
Comparison of Height, Body Mass Index, and Nutrient Adequacy
Ratio of the Nutritional Status of School-Age Children in Coastal
and Non-Coastal Areas in Aceh
Muhammad Iqbal S
1
, Kartini Hasballah
2
, Teuku Tahlil
3
1
Master of NursingScience, Faculty of Nursing, Syiah Kuala University, Banda Aceh
2
Pharmacology Departement, Faculty of Medicine, Syiah Kuala University, Banda Aceh
3
Department of Community Health Nursing, Faculty of Nursing, Syiah Kuala University, Banda Aceh
Keywords: School-agechildren, Nutritional status, Anthropometry, Nutrient adequacy ratio
Abstract: Nutrition is one of the most common issues in several developing countries including Indonesia, which is
currently facing malnutrition. Indonesian’s coastal and non-coastal areas have different environments which
lead to differences in commodities and types of food affecting children's nutrition. This study aimed to
assess the nutritional status of school-age children based on height, bodymassindex, and nutrient adequacy
ratio in coastal and non-coastal areas in Aceh. The study used a descriptive comparative research design,
with a population of 226 children. A representative sample of 98 school-age children (49 from each area)
was selected by using the simple random sampling technique. The instrument of data collection was the
Food Recall 24 Hour. The methods employed were interview, and weight and height measurement forms.
The data were analyzed by using independent sample t-test. The results indicated that there were no
differences either in nutritional status of school-age children incoastal and non-coastal areas (ρ = .156), in
height (ρ = .155), in body mass index (ρ = .064), or in nutrient adequacy ratio (ρ = .188). It is suggested that
the Health Office pay more attention to and evaluate nutrition programs of school-age children at the
puskesmas level to improve the promotion of healthy living community movement in coastal and non-
coastal areas so that they are more aware of good nutrition, and also to provide training in the use of
nutritious food sources within the areas.
1 INTRODUCTION
Nutrition is one of the essential factors determining
the level of health and balance of one’s physical and
mental development. In the case of a child's growth
and development, nutritional adequacy is a crucial
issue that parents should pay close attention to
(Suryanto & Restuastuti, 2016). Nutritional
problems in elementary school children are still
relatively high. The World Health Organization
(2014) reported that in 2013, 17% (98 million) of
children in developing countries experienced
malnutrition, with the highest prevalence of 35.7%
was stunting in the Asian region. Indonesia, in fact,
is included in the five categories in the world in
terms of the number of stunting in children. One in
three (37.2%) Indonesian children, approximately,
suffered from stunting (World Food Programme,
2014). The Basic Health Research (2013) found that
the prevalence of stunting in children aged 5-12
years was 30.7%, malnutrition based on body mass
index (BMI) was 11.2%, and obesity categorized as
high with an incidence of 18.8%. In the case of
malnutrition, Aceh Province, Indonesia, ranked
seventh with a prevalence of 26.3% (Basic Health
Research, 2013).
The nutritional problems occuring in the
community are closely related to environmental
aspects as they have the largest impact on the level
of public health, such as differences in the types of
commodities, food produced and food available in
the environment (Umi, 2005). Malnutrition can be
triggered by several factors including food intake,
patterns of health care, and parenting (Burchi, 2012;
Meriska, 2014).
Based on the geographical condition, people in
coastal areas are very likely to consume more animal
protein sources from the sea such as fish and clams.
In contrast, most rural people tend to consume more
Iqbal S, M., Hasballah, K. and Tahlil, T.
Comparison of Height, Body Mass Index, and Nutrient Adequacy Ratio of the Nutr itional Status of School-Age Children in Coastal and Non-Coastal Areas in Aceh.
DOI: 10.5220/0008394400002442
In Proceedings of the Aceh International Nursing Conference (AINC 2018), pages 49-57
ISBN: 978-989-758-413-8
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
49

carbohydrate and vegetable protein sources
(Hamidah, Sartono, & Kusuma, 2017). A study by
Umi (2005) revealed that the level of energy intake
of children in coastal areas and mountainous areas
was significantly different (p = .05); the intake was
higher in coastal areas than in mountainous areas.
The level of energy intake of children in coastal
areas was quite fulfilled (77.09%) while that in
mountainous areas was fairly sufficient (51.43%).
On the other hand, the level of protein intake of
children in coastal areas and mountainous areas was
significantly different, in which the intake was better
in coastal areas. Further, Hamidah’s study (2016) on
the differences in consumption patterns of protein-
based foods in coastal areas, low landsand highlands
concluded that there were differences in terms of
diversity, frequency, and amount of food consumed
by families within the three areas.
Children who experience malnutritionare highly
likely to grow small, thin, and short. Poor nutrition
will have an adverse impact on the children’s
cognitive ability or intelligence, and decline the
productivity of the children's performance in
everyday life (Indonesian Ministry of Health, 2014).
There should be efforts taken to increase the
availability of quality food to help improve the
children's nutrition (Almatsier, 2009).
Pidie is one of the districts in the Aceh Province,
ranked second after East Aceh for people with
malnutrition. The number of children suffering from
malnutrition reached 32 cases and the number of
malnourished patients reached 488 people (Bakri,
2015). Data on Pidie District Nutrition Status
Monitoring Report (2014) showed that the
prevalence of short stature children was 30.8% and
very short stature of 8.35%, within the work area of
Muara Tiga Puskesmas (community health center).
There was also an increase in the prevalence of
stunting among infants from 2013 to 2014 (Ariyanti,
2015).
Nutritional deficiencies in school-age children
will result in a long-term effect until adulthood, such
as growth failure, if parents neglect the patterns of
feeding with insufficient nutritional values.
Therefore, the District Health Office should concern
more on the nutritional problems of school-age
children in order for the community to have more
awareness in evaluating the nutrition of these
children.
The preliminary study has shown that there were
children aged 6-12 years with low body weight in
the coastal areas in Pidie District. To make ends
meet, the local people have been working as
fishermen. 85% of the children stated that they
consumed rice and fish obtained from fishing daily,
often consumed processed salted fish, rarely ate
fruits, and only had common side dishes brought by
their parents. Every week the children would be
served with vegetables such as kale, corn, potatoes,
spinach, mustard greens, and eggplants, and during
their parents fishing periods, they would prepare
their own meals. In non-coastal areas in Pidie
District, on the contrary, the people’s livelihoods
included paddy farming, livestock farming, and
vegetable gardening as these areas are far from
urban or shopping centers. There were also children
aged 6-12 years who were underweight. The results
of interviews showed that out of 10 children, 80% of
of them mentioned that every day they would
consume rice and processed foods from their parents'
gardening, including side dishes (i.e., vegetable
beans, beans, eggplants, melinjo leaves, melinjo
fruit, sweet potato leaves, bananas, kale, mustard
greens, spinach, gambas fruit, pumpkin, lime leaves,
celery, reed starfruit, fern leaves, papaya leaves,
mustard leaves, coconuts, and peanut shells), and
fruit (i.e., papaya, cucumber, banana, mango, guava,
and watermelon).
From the aforementioned findings, it can be
further stated that there is a difference in the daily
consumption of children either in coastal or non-
coastal areas. As such, community nurses need to
make efforts to improve community nutrition
through a socio-cultural approach towards the eating
culture of coastal and non-coastal communities, one
of which is by organizing the Family Nutrition
Awareness Program (KADARZI). The approach that
may be taken is by teaching families on the
nutritional values of food (i.e., contents of proteins,
calories, and carbohydrates), and by teaching
families in the preparation of healthy and balanced
diets from any potential food within the coastal and
non-coastal areas. With the involvement of parents,
Puskesmas, cadres Posyandu, cadres of nutrition
health, and PKK (Family Welfare Empowerment)
women, there should be a significant impact in
achieving good nutrition for children.
The differences in food commodities and types
have made it obvious that there is an influence of the
quality or quantity of nutrition in food dishes
consumed by children, especially on children's
physical growth. Therefore, the study sought to
assess the nutritional status of school-age children
incoastal and non-coastal areas, by comparing their
height, body mass index (BMI), and nutrient
adequacy ratio.
AINC 2018 - Aceh International Nursing Conference
50

2 METHODS
This study employed a comparative research design
intending to obtain differences in the nutritional
status of school-age children in coastal and non-
coastal areas. Population in this study were 226
children aged 6-12 years living in one village, Sigli
Sub-district and one village, Mutiara Sub-district, in
Pidie District, Aceh Province. A representative
sample of 98 children, with 49 children selected in
each village, was taken by using the simple random
sampling (lottery) technique.
The measuring instruments used included a Food
Recall 24 Hour form, a height gauge of Gea Medical
Brand microtoise with a capacity of 200 cm, and a
weight gauge with a tread needle scale of Gea
Medical Brand with a capacity of 120 kg. The scale
has been calibrated in the Metrology UPTD
(regional technical implementation unit) of Banda
Aceh City.
Data collection was conducted from July 16 to
23, 2018, after receiving permission for research at
both sites. The selected respondents were given an
explanation of the procedural research and also the
informed consent to be signed by both the
respondents and their families/guardians prior to
data collection. Data on height and BMI were
obtained from direct measurements on the
respondents, which then calculated by using the Z-
score of the 2005 WHO Anthroplus application.
Meanwhile, the nutrient adequacy ratios was gained
from the interviews with Food Recall 24 Hour, and
were later measured for energy and protein adequacy
ratios. The calculation of the nutrient adequacy
ratios were manually referred to the Food
Composition List to consult for the contents of the
nutritional values and weights of food in each food
consumed by children. Appropriate univariate and
bivariate analyses (independent sample t-test) were
conducted in the data analysis.
3 FINDINGS
3.1 Demographic Characteristics
The characteristics of the respondents are described
in table 1. The average age of primary school
children in coastal areas was 9 years and 9 months
old while that in non-coastal areas was 8 years and 8
months old. However, in terms of birth weight, the
respondents of both areas had a relatively similar
weight of 3kg. The average respondents’ education
in coastal areas was Grade 4 while that in non-
coastal areas was Grade 2. Further, both coastal and
non-coastal areas were predominantly females. For
the past three years, the children in coastal and non-
coastal areas were mosly had a history of fever. In
terms of parents’ livelihoods, in coastal areas, the
fathers have been working as fishermen and the
mothers as housewives, whereas in non-coastal
areas, both fathers and mothers were farmers. The
parents living in coastal and non-coastal areas had
generally primary school educational background,
with the average family income under the Aceh
government’s minimum wage (Rp. 2,700,000).
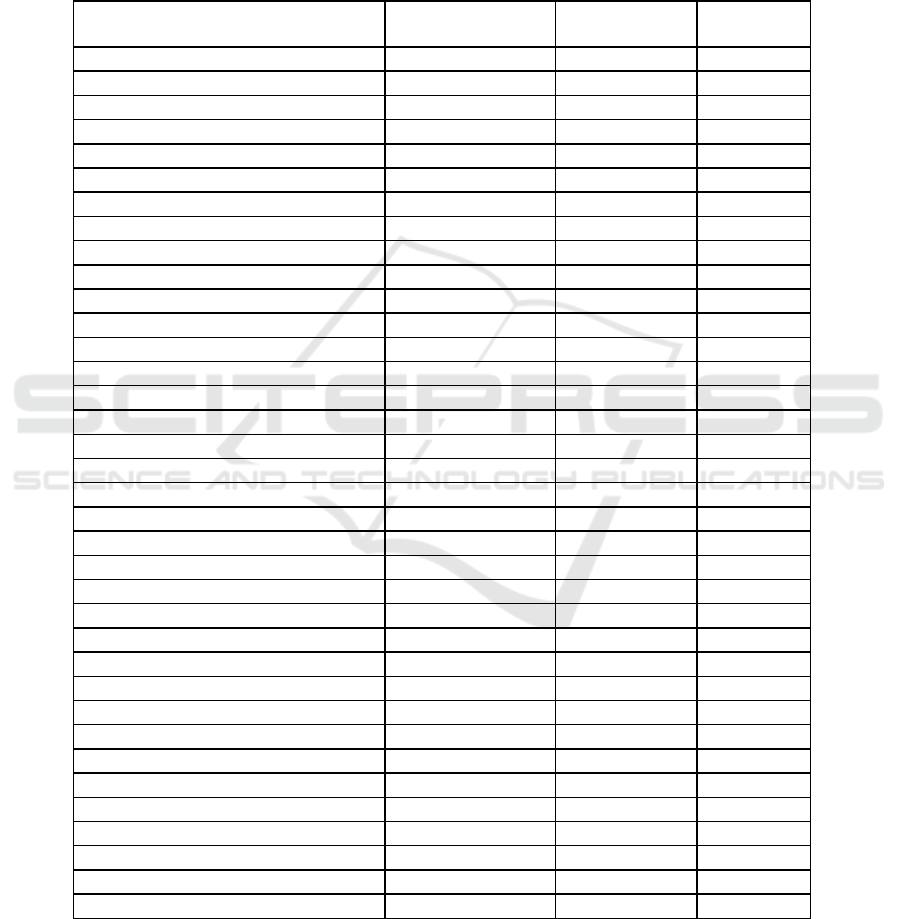
3.2 Nutritional Status of Children in
Coastal and Non-Coastal Areas
The nutritional status of the respondents in coastal
and non-coastal areas is depicted in Table 2. The
table shows that the nutritional status of school-age
children in these two areas was mostly categorized
as malnourished, in which 25 (51%) respondents in
coastal areas had an average nutritional value of 176
(SD 52.33) while in non-coastal areas, 28 (57.1%)
respondents had an average nutrition of 159 (SD
62.95).
3.3 Height-based Nutritional Status
Therespondents’nutritional status based on height in
coastal and non-coastal areas is shown in Table 2.
Overall, the nutritional status of school-age children
in both areas was generally in the normal stature
category, where in 40 (81.6%) respondents in coastal
areas had an average z-score of -1.24 (SD 1.014) and
31 (63.3%) respondents in non-coastal areas had an
average z-score of 1.50 (SD 1.091).
3.4 Body Mass Index of Children in
Coastal and Non-Coastal Areas
Table 2 provides BMI of the respondents in coastal
and non-coastal areas, in which the BMI was mostly
normal in both areas, with 43 (87.8%) respondents
in coastal areas had an average z-score of -.37 (SD
1.183) and 30 (61.2%) respondents in non-coastal
areas of -.64 (SD 1.908).
3.5 Nutritient Adequacy Ratio of Children
in Coastal and Non-Coastal Areas
Figures on the nutrient adequacy ratios of the
respondents in coastal and non-coastal areas are
Comparison of Height, Body Mass Index, and Nutrient Adequacy Ratio of the Nutritional Status of School-Age Children in Coastal and
Non-Coastal Areas in Aceh
51
reported in Table 2. In general, the nutritional status
of school-age children based on the nutrient
adequacy ratios was low in both areas, with 25
(51%) respondents had an average value of 177 (SD
52.18) in coastal areas and 27 (55.1%) respondents
had an average of 162 (SD 64.26) in non-coastal
areas.
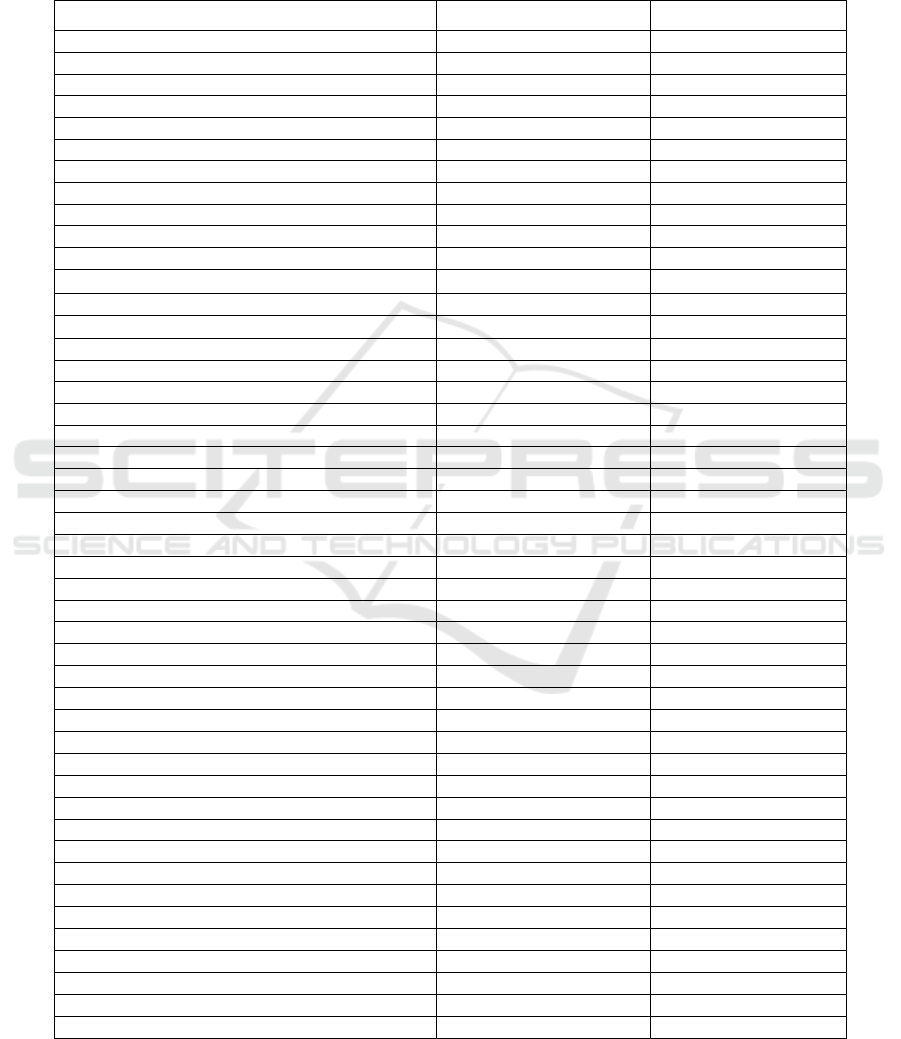
Table 1. Demographic characteristics of school-age children incoastal and non-coastal areas (n=98).
Demography
Coastal area (n=49)
Non-coastal area (n=49)
Children
Age, mean (SD)
9.11 (1.79)
8.60 (1.70)
Birth Weight, mean (SD)
3:00 (.48)
3:00 (.75)
Sex, f (%)
Boys
23 (47)
21 (43)
Girls
26 (53)
28 (57)
Current Education, f (%)
Grade 1 of elementary school
7 (14.3)
6 (12.2)
Grade 2 of elementary school
6 (12.2)
13 (26.5)
Grade 3 of elementary school
6 (12.2)
10 (20.4)
Grade 4 of elementary school
11 (22.4)
2 (4.1)
Grade 5 of elementary school
7 (14.3)
9 (18.4)
Grade 6 of elementary school
12 (24.5)
9 (18.4)
History of Diseases, f (%)
Fever
46 (94)
46 (94)
Itchiness
1 (2)
0(0)
Urinary tract infection
1 (2)
0(0)
Polyp
1 (2)
0(0)
Down syndrome
0(0)
1 (2)
Asthma
0(0)
1 (2)
Fracture
0(0)
1 (2)
Father's occupation, f (%)
Fisherman
33 (67)
0(0)
Farmer
0(0)
35 (72)
Trader
9 (19)
2 (4)
Civil Servant
3 (6)
1 (2)
Entrepreneur
4 (8)
11 (22)
Mother's Occupation, f (%)
Housewife
35 (72)
17 (35)
Farmer
0(0)
28 (57)
Weaver
6 (12)
0(0)
Trader
6 (12)
0(0)
Labor
2 (4)
0(0)
Entrepreneur
0(0)
3 (6)
Teacher
0(0)
1 (2)
Father's Education, f (%)
Primary
37 (76)
39 (80)
Secondary
11 (22)
10 (20)
Higher Education
1 (2)
Mother’s Education, f (%)
Primary
33 (67)
33 (67)
Secondary
14 (29)
14 (29)
Higher Education
2 (4)
2 (4)
Parent Income, f (%)
Under Aceh minimum rate
48 (98)
49 (100)
Above Aceh minimum rate
1 (2)
0(0)
AINC 2018 - Aceh International Nursing Conference
52
3.6 Comparison of the Nutritional Status
of School-Age Children inCoastal and
Non-Coastal Areas
Table 3 summarizes the comparison of the
nutritional status of school-age children in coastal
and non-coastal areas. The table shows that there
were no significant differences between the
nutritional status (p-value = .156), between height
(p-value = .155), between BMI (p-value = .064), and
between nutrient adequacy ratios (p-value = .188) of
school-age children in both areas.
Table 2. Nutritional status, height, body mass index, nutrient adequacy ratio of school-age children in coastal and non-
coastal areas (n=98).
Variables
Percentage
Mean
SD
Nutritional Status
Coastal areas
Good
49
176.1
52.33
Poor
51
Non-coastal areas
Good
42.9
159.3
62.95
Poor
57.1
Height
Coastal areas
Normal
81.6
1.27
1.014
Short
18.4
Non-coastal areas
Normal
63.3
Short
36.7
1.57
1.091
Body Mass Index
Coastal areas
Normal
87.8
-.40
1.183
Thin
4.1
Very thin
2.0
Fat
4.1
Obese
2.0
Non-coastal areas
Normal
61.2
-1.00
1.908
Thin
12.2
Very thin
16.3
Fat
6.1
Obese
4.1
Nutrient Adequacy Ratio
Coastal areas
Normal
26.5
177.6
52.58
Low
51.0
High
22.4
Non-coastal areas
Normal
42.9
162.0
64.26
Low
55.1
High
2.0
Comparison of Height, Body Mass Index, and Nutrient Adequacy Ratio of the Nutritional Status of School-Age Children in Coastal and
Non-Coastal Areas in Aceh
53
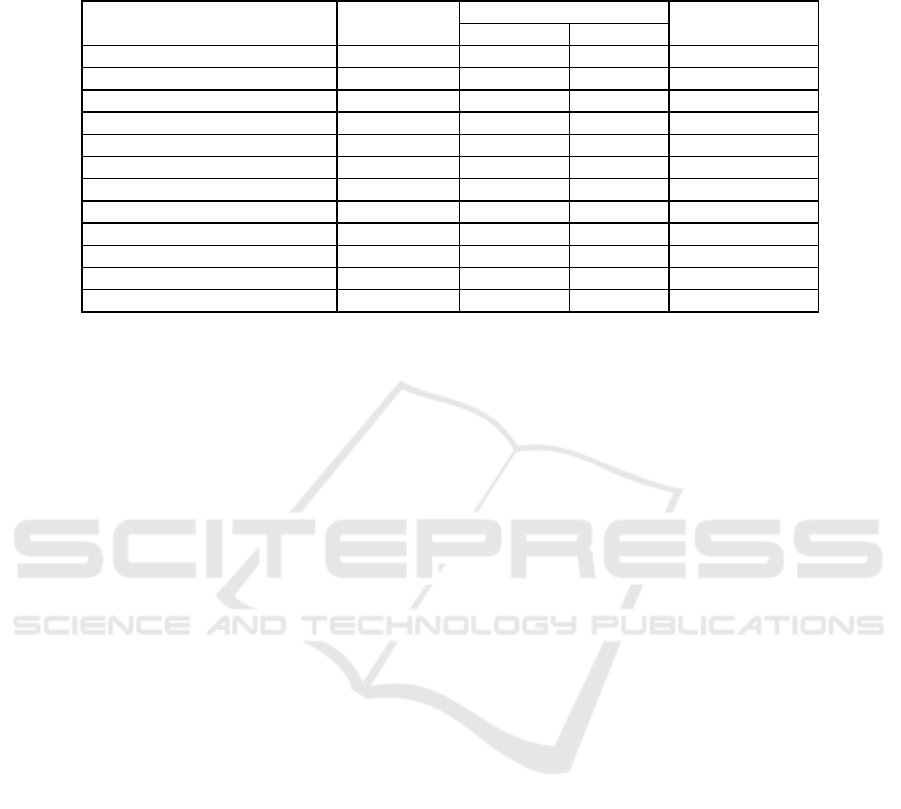
Table 3. Comparison of nutritional status of school-age children in coastal and non-coastal areas (n=98).
Measure Results
Mean
95% CI
Sig.
(2-tailed)
Lower
Upper
Nutritional Status
Coast
176.1
-6.5
39.9
.156
Non-coast
159.3
Height
Coast
-1.3
-.1
.7
.155
Non-coast
-1.6
Body Mass Index
Coast
-.4
-.4
1.2
.064
Non-coast
-1.0
Nutrient Adequacy Ratio
Coast
177.6
-7.8
39.2
.188
Non-coast
162.0
4 DISCUSSION
Nutrition is the key pillar of health and well-being
throughout one’s life cycle (Rohaedi, Julia&
Gunawan, 2014). Therefore, nutritional deficiencies
may yield to growth and development failures which
can continue into adulthood if not addressed early
(Rahmad, 2017). To determine one’s good
nutritional status, the availability of nutrients in the
body cells should be in sufficient amount. In
principle, however, one’s nutritional status is
directly affected by food consumption and disease
infection (Saputri, 2010).
Further, mother's knowledge of nutritional intake
and parenting methods are also closely related to
maternal education and food habits in the family and
community. The demography of this present study
reported that the family heads worked either as
fishermen or farmers with the income below the
minimum wage of Aceh workers. In addition, the
average maternal education in these two areas was
elementary school education, making it
understandable that the awareness of mothers in the
maintenance and modification of food concerning its
nutritional values was very lacking, which
subsequently had an impact on their children's
nutrition.
Adequacy of nutrient intake plays a crucial role
in children's nutritional needs. The role of mothers
and parenting is influential in achieving proper
children’ nutrition. Engle, Menon & Hadad (1997 in
Pratiwi, 2016) emphasize that three important
components, food, health, and psychosocial stimuli,
significantly contribute to the optimal growth of
children. At the basic stage, food is highly necessary
as it is the main element in the formation of
children's nutrition, allowing them to grow properly
according to their age. This is in line with the
research conducted by Nti and Lartey (2007) on the
effect of nutritional status care practices on children
in Ghanaian on 100 mothers of infants aged 6-12
months. Their results indicated that care givers who
practiced better nutritional care would have children
with good nutritional status. Another study by Isnida
(2016) concerning the relationship of socio-
demographic factors to the nutritional status of
children of SD Negeri 1 South Pringsewu found that
there was a relationship between maternal education
level (p-value < .001), father's type of work (p-value
< .001), and family income level (p-value < .001)
with the children’s nutritional status.
In this study, however, there was no difference in
the nutritional status of school-age children in
coastal and non-coastal coastal areas. It is highly
likely that low proportion of children’s nutrition
overall with a difference of 4.1%, normal body mass
index with a difference of 26.6%, normal stature
height with a difference of 18.3%, and low nutrient
adequacy ratios in average with a difference of 2.1%
have caused no signicant difference between two
studied areas. The low average of energy and protein
intake in children’s food consumption have led to
the lack of children’s nutritional status in coastal and
non-coastal areas. The findings of this study have
suggested that the low average of children’s
nutrition in the two areas may create a risk in the
children’s long-term growth and development.A
slightly similar study by Aulia (2015) on the
nutritional status profile of children based on the
topography of the residential area of Jepara District,
AINC 2018 - Aceh International Nursing Conference
54

surveying 30 coastal-area toddlers and 30 hillside
toddlers, also claimed that there was no difference in
the nutritional status (p-value = . 59), energy
consumption level (p-value = .51), energy efficiency
level (p-value = .25), and the availability level of (p-
value = .02) between the coastal area and the
hillside.
As nutrition is important in balancing children’s
physical and mental development, parents should be
more attentive to their children during parenting
(Ningsih, Suryanto & Restuastuti, 2016).
Differences in geographical environments will also
lead to differences in children’s growth and
development, particularly in height. A child’s height
is influenced not only by genetic traits, but also by
environmental factors. Sindiaga (2008) studied the
children’s height in terms of genetic and
environmental factors within the Batak Toba tribe
with a sample of 100 children in rural areas and 100
in urban areas aged 8-10 years. His study showed
that the rural children’s height was more correlated
with the fathers’ genetic factors while that in urban
areas was more correlated with child feeding.
In this study, however, there was no difference
between the nutritional status of school-age children
with their height in both areas. The study found that
the nutritional status was equally normal, with a
slight difference of 18.3%, in the two areas. The
anthropometric measurements reported that the
school-age children in coastal areas had an average
height of 126.7 cm while that in non-coastal area of
123.11 cm, indicating that the two regions had an
ideal height and thus, the children did not experience
a difference in their nutritional status. Additionally,
the children’s birth weight had an average of 3 kg in
both regions, and the normal growth of height
inschool-age children in the two areas was closely
related to the parents’ height. It was observed during
data collection that the average height of families
accompanying the respondents was generally in
good stature, suggesting that their children’s would
also be alike in the future.
In terms of the energy adequacy level consumed
by children, the coastal areas had an average of
65.3% while the non-coastal areas of 65.7%. Despite
being under the nutritional needs standard, some
children showed good energy intake which helped
them to burn the calories during activities and to
optimize their growth. Likewise, in terms of the
protein content, the children of the coastal areas had
an average protein of 114.5% and non-coastal areas
of 95.14%. Such a better protein intake also
contributes highly in developing the muscle cells
and body tissues, in repairing tissue damage, and in
maintaining a proper body height of children.
Sufficient nutrition will gradually improve the
growth and development of children; therefore,
malnourished children tend to grow small, thin and
short. Poor nutrition in children will also result in
the low cognitive ability or intelligence and decline
the children's productivity (Indonesian Ministry of
Health, 2014).
Malnutrition can occur due to a number of
factors, one of which is the lack of nutrient intake
and quality food (i.e., varied, as needed, clean, and
safe) consumed by children (Oktavia & Widajanti,
2017; Indonesian Ministry of Health,
2010).Changesin nutritional status can take place
because of a change (increase or decrease) in b ody
weight, a consequence of the knowledge and
attention f parents to nutritional problems.
According to Almatsier (2003), food consumption is
influenced by two external factors: food provided by
the family and the family purchasing ability of food.
If the food consumed meets adequate quantity and
quality, a good health status will be yielded. Parents,
especially mothers, should be good at selecting
quality food for their children to consume (Soegeng,
2009). Children needs for energy and protein are
relatively larger than adults because children
experience rapid growth and development (Auliya,
2015). Almatsier (2001) explains that the lack of
energy can cause children’s body to experience a
negative balance, resulting in the body weight to be
lower than the ideal standard, and the lack of protein
intake can greatly affect children’s nutrition, causing
the body tissues to get easily damaged.
In this present study, the total number of nutrient
adequacy ratios for children in coastal and non-
coastal areas were low, in which the coastal and
non-coastal children had a gap of 2.1%. The
inadequacies could be seen from the lack of
children's energy adequacy of 6.1% between two
areas, and the average consumption of protein needs
of 55.1% in coastal areas and of 36.7% in non-
coastal areas, yielding to a drop in the nutritional
status of children.
Brown and Isaacs (2014) argue that eating
behavior and food choices of school-age children are
strongly affected by parents and siblings as parents
are usually responsible for the types, the time, and
the amount of meals provided at home.
Nutritional status is a state of body that describes
food intake and uses of nutrients, wherein nutrients
are needed as the source of energy, growth, and
maintenance of body tissues (Almatsier, 2003).
School-age children, between the ages of 4-12,
require an average calorie of energy between 1,600-
Comparison of Height, Body Mass Index, and Nutrient Adequacy Ratio of the Nutritional Status of School-Age Children in Coastal and
Non-Coastal Areas in Aceh
55

2,100 kcal and an average protein of 35-56gr (Widya
Karya Pangan Nasional dan Gizi, 2004). The
consumption patterns will determine the qualitative
and quantitative aspects of the amount of nutrients
consumed.
The people in the coastal areas who are mostly
fishermen are more inclined to consume animal
protein food from the sea, whereas the people in
hilly areas (uplands), most of which are farmers,
have a tendency to eat vegetable protein food
sources. The difference in the types of these
commodities has led to differences in the types and
amounts of food commonly consumed daily
(Khomsan, 2006).
A person's nutritional status can be seen from
what is consumed and how the food pattern is. If the
diets are proper and correct, the nutritional status
will turn out to be well, and vice versa. Nutrition is
further associated with one's economic potential
because nutrition is related to brain development,
learning ability, and child labor productivity
(Almatsier, 2010).
In terms of the nutritional intake, this study
found that children in coastal and non-coastal areas
had low energy intake with a 6.1% difference.
Further, the average consumption of protein was
55.1% in coastal areas and 36.7% in non-coastal
areas. The analysis showed that there was no
difference in the status of school-age children in the
two areas. The finding suggested that both coastal
and non-coastal areas have had considerably similar
characteristics, i.e., types of food (carbohydrate,
protein, fat, and energy) consumed by the children,
as evidenced from Food Recall assessment form.
The form described that the children in both studied
sites consumed almost the same food, such as rice
(fried, savory, and steam), mackerel tuna, milkfish,
shrimp, bread, vegetables, fried noodles, rice cake,
sponge cake, and snacks. These foods were quite
similar, and therefore, the impact was relatively the
same in spite of differences in location, frequency of
food intake, childhood history of illnesses, parental
work, and parental education.
Parental income was another influencing factor
in the absence of nutritional adequacy differences
between children in coastal and non-coastal areas.
Due to low wages, the fishermen and farmers
preferred selling raw materials gained from fishing
and gardening to processing them for their families;
thus, preventing their children to attain better energy
and protein intake. Research by Khayati (2011) and
Lutviana (2010) conformed to this finding that more
toddlers (8%) in fisherman families had poor
nutritional status than those (4.2%) in farmer
families since the toddlers in fishermen families had
much lower levels of energy and protein (9% and
12%) deficiency compared to those (4.2% and 1.4%)
in farmer families.
5 CONCLUSION
The study concluded that there were no differences
in the nutritional status, in height, in body mass
index, and also in the nutrient adequacy ratio of
school-age children (6-12 years) in the coastal and
non-coastal areas in Aceh, Indonesia.
REFERENCES
Almatsier, S. (2010). Nutrition Science Basic Principle.
Gramedia Pustaka Umum, Jakarta, Indonesia
Almatsier, S. (2009). Nutrition Science Basic Principle.
Gramedia Pustaka Umum, Jakarta, Indonesia
Almatsier, S. (2003). Nutrition Science Basic Principle.
Gramedia Pustaka Umum, Jakarta, Indonesia
Almatsier, S. (2001). Nutrition Science Basic Principle.
Gramedia Pustaka Umum, Jakarta, Indonesia
Ariyanti, F S. (2015). Analisis Faktor Risiko Kejadian
Stunting Pada Anak Balita Di Wilayah Kerja
Puskesmas Muara Tiga Kabupaten Pidie [Analysis Of
Risk Factors For The Incidence Of Stunting In Under
Five Years-Old Children In The Working Area Of
Muara Tiga Puskesmas Pidie District]. Thesis,
Faculty of Public Health, University of Sumatera
Utara, Medan, Indonesia.
Auliya, C., Woro, O & Budiono, I. (2015). Profil Status
Gizi Balita Ditinjau Dari Topografi (Studi
Wilayah Pantai Dan Wilayah Punggung Bukit
Kabupaten Jepara) [Profile Oftoddler Nutritional
Status From Topographic Territory Residentials (A
study in the coastal regions and hillsides of Jepara
District)]. Unnes Journal of Public Health, 4(2)
Basic Health Research (RISKESDAS) 2013. National
Research and Development Department of Ministry of
Health. Jakarta, Indonesia
Brown, J. E., & Isaacs, J. S. (2014). Nutrition Through
The Life Cycle. CENGAGE Learning. United States of
America: Thomson Wadsworth
Burchi, F. (2012). Whose Education Affects A Child's
Nutritional Status? From Parents' To Household's
Education. Demographic Research, 27 (9).
Hamidah, S., Sartono, A., & Kusuma, H.S. (2017).
Perbedaan Pola Konsumsi Bahan Makanan Sumber
Protein di Daerah Pantai, Dataran Rendah dan Dataran
Tinggi [Difference the Pattern of Food Consumption
in Protein Sources in Coastal Areas, Lowlands and
Highlands]. Jurnal Gizi, 6 (1)
AINC 2018 - Aceh International Nursing Conference
56

Indonesian Ministry of Health. (2014). Balanced
Nutrition Guidelines. Department of Ministry of
Health, Jakarta, Indonesia.
Khayati, S. (2011). Faktor Yang Berhubungan Dengan
Status Gizi Balita Pada Keluarga Buruh Tani Di Desa
Situwangi Kecamatan Rakit Kabupaten Banjarnegara
[Factors Which Related With Nutritional Status Of
Children Under Five In Farm Worker Families In The
Situwangi Village, Rakit District, Banjarnegara
Regency]. Bachelor Thesis. State University of
Semarang, Lambang, Indonesia
Lutviana, E. (2010). Prevalensi dan Determinan Kejadian
Gizi Kurang Pada Balita (Studi Kasus Pada Keluarga
Nelayan di Desa Bojomulyo Kecamatan Juana
Kabupaten Pati) [Prevalence And Determinants Of
Less Nutrition Events In The Toddler (Case Study of
Fisherman Families in Bojomulyo Village, Juana
District, Pati Regency0]. Thesis. State University of
Semarang, Lambang, Indonesia
Meriska, I.,Pramudho, K & Murwanto, B. (2014). Perilaku
Sarapan Pagi Anak Sekolah Dasar [The Behavior Of
Breakfast In Elementary School Child]. Jurnal
Kesehatan Poltekes Tanjung Karang, 5 (1)
Ningsih, Y. A., Suryanto, & Restuastuti, T. (2016).
Gambaran Status Gizi Pada Siswa Sekolah Dasar
Kecamatan Rangsang Kabupaten Kepulauan Meranti
[Describe The Nutritional Status Of Elementary
School Students In The District Rangsang Kepulauan
Meranti]. Jurnal Online Mahasiswa Fakultas
Kedokteran, 3 (2)
Nti, A. C., Lartey, A. (2007). Effect of Caregiver Feeding
Behaviours on Child Nutritional Status in Rural
Ghana. International IJC, 31(3)
Oktavia, S., Widajanti, L & Aruben, R. (2017). Faktor-
Faktor Yang Berhubungan Dengan Status Gizi Buruk
Pada Balita Di Kota Semarang [The Factors
Associated With Malnutrition Status In Under Five
Child In Nutrition House Of Semarang City]. Jurnal
Kesehatan Masyarakat Undip, 5 (3)
Pratiwi, D. T., Masrul & Yerizel, E. (2016). Hubungan
Pola Asuh Ibu dengan Status Gizi Balita di Wilayah
Kerja Puskesmas Belimbing Kota Padang [The
Relationship Mother's Parenting Style with Toddler
Nutrition Status In The Work Area of Belimbing
Health Center In Padang City]. Jurnal Kesehatan
Andalas, 5 (3)
Rahmad, A. H. A. (2017). Pemberian Asi Dan MP-Asi
Terhadap Pertumbuhan Bayi Usia 6 – 24 Bulan [The
Relationship Between Breastfeeding And
Complementary Feeding With Infant Growth At 6-24
Months in in Lamreung Aceh Besar]. Jurnal
Kedokteran Syiah Kuala, 17 (1)
Riyadi, H., Khomsan, A., Dadang, S., Faisal, A., Eddy, S.
(2006). Studi tentang status gizi pada rumah tangga
miskin dan tidak miskin [Nutritional Status Of Poor
And Non-Poor Households]. Journal Of The
Indonesian Nutrition Association, 29 (1)
Rohaedi, S., Julia, M., & Gunawan I. M. (2014). Tingkat
ketahanan pangan rumah tangga dengan status gizi
balita di daerah rawan pangan Kabupaten Indramayu
[The Relationship Between Household Food Security
Level With Under Five Children’s Nutritional Status
In Family Of Food Scarcity-Area In Indramayu Sub-
District]. Jurnal Gizi Dan Dietetik Indonesia, 2 (2).
Sandiaga, P. J. (2008). Tinggi Badan Anak Ditinjau Dari
Segi Faktor Genetik Dan Lingkungan (Studi
Antropologi Ragawi Pada Suku Batak Toba) [Child
Height Viewed From The Aspect Of Genetic Factors
And The Environment]. MEDIKORA, 4 (2)
Saputri, A., (2010). Hubungan Antara Tekanan Darah
Dengan Status Gizi Berdasarkan CDC 2000 Pada
Anak Usia 6-13 Tahun SD Negeri 060900 Medan
Johor [Relationship Between Blood Pressure With
Nutritional Status Based On Cdc 2000 In Children
Aged 6-13 Years Primary School 060900 Medan
Johor] . Bachelor Thesis. Faculty of Medicine, Islamic
University of North Sumatra, Medan, Indonesia.
Soegeng, S. (2009). Health and Nutrition. Rineka Cipta
Bina Adiaksara, Jakarta, Indonesia
Umi, I. (2005). Perbedaan Status Gizi dan Prestasi
Belajar anak Di Sekolah Dasar Negeri Daerah Pantai
dan Daerah Pegunungan Kabupaten Pati [Difference
in Nutritional Status and Child Learning Achievement
In Public Elementary School Coastal Areas and
Mountain Regions Pati Regency]. Bachelor Thesis.
State University of Semarang, Lambang, Indonesia
Widyakarya Nasional Pangan dan Gizi (National Food and
Nutrition Forum). (2004). Nutrient Adequacy Ratio of
the Nutritional Indonesian, Jakarta, Indonesia
World Health Organization. (2014). Situation:
Underweight In Children in Global Health
Observatory. World Health Organization, Geneva.
World Food Programme. (2014). 10 Facts About
Malnutrition In Indonesia. World Food Programme,
Rome, Italy.
Yani, M., Bakri. (2015). Pidie Peringkat Kedua Gizi
Buruk [Pidie Ranks Second In Malnutrition]. TRIBUN
News
Comparison of Height, Body Mass Index, and Nutrient Adequacy Ratio of the Nutritional Status of School-Age Children in Coastal and
Non-Coastal Areas in Aceh
57
