
Public Counseling: An Educational Model to Improve Medication
Adherence in Type 2 Diabetes Mellitus Patients
Daniek Viviandhari, Nora Wulandari and Francyska Putri Puspita
Delima II Street, Klender, East Jakarta, Indonesia
Keywords: Public counseling, medication adherence, type 2 diabetes mellitus, the A1C.
Abstract: Introduction: Diabetes mellitus is a major chronic illness worldwide, including in Indonesia. Also, the
adherence to antidiabetic medicines remains unsatisfactory. Aim: This study aimed to evaluate the effectiveness
of public counseling to increase medication adherence in patients with type 2 diabetes mellitus. Methods: This
prospective study used a pre-test-post-test quasi-experimental design. It was conducted at Pondok Kelapa
primary health care center in East Jakarta. The intervention was public counseling that was delivered once per
month for three months (12 weeks) of the study period. The A1C (glycated haemoglobin) was assessed twice,
i.e., before and after the intervention. Results: Among the 30 patients who met the inclusion criteria, 83.3% of
them had the A1C level >6.5%. After 12 weeks of intervention, the percentage of A1C signicantly declined
to 23.3% (p=0.00). Conclusion: Public counseling is effective to increase medication adherence in patients
with type 2 diabetes mellitus.
1 INTRODUCTION
Diabetes mellitus (DM) is dened as elevated blood
glucose attributable to inadequate or no pancreatic
insulin secretion, with or without the concurrent
impairment of insulin action (Katzung and Trevor,
2015). In most cases, type 2 DM is characterized by a
combination of some degree of insulin resistance and
relative insulin deciency (DiPiro et al., 2015).
Using a DM-based interview, the national survey
in 2013 showed that the prevalence of DM increase
from 1.1% (2007) to 2.1% (2013). The highest
prevalences were found in Yogyakarta (2.6%), Jakarta
(2.5%), North Sulawesi (2.4%), and East Kalimantan
(2.3%) (Badan Penelitian dan Pengembangan
Kesehatan, 2013). According to WHO (World
Health Organization, 2016), the prevalence of DM in
Indonesia in 2016 was 7.0%.
DM is a chronic illness that requires continuous
medical care and patient education and support in
self-management to prevent acute complications and
reduce the risk of long-term complications. Diabetes
care is complex, and it requires multifactorial risk
reduction strategies beyond glycemic control (Care,
2013).
The American Diabetes Association (ADA, 2017)
mentions that 33-49% of patients still persistently
fail to meet the targeted A1C level. One of the major
contributing factors is poor medication adherence
(Polonsky and Henry, 2016). Patients with DM
usually have comorbidities that make their treatment
regimens even more complex and probably lower the
adherence. Poor adherence to DM treatment results
in the avoidable development of complications of
diabetes and the extra costs for the healthcare system
(De Geest and Sabaté, 2003).
Education is one of the various measures to
increase adherence in type 2 DM patients (García-
Pérez et al., 2013). Patient education constitutes
a critical tool used to control diabetes better and
help with the prevention of complications and cost
reduction. There is no adequate evidence of which
education methods are the most effective in improving
the clinical outcomes of people with type 2 DM
(Merakou et al., 2015). Pharmacists can contribute
and play a major role in the assessment of patients’
understanding of the illness and therapy of DM,
including the discussion of any barriers to adherence
that patients may have (Inamdar et al., 2013).
Group education has been characterized as a
Faculty of Pharmacy and Science, Universitas Muhammadiyah Prof. DR. HAMKA,
Viviandhari, D., Wulandari, N. and Puspita, F.
Public Counseling: An Educational Model to Improve Medication Adherence in Type 2 Diabetes Mellitus Patients.
DOI: 10.5220/0008239600710076
In Proceedings of the 1st Muhammadiyah International Conference on Health and Pharmaceutical Development (MICH-PhD 2018), pages 71-76
ISBN: 978-989-758-349-0
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
71

cost-effective alternative to individual education for
DM. Taking place in a primary health care center in
Greece, Merakou et al. (2015) conrm that group-
based patient education with some models for people
with type 2 DM is more effective in diabetes self-
management compared with individual education.
This nding is positively encouraging since group
education needs a small amount of resource but
improves patient outcome, especially when faced with
the limited number of pharmacists in primary health
care centers in Indonesia. Many models apply to
group discussions. One of them is public counseling.
Hence, this research aimed to assess the effectiveness
of public counseling model at a primary health care
center in East Jakarta.
2 MATERIALS AND METHOD
2.1 Materials
The tool used to collect the research data was the A1C
level reader, i-Chroma TM.
2.2 Methods
This prospective study used a total sampling
method and took place at Pondok Kelapa primary
health care center in East Jakarta, Indonesia from
July 2017 to October 2017. The participants were
patients with type 2 DM. The pre-test-post-test
quasi-experimental design was intended to measure
the effectiveness of public counseling that was
delivered during the study period. The intervention
was given three times in 12 weeks. The collected
data was A1C (the glycated haemoglobin) levels
from the pre-test and post-test.
The inclusion criteria:
▪ Patients aged >18 years;
▪ Patients had DM for more than one year;
▪ Patients took oral antidiabetic drugs (OADs);
▪ Patients with fasting blood sugar level >126 mg/
dL in three (3) consecutive months;
▪ Patients who regularly came to the primary health
care center for a routine check-up.
The exclusion criteria:
▪ Pregnant women
The research proposal was submitted to the
Research Ethics Committee of Faculty of Medicine,
University of Indonesia. This study had received the
Ethical Approval test and passed the study ethics
(No. 325/UN2.FI/ETIK/2017). Patient screening
was conducted after the research permit was granted.
Patients were asked for their willingness to participate
as research respondents by signing a letter of approval
of participation or informed consent and given
information in advance. The stages of data collection:
▪ Subjects who had declared their willingness to
become respondents lled out the consent form to
participate in the research. The minimum sample
size was not specied. The data collection used
total sampling method, i.e., the samples are all
respondents who are willing to follow the course
of the entire study and within the inclusion criteria;
▪ The initial measurement of HbA1C levels as the
pre-test data;
▪ Respondents were given education in the form of
public counseling three times in three (3) months;
▪ The public counseling was delivered to the patients
by two researchers, i.e., the lecturers at the Faculty
of Pharmacy and Sciences, UHAMKA. The one-
hour lecture was then followed by another hour
of Q&A session. This provision of education was
conducted in one of the rooms in the primary health
care center. The presented material was divided
into three parts: (1) General explanation of DM,
complications of DM, and DM therapy (including
the explanation of ‘if the patient forgets to take
medication’) (2) Diabetic diet plan and repeated
explanation of DM therapy, (3) Physical exercise
plan and repeated explanation of DM therapy.
Technically, patients were gathered in a room at
the primary health care center and then provided
with the education in the form of lectures. At the
end of the lectures, a Q&A session (discussion)
was conducted;
▪ The post-test data were obtained by re-measuring
HbA1C levels after three months;
▪ The data was then subjected to processing and
analysis.
2.3 Data Analysis
The data were analyzed descriptively to obtain
a frequency distribution and the proportion of
various research variables. The three variables
were sociodemographic characteristics, clinical
characteristics, and lifestyle characteristics. The
Wilcoxon’s t-test was performed to determine the
changes in A1C level. Statistical signicance was set
at p<0.05. All statistical analyses were performed in
the Statistical Package for Social Sciences (SPSS)
software for Windows version 22.0.
MICH-PhD 2018 - 1st Muhammadiyah International Conference on Health and Pharmaceutical Development
72
3 RESULTS AND DISCUSSION
From July to October 2017, as many as 50 patients
were selected as respondents, but only 30 of them
participated until the end of the 12-week study.
3.1 Patient Characteristics
The distribution of respondents based on
sociodemographic characteristics is shown in Table
1. The majority of the respondents were female
(63.3%). The national data of the prevalence of type
2 DM veries this nding, i.e., that the majority of
type 2 DM patients are females (Badan Penelitian
dan Pengembangan Kesehatan, 2013). Most of
the respondents were aged ≥ 60 years (80.0%).
According to a consensus report, population aging is
a signicant driver of the diabetes epidemic (Kirkman
et al., 2012). The respondents mostly had middle and
high levels of education (36.7% each). According
to a study at a primary health care center in Jakarta,
there is no signicant correlation between the level of
education and type 2 DM incidence (Trisnawati and
Setyorogo, 2013). Around 90% of the respondents
were unemployed since most of them were retired.
The distribution of respondents based on clinical
characteristics is presented in Table 2. Approximately
63.3% of them had a history of type 2 DM for ≥ 5
years. Gimenes et al., (2009) and Elsous et al. (2017)
claim that there is a negative relationship between the
history of DM and patients’ adherence to medications.
In other words, the longer the history of DM, the
more noncompliance a patient to his/her medication.
The majority of the respondents received >1 oral
antidiabetic drugs (OAD) (80.0%). A single or a
combination of OAD can be used if necessary, and the
combined OADs should act by different mechanisms
(PERKENI, 2015). Most of the respondents had one
comorbidity (60.0%). Hypertension was the most
common comorbidity in this study. Hypertension
substantially increases the risk of both macrovascular
and microvascular complications, including stroke,
coronary artery disease, and peripheral vascular disease,
retinopathy, nephropathy, and possibly neuropathy
(ADA, 2003). The majority of the respondents (86.7%)
used other medicines. This condition was attributable
to the comorbidity, which made their treatment
regimens even more complex and probably reduced the
adherence (De Geest and Sabaté, 2003). Only 26.7% of
the respondents experienced an adverse drug reaction
(side effect). Wabe et al., (2011) explain that the main
external factors for nonadherence are lack of nance
(37.1%) and, followed by, a perceived side effect of the
drug (29.2%).
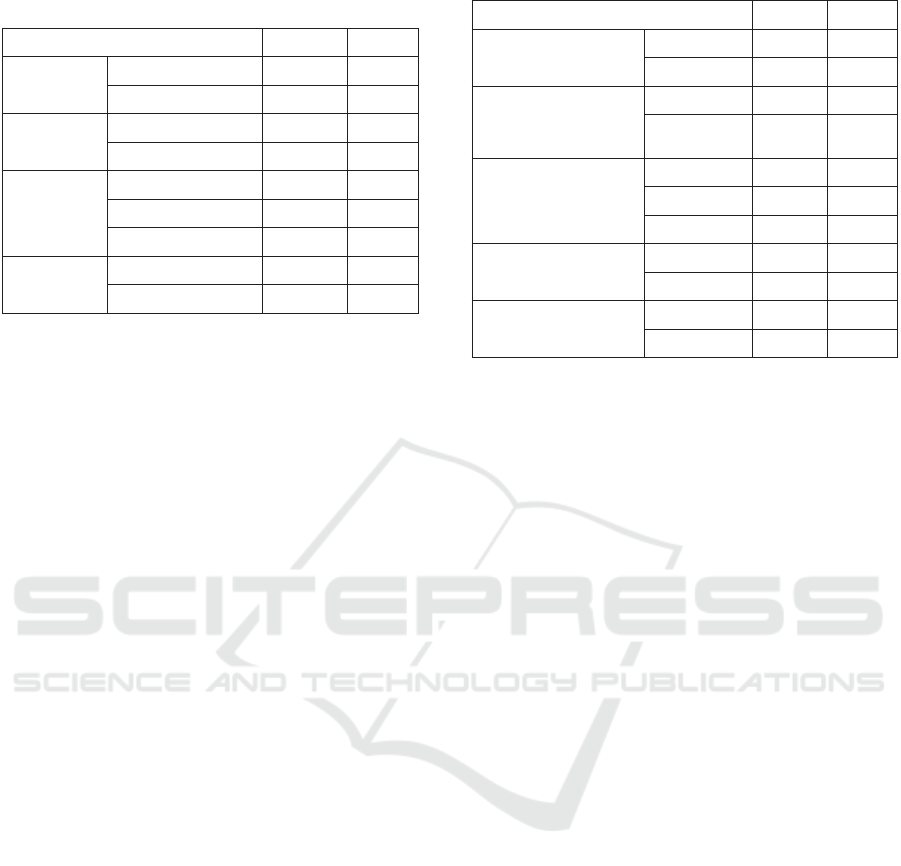
The distribution of respondents based on lifestyle
characteristics is summarized in Table 3. Around
83.3% of them adjusted their dietary habit to include
sugar and carbohydrate restriction. Patients with type 2
DM often require caloric restriction to promote weight
loss (DiPiro et al., 2015). Patients should have good
knowledge about their disease and recommended diet,
and, for this purpose, the health care providers must
inform them to make changes in their nutritional habits
and food preparations. Active and effective dietary
education may prevent the onset of diabetes and its
complications (Sami et al., 2017). The comparison of
pre-test and post-test data showed a decrease in the
number of respondents who were smoking. Several
studies have also associated smoking with an increased
risk of developing diabetes. Smoking increases diabetic
incidences and aggravates glucose homeostasis
and chronic diabetic complications (Chang, 2012).
Table 1: The Sociodemographic characteristics of the
Respondents.
Characteristics n = 30 %
Sex
Male 11 36.7
Female 19 63.3
Age
< 60 years 6 20.0
≥ 60 years 24 80.0
Level of
education
Low 8 26.7
Middle 11 36.7
High 11 36.7
Occupation
Unemployed 27 90.0
Employed 3 10.0
Table 2: The clinical characteristics of the respondents.
Characteristics n = 30 %
History of type 2 DM
< 5 years 11 36.7
≥ 5 years 19 63.3
Numbers of oral
antidiabetic drug
(OAD)
1 6 20.0
> 1 24 80.0
Comorbidity
No 4 13.3
1 18 60.0
2 or more 8 26.7
Other medicines
Yes 26 86.7
No 4 13.3
Adverse Drug
Reaction
Yes 8 26.7
No 22 73.3
Public Counseling: An Educational Model to Improve Medication Adherence in Type 2 Diabetes Mellitus Patients
73

The Indonesian Association of Endocrinologists
(Perkumpulan Dokter Endokrinologi Indonesia) state
that exercise is one of the most important things in
DM management if not accompanied by nephropathy.
Exercise should be practiced regularly, i.e., 3-5 times a
week for about 30-45 minutes with 150 minutes in total
per week. The pause between exercises is not more than
two consecutive days (PERKENI, 2015). According to
Puspitasari et al. (2013), the use of herbal medicines as
hypoglycemic agents does not give a signicant effect
on the A1C level because the information regarding
the dose, duration, and administration of the herbal
medicines may be uncertain.
3.2 The Eectiveness of Education
(Public Counseling)
The parameter used to assess compliances was A1C
level. A1C reects the average glycemia over several
months and has a strong predictive value for diabetes
complications (Cameron, 2006). Some studies have
reported that an increase in medication adherence to
oral hypoglycemics is associated with a reduction
in the A1C level, indicating a positive correlation
between A1C level reduction and medication
adherence (Lin et al., 2017). The goal of the A1C level
in DM management is ≤ 6.5% (American Diabetes
Association (ADA), 2017).
The A1C level in this research was measured at the
Indonesian Center for Health Laboratory, Ministry of
Health, which has been accredited according to ISO/
IEC 17025:2005. The analysis of the measurement
results referred to the methods used in DCCT (The
Diabetes Control and Complication Trial), i.e., HPLC
method (High-Performance Liquid Chromatography)
(Sacks et al., 2011). The mean A1C levels in the pre-
test and post-test are shown in Table 4.
Around 83.3% of the respondents still had a high
A1C level (≥ 6.5%) before the intervention. However,
the number declined to 23.3% after they received the
education. The results showed a signicant difference
(p = 0.00) between the A1C levels before and after
the intervention. The mean A1C level before the
intervention was 7.83±1.59%, which declined after
the public counseling (5.41±1.34). As a conclusion,
education increases medication adherence in type 2
DM patients.
Wulandari et al. (2017) conducted similar research
at Makasar and Kebon Pala primary health care centers
in East Jakarta in 2017. Using public counseling and
booklet handouts as a model of education, they reveal
that among the type 2 DM respondents who completed
the interventions, 63.3% of them initially had HbA1C
level >7%. However, after the interventions, the
percentage declined signicantly (p < 0.05) to 23.3%,
Table 3: The lifestyle characteristics of the respondents.
Characteristics
n = 30
Pre-test Post-test
% n = 30 %
Dietary habit Adjusted 25 83.3 24 80.0
Not adjusted 5 16.7 6 20.0
Smoking Yes 3 10.0 1 3.3
No 27 90.0 29 96.7
Exercise Yes 28 93.3 27 90.0
No 2 6.7 3 10.0
Herbs Yes 1 3.3 1 3.3
No 29 9.7 29 96.7
Table 4: The mean A1C levels before and after intervention.
A1C levels
Pre-test Post-test
n = 30 % n = 30 %
a. < 6.5% 5 16.7 23 76.7
b. ≥ 6.5% 25 83.3 7 23.3
Mean ± SD 7.83±1.59 5.41±1.34
P 0.00
Table 5: The mean A1C levels before and after intervention
at Makassar and Kebon Pala primary health care centres.
A1C levels
Pre-test Post-test
n = 30 % n = 30 %
a. < 7% 11 36.7 23 76.7
b. ≥ 7% 19 63.3 7 23.3
Mean ± SD 7.72±1.356 6.18±0.988
P 0.00
MICH-PhD 2018 - 1st Muhammadiyah International Conference on Health and Pharmaceutical Development
74

as seen in Table 5. As a conclusion, intervention with
public counseling and booklet handouts is effective to
improve the compliance of patients with type 2 DM.
Both Wulandari et al. (2017) and this study used
respondents from primary health care centers in East
Jakarta, but they differed in the model of education.
Public counseling alone also signicantly improves
patient’s adherence to complete the medication.
Taking place in a primary health care center in Greece,
Merakou et al. (2015) state that group-based patient
education with some models for people with type 2
DM is more effective in diabetes self-management
compared with individual education.
Medication adherence is the most important
component in type 2 DM management. It is achievable
by giving routine education to patients to increase
their knowledge about their disease and medication.
Pharmacists can contribute and play a major role in
the assessment of patients’ understanding of the illness
and therapy of DM (Inamdar et al., 2013). Hughes et
al. (2017) explain that there is signicant evidence to
support the role of pharmacists in providing a range of
extensive diabetes care services, from the screening
to the continuous management of the state of the
disease. Furthermore, Supardi and Susyanti (2012)
state that only 10% of the primary health care centers
in Indonesia have pharmacists. The limited number of
pharmacists at primary health care centers inhibits the
provision of personal education by pharmacists to the
patients. Public counseling becomes an alternative
that is effective and cost-efcient.
4 CONCLUSIONS
Educational intervention through public counseling
is signicantly effective to improve medication
adherence in type 2 diabetes mellitus patient.
ACKNOWLEDGMENTS
The authors would like to acknowledge all
pharmacists and other health professionals at Pondok
Kelapa primary health care center in East Jakarta who
were involved in this research.
REFERENCES
American Diabetes Association (ADA), 2003. Treatment
of hypertension in adults with diabetes, Diabetes
Care, 26(suppl 1), pp. S80–S82. doi: 10.2337/
DIACARE.26.2007.S80.
American Diabetes Association (ADA), 2017. Standard of
medical care in diabetes - 2017, Diabetes Care, 40 (sup
1)(January), pp. s4–s128. doi: 10.2337/dc17-S003.
Badan Penelitian dan Pengembangan Kesehatan, 2013.
Riset Kesehatan Dasar (RISKESDAS) 2013, Laporan
Nasional 2013, pp. 1–384. doi: 1 Desember 2013.
Cameron, F., 2006. Standards of Medical Care in Diabetes -
2016, Australian family physician, 35(6), pp. 386–390.
doi: 10.2337/dc14-S014.
Care, M., 2013. Standards of medical care in diabetes - 2013,
Diabetes Care, 36(SUPPL.1). doi: 10.2337/dc13-S011.
Chang, S. A., 2012. Smoking and type 2 diabetes mellitus,
Diabetes and Metabolism Journal, 36(6), pp. 399–403.
doi: 10.4093/dmj.2012.36.6.399.
De Geest, S. and Sabaté, E., 2003. Adherence to long-term
therapies: Evidence for action, European Journal of
Cardiovascular Nursing, 2(4), p. 323. doi: 10.1016/
S1474-5151(03)00091-4.
DiPiro, J. T., Wells, B. G., Schwinghammer, T. L., DiPiro,
C. V., 2015. Pharmacotherapy handbook. Available
at: http://www.loc.gov/catdir/toc/mh023/99073195.
html%5Cnhttp://www.loc.gov/catdir/enhancements/
fy0653/99073195-d.html.
Elsous, A., Radwan, M., Al-Sharif, H., Mustafa, A. A., 2017.
Medications adherence and associated factors among
patients with type 2 diabetes mellitus in the Gaza Strip,
Palestine, Frontiers in Endocrinology, 8(JUN), pp. 1–9.
doi: 10.3389/fendo.2017.00100.
García-Pérez, L.-E., Alvarez, M., Dilla, T., Gil-Guilen, V.,
Orozco-Beltran, D., 2013. Adherence to Therapies in
Patients with Type 2 Diabetes, Diabetes Therapy, 4(2),
pp. 175–194. doi: 10.1007/s13300-013-0034-y.
Gimenes, H., Zanetti, M. and Vanderlei, J., 2009. Factors
related to patient adherence to antidiabetic drug therapy,
Revista latinoam Enfermagem, 17(1), pp. 46–51. doi:
10.1590/S0104-11692009000100008.
Hughes, J. D., Wibowo, Y., Sunderland, B., Hoti, K., 2017.
The role of the pharmacist in the management of type
2 diabetes: current insights and future directions,
Integrated Pharmacy Research and Practice, 6, pp.
15–27. doi: 10.2147/IPRP.S103783.
Inamdar, S. Z., Kulkarni, R. V., Karajgi, S. R., Manvi, F.
V., Ganachari, M. S., Mahendra-Kumar. B. J., 2013.
Medication Adherence in Diabetes Mellitus : An
Overview on Pharmacist Role, American journal of
advanced drug delivery, 1(3), pp. 238–250.
Katzung, B. G. and Trevor, A., 2015. Basic & Clinical
Pharmacology, 13th Edition, Basic and Clinical
Pharmacology.
Kirkman, M. S., Briscoe, V. J., Clark, N., Florez, H., Haas,
L. B., Halter, J. B., Huang, E. S., Korytkowski, M. T.,
Munshi, M. N., Odegard, P. S., Pratley, R. E., Swift,
C. S., 2012. Diabetes in older adults, Diabetes Care,
35(12), pp. 2650–2664. doi: 10.2337/dc12-1801.
Lin, L.-K. Sun, Y., Heng, B H., Chew, D. E. K.,Chong, P.
N., 2017. Medication adherence and glycemic control
among newly diagnosed diabetes patients, BMJ Open
Public Counseling: An Educational Model to Improve Medication Adherence in Type 2 Diabetes Mellitus Patients
75

Diabetes Research & Care, 5(1), p. e000429. doi:
10.1136/bmjdrc-2017-000429.
Merakou, K. Knithaki, A., Karageorgos, G., Theodoridis,
D. Barbouni, A., 2015. Group patient education:
Effectiveness of a brief intervention in people with type
2 diabetes mellitus in primary health care in Greece: A
clinically controlled trial, Health Education Research,
30(2), pp. 223–232. doi: 10.1093/her/cyv001.
PERKENI, 2015. Konsensus Pengendalian dan
Pencegahan Diabetes Melitus Tipe 2 di Indonesia 2015,
Perkeni. doi: 10.1017/CBO9781107415324.004.
Polonsky, W. H. and Henry, R. R., 2016. Poor medication
adherence in type 2 diabetes: Recognizing the scope of
the problem and its key contributors, Patient Preference
and Adherence, 10, pp. 1299–1306. doi: 10.2147/PPA.
S106821.
Puspitasari, A. W., R.Andrajati and A.Bahtiar, 2013.
Analisis Efektivitas Booklet Obat terhadap Tingkat
Kepatuhan Pasien Diabetes Melitus tipe-2, Journal of
Management and Pharmacy Practice, 2, pp. 1–7.
Sacks, D. B. Arnold, M., Bakris, G. L., Bruns, D. E., Horvath,
A. R., Kirkman, M. S., Lernmark, A., Metzger, B. E.,
Nathan, D. M., 2011. Guidelines and recommendations
for laboratory analysis in the diagnosis and management
of diabetes mellitus, Diabetes Care, 34(6). doi: 10.2337/
dc11-9998.
Sami, W. Ansari, T., Butt, N. S., Hamid, M. R. A., 2017.
Effect of diet on type 2 diabetes mellitus: A review,
International journal of health sciences, 11(2), pp. 65–
71. doi: 10.1002/dmrr.2515.
Supardi, S. and Susyanti, A. L., 2012. Kebijakan penempatan
apoteker di puskesmas, Buletin Penelitian Sistem
Kesehatan, (15), pp. 133–142. Available at: http://
ejournal.litbang.depkes.go.id/index.php/hsr/article/
view/2987/2220.
Trisnawati, S. K. and Setyorogo, S., 2013. Faktor Risiko
Kejadian Diabetes Melitus Tipe II Di Puskesmas
Kecamatan Cengkareng Jakarta Barat Tahun 2012,
Jurnal Ilmiah Kesehatan, 5(1), pp. 6–11.
Wabe, N. T., Angamo, M. T., & Hussein, S., 2011.
Medication adherence in diabetes mellitus and self-
management practices among type-2 diabetics in
Ethiopia, North American Journal of Medical Sciences,
3(9), 418–.
World Health Organization, 2016. Diabetes Country
Prole, diabetes country prole Indonesia,
48(6), p. 18882A–18882B. doi: 10.1111/j.1467-
825X.2011.03931.x.
Wulandari, N., Viviandhari, D. and Nurhayati, 2017. A
Strategic Approach to Increase the Compliance of
Patients with Type 2 Diabetes Mellitus, in Unity in
Diversity and the Standardisation of Clinical Pharmacy
Services: Proceedings of the 17th Asian Conference
on Clinical Pharmacy (ACCP 2017), in Elida, Z. et al.
(eds). Yogyakarta: CRC Press/Balkema. doi: ISBN:
978-1-138-08172-7 (Hbk) ISBN: 978-1-315-11275-6
(eBook).
MICH-PhD 2018 - 1st Muhammadiyah International Conference on Health and Pharmaceutical Development
76
