71%
Negative with empirical evaluation S35, S55, S71, S73, S135, S141 6 3.53%
3.4.2 Analysis and Discussion
Majority of the studies (91.07 %, 153 studies) pre-
sented positive evidence of the efficacy on using edu-
cational technologies in the context of medical educa-
tion. Within these studies, 44.71% presented positive
arguments and 45.29% reported positive evidence.
These results indicate the potential of using educa-
tional technologies for medicine education. However,
negative evidence is also reported in the studies. This
result is interesting, since they are showing the crit-
icism of the scientific community publishing a work
that did not provide results as expected.
In summary, the evidence reported on studies sug-
gests that different types of educational technologies
benefit medical education in several distinct domains.
A Systematic Review on the Use of Educational Technologies for Medical Education
159

However, more research is needed to better explore
promising educational technologies, for instance, ed-
ucational games, gamification, ITS, CSCL – or the
combination of them – considering different contexts.
4 CONCLUDING REMARKS
In this work, we aimed at understanding how educa-
tional technologies have been used in medical educa-
tion through the conduction of a SLR. More specif-
ically, the major objective of this SLR was to better
understand how current educational technologies can
give support to medical education and identify in what
way this concept is being applied to this field.
One hundred and sixty eight papers on the re-
view topic were included, in which nine types of tech-
nologies are applied in forty-two medical domains.
Among the nine types of educational technologies,
LMS is the highest technology used in medical ed-
ucation. Moreover, it is worth noting that the com-
munity is interested in using more ”intelligent“ ed-
ucational systems or promising technologies to tar-
get medical education since technologies such as ITS,
mobile learning applications, educational games and
MOOCs have also been used (despite being quite un-
derexplored so far).
As future work we intend to explore other research
questions for this SLR, for instance, to understand
which features have been incorporated in the educa-
tional technologies applied in medical education as
well as to gather metrics for evaluating the effective-
ness of the such technologies in learning improve-
ment.
REFERENCES
Dermeval, D., Paiva, R., Bittencourt, I. I., Vassileva, J., and
Borges, D. (2017). Authoring tools for designing in-
telligent tutoring systems: a systematic review of the
literature. International Journal of Artificial Intelli-
gence in Education, pages 1–49.
Easterbrook, S., Singer, J., Storey, M.-A., and Damian, D.
(2008). Selecting empirical methods for software en-
gineering research. In Guide to advanced empirical
software engineering, pages 285–311. Springer.
Ellaway, R. and Masters, K. (2008). Amee guide 32: e-
learning in medical education part 1: Learning, teach-
ing and assessment. Medical teacher, 30(5):455–473.
Jabbar, A., Militk
`
y, J., Kale, B. M., Rwawiire, S., Nawab,
Y., and Baheti, V. (2016). Modeling and analysis
of the creep behavior of jute/green epoxy compos-
ites incorporated with chemically treated pulverized
nano/micro jute fibers. Industrial Crops and Products,
84:230–240.
Kalaian, S. A. and Kasim, R. M. (2017). Effectiveness of
various innovative learning methods in health science
classrooms: a meta-analysis. Advances in Health Sci-
ences Education, 22(5):1151–1167.
Kitchenham, B. and Charters, S. (2007). Guidelines for per-
forming systematic literature reviews in software en-
gineering.
Taveira-Gomes, T., Ferreira, P., Taveira-Gomes, I., Severo,
M., and Ferreira, M. A. (2016). What are we looking
for in computer-based learning interventions in medi-
cal education? a systematic review. Journal of medi-
cal Internet research, 18(8).
CSEDU 2019 - 11th International Conference on Computer Supported Education
160
