
Muscle Force Assessment in the Presence of Indeterminate Deficiency
Joseph Mizrahi
1
, Etgar Marcus
1
and Avi Wiener
2
1
Technion, Israel Institute of Technology, Haifa, Israel
2
Rambam Medical Center, Haifa, Israel
Keywords: Indeterminate Deficiency, Force Assessment, Mind Distraction, Computer Adaptive Testing.
Abstract: Indeterminate deficiency is encountered when a subject puts an artificial limit on his/her muscle abilities, in
which case his/her true muscle force cannot be assessed in a straight forward manner. Self-restriction of
muscle performance during testing may be unintentional due to lack of motivation, lack of self-confidence or
due to fear of pain. It can, however, be intentional resulting from unwillingness to cooperate. The aim of this
study was to develop an objective system aimed at directing subjects into generating more intense muscle
forces than they aimed, thus leading to their true force potential. The methodology used combines mind
distraction techniques and Computer Adaptive Testing (CAT) theory. The first element is aimed at distracting
the examinees from restricting their muscle force, or shifting the interval of convenience of their performance.
The examined subject is thus directed into generating higher muscle forces than he/she has intended to, thus
reaching the highest possible force. Practically, the tested subject is asked to perform tasks of varying
intensities, visually presented in subject-unanticipated real-time converted-scale display biofeedback. For the
second element of our methodology we made use of the Item Response Theory custom-tailored itemized test,
for people with various ability levels. A developed iterative CAT algorithm provided, individually for each
subject, rapid convergence to the highest force level possible. The results of this study bear potential
significance in two major areas: Rehabilitation Medicine, by indicating training procedures for unconfident
patients and in Occupational Medicine, for the functional evaluation of subjects who exhibit lack of
motivation or cooperation.
1 INTRODUCTION
The neuro musculo skeletal system is characterized
by redundancies, whereby a motor task can be
normally performed with the simultaneous
involvement of more muscles than strictly necessary.
Furthermore, this same task may be performed in
multiple ways, with different muscle combinations.
From the mechanical viewpoint the musculoskeletal
system is indeterminate, whereby the number of
unknown muscle forces exceeds the number of
available equations. Impairment has been associated
with reduced redundancy (Mizrahi et al 2011). The
level of indeterminacy was shown to decrease with
the reduction of redundancy, e.g. through single
stance (compared to double stance) standing or
through fatiguing of part of the muscles implying, that
higher levels in the nervous system become more
unequivocally related to lower levels (Levin et al
2000; Suponitsky et al 2008;). An interesting type of
deficiency is found when neither the identity of
impairment, nor its extent are certain, thus suggesting
the term Indeterminate Impairment.
This study deals with false impairment,
encountered when tested subjects, either
unintentionally or intentionally, exert an untrue limit
on their force, in which case their real capacity cannot
be disclosed in a straight forward measurement. The
need for force measurement arises when physical
performance is to be assessed such as in Occupational
Medicine.
Assessment of muscle force is usually performed
by evaluating the maximal voluntary contraction
(MVC) of the tested muscle (Chaffin et al, 1999),
necessitating cooperation of the tested subjects.
However, since the muscles are sub-activated because
the tested subject does not apply his/her maximal
force capacity, the accuracy by which the measured
force reflects the real muscle capacity becomes
questionable (Shechtman et al 2012, Garcia et al
2014). This may happen in either of the following two
cases: (a) unintentional self-restriction, due to lack
motivation or self-confidence, fear of pain or injury
Mizrahi, J., Marcus, E. and Wiener, A.
Muscle Force Assessment in the Presence of Indeterminate Deficiency.
DOI: 10.5220/0007565400810086
In Proceedings of the 12th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2019), pages 81-86
ISBN: 978-989-758-353-7
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
81
(Sullivan et al. 2009), guarding; or (b) deliberate
restriction, due to low, or no willingness to cooperate.
Muscle force malingering has been reported in the
literature. Although there are no definite indications
about the extent of malingering during physical
functional assessment, reviewed studies have
indicated that malingering does occur within the
chronic pain setting, at the rate of 1.25-10.4% of
chronic pain complaints (Fishbain et al 1999).
Here, we developed a Computer Adaptive Testing
(CAT) system (Hambleton 2000; Hays et al. 2000),
specially adapted for physical testing, and aimed at
objectively evaluating muscle forces, in those cases
where the muscles are sub-activated. Basically, CAT
is based on modern testing theory to select the optimal
next task to be administered based on the examinee’s
previous responses.
In addition, we established a computerized task
algorithm, combined with real-time visual feed-back
designed to distract the examinees’ attention away
from the actual testing objectives. We hypothesized
that, by combining CAT principles and mind-
distraction techniques, it is possible to direct subjects
into generating a greater sub-maximal force than they
intended (Sullivan et al. 2009; Wiener et al 2007). In
this way, it was expected that a more objective MVC
can achieved from the tested subject (closer to the real
capacity of the muscle), which is less dependent on
the level of cooperation of the participating subjects
in the testing procedure. The results of this study bear
potential significance in two major areas:
Rehabilitation Medicine, by indicating training
procedures for unconfident patients and, in
Occupational Medicine, for the functional evaluation
of subjects who exhibit lack of motivation or
cooperation.
2 MATERIALS AND METHODS
2.1 Apparatus
Muscle forces were measured through the
corresponding joint torques. Two experimental
systems were thus designed to measure the torques
during isometric extension efforts of the knee, or
during isometric flexion of the elbow. The systems
were adjustable with restraints on which the volunteer
subjects were seated during testing (Fig. 1). Data
acquisition was made by sampling the force from the
transducer at 200 Hz into an A/D acquisition card and
a Lab-View interface (National Instruments
Corporation, Austin, TX).
2.2 Procedure
The concept of CAT combined with mind distraction
was tested on a group of 11 able-bodied female
subjects, aged 26.2 (1.6) years, who were instructed
to cooperate in fulfilling the testing instructions, as
described in Table 1.
First, the examinee was asked to exert the highest
isometric force, denoted as the initial maximal
voluntary contraction (MVCi). This was repeated
three times with an interval time of 10 min for
averaging the actual MVCi. It was assumed that,
since the subjects were cooperative, the measured
MVCi was representative of the true initial maximal
voluntary contraction. Thus, except for adjustment
due to possible existence of fatigue, the individual
MVCi could be used as a reliable measure for force
normalization.
Table 1: Summary of the Testing protocol, indicating
subject cooperativity.
Exert MVC Subject cooperates
Training to memorize Fssl Subject cooperates
CAT tests Subject does not obey
task, but instead observes
his/her force limit Fssl
Post-test MVC Subject cooperates
Repeatability of Fssl Subject cooperates
Thereafter, each tested subject was trained to set
and memorize a self-selected force limit Fssl (usually
near 20–50% his/her MVCi). The training process
was made with real-scale feedback, as displayed on a
monitor and was not limited in time. Training was
terminated when the examinee felt confident in being
able to memorize his/her Fssl, which usually
corresponded to force reproducibility of better than
5% of the selected Fssl. This memorized force (force
or joint memory) was later used by each subject to
apply force restriction irrespective of the force being
instructed to apply in the testing algorithm. It should
be noted that successfully memorizing this limit force
and observing the limit was essential for indicating
whether the testing algorithm was capable of
distracting the tested subject to higher forces.
BIODEVICES 2019 - 12th International Conference on Biomedical Electronics and Devices
82
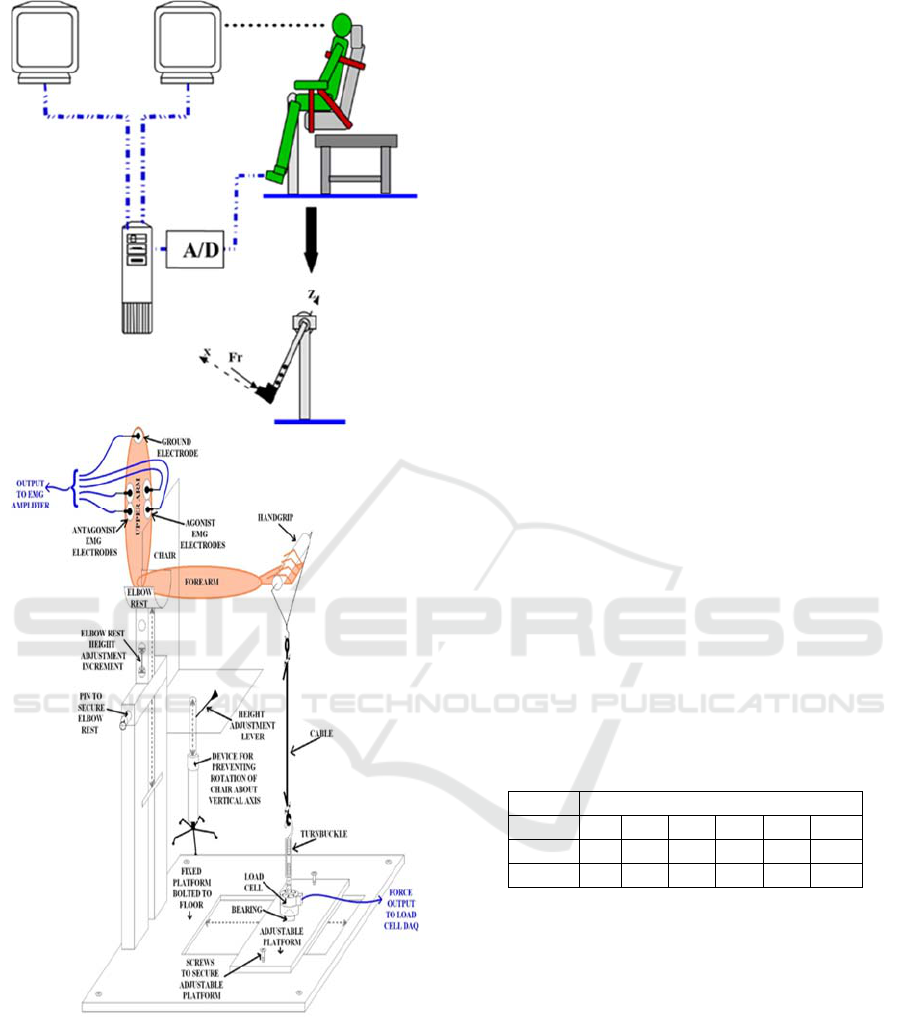
Figure 1: Isometric testing apparatus: top, for knee
extensors; bottom for elbow flexors. Experimental features
include, among others, dual visual screens and EMG
electrodes.
2.3 CAT Testing Algorithm
The CAT phase consisted of two different tests: The
algorithm-test and, the repeatability-test. The
algorithm-test was designed to verify whether the
CAT system could cause the examinee to
unintentionally exert a higher force than he/she
intended to. We developed an algorithm aimed to
distract the examinee’s attention from the objective of
keeping steady the memorized limit force on each
new task. For this purpose, the algorithm consisted of
two scales to describe the examinee’s effort. A real
scale was displayed on the operator screen monitor
and a false (converted) scale was displayed on the
examinee’s (apparent) screen monitor (Fig. 1, top).
The examinee was asked to perform a force-
application task which, on the operator monitor was
displayed in MVC percentage units (real force). This
was indicated on the screen by means of two
horizontal parallel “target lines” between which the
force should be aimed. On the examinee’s monitor,
this same task (apparent force) was represented in a
converted scale. The scaling (or distraction) factor SF
is defined as Apparent Force / Real Force. During
task performance, the examinee was reminded not to
exceed his/her self-selected limit force (Fssl).
For each testing cycle, a baseline mission was set
and, every task was considered to be equal 100%,
50% or 150% of this baseline according to the
difficulty level set by the force target factor (FTF).
On the operator screen, the real Ftarget force was
displayed. On the examinee’s screen the task was
represented as the product of the target force, the
scaling factor (SF, or distraction factor) and the force
target factor (FTF). Values of SF, and FTF in a cycle
are given in Table 2.
Table 2: Values of SF and FTF for every task, in a one
complete cycle.
One Task cycle
Task 1 2 3 4 5 6
SF 1 2 1 0.5 0.5 0.5
FTF 1 0.5 0.5 0.5 1 1.5
The operator terminated the algorithm test when
the examinee exerted a significantly higher force than
his/her self-selected limit force, or after completion of
two cycles.
2.4 Adjustment for Muscle Fatigue
After completion of the CAT, the maximal voluntary
contraction was measured again to verify whether the
muscle had undergone fatigue during the test (final,
MVCf). This was repeated three times and the
average was taken to represent the actual MVCf. Thus,
the true final maximal voluntary contraction MVCf,
provided a correction for MVCi due to the possible
development of muscle fatigue during the test. The
Muscle Force Assessment in the Presence of Indeterminate Deficiency
83
values of MVCf and MVCi were used to linearly
interpolate MVCtask, corresponding to each actual
task and to which the force values were normalized
during the test.
2.5 Repeatability of Joint Memory
Repeatability of joint memory was tested one week
after the CAT with similar number of cycles and
testing durations as in the CAT. Its purpose was to
confirm the subject’s ability to remember her Fssl.
3 RESULTS
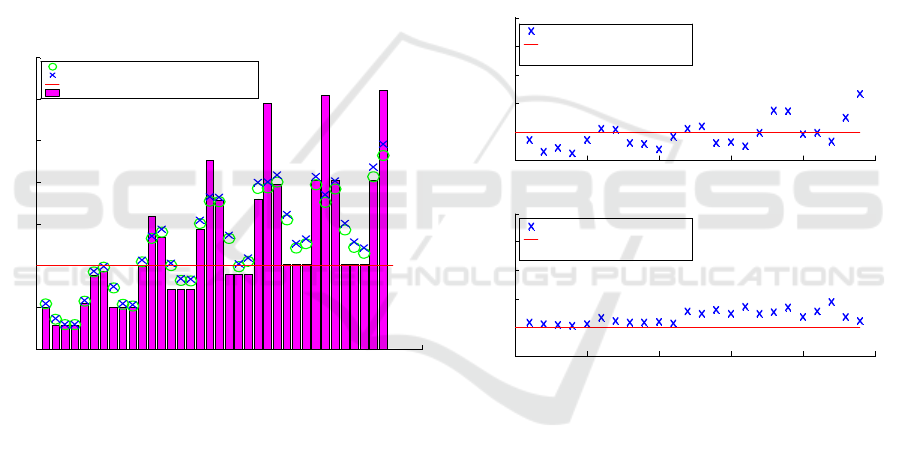
A typical force-task during a complete test cycle is
shown in Fig. 2. The memorized force limit (0.4
MVC, in this case) is displayed by the horizontal line.
It
is noted that the task intensities generated by the
Figure 2: Force tasks in complete cycle (36 tests) for subject
10 (with Fssl at 0.4 MVC, shown as a horizontal line). Note
the zigzag effect of the algorithm on the task intensity
between the tasks. This effect is added to the distraction
effect caused on the subject’s screen. Force results are
shown: without fatigue adjustment (o) and with fatigue
adjustment (x).
CAT algorithm demonstrate a zigzag pattern. The
tested subject obtains these tasks on his/her screen in
a false (converted) scale, thus distracting him/her
from the real task, resulting in producing higher
forces than he/she meant to.
Fig. 3 demonstrates the force output for one
subject, as obtained using the CAT in a complete
cycle (top), as compared to the force output during the
repeatability test. The force values at the initial and
final ends of the test were normalized by using the
respective MVC values. For any intermediate task,
the MVC was interpolated. In the CAT (upper panel)
the examinee’s performance was characterized by
oscillations of the exerted forces below and over Fssl.
The applied force eventually reached a magnitude of
as high as 2.34 Fssl (score of the CAT). However, in
the repeatability test (lower panel), the fluctuations
around the level of Fssl were smaller compared to the
CAT with a maximum score of 1.88 Fssl. Thus, the
testing algorithm was successful in ‘tricking’ subject
5 and a higher force was obtained despite her attempts
to maintain the memorized force Fssl.
Summary of the scores, for the CAT and for the
repeatability tests, for all the subjects, is presented in
Table 3. The mean score values of the CAT and the
repeatability tests for all the participants were 1.995
Fssl and 1.554 Fssl, respectively, with a statistically
significant difference (p < 0.05) between them. Ten
out of the eleven subjects rendered a higher force than
intended by their self-imposed limit.
Figure 3: Force applied (normalized to base-line force Fbl):
comparison between CAT and repeatability tests (subject
5). The value of Fssl was in this case 0.3 MVCi. Test score
denotes the highest force value attained during the test
(CAT, or repeatability).
4 DISCUSSION
Accurate functional testing and physical
measurement is important for the objective diagnosis
of physical impairment. This however is being
prevented whenever the tested subject sets an
artificial upper limit on his/her muscle force, resulting
in sub-activation of the muscle. The true force
capacity cannot in this case be assessed or utilized in
a straight forward manner. In this study a model of
able-bodied subjects served to simulate muscle sub-
0 5 10 15 20 25 30 35 40
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Performance - Algorithm Test - subject # 10
Normalized Force
Task [#]
Performance (Fmeasured) without fatigue adjustment
Performance (Fmeasured) with fatigue adjustment
Self Selected Limit Force [level of MVC]
Task Difficulty (Ftarget)
0 5 10 15 20 25
0
1
2
3
4
5
Performance - Algorithm Test - subject # 5
Normalized Force
Task [#]
Subject Task Performance (Fmeasured)
Self Selected Limit Force [0.3 MVC]
Score= 2.3442
0 5 10 15 20 25
0
1
2
3
4
5
Performance - Repeatability Test - subject # 5
Normalized Force
Task [#]
Subject Task Performance (Fmeasured)
Self Selected Limit Force [0.3 MVC]
Score= 1.8881
BIODEVICES 2019 - 12th International Conference on Biomedical Electronics and Devices
84
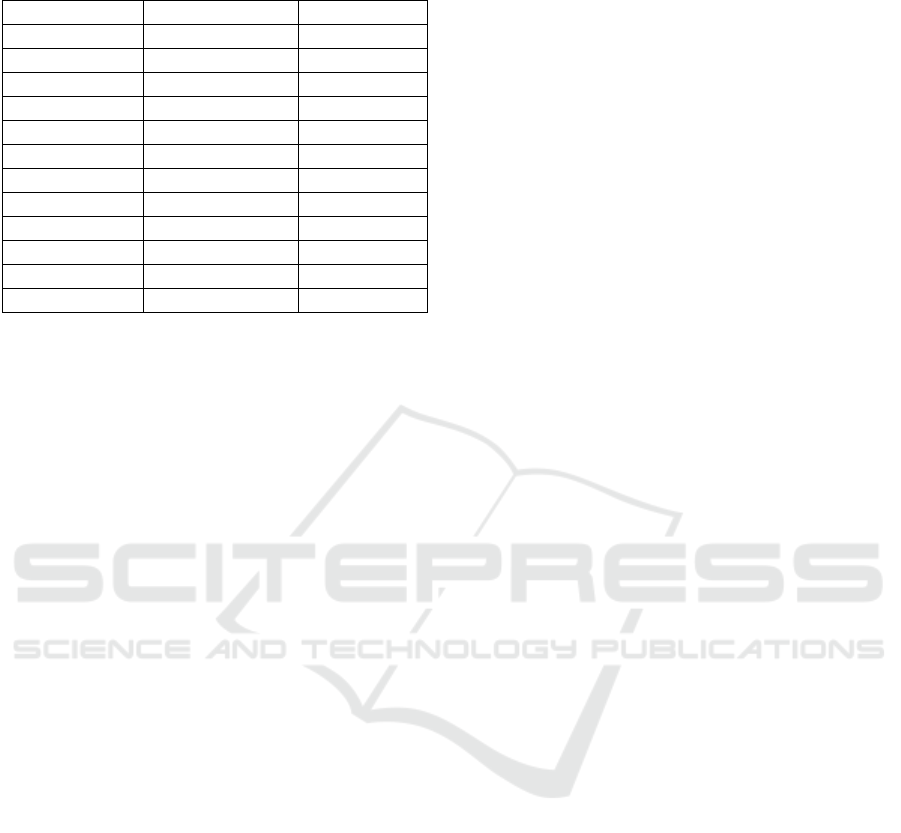
Table 3: Results of algorithm and repeatability tests for all
subjects.
Subject # CAT Algorithm Repeatability
1 1.979 1.403
2 2.089 1.183
3 2.436 2.674
4 0.957 0.954
5 2.344 1.888
6 1.385 1.155
7 2.027 1.552
8 3.193 1.742
9 1.850 1.590
10 2.458 1.672
11 1.225 1.279
Average (SD) 1.995 (0.64) 1.554 (0.47)
activation. These subjects were trained to memorize a
certain sub-maximal force in their muscle (via its
corresponding joint). In subsequent force tasks, each
subject was instructed to watch that during task
performance his/her memorized force is not exceeded.
The force tasks were within a series of tests
combining CAT and mind distraction. The former
element was based on IRT (item response theory), a
custom-tailored itemized test based on probability of
a favourable outcome for people of various ability
levels, and testing was done in iterative steps taking
into account the subjects abilities and task scores. The
second element, mind distraction, was designed to
distracting the examinee from restricting his/her
muscle force, or shifting the interval of convenience
of his/her performance, so as to direct him/her into
generating higher muscle forces than he/she has
intended to, and thus reaching the highest forces
possible for this subject. The results demonstrated
that in 10 of the 11 tested subjects the algorithm was
successful in revealing higher forces in knee
extensors than intended by the tested subjects. The
tests should be extended to elbow flexors as well.
These results can serve as an encouragement to apply
the method described to populations of subjects
characterized by muscle sub-activation, either from
unintentional or intentional reasons.
Unintentional muscle sub-activation may be due
to lack of motivation, lack of self-confidence, or fear
of pain, such as may take place after trauma, injury or
surgery and involving time periods of recovery and
rehabilitation. Intentional sub-activation is
encountered when the tested subject declines to
revealing his/her muscle force potential within his/her
overall physical functioning and resulting in lack of
willingness to cooperate.
The significance of revealing the true muscle
force potential is thus clear: In rehabilitation
medicine, Increased rehabilitation and treatment
progress and efficiency, design and assessment of
suitable treatment plan and increased self-esteem of
the patient, decreased burden on patients; In
occupational medicine, better functional assessment
and return to employment, decreased cost to patients,
treatment facilities, and insurance companies. Future
work should extend the suggested method to these
populations.
REFERENCES
Chaffin, D.B.; Andersson, G.B.J. and Martin, B.J. (1999)
Occupational biomechanics. 3rd ed. New York: John
Wiley & Sons, pp. 91–130.
Fishbain, D. A., Cutler, R.; Rosomoff, H. L. and Rosomoff,
R. S. (1999). Chronic Pain Disability
Exaggeration/Malingering and Submaximal Effort
Research, Review, The Clinical Journal of Pain 15(4):
244-274.
García, D.V., Dierckx, R. A., Otte, A. and Holstege, Gert
2014. Whiplash, real or not Real? A review and new
concept. In: PET and SPECT in Neurology. Springer,
Berlin Heidelberg, pp 947-963.
Hambleton, R. K. (2000). Emergence of item response
modeling in instrument development and data analysis.
Med Care 38:II: 60-65.
Hays, R. D., Morales, L. S. and Reise, S. P. (2000). Item
response theory and health outcomes measurement in
the 21st century. Med Care 38:II: 28-42.
Levin, O.; Mizrahi, J.; Adam, D., Verbitsky, O. and Isakov,
E. (2000). On the Correlation Between Force Plate Data
and EMG in Various Standing Conditions, In:
Proceedings of the Fifth Annual Conference of the
International Functional Electrical Stimulation
Society, T. Sinkjaer, D. Popovic & J.J. Struijk (Eds), pp.
47–50, Center for Sensory- Motor Interaction, Aalborg
University, Denmark,. June 18–24, 2000.
Mizrahi, J. (2011). The Role of Electromyograms in
Resolving Musculoskeletal Interactions in Able-bodied
and Disabled Human Individuals, In: Advances in
Applied Electromyography, Ed. Joseph Mizrahi,
InTech, (ISBN 978-953-307-382-8), pp 3-24.
Shechtman, O.; Sindhu, B.S. and Davenport, P.W (2012).
Using the “Visual Target Grip Test” to Identify
Sincerity of Effort during Grip Strength Testing,
Journal of Hand Therapy 25(3): 320-329.
Sullivan, M., Tanzer, M., Stanish, W., Fallaha, M., Keefe,
F. J., Simmonds, M. and Dunbar, M. (2009).
Psychological determinants of problematic outcomes
following Total Knee Arthroplasty. Pain 143:123-129.
Suponitsky, Y., Verbitsky, O., Peled, E., and Mizrahi J.
(2008). Effect of Selective Fatiguing of the Shank
Muscles on Single-Leg-Standing Sway, J.
Electromyography and Kinesiology, 18:682-689.
Muscle Force Assessment in the Presence of Indeterminate Deficiency
85

Wiener, A., Marcus, E., and Mizrahi, J. (2007). Objective
measurement of knee extension force based on
computer adaptive testing, J. Electromyography and
Kinesiology, 17:41-48.
BIODEVICES 2019 - 12th International Conference on Biomedical Electronics and Devices
86
