
Emotional and Behavioral Aspects of Children with Thalassemia
in Banda Aceh, Indonesia
Ilma Tawarina
1
, Farah Diba
2
1
Undergraduate Programme of Nursing Science, Faculty of Nursing, Syiah Kuala University, Banda Aceh, Indonesia
2
Department of Community Health Nursing, Faculty of Nursing, Syiah Kuala University, Banda Aceh, Indonesia
Keywords: Emotion, Behavior, Thalassemia patient, Strengths and Difficulties Questionnaire (SDQ)
Abstract: Thalassemia is an inherited disorder that can hardly be cured. A thalassemia patient needs blood transfusion
for a lifetime. A child with thalassemia might experience emotional and behavioural changes due to some
changes in his or her physical function which might lead to particular psychosocial effects. The purpose of
this research was to identify the overview of emotional and behavioural aspects of children with thalassemia
in one of the public hospital in Aceh. This descriptive-quantitative research was conducted with a cross-
sectional study approach. There were 117 respondents participated in the study by using consecutive
sampling technique. The data collected by utilising the ‘Strengths and Difficulties Questionnaire’ (SDQ)
assessing the emotional symptoms, behavioural issues, peer relations, hyperactivity disorder, and prosocial
behaviour as the five sub-variables. The result of univariate data analysis showed that children with
thalassemia had the emotional and behavioural aspects (89.7%), and the five sub-variables – emotional
symptoms (74.4%), behavioural issues (76.9%), peer relations (59.0%), hyperactivity disorder (84.4%), and
prosocial behaviour (69.2%). Hence, it is suggested that the medical workers keep educating the parents in
order to maintain the emotional and behavioural aspects of children with Thalassemia.
1 INTRODUCTION
Thalassemia is a hereditary disease characterized by
a disturbance in the synthesis of haemoglobin (Hb)
resulting from a change in the level of globin chain
production. In 2011 the World Health Organization
(WHO) stated that about 5% of the world's
population carries haemoglobin-carrying genes,
especially sickle cell disease and thalassemia.
However, in some regions shows the percentage of
carriers is 25%, with an estimated more than
300,000 babies born with haemoglobin
abnormalities every year and mostly in low and
middle income countries. WHO also states that this
condition is mostly common in the tropical region,
but the migration of residents has spread this disease
to most countries (Fatmasyithah & Rahayu, 2014).
Thalassemia International Federation (TIF)
(2011) reported that Indonesia is included in the
group of countries with high risk of thalassemia.
According to the Indonesian Ministry of Health
(2013) the prevalence of thalassemia’s carrier in
Indonesia is estimated around 3-8%. If the
percentage of thalassemia reaches 5%, with a birth
rate of 23 per 1,000 of the 240 million population, it
is estimated that there are around 3,000 babies with
thalassemia born every year. The results of the 2007
Indonesian Basic Health research (RISKESDAS)
showed the national prevalence of thalassemia was
0.1%. Currently, thalassemia is still a global
problem that requires special attention. Thalassemia
is found throughout the world with the highest
prevalence of thalassemia genes in several tropical
countries (TIF, 2008).
Data from the Indonesian Ministry of Health in
2010, Aceh province was recorded as a province
with the highest percentage of thalassemia in
Indonesia with a figure of 13.4% (Fatmasyithah &
Rahayu, 2014). According to WHO global incidents,
1 in 5 children aged less than 16 years’ experience
emotional and behavioural problems. In Singapore
for example, 12.5% of children aged 6 -12 years
have emotional and behavioural problems (Wiguna
et al., 2010). Research conducted in one of hospitals
in Surakarta, Indonesia in 2013 found that the
prevalence of emotional and behaviour problems in
Thalassemia children is 26% (Nurhaeni, 2015).
Tawarina, I. and Diba, F.
Emotional and Behavioral Aspects of Children with Thalassemia in Banda Aceh, Indonesia.
DOI: 10.5220/0008397200002442
In Proceedings of the Aceh International Nursing Conference (AINC 2018), pages 255-260
ISBN: 978-989-758-413-8
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
255
Emotional and behavioral problems in children
lead to difficulties in learning since it is difficult to
focus and concentrating, poor ability to remember,
behave inappropriately in the school environment
and will increase delinquency and crime in
adulthood (Blanchard et al., 2006). Emotional and
behavioral problems are one of the several problems
that cause barriers to a child's development such as
psychosocial problems, depression in children, and
other mental disorders. Emotional and behavioral
problems in children are a serious problem since
they affect the children development and cause a
decrease in productivity and quality of life (Wiguna
et al, 2010). Various bio psychosocial stressors are
often associated with the occurrence of emotional
and behavioral problems in children, such as
physical illness, domestic violence, inadequate peer
relationships and parenting (Wiguna et al., 2010).
Inadequate parenting will have an impact on
children development, namely parents who are
authoritarian children will tend to be hostile and
rebellious. Children whose parents are permissive
tend to behave freely or uncontrolled and in children
whose democratic parents tend to avoid anxiety
chaos (Yusuf, 2009).
This study aimed to assess the major chronic
thalassemia pain conditions which include:
emotional and behavioral disorders by using the
standard instrument in order to detect psychosocial
problems of children aged 4 - 17 years. The
instrument called the ‘Strength and Difficulties
Questionnaires’ (SDQ). SDQ has become one of the
most widely used standard measurements in child
psychology to evaluate behavioral and emotional
problems. Research conducted by Riyana & Riza
(2017) mentioned that there is a behaviour disorder
in major thalassemia children. It was found there
were 22 children (73.3%) with disrupted categories
from children with internal behavioral disorders.
Whilst for children with external behaviour, there
were 12 children (40.0%) from 30 children with
major thalassemia is classified as a normal category.
2 METHODS
2. 1 Study Design
This is a descriptive quantitative study with cross
sectional design. The respondent in this study is 117
parents who have children with thalassemia aged 4 -
17 years. The data was collected consecutively in the
provincial referral public hospital in Banda Aceh.
2.2 Instrument
Data collection tools used in this study is SDQ
instrument consisting of three parts; parent
demographic data, child demographic data, and an
existed questionnaire “Strength and Difficulties”
Questioner consists of 25 questions and divided into
5 sub-variables namely, 1) Emotional symptoms, 2)
Behaviour changes, 3) Peer relationships, 4)
Hyperactivity, and 5) Prosocial behaviour. Each sub-
variable consisted of 5 questions (Goodman, 2010).
This SDQ questionnaire has been translated to 87
languages around the world including Bahasa
Indonesia.
2.3 Data Analysis
The scoring template is available on the SDQ
website. The total score of each aspect also the
overall result of the 5 sub-variables are classified
with normal, borderline, and abnormal categories.
Demographic data is analysed with the univariate
analysis.
3 RESULTS
Based on the research conducted on 117
respondents, the following results were obtained:
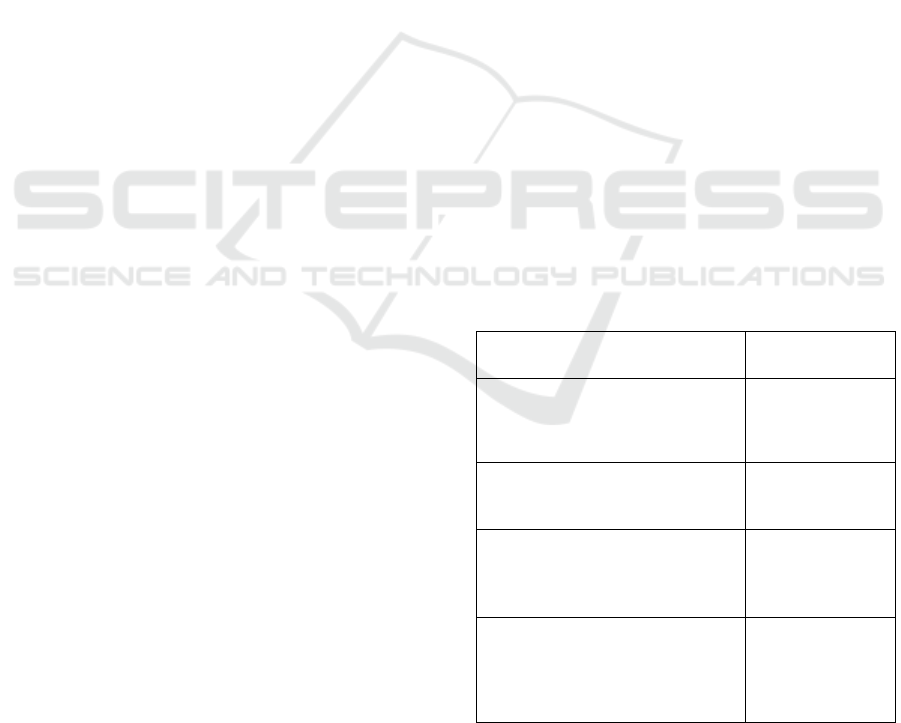
Table 1: Demographic Data of Parents of Children with
Thalassemia.
Demographic Data
Percentage
N=117
Age
17-25
26-35
36-45
2.6
38.5
59.0
Gender
Male
Female
33.3
66.7
Education
Elementary -Junior High School
Senior High School
University
25.6
64.1
10.3
Occupation
Farmers
Labourers
Housewives
Entrepreneur
51.3
2.6
41.0
2.6
Based on table 1, it can be concluded that most
respondents who have children with thalassemia are
generally in the late adults with the average age of
AINC 2018 - Aceh International Nursing Conference
256
38 to 45 years old (59.0%). Most children come to
hospital with their mother (66.7%). Parent education
level is on senior high school (46%). Most parents
(51.3%) work as farmers.
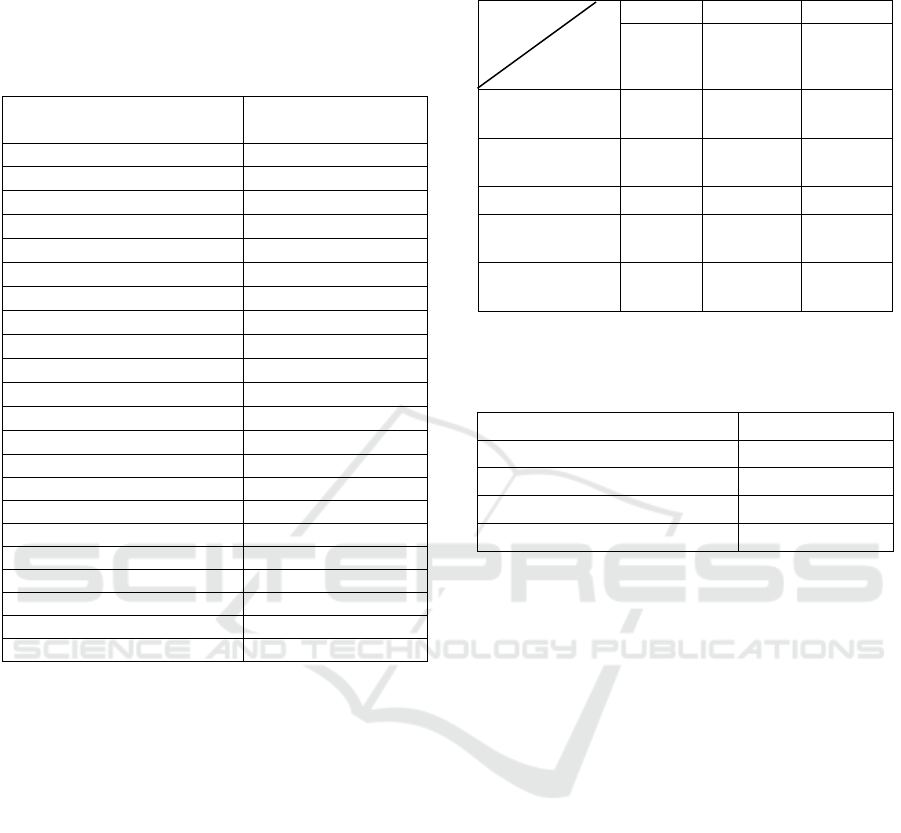
Table 2: Demographic Data of Thalassemia Children.
Demographic Data Percentage (%)
N= 117
Age:
Toddler 20.5
School Age 46.2
Early teenage 30.8
Late teenage 2.6
Gender:
Boy 43.6
Girl 53.8
Education:
No Education 41.0
Elementary School 48.7
Junior High School 10.3
Family order:
First child 51.3
Second child 7.7
Third Child 30.8
Fourth child 7.7
Fifth child 2.6
First Diagnosed
0-1 years old 66.7
2-3 years old 30.8
4-5 years old 2.6
Based on table 2, it can be concluded that 46.2%
thalassemia children are in the school age and come
to do the treatment at the provincial referral public
hospital in Banda Aceh. 53.8% of the children who
were doing the thalassemia therapy are girls. Most of
them are in elementary school (48.7%). More than
50% of the children with thalassemia are the first
children in the family. They were first diagnosed on
the age below 1 year old (66.7%).
Table 3 shows the result of each aspects of the
emotion and behaviour of children with thalassemia
in Aceh. For emotional symptoms shows that 74.4%
children are in abnormal category and 76.9 %
children with thalassemia has abnormal behaviour
issues. In regards with peer relations with other
children, 59% are in abnormal category. 84.6%
children with thalassemia have hyperactivity
disorder and lastly 69.2% of the children have
problems with prosocial behaviour in abnormal
category.
Table 3: Distribution of each Aspect of Emotions and
Behaviour of Thalassemia Children.
Aspects
Category
Normal Borderline Abnormal
(%) (%) (%)
Emotional
symptoms
15.4 10.3 74.4
Behavioral
issues
12.8 10.3 76.9
Peer relations
33.3 7.7 59.0
Hyperactivity
disorder
10.3 5.1 84.6
Prosocial
behaviour
7.7 23.1 69.2
Table 4: Total distribution of total score of emotional and
behaviour aspects children with thalassemia in Aceh.
Category (%)
Normal 4.1
Borderline 6.2
Abnormal 89.7
Total 100
From 117 respondents, total score of all aspects
measured namely emotional symptoms, behaviour
changes; peer relation, hyperactivity and prosocial
behaviour, 89.7% of the children with thalassemia in
Aceh is in abnormal category.
4 DISCUSSION
Emotions are responses or reactions of individuals to
stimuli, feelings and desires both positive and
negative. The cognitive theory view states that
emotions are more determined by the results of
individual interpretations of an event, and then
emerge changes internally in the body. Such
changes, for example, changes in facial expression,
tears out, and reddened eyes (Notoadmodjo, 2013).
The results of the study found that many
children had restless responses, fast breathing and
banging during blood transfusions. This is in line
with the research conducted by Putri, Mardhiyah &
Widianti (2015) who said that the results of the
response most frequently indicated by patients with
thalassemia at the time of transfusion took place
were that almost all of them showed a response
requesting significant emotional support in people
(84%).
Emotional and Behavioral Aspects of Children with Thalassemia in Banda Aceh, Indonesia
257

This is also related to research by Mazzona et
al. (2009), which says that thalassemia children tend
to experience high emotional temperament and poor
socialization. Researchers argue that emotional
symptoms in thalassemia children do tend to be
more emotional, as evidenced by research showing
an abnormal category of 74.4%, because sufferers
feel different from others, and there are still people
who think thalassemia is an infectious disease.
Based on table 3 it was found that behaviour
problems in children with thalassemia in Aceh are in
an abnormal category (76.9%). It is on-going
opposing behaviour without serious violations of
social norms or the rights of others. This behaviour
problem is a difficult problem often shown by
children such as hitting, fighting, mocking, refusing
to obey other people's requests (Istiqomah, 2017).
According to Rescorla et al. (2007) as cited in
Halimah, Allendekania, & Fajar T W (2016), the
next behaviour change that occurs is the problem of
decreasing attention. The risk of this problem is
influenced by gender, ethnicity, and mother's
education, adolescents with male sex increase the
risk of decreasing attention.
The results of the study found that many children
had behavioral changes starting from facing down
when the researcher invites to speak, and looks very
nervous. This is in line with the research of Riyana,
& Riza (2017) which says that thalassemia children
experience behavioral disorders as much as 73.3%.
Another study by Halimah, Allendekania, &
Waluyanti (2016) says that adolescent boys with
thalassemia have a higher risk of experiencing
behavioral problems such as anxiety problems,
social problems, and problems with less attention.
Although, it does not rule out that behavioral
problems could also occur in adolescent girls. Other
factors that increase the risk of behavioral changes
are the ethnicity, multi transfusion, maternal
education, and the involvement of next of kin and
relatives.
Based on the table 3, peer relationships in
thalassemia children is in the abnormal category
(59.0%). Children are less able to socialize with
their peers both at home and at school. The difficulty
of children in socializing often makes children less
accepted by their peers. This could limit the children
in interacting actively within their peers (Istiqomah,
2017). The results of the study found that many
thalassemia children have poor relationships with
their surroundings or peers. This is inherent with the
research of Maghfiroh et al. (2014), who said that
almost half of thalassemia children had low feelings
of being accepted in a friendship environment. Thus,
self-esteem is obtained from one self and social
interaction with peers. Individuals will feel high
self-esteem if they often experience success.
However, there are influencing factors such as
parents and peers that greatly affect the development
of self-esteem. If children have good peers, they
could increase their self-esteem.
Researchers argue that the social environment
has a relationship with peers. Therefore, the
difficulty of socializing often makes children less
accepted by their peers. This study showed an
abnormal category of 59% for peer relation aspect of
the children with thalassemia. The most important
thing about peer groups is to provide sources of
information and comparisons about the world
outside the family, peer interactions that have their
peer to play a special role in socio emotional
development.
Researchers argue that many children tend to be
more silent and unwilling to play; this is evidenced
by the results of the study showing 84.6% abnormal
categories in hyperactivity disorder. Although
thalassemia children are not allowed to overact,
nurses should provide counselling about child
development, starting from motoric training and
playing according to their age, but within limits they
do not force children to play excessively. The
researcher found that many thalassemia children
who are not able to move much and prefer to be
quiet, if they play only briefly but not too much
because the child is easily weakened. This is in line
with the research of Fetriyah, et. Al (2016), which
explains that most mothers regulate children's daily
activities. This is so that rest and activity remain
balanced, so that the mother gives direction to the
child to rest because if you do too much activity and
lack of rest will affect Haemoglobin levels in the
blood and can affect health in general.
The condition of children with thalassemia also
affected the relationship with their families. It could
potentially interfere with their welfare as individuals
and disrupt their functioning socially. The research
conducted by Indanah (2010), found that prosocial
behaviour plays an important role in psychosocial
support from family and peers. The family play a
role by helping to control the behaviour of children
facing physical and psychological changes. Indanah
said only 59% of respondents reported getting peer
support. Prosocial support and behaviour are mostly
indicated by the involvement of friends in social
activities that do not drain the child's energy.
Researchers argue that there are still many children
who lack of prosocial relationships with their peers.
This is evidenced by the results of this study
AINC 2018 - Aceh International Nursing Conference
258

showing an abnormal category of 69.2% in prosocial
behaviour, teachers and nurses should provide
examples of behaviour, guidance and motivation to
raise children's awareness of other people's feelings
as well as awarding prosocial behaviour in
thalassemia sufferers, situations and the hospital
affects children's opportunities to develop prosocial
behaviour.
The emotional and behavioral disorders in
children with thalassemia have complex
characteristics. These characters consist of moving a
lot, fighting behaviour and sometimes being alone
(Istiqomah, 2017). The researcher argues that the
high number of emotions and behaviour of
thalassemia sufferers that cause a decrease in self-
esteem. The result of this study showed an abnormal
category of 89.7% of emotional and behavioral
aspects of children with thalassemian in Aceh. The
description of emotional and behavioural aspects of
children with thalassemia is also influenced by the
demographic data of children and parents such as
gender, child's age and parental occupation. This is
in line with research by Aji et al. (2009) mentioned
that thalassemia suffer a poor quality of life because
of the changes in their psychosocial aspect.
Thalassemia children have a lifelong blood
transfusion where at these times medical treatment
usually requires non-cheap medical expenses. In
addition, long-term treatment can change all aspects
of life, not only for patients but also for their
families.
5 CONCLUSION
All the participated children with thalassemia,
measured with the ‘Strengths and Difficulties
Questionnaire’ (SDQ) showed that the emotional
and behavioral aspect of the children with
thalassemia is in abnormal category (89.7%).
Besides providing physical and medical cure to the
children who suffer from thalassemia, care givers
should also consider the emotional and behavioural
aspects of the children. Hence, it is suggested that
the medical workers keep educating the parents
regarding the emotional and behavioural aspect of
children with thalassemia.
ETHICS APPROVAL
This study holds ethical approval from Ethics
Committee of Faculty of Nursing, Syiah Kuala
University in Banda Aceh, Indonesia.
REFERENCES
Aji, D.N., Silman, C., Aryudi, C., Cynthia, Centauri,
Andalia, D., Astari, D., Pitaloka, D., Wawolumaya, C.,
Sekartini, R., Amalia, P. 2009. Faktor-Faktor yang
Berhubungan dengan Kualitas Hidup Pasien
Thalassemia Mayor di Pusat Thalassemia Departemen
Ilmu Kesehatan Anak RSCM. Sari Pediatri. 11(2): 85-
89.
Blanchard, L.T., Gurka, M.J & Blackman, J.A., 2006.
Emotional Developmental, and Behavioral Health of
American Children and Their Families: A Report
From the (2003) National Survey of Children’s
Health. Pediatrics, 117.
Fatmasyitah, V., Rahayu, SR.. 2014. Gambaran Penderita
Thalassemia Di Ruang Rawat Anak Rumah Sakit Cut
Meutia Aceh Utara Tahun 2012. Jurnal Edukasi dan
Sains Biologi. 3 (5).
Goodman, R., Ford, T., Simmons, H. & Gatward, R.,
2000. Using The Strength and Difficulity Questionaire
(SDQ) to Screen for Child Psychiatric Disorders in
Community Sampel. British journal of Psychiatric.
Halimah, Allenidekania, Waluyanti. 2016. Resiko remaja
thalasemia terhadap perubahan perilaku. Ners Jurnal
Keperawatan. 12 (1): 23 – 27.
Inandah. 2010. Analisisi faktor yang berhubungan dengan
Self Behavioural pada anak usia sekolah dengan
thalasemia mayor di RSU dr. Cipto Mangunkusumo,
Fakultas Ilmu Keperawatan Program Pasca Sarjana
Magister Keperawtaan, Universitas Indonesia. Jakarta
Istiqomah. 2017. Parameter Psikometri Alat Ukur
Strengths And Difficulties Questionnaire (SDQ).
Profil Kesehatan Indonesia Tahun 2012. 4 (2).
Kementerian Kesehatan Republik Indonesia.. Jakarta:
Kementerian Kesehatan RI, 2013
Mazzone. L, Battaglia. L, Francesca. A, Maria. A,
Domenico. M. 2009. Emotional Impact Thalassemia
Major Children Following Cognitive-Behavioral
Family Therapy and Quality Of Life of Caregiving
Mother. Clinical Practice and Epidemiology in Mental
Health. 5:5
Meila. SP, Mardhiyah. A, Efri. W. 2015, Gambaran
Respon anak usia sekolah dalam Menjalankan Proses
Trasfusi. Jurnal Keperawatan Padjajaran. 3 (2).
Notoadmodjo, Soekidjo. 2013. Ilmu Kesehatan
Masyarakat: Prinsip-Prinsip Dasar. Jakarta : PT.
Rineka Cipta
Nurhaeni, Y. 2015. Penerapan Analisis Transaksional
Dasar Untuk Memperbaiki Masalah Emosi dan
Perilaku Anak dan Remaja. Tesis Universitas Sebelas
Maret.
Emotional and Behavioral Aspects of Children with Thalassemia in Banda Aceh, Indonesia
259

Maghfiroh, R., Okatiranti., Sitorus E.R. 2014. Gambaran
Harga Diri Pasien Thalasemia Remaja Usia 14-21 di
Klinik Hemato-Onkologi RSUO dr. Hasan Sadikin
Bandung. Jurnal Keperawatan BSI. 11 (2).
Riyana. M., Riza. Muhammad. 2017. Penilaian gangguan
perilaku anak thalasemia mayor dengan menggunakan
the child behavior cheklist. Sari Pediatri. 19.(3).
TIF. 2008. Guidlines for the Clinical Management of
Thalassaemia 2nd Revised Edition. TIF No.9.
http://www.thalassaemia.org.cy/pdf_2nd _ revised_
edition_EN.pdf, 4-5.
Fetriyah, U.H., Elasari, Y., Hernanti, S.W. 2016.
Pengalaman Ibu Merawat Anak Usia Sekolah Dengan
Beta Thalasemia Mayor di RSUD Ulin Banjarmasin.
Dinamika Kesehatan. Volume. 7 (2)
Wiguna T. 2010. Masalah Kesehatan Emosional pada
remaja di Era Globalisasi dalam the 2 Adolescent
Health National Symposia, Current Challenges in
Management. Departemen Ilmu Kesehatan Anak
FKU1- RSCM : Jakarta.
Yusuf, S. 2009. Psikologi Perkembangan anak dan
Remaja, PT Remaja Rosdakarya, Bandung.
AINC 2018 - Aceh International Nursing Conference
260
