
Allergen Activity Pattern in Patch Test on Allergic Contact
Dermatitis Patient at Dermato-Venereology Clinic, Dr. Sardjito
Central General Hospital, Yogyakarta 2012-2016
Budi Satria, Fajar Waskito, Niken Indrastuti, Duma Mauliyasari, Sri Awalia Febriana
Dermato–Venereology Department Sardjito Central General Hospital, Gadjah Mada Medical Faculty, Yogyakarta,
Indonesia.
Keywords: Allergic Contact Dermatitis, allergen activity pattern, sensitizer, irritant, ascending pattern, descending
pattern.
Abstract: Allergic Contact Dermatitis (ACD) was caused by some group of substances which was called allergen.
Groups of those substances have their own characteristic as a sensitizer or irritant. Clinical manifestation as a
visible symptom is a balancing result between sensitizer and irritant that will be describe on pattern of allergen
activity from patch test result. This research was performed to describe allergen activity pattern for five of
most common founded allergen in patch test for ACD patient performed at Dermato-Venereology Clinic, dr.
Sardjito Central General Hospital, Yogyakarta from 2012-2016. The most common allergen was Nickel
Sulphate, Potassium dichromate, Cobalt chloride, Fragrance mix I and Fragrance mix II. Literally found that
primarily all of them are irritant, and secondary are sensitizer. Activity pattern dominantly as sensitizer were
showed by Nickel Sulphate, Potassium dichromate, Cobalt chloride for interpretation at 48-72 and 48-96
hours, where for Fragrance mix I and Fragrance mix II dominantly as a sensitizer was described for
interpretation at 48-72 hours and dominantly as irritant for 48-96 hours. Interpretation at 48-72-96 hours
continuously showed no specific allergen pattern.
1 INTRODUCTION
Contact allergies are complex diseases, and one of the
important challenges for public health and
immunology. It was still a challenge for medical
sciences to perform optimum management for the
patient. Contact dermatitis was divided to Allergic
Contact Dermatitis (ACD) and Irritant Contact
Dermatitis (ICD). 15–20% of the general population
was estimated suffered from contact allergy.
Workplace exposure, age, sex, use of consumer
products and genetic predispositions were identified
as the most important risk factors. (Peiser,2012). The
basic pathophysiology for this disease is
hypersensitivity mechanism especially type IV/ slow
onset type for the person who has experiencing
sensitization and elicitation previously and finally
show clinical manifestation, while ICD could be
suffered by any individual. ( Diepgen, 1999) ACD
was founded mostly on developing country where the
incidence rate is believed to be around 0.5±1.9 cases
per 1000 full-time workers per year.( English, 2004).
Each allergen has their own characteristic and differ
from each other and it was one of the factor which
caused variation on clinical manifestation for the
person who has been contacted to those allergen. The
characteristic / activity for chemical substance were
sensitizer and irritant, and each of them showed
different activity pattern where it was ascending for
sensitizer and descending for irritant on the patch test
interpretation result. Although contact dermatitis
uncommonly leads to hospitalization, and minor
degrees of contact dermatitis are often accepted as a
normal hazard of life, the occupational, domestic,
social and psychological implications may be
considerable. It must be assumed that the total
economic impact of ACD is very high. The research
was performed to describe allergen activity pattern
visible on interpretation of patch test result on ACD
patient at Dermato-Venereology clinic, dr. Sardjito
central general hospital, Yogyakarta from 2012-2016.
Satria, B., Waskito, F., Indrastuti, N., Mauliyasari, D. and Febriana, S.
Allergen Activity Pattern in Patch Test on Allergic Contact Dermatitis Patient at Dermato-Venereology Clinic, Dr. Sardjito Central General Hospital, Yogyakarta 2012-2016.
DOI: 10.5220/0008153801950198
In Proceedings of the 23rd Regional Conference of Dermatology (RCD 2018), pages 195-198
ISBN: 978-989-758-494-7
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
195

2 METHODS
This is a descriptive retrospective research using
medical record data from patients that have been
diagnosed as an ACD and have been performed patch
test in Dermato-Venereology clinic dr. sardjito
central general hospital Yogyakarta from 2012-2016
using standard serial patch test and listed for five of
the most common founded allergen. The listed
allergen was analyzed for its activity pattern showed
on patch test interpretation from 48, 72, 96 hours.
Each allergen was compared for its activity from 48
to 72 hours, 48 to 96 hours, and 48-72-96 hours then
calculated for percentage.
3 RESULTS
Five of most common founded positive allergen listed
were Nickel sulphate, Potassium dichromate, Cobalt
chloride, Fragrance mix I, and Fragrance mix II.
Interpretation on patch test result for Nickel sulphate,
Potassium dichromate, Cobalt chloride at 48-72 hours
and 48-96 hours showed dominantly sensitizer
pattern (ascended). Interpretation for Fragrance mix
I, and Fragrance mix II showed sensitizer pattern on
interpretation at 48-72 hours, while for interpretation
at 48-96 hours showed dominantly irritant pattern. No
specific dominant pattern was showed on
interpretation at 48-72-96 hours, as minimal
limitation score as sensitizer and irritant showed on
table 2.
4 DISCUSSION
The prevalence of contact allergy is rising worldwide.
This results in high costs for health care systems and
the economy as well as in an impairment of the
quality of life for the patients.(Nguyen, 2008),(
Kohl,2002), (Lunder, 2000). Contact dermatitis is
often localized on the hands, a highly visible area of
the body, thus drawing attention and causing
difficulties in social interaction. Jowett and Ryan
found that, in general, 38% of patients with eczema
noticed interference with social life ( Jowett,1985). In
a follow-up study of 954 patients with contact
dermatitis, 61% reported that they had lost time from
work due to their skin disease ( Mälkönen, 2009).
About 6% of all patients had been off work for longer
than 12 months continuously.
Each allergen or chemical substance has been
studied and analyzed then listed on some literation,
but visible clinical manifestation caused by those
allergen or chemical substance could be varied, and
not always as a result of its main characteristic. (
Thyssen,2007) In Europe about 20% of the general
population suffers from contact allergy to at least one
contact allergen. Most common are allergies to
nickel, fragrances and preservatives. Allergic
reactions to chromate and p-phenylenediamine (PPD)
are generally less common but occur frequently in
occupationally exposed subgroups of the population.
Contact dermatitis occurs twice as frequently in
women as in men and often starts at a young age, with
a prevalence of 15% in 12–16 year olds. (
Nosbaum,2009). Literally said that all of those
allergen most common founded positive on patch test
for ACD patient at Dermato-venereology clinic
central general hospital Yogyakarta 2012-2016 which
are Nickel sulphate, Potassium dichromate, Cobalt
chloride, Fragrance mix I and Fragrance mix II were
mainly irritant and sensitizer secondarily (ASTM,
2005), (Sciencelab, 2013), (Sheet,2009). Dominant
activity pattern as sensitizer showed on interpretation
on patch test result for Nickel sulphate, Potassium
dichromate, Cobalt chloride at 48-72 and 48-96
hours. Dominant activity pattern as sensitizer showed
on interpretation on patch test result for Fragrance
mix I and Fragrance mix II at 48-72 hours while
dominant activity pattern as irritant showed on
interpretation at 48-96 hours. Interpretation at 48-72-
96 hours continuously showed no specific allergen
pattern. Contact dermatitis is a pattern of
inflammatory response of the skin that may occur as
a result of contact with external factors (allergens,
irritants). The clinical picture is a polymorphic
pattern of inflammation of the skin characterized by a
wide range of clinical features like itching, redness,
scaling, erythema, vesiculation, and clustered
papulovesicles. In chronic cases, assuring,
hyperkeratosis, and lichenification occur. The variety
of morphologies and natural histories makes it
difficult to define a widely accepted, standardized
definition of the disease, which is needed to compare
epidemiological studies. (Diepgen,1999)
The difference on clinical manifestation could be
caused by combination of endogenous factor (atopic)
and exogenous factor (allergen concentration), and
the balance of sensitize and irritant activity. Skin
contact with irritants and/or allergens is a necessary
condition of contact
RCD 2018 - The 23rd Regional Conference of Dermatology 2018
196
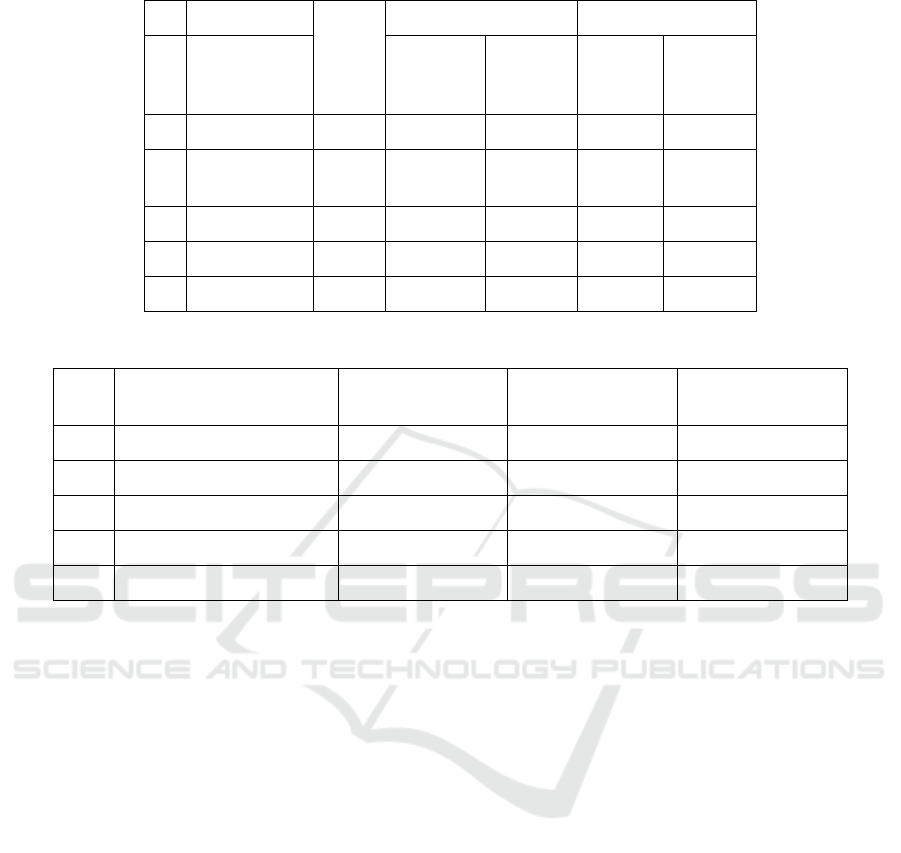
Table 1 Allergen activity pattern for interpretation on 2 timing comparation
No Allergen Case
number
48 and 72 hours pattern 48 and 96 hours pattern
Ascending
(case/
percent)
Descending
(case/
percent)
Ascending
(case/
percent)
Descending
(case/
percent)
1 Nickel sulphate 137 81 / 59,12 15 / 10,9 91 / 66,42 12 / 8,75
2 Potassium
dichromate
123 69 / 56,09 12 / 9,25 83 / 67,47 13 / 10,56
3 Cobalt chloride 98 48 / 48,9 10 / 10,2 32 / 32,65 21 / 21,42
4 Fragrance Mix I 88 42 / 47,72 15 / 17,05 13 / 14,77 41 / 46,59
5 Fragrance Mix II 87 43 / 49,42 3 / 3,44 14 / 16,09 39 / 44,82
Table 2 Allergen activity pattern for interpretation on 3 timing comparation (48-72-96)
No Allergen Ascending (case/
percent)
Descending (case/
percent)
Non Pattern (case/
percent)
1 Nickel sulphate 41 (29,92) 9 (6,56) 87 (63,50)
2 Potassium dichromate 37 (30,08) 4 (3,25) 82 (66,67)
3 Cobalt chloride 11 (11,22) 8 (8,16) 79 (80,61)
4 Fragrance Mix I 13(14,77) 9 (10,22) 66 (76,13)
5 Fragrance Mix II 21 (24,13) 2 (2,29) 64 (73,56)
dermatitis and the probability and severity of a
reaction depend on the type and intensity of exposure.
Additionally, apart from exposure to hazardous
substances, there are many endogenous factors that
may influence the development of contact dermatitis
other than atopic condition such as the condition of
the epidermal barrier, sensitization, psychological
factors, age, and gender. Environmental factors may
play a role in this process by influencing the
individual susceptibility and the characteristics of
exposure. A wide spread application of a weak
allergen or irritant is more likely to result in a high
proportion of cases than the use of a particularly
strong but rare agent. It should be noted that exposure
is characterized by concentration and duration. (
Diepgen,1999), (COENRAADS,1983) It should be
noticed that basically pathogenesis of ICD and ACD
start simultaneously. (Diepgen,1999)
Strategies for prevention of ACD include
identifying allergens and irritants, substituting
chemicals that are less irritating or allergenic,
establishing engineering controls to reduce exposure,
and organizing the work in a way that all employees
are exposed to the same degree. Personal protection,
such as gloves or barrier cream, has to be the last
choice, but is often resorted to in the first place. (Rea,
1967) Allergen activity pattern aid to describe the
characteristic of each allergen and to create the
prevention system and management. Further research
needed with attention on availability of atopic factor
and exact allergen concentration needed to caused
skin reaction on patch test to normal population
especially.
5 CONCLUSIONS
Data has showed that five of the most common
founded positive allergen on ACD patient that has
performed patch test in Dermato-venereology clinic
dr. sardjito central general hospital Yogyakarta from
2012-2016 were Nickel sulphate, Potassium
dichromate, Cobalt chloride, Fragrance mix I and
Fragrance mix II. Activity pattern dominantly as a
sensitizer was showed for Nickel sulphate, Potassium
dichromate, Cobalt chloride at 48-72 hours and 48-96
hours’ interpretation. Activity pattern dominantly as
sensitizer for Fragrance mix I and Fragrance mix II
was showed at 48-72 hours’ interpretation while for
48-96 hours show dominantly irritant pattern.
Interpretation for 48-72-96 hours continuously
Allergen Activity Pattern in Patch Test on Allergic Contact Dermatitis Patient at Dermato-Venereology Clinic, Dr. Sardjito Central General
Hospital, Yogyakarta 2012-2016
197

showed no specific dominant activity pattern. Further
research needed for assessment the atopic risk
factor’s influence and exact allergen concentration
needed for skin reaction on patch test for normal
population
ACKNOWLEDGEMENTS
Special thanks to Dr. Fajar
Waskito,Sp.KK(K),M.Kes for his idea and assistance
during the research, and also for DR.Dr. Niken
Indrastuti,Sp.KK(K), and Dr. Sri Awalia
Febriana,M.Kes, SP.KK, Ph.D, for their contribution
during this research. Hopefully that the result of this
research could be as a guidance for optimum
management of ACD through patch test
interpretation. None of the authors had a conflict of
interest
REFERENCES
ASTM., 2015. Standard Test Method for Accelerated Life
of Nickel-Chromium and Nickel-Chromium- Iron
Alloys for Electrical Heating 1. Vol. 90, Astm.
Coenraads, P. J., Nater, J. P., & Van der Lende, R., 1983.
Prevalence of eczema and other dermatoses of the
hands and arms in the Netherlands. Association with
age and occupation. Clinical and experimental
dermatology, 8(5), pp. 495-503.
Diepgen, T. L., & Coenraads, P. J., 1999. The epidemiology
of occupational contact dermatitis. International
archives of occupational and environmental
health, 72(8), pp. 496-506.
English, JSC., 2004. Occupational dermatoses: Overview.
Vol. 54, Occupational Medicine. p. 439–440.
Kohl, L., Blondeel, A., & Song, M., 2002. Allergic contact
dermatitis from cosmetics: Retrospective analysis of
819 patch-tested patients. In: Dermatology. p. 334–
337.
Jowett, S., & Ryan, T., 1985. Skin disease and handicap: an
analysis of the impact of skin conditions. Social science
& medicine, 20(4), pp. 425-429.
Lunder, T., & Kansky, A., 2000. Increase in contact allergy
to fragrances: patch-test results 1989–1998. Contact
Dermatitis, 43(2), pp. 107-109.
Mälkönen, T., Jolanki, R., Alanko, K., Luukkonen, R.,
Aalto-korte, K., Lauerma, A., & Susitaival, P., 2009. A
6-month follow-up study of 1048 patients diagnosed
with an occupational skin disease. Contact
Dermatitis, 61(5), pp. 261-268.
Nguyen SH, Dang TP, MacPherson C, Maibach H,
Maibach HI. 2008. Prevalence of patch test results from
1970 to 2002 in a multi-centre population in North
America (NACDG). Contact Dermatitis;58(2):101–6.
Nguyen, S. H., Dang, T. P., MacPherson, C., Maibach, H.,
& Maibach, H. I., 2008. Prevalence of patch test results
from 1970 to 2002 in a multi-centre population in North
America (NACDG). Contact dermatitis, 58(2), pp.
101-106.
Nosbaum A, Vocanson M, Rozieres A, Hennino A, Nicolas
J-F.2009. Allergic and irritant contact dermatitis. Eur J
Dermatol [Internet];19(4):325–32. Available
from:http://www.ncbi.nlm.nih.gov/pubmed/19447733
Peiser M, Tralau T, Heidler J, Api AM, Arts JHE, Basketter
DA, et al. 2012. Allergic contact dermatitis:
Epidemiology, molecular mechanisms, in vitro methods
and regulatory aspects. Vol. 69, Cellular and Molecular
Life Sciences. p. 763–81.
Rea JN, Newhouse ML, Halill AT.1976. Skin disease in
Lambeth A community study of prevalence and use of
medical care. Brit J prev soc Med.;30:107–14.
Sciencelab. 2013. Material Safety Data Sheet. Mater Saf
Data Sheet Ethyl Glycol MSDS.;4:4–9.
Sheet SD. 2009. Safety data sheet. ReVision [Internet];
40(1907):1–4. Available
from:http://wws.app.com.pl/files/File/MSDS/GB-
MSDS-090502.pdf
Thyssen JP, Linneberg A, Menné T, Johansen JD. 2007.
The epidemiology of contact allergy in the general
population--prevalence and main findings. Contact
Dermatitis;57(5):287–299.
RCD 2018 - The 23rd Regional Conference of Dermatology 2018
198
