
The Correlation between Cultural Internalization and the Incidence
of Iron Deficiency Anemia on Pregnant Women
Darmawati
1,2
, Teuku Tahlil
3
, Hajjul Kamil
4
, Toungku Nizwan Siregar
5
, Williza Umami
2
1
Doctoral Program of Mathematic and Applied Sciences, Syiah Kuala University, Banda Aceh, Indonesia,
2
Department of Maternal Health Nursing, Faculty of Nursing, Syiah Kuala University, Banda Aceh, Indonesia
3
Department of Community Health Nursing, Faculty of Nursing, Syiah Kuala University, Banda Aceh, Indonesia
4
Department of NursingManagement, Faculty of Nursing, Syiah Kuala University, Banda Aceh, Indonesia
5
Faculty of Veterinary, Syiah Kuala University, Darussalam Banda Aceh, Indonesia
iza_williza@yahoo.com
Keywords: Belief, Culture, Iron deficiency anemia, Pregnancy, Taboo
Abstract: Unhealthy practices in community during pregnancy can cause complications during pregnancy, one of
them is iron deficiency anemia. Some pregnant women avoid some foods and adhering to certain beliefs.
This study aims to determine the relationship between cultural internalization with iron deficiency anemia
prevalence among pregnant women. This study used cross-sectional study design, involved 126 pregnant
women from working areas of a Community Health Center in the western part of Indonesia. The
participants were recruited using purposive sampling method. Data were collected by self-report
questionnaires developed by the researchers. Data analysis was done using chi-square test. Finding show
that there was a relationship between taboo in food and norm/belief with the incidence of iron deficiency
anemia among pregnant women. It is recommended that community health center should consider the use
of cultural practices in the community in their health education and information design and promote
positive cultural practices to reduce the negative impact on pregnant women..
1 INTRODUCTION
Maternal Mortality Rate (MMR) is one of important
indicators in upholding women's health status. MMR
was 305 per 100,000 live births in Indonesia and
was 30 per 100.000 live birth (23%) in Aceh
(Dinkes Aceh, 2016). In Aceh Besar, MMR was 88
per 100,000 live births in 2015 (Dinkes Aceh Besar,
2016). Factors affecting maternal mortality include a
history of illness, family planning history (named
keluarga berencana), history of complications and
anemia status (Jayanti, Basuki and Wibowo, 2016).
Anemia during pregnancy is a serious global
public health problem. It is estimated that more than
half of pregnant women have hemoglobin levels that
indicate anemia, which is <11.0 g / dL (Onyeneho et
al., 2016). The prevalence of anemic pregnant
women in Indonesia was 37.1% (Kemenkes RI,
2013). Iron deficiency anemia is one of the most
common disorders during pregnancy. Pregnant
women generally experience iron depletion. So that,
the iron in mother's body was given to the fetus. Iron
is needed for hemoglobin formation and blood
volume will increase due to changes in the pregnant
women's body and fetal blood supply. Iron
deficiency can cause disorders to fetal growth both
in body and brain cells, fetal death in the womb,
abortion, low birth weight and anemia in infants
(Kemenkes RI, 2014).
Iron deficiency anemia during pregnancy is
caused by nutritional deficiencies, one of them is
iron that can occurs due to inadequate intake of iron
and lack of availability of iron in food (Vir, 2011;
Silverberg, 2012). Other factors that cause iron
deficiency anemia was diet, socioeconomic,
environmental, health status, knowledge and culture
(Masrizal, 2007; Vir, 2011; Hartinah and Eswantii,
2017). The result of the study conducted by Kaphle,
Hancock, & Newman (2013) in Nepal found that
women in highland area considered tradition and
belief to be positive contributors to their safety and
survival and also their babies during pregnancy. The
behavior of the people in the village is based on their
belief in supernatural powers that directly oppose to
Darmawati, ., Tahlil, T., Kamil, H., Siregar, T. and Umami, W.
The Correlation between Cultural Internalization and the Incidence of Iron Deficiency Anemia on Pregnant Women.
DOI: 10.5220/0008396400002442
In Proceedings of the Aceh International Nursing Conference (AINC 2018), pages 199-204
ISBN: 978-989-758-413-8
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
199
medical views, where they will not abandon the
tradition of seeking medical care during pregnancy.
Acehnese culture has several traditions during
pregnancy. First, there was a tradition named Ba
Boh Kayee (bringing fruit) to pregnant women by
mother in-laws after enter a 3-month pregnancy
period. Second, Me Bu (tradition of carrying rice)
was done when pregnant women enter 7-8 months of
pregnancy and the tradition of abstaining from food
during pregnancy (Puspitawati and Batubara, 2015;
Samad, 2015). The study conducted by Puspitawati
& Batubara (2015) in Aceh Utara found that many
pregnant women were still abstaining from certain
types of food, such as not being able to eat pineapple
because it can cause miscarriages, should not eat sea
fish such as cuttlefish, octopus or other types of
strange fish, and forbidden to eat eggplant, jackfruit
and gummy vegetable. Based on this phenomenon,
researchers want to assess "The Relationship of
Cultural Internalization with the Incidence of Iron
Deficiency Anemia in Pregnant Women in Aceh
Besar".
2 METHODS
This research was a quantitative research with
descriptive correlative method, carried out with a
cross sectional study approach. This study used a
questionnaire developed by researchers based on
theoretical objectives consisting of 3 parts, which
included demographic data, taboo in food, and
norms/beliefs about eating food during pregnancy,
as well as the use of Hb meters to measure maternal
hemoglobin levels.
The study population were all pregnant women
who visited a selected Community Health Center,
between September 2017 and February 2018. The
sample of this study was 126 pregnant women who
recruited by non-probability sampling, using 3
inclusion criteria as follow: (1) Acehnese pregnant
women; (2) pregnant women who did not experience
blood disorders, and; (3) pregnant women in their
second and third trimesters.
Data collection was started by asking for
approval from the research place/community, the
visited the respondents and explained them the study
purpose and objectives. Next, the researchers asked
the respondent's approval by signing an informed
consent sheet. Then, the researchers distributed
questionnaires and measured the respondent's
hemoglobin. Data were analyzed using Chi-Square
test. This study was approved by the Ethical
Committee of Nursing Faculty, Syiah Kuala
University.
3 RESULTS
3.1. Characteristic of Respondents
The distribution of respondents based on their
demographic characteristics is shown in Table 1.
Table 1: Demographic Characteristics of pregnant women (N=126).
Characteristics F (%)
Age
Risk age (<20 and >35 years old) 27(21.4)
Not risk age (20-35 years old) 99(78.6)
Education
Low 8(6.3)
Middle 79(62.7)
High 39(31.0)
Job
Not Working 110(87.3)
Work 16(12.7)
Gestational Age
2
n
d
trimester 78(61.9)
3
r
d
trimester 48(38.1)
Number of Deliveries:
Primiparous 32(25.4)
Multiparous 94(74.6)
Lived with
Parents 64(50.8)
Husband 62(49.2)
AINC 2018 - Aceh International Nursing Conference
200
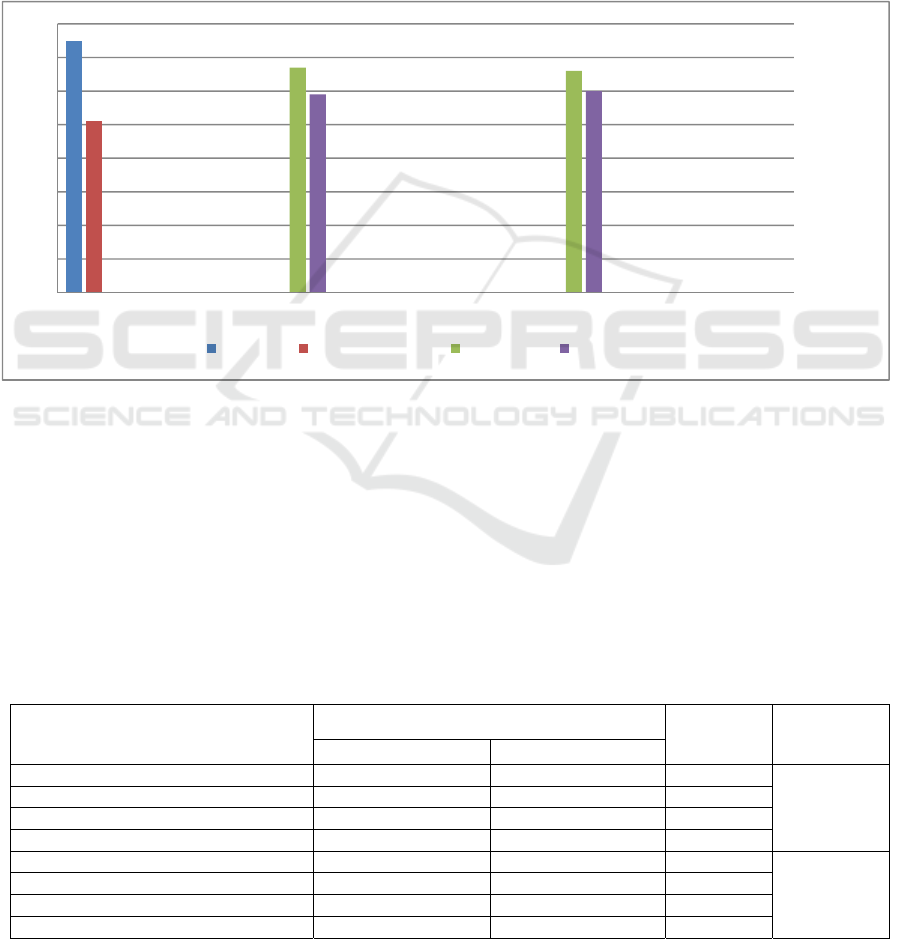
Table 1 shows that most of the respondents were in
not at risk age (20-35 years), half of the respondents
have last education in the middle category, two
thirds of respondents did not work, and the
respondent’s gestational age was mostly in the
second trimester category. The majority of
respondents were multiparous and half of the
respondents lived with their parents
3.2. Distribution of Food Taboos,
Norms/Beliefs and Iron Deficiency
The distribution of food taboos, norms/beliefs and
iron deficiency is shown on Graph 1. The incidence
of iron deficiency anemia in pregnant women was
59.5%; 53.2% of respondents supported taboos in
food; and 52.4% of respondents supported
norms/beliefs during pregnancy.
Graph 1. Distribution of Food Taboos, Norms/beliefs and Iron Deficiency Among Pregnant Women.
3.3. Relationship between Food Taboos,
Norms/Beliefs and Iron Deficiency
The proportion of anemia among pregnant women
who supported food taboos (68.7%) differed
significantly with respondents who did not support
(49.2%) food taboos in food (p-value = 0.04). The
proportion of anemia among pregnant who
supported the norms and beliefs (69.7%) differed
significantly with respondents who did not
supported the norms/beliefs (48.3) food taboos in
food (p-value = 0.024). It can be interpreted that
there was a statistical relationship between food and
norms/ beliefs with the
incidence of iron deficiency
anemia. The Relationship between food taboos,
norms/belief and the Incidence of Iron Deficiency
Anemia in pregnant women is described in Table 2
as follows.
Table 2: The Relationship of Food Taboos and the Incidence of Iron Deficiency Anemia in Pregnant Women.
Sub-variables
Iron Deficiency Anemia
Total
p-value
Anemia f (%) Not Anemia f (%)
Food Taboos
0.041
Supported 46(68.7) 21(31.3) 67
Not Supported 29(49.2 30(50.8) 59
Total 75(59.5) 51(38.5) 126
Norms/beliefs
0.024
Supported 46(69.7) 20(30.3) 66
Not Supported 29(48.3) 31(51.7) 60
Total 75(59.5) 51(40.5) 126
75
51
67
66
59
60
0
10
20
30
40
50
60
70
80
Iron Deficiency Anemia Food Taboos Norms/Beliefs of Pregnant Women
Anemia Did not Anemia Supported Not Supported
The Correlation between Cultural Internalization and the Incidence of Iron Deficiency Anemia on Pregnant Women
201

4 DISCUSSIONS
The results of this study were supported by the
research conducted by Martini dan Haryanti (2015)
and found that there was an effect of food taboos on
the incidence of anemia (p-value = 0.047). There
are still many cultural beliefs in the society that
potentially increase pregnancy complications.
Pregnancy complications had an impact on maternal
morbidity and mortality include anemia in
pregnancy.
Culture gives different roles and values for food.
There are certain foods that are considered taboo or
should not be consumed during pregnancy.
Community beliefs formed because of the meaning
or reason contained in every word of their parents
(Humaeni, 2015; Mubarak, 2011).
One factor that contributes to problems during
pregnancy in rural areas was food taboos during
pregnancy. In several studies, it seen that pregnant
women in various country of the world were forced
not to consume nutritious food as part of their
traditional eating habits (Ugwa, 2016).
Based on the results by respondents' answers, it
is known that pregnant women in this study were
still not consume shrimp (10.3%), did not consume
fish (21.4%), did not consume goat meat (28.6%),
did not consume vegetables (31.0%), did not
consume fruits (34.1%), did not consume iron
tablets (27.8%), and there were still many
restrictions on pregnant women in the surveyed
community.
This study result was similar with the result
conducted by Sholihah & Sartika (2014) in Suku
Tengger. From the interviews conducted on
traditional birth practitioners (named dukun
beranak), families and pregnant women, it is known
that bananas, pineapple, fish, cabbage, and others
are foods that often abstained during pregnancy.
Research conducted by Nurrachmawati &
Anggraeni (2010) in East Borneo found that
pregnant women were still prohibited to eat salty
fish, squid, shrimp, pineapple, durian and others.
The same results are also obtained by Zerfu, Umeta,
& Baye (2016)
in Arsi found that pregnant women
also abstinence from foods such as spinach,
cabbage, kale, meat, chicken and others. Research
conducted by Eram, Tamanna, & Humaira (2016)
mentioned that out of a total of 100 studied women
in India, 78 pregnant women avoided papaya, 43
avoided fish, 33 avoided badi foods (which caused
flatulence), 27 avoided citrus foods, and 8 avoided
peanuts and tea or brinjal.
Food abstinence by pregnant women in this
study is contradictory to the concept mentioned by
Gluckman, Hanson, Seng, & Bardsley (2015);
Almatsier (2001). This study found that the foods
they avoided were rich of such as fish, vegetables,
fruits, meat, chicken, ducks and others. The iron is
used to formed hemoglobin in red blood cells that
acts as an oxygen carrier from the lungs to the
tissues. In the condition of iron deficiency, the
hemoglobin in the body will also decrease. This
condition causes iron deficiency anemia in pregnant
women.
Researchers assumed that food taboos during
pregnancy occur due to a lack of information from
health workers regarding the importance of nutrition
during pregnancy, so that many pregnant women
avoided some foods which were needed during
pregnancy, especially iron. This research area still
has cultures and beliefs trusted by local community,
especially regarding food taboos that trusted by
their parents. The pregnant women still affected to
follow that beliefs because they were afraid to have
several dangerous condition for themselves or their
babies.
This study result was supported by a study
conducted by Zerfu et al., (2016)
in Arsi. It is
known that there were still many pregnant women
who believe that body weight should not be
increased during pregnancy; milk and eggs should
not be consumed because it can caused large babies.
They also belief that pregnant women should not
allowed to consume green leaf vegetables because it
was dangerous for themselves and their fetuses.
Results of research conducted by Zepro (2015)
found that from 49.8% of total respondents avoided
one or more foods during pregnancy. Honey and
milk/yogurt are usually avoided because they
believe it can make the baby were fat so it would be
difficult for giving birth, can cause abortion and
fetal abnormalities. More than 82.4% of
respondents believe that reducing food intake
during pregnancy was very important.
The recapitulation of respondents’ answers in
previous study found that pregnant women in the
surveyed area were still believed things that were
contrary to health during pregnancy. It was found
that 42.9% believed that consuming too much
food caused a large baby. Pregnancy is the most
important stage and requires adequate nutrition.
During pregnancy, the mother needs extra calories
and essential nutrients every day to support fetal
growth. Incorrect belief in avoidance of food can
drain important body nutrients that will affect the
mother and fetus growth (Ugwa, 2016).
AINC 2018 - Aceh International Nursing Conference
202

From total 26.2% of respondents believed that
consuming iron tablets can caused large babies. Iron
(Fe) is an essential mineral that is important in the
formation of hemoglobin, myoglobin and collagen
and has a good function for fetal growth and
development (Kemenkes RI, 2016).Without iron
therapy, pregnant women who consume adequate
nutrients would be experience iron deficiency
during pregnancy. Diet alone cannot replace iron
loss during pregnancy. Oral iron should be given for
at least 6 months to correct anemia and to replenish
iron reserves (Bobak, Lowdermilk and Jensen,
2005; Silverberg, 2012).
There was 34.1% respondents believed that eggs
can make a big baby, 47.6% trusted milk can cause
large babies and difficult to give birth. Milk and
eggs contained protein which was one of the factors
that can facilitate iron absorption (Adriani and
Wirjatmadi, 2012), 69.8% respondents believed that
pineapple can cause miscarriages. Pineapple is one
of the fruits that contain vitamin C. Vitamin C was
good to be consumed because iron from plants
cannot be absorbed effectively without it. So, the
pregnant women need to consume vitamin C to
helath iron absorption (Mariana, Wulandari and
Padila, 2018). There was 30.2% respondents
believed that consuming goat meat can cause
cramps in the stomach or miscarriage. Goat meat is
one of the foods that contain heme iron. Heme iron
has a small iron content, but it would be well
absorbed by the body (Gluckman, Hanson, Seng, &
Bardsley, 2015 ; Almatsier, 2001).
The beliefs held by pregnant women in this
study were still contradicted from the health sector,
the results above was the evidenced. Actually, what
they believe is about the nutrients needed during
pregnancy. Energy metabolism during pregnancy is
increases, therefore they need energy and other
nutritional that also increased for fetal growth and
development and the changes of the composition
and metabolism of mother's body. Basically,
pregnant women need all the additional nutrients,
but what often becomes deficiency was iron
(Sukarni & Margareth, 2013).
The beliefs about pregnancy can also change the
mother's eating habits so that nutritional intake is
not in balance with the needs, this can cause the
metabolism of hemoglobin formation is inhibited
and the body's need for nutrients cannot be fulfilled,
such as iron, vitamin C, protein and others. This
condition can cause iron deficiency anemia during
pregnancy (Widyawati et al., 2015; Mariana,
Wulandari and Padila, 2018).
Pregnant women in study who have different
beliefs from the medical concepts majority lived
with their parents. This makes the researchers
assumed that pregnant women who have these
beliefs were obtained from their parents.
Researchers also assumed that pregnant women feel
anxious and fear that something will happen to their
pregnancy if they did not obey what the other
people or who are more experienced about
pregnancy said. It caused the pregnant women tend
to obey or trust everything related to pregnancy,
whether that was true or contrary to health concepts.
Pregnant women in this study mostly in the middle
school level category. This condition can caused the
level of trust held by pregnant women was high,
because pregnant women tend to take information
without thinking about the effects of that good or
bad information.
This study also has limitation. It is very difficult
to find the respondent address because the selected
Community Health Center working area has a large
area, it consists of 47 villages and there are several
villages that are difficult to reach, so this study
implemented in a long time period.
5 CONCLUSION
Based on the results and discussion in this study, it
can be concluded that food taboos and
norms/beliefs were associated with the incidence of
iron deficiency anemia in pregnant women. It is
recommended that the community health center
providers must consider the cultural practices that
apply in the community for designing health
education and information. They should consider to
internalize positive cultural practices for health life
so it can reduce the negative impact on pregnant
women.
ACKNOWLEDGEMENTS
The authors thank the pregnant women for their
participation and enthusiasm, also for the health
workers and other personnel from Kuta Baro
Community Health Center and Aceh Besar Health
Office for the permission and support provided for
this research process.
The Correlation between Cultural Internalization and the Incidence of Iron Deficiency Anemia on Pregnant Women
203

REFERENCES
Adriani, M. and Wirjatmadi, B. 2012. Pengantar Gizi
Masyarakat. Jakarta: Kencana.
Zepro, B.N. 2015. ‘Food Taboos and Misconceptions
Among Pregnant Women of Shashemene District,
Ethiopia, 2012’, Science Journal of Public Health,
3(3): 410.
Bobak, Lowdermilk and Jensen. 2005. Buku Ajar
Keperawatan Maternitas Edisi 4. Jakarta: EGC.
Dinkes Aceh. 2016. Kesehatan Provinsi Aceh 2015.
Aceh: Dinkes Aceh.
Dinkes Aceh Besar. 2016. Profil Kesehatan Kabupaten
Aceh Besar tahun 2015. Aceh Besar: Dinkes Aceh
Besar.
Eram, U., Tamanna, & Humaira. 2016. ‘Taboos and
misconceptions associated with pregnancy among
rural women in Aligarh’, International Journal of
Information Research and Review, 3: 3407–3409.
Gluckman, P. et al. 2015. Nutrition & Lifestyle for
Pregnancy & Breastfeeding. United Kingdom: Oxford
University Press.
Hartinah, D. and Eswantii, N. 2017. ‘Hubungan antara
kesiapan kehamilan dengan Anemia Pada Ibu Hamil di
wilayah kerja Puskesmas Jadi Kabupaten Kusus’, The
5
th
Urecol Proceeding, 496–502.
Humaeni, A. 2015. ‘Tabu Perempuan Dalam Budaya
Masyarakat Banten’, Humaniora, 27 (2).
Jayanti, K. D., Basuki, H. and Wibowo, A. 2016. ‘Faktor
yang mempengaruhi kematian ibu (Studi Kasus di
Kota Surabaya)’, Jurnal Wiyata, 3 (1): 46–53.
Kaphle, S., Hancock, H. and Newman, L. A. 2013.
‘Childbirth traditions and cultural perceptions of safety
in Nepal: Critical spaces to ensure the survival of
mothers and newborns in remote mountain villages’,
Midwifery, 29 (10): 1173–1181.
Kemenkes RI. 2013. Riset kesehatan dasar 2013. Jakarta:
Badan Penelitian dan Pengembangan Kementerian
Kesehatan RI.
Kemenkes RI. 2014. Buku Ajar Kesehatan Ibu dan Anak.
Jakarta: Pusdiknakes.
Kemenkes RI. 2016. Profil kesehatan Indonesia 2015.
Jakarta: Kementerian Kesehatan Republik Indonesia.
Mariana, D., Wulandari, D. and Padila. 2018. ‘Hubungan
pola makan dengan kejadian anemia pada ibu hamil di
wilayah kerja Puskesmas’, 1 (2):108–122.
Masrizal. 2007. ‘Anemia defisiensi besi’, Jurnal
Kesehatan Masyarakat, II (1):140–145.
Nurrachmawati, A. and Anggraeni, I. 2010. ‘Tradisi
kepercayaan masyarakat pesisir mengenai kesehatan
ibu di Desa Tanjung Limau Muara Badak Kalimantan
Timur tahun 2008’, Kesehatan Reproduksi, 1(1)42–50.
Onyeneho, N. G. et al. 2016. ‘Factors associated with
compliance to recommended micronutrients uptake for
prevention of anemia during pregnancy in urban, peri-
urban, and rural communities in Southeast Nigeria’,
Journal of Health, Population, and Nutrition, 35 (1):
35.
Puspitawati and Batubara, R. R. 2015. ‘Pertolongan
persalinan ma’blien pada masyarakat Desa Sawang
Kecamatan Samudera Aceh Utara’, Antropologi Sosial
dan Budaya, 1 (2): 124–132.
Samad, S. A. A. 2015. ‘Pengaruh agama dalam tradisi
mendidik anak di Aceh : Telaah terhadap masa
sebelum dan pasca kelahiran’, Gender Equality :
Internasional Journal of Child and Gender Studies. 1
(1): 111–123.
Sholihah, L. A. and Sartika, R. A. D. 2014. ‘Makanan
Tabu pada Ibu Hamil Suku Tengger’, Jurnal
Kesehatan Masyarakat Nasional, 8 (7): 319–324.
Silverberg, D. S. 2012.Anemia. Croatia: InTech.
Sukarni, I. and Margaret, Z. 2013. Kehamilan, Persalinan
dan Nifas dilengkapi dengan Patologi. Yogyakarta:
Nuha Medika.
Ugwa, E. 2016. ‘Nutritional practices and taboos among
pregnant women attending antenatal care at general
hospital in Kano, Northwest Nigeria’, Ann Med Health
Sci Res, 6 (2): 109–114.
Vir, S. C. 2011.Public Health Nutrition in Developing
Countries. New Delhi: Woodhead Publishing India
Pvt. Ltd.
Widyawati, W. et al. 2015. ‘A qualitative study on
barriers in the prevention of anaemia during pregnancy
in public health centres: Perceptions of Indonesian
nurse-midwives’, BMC Pregnancy and Childbirth, 15
(1): 1–8.
Zerfu, T. A., Umeta, M. and Baye, K. 2016. ‘Dietary
habits, food taboos, and perceptions towards weight
gain during pregnancy in Arsi, rural central Ethiopia:
a qualitative cross-sectional study’, Journal of Health,
Population, and Nutrition, 35 (1): 22.
AINC 2018 - Aceh International Nursing Conference
204
