
Correlation between Stress and Dermatology Life Quality Index in
Psoriasis Vulgaris Patients
Nyoman Suryawati, I. G. A. A. Praharsini, Irene Jessica Soputro
Department of Dermatology and Venereology, Faculty of Medicine Universitas Udayana, Sanglah Hospital, Bali,
Indonesia
Keywords: stress, DASS-21, DLQI, psoriasis vulgaris, cross-sectional study
Abstract : Psoriasis vulgaris is a chronic inflammatory disease of the skin comprising chronic relapse. This condition
has frequently caused discomfort, social stigma, psychological disorders such as depression, anxiety, and
stress affecting psoriasis vulgaris patients’ quality of life. This cross-sectional study aimed to identify
relationship between stress and quality of life in psoriasis vulgaris patients. Study sample included 42 psoriasis
vulgaris patients ranging from 16 to 65 years old during October-December 2017 period, fulfilling inclusion
and exclusion criteria. Stress was measured using Depression, Anxiety and Stress Scale-21 items (DASS-21)
scoring system, while quality of life was measured using Dermatology Life Quality Index (DLQI) scoring
system. Data was analyzed using SPSS 20 with Spearman’s Rho correlation test. The result showed most of
psoriasis vulgaris patients were male (69.05%), Balinese ethnic group (83.33%), senior high school graduate
(47.62%) and private sector employee (52.38%). Mean age of psoriasis patients was 45.93 ± 11.07 years old
with first onset ranging from 1 to 30 years and mean onset was 8.26 ± 7.6 years. Stress measurement using
DASS-21 found stress range between 0-42 and mean range was 10.81 ± 10.00. Quality of life measurement
using DLQI found score range between 0-23 and mean range was 10.74 ± 6.44. This study found stress as
risk factor of increased DLQI in psoriasis patients (PR 6.80, CI 95%; 0.96-48.33; p<0.05) and increased stress
score had positive correlation with DLQI (r=0.53; p<0.05). According to quality of life variable measurement,
stress was found to have positive correlation with symptoms and feelings (r=0.41; p<0.05) and daily activities
(r=0.38; p<0.05).
1 INTRODUCTION
Psoriasis is a chronic inflammatory disease of the skin
comprising chronic relapse. Psoriasis prevalence has
been reported variably between 0.1%-3% in various
population, with highest prevalence reported in
Denmark (2.9%), and low prevalence was reported in
Asia (0.4%) (Gudjonsson, 2012). Psoriasis is
characterized by presence of skin disorders such as
erythematous plaque covered by multiple layers of
thick white scales. Psoriasis vulgaris may cause
psychological disorders such as shyness, anxiety,
depression, stress, and social stigma reducing
patients’ quality of life (Gudjonsson, 2012), (Sharma,
2011), (Bhosle, 2006), (Basavaraj, 2011), (Nasren,
2008). Psoriasis affects patients’ quality of life which
may cause significant pressure on daily basis and
patients’ psychological morbidity (Basavaraj, 2011).
Stress is an individual condition caused by
environmental interaction considered as demand and
threat for the well-being of an individual. The cause
of stress is not only physical factors but also
emotional factors (Kenari, 2014). There are several
methods to measure stress, one of which is
Depression, Anxiety and Stress Scale (DASS). At
first, DASS scoring consisted of 42 questions, but
Lovibond and Lovibond (1995) created shorter
version composing 21 questions (DASS-21). DASS-
21 technique has been used frequently by
psychologists or clinicians because of its validity and
good reliability (Oei, 2013).
Quality of life defined as the ability to perform
daily activities according to an individual’s age and
role in the community. Quality of life measurement
of patients with skin disorder can be done using
Dermatology Life Quality Index (DLQI), a valid,
simple, and practical questionnaire (Bhosle, 2006).
.
Suryawati, N., Praharsini, I. and Soputro, I.
Correlation between Stress and Dermatology Life Quality Index in Psoriasis Vulgaris Patients.
DOI: 10.5220/0008150100310034
In Proceedings of the 23rd Regional Conference of Dermatology (RCD 2018), pages 31-34
ISBN: 978-989-758-494-7
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
31
Numerous studies had reported the relation
between psoriasis vulgaris severity and patients’
quality of life, but only few studies managed to
identify relation between stress and patients’ quality
of life along with other variables of psoriasis vulgaris
patients’ quality of life. This study aimed to identify
the relation between stress and quality of life in
psoriasis vulgaris patients.
2 METHODS AND RESULTS
This study used cross-sectional design with sample
number of 42 persons. Samples were recruited from
psoriasis patients visiting dermatology and
venereology clinic in Sanglah General Hospital,
fulfilling inclusion and exclusion criteria, during
October-December 2017 period. Psoriasis vulgaris
diagnosis was confirmed by anamnesis and physical
examination, and for doubtful cases, histopathology
examination was performed.
Stress level was measured using DASS-21
consisting 21 questions and each question comprising
7 questions to measure depression, anxiety, and
stress. In DASS-21, stress scale was sensitive to
chronic non-specific arousal. Each question was
scored from 0 to 3 and final score was obtained from
total score multiplied by two. Total score ranged from
0 to 42. Stress measurement were classified into
normal (score 0 – 10), mild (score 11- 18), moderate
(score 19 – 26), severe (score 27 – 34), and extremely
severe (score 35 – 42).
Quality of life measurement using DLQI
consisting 10 questions related to quality of life
variables including: symptoms and feelings, daily
activities, leisure, work or school, personal
relationships and treatment filled by patients. DLQI
score was attained by adding 4 point to each variable
scoring from 0 to 3. Total score ranged from 0 to 30.
Highest score indicated great influence to
patients’ quality of life (Bhosle, 2006).Data was
processed using SPSS 20 software. Descriptive
analysis was performed to identify subjects’
characteristics. Data normality test was performed
using Kolmogorov-Smirnov. Correlation between
stress and DLQI as well correlation between stress
and each quality of life variable were analyzed using
Spearman’s Rho test. Statistical analysis was
considered significant when p<0.05.
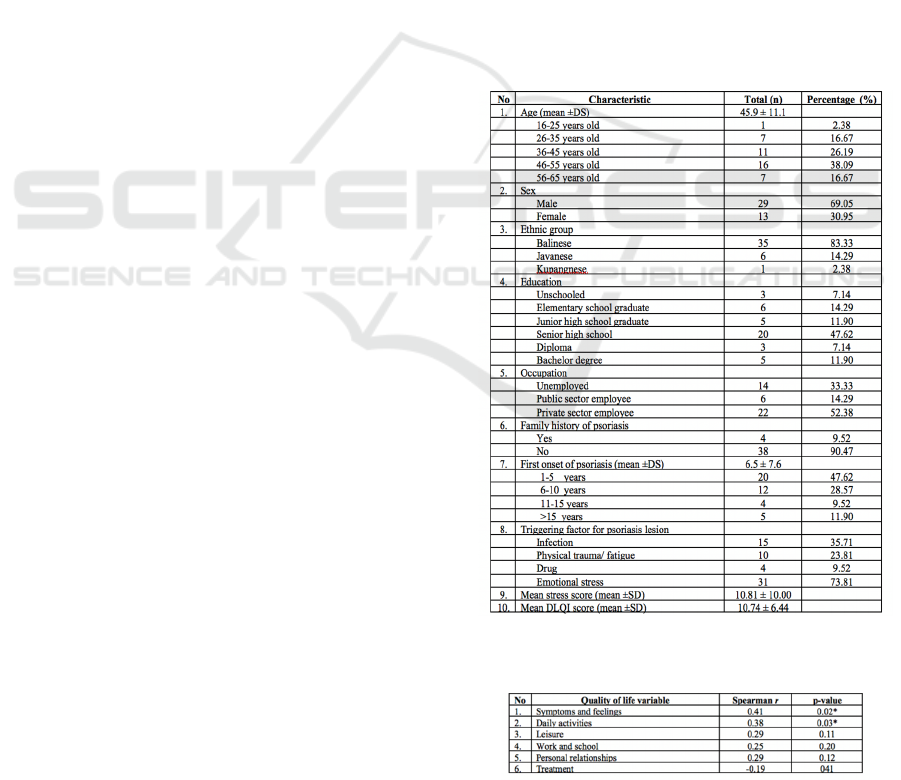
Psoriasis patients involved in this study were 42
persons, including 29 males (69.05%) and 13 females
(30.95%), Balinese ethnic group (83.33%), senior
high school graduate (47.62%) and private sector
employee (52.38%). Mean age of psoriasis patients
was 45.93 ± 11.07 years old with first onset ranging
from 1 to 30 years and mean onset was 8.26 ± 7.6
years. Family history of psoriasis was found in 4
patients (9.52%) with stress as the most common
triggering factor found in 31 patients (73.81%). Stress
measurement using DASS-21 found stress range
between 0-42 and mean range was 10.81 ± 10.00.
Quality of life measurement using DLQI found score
range between 0-23 and mean range was 10.74 ± 6.44
(Table 1).
This study identified stress as risk factor of
decreased quality of life in psoriasis patients (PR
6.80, CI 95%; 0.96-48.33; p<0.05). Increased stress
score had positive correlation with decreased
patients’ quality of life (r=0.53; p<0.05) shown in
Figure 1. According to quality of life variable
measurement, stress was found to have positive
correlation with symptoms and feelings (r=0.41;
p<0.05) and daily activities (r=0.38; p<0.05) (Table
2).
Table 1. Characteristic of the subject
Table 2. Correlation between stress and each quality of life
variable
RCD 2018 - The 23rd Regional Conference of Dermatology 2018
32
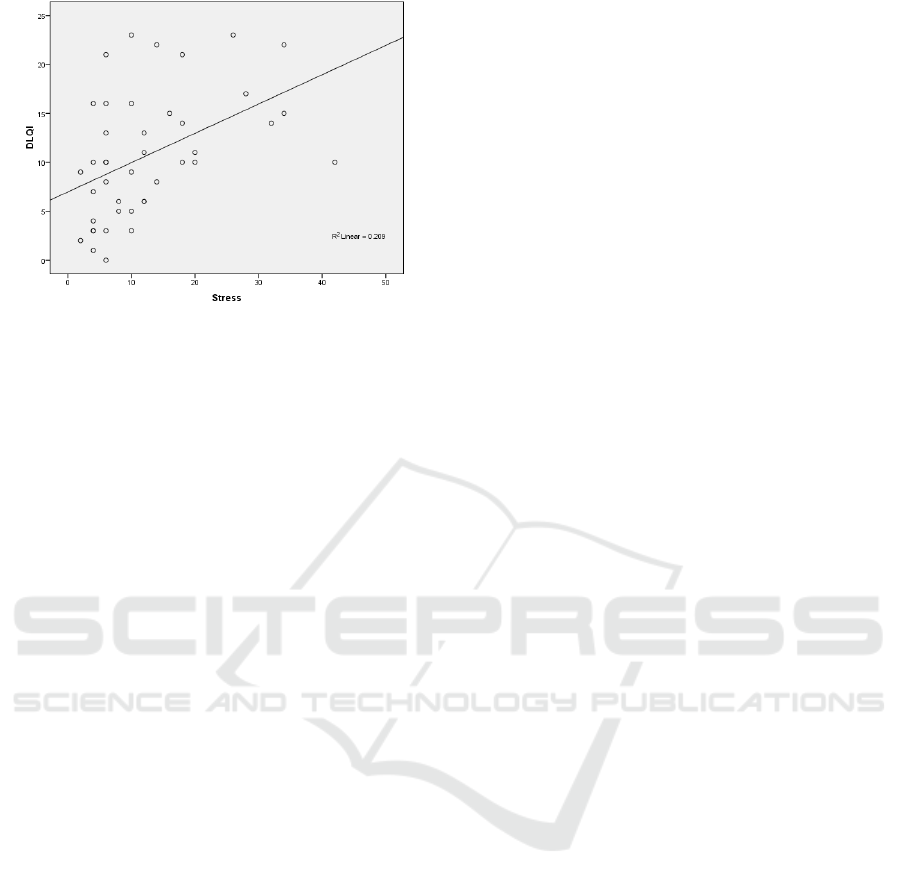
Figure. 1. Scattered plot graphic of correlation between
stress and D
3 DISCUSSION
In this study, mean age of psoriasis patients was 45.93
± 11.07 years old. This result was consistent with
previous study in India (2014) stating mean age of
psoriasis patients was 49.45 ± 14.8 years old, as well
similar study in Croatia (2013) with mean age of 49.9
± 14.8 years old. Psoriasis can affect individuals of all
ages although it tends to occur in adults rather than
children and its incidence decreases in elderly.
Several previous studies showed increased psoriasis
incidence with age. Psoriasis incidence increases over
the age of 39 years old and it is predicted to decline
during elderly (Parisi, 2013).
This study found majority of psoriasis patients
were males comprising as many as 29 persons
(69.05%). This result was consistent with studies in
Taiwan (2013) and China (2013) obtaining psoriasis
vulgaris events were more common in male than in
female patients with a ratio of 2:1 (Tseng, 2013),
(Wu, 2013). Generally, it was known that psoriasis
number of events was almost the same both in male
and female patients. There has been no evidence
showing phenotype difference of psoriasis vulgaris in
both sexes (Griffiths, 2010).
Genetics was alleged to play role in pathogenesis
of psoriasis vulgaris. From this study, family history
of psoriasis was found in 4 patients (9.52%). This
result was consistent with Shobaili, et al study
identifying family history of psoriasis in 8.4%
patients (Alshobaili, 2010).
In this study, stress was found to be a triggering
factor for psoriasis lesion in 31 patients (73.81%).
Stress is one of triggering factors for exacerbation of
psoriasis lesion and approximately 40-80% psoriasis
vulgaris exacerbation is caused by stress. Severe
psoriasis vulgaris condition may cause stress,
meanwhile stress is able to worsen psoriasis
symptoms (Basavaraj, 2011). Stress can aggravate
psoriasis vulgaris condition and prolong healing time
of the disease. Stress effect on psoriasis vulgaris
exacerbation is possibly mediated by immunology
effect involving hypothalamus-pituitary-adrenal
(HPA) axis and increase in reactivation of
sympathetic adrenomedular (SAM) leading to
activation of mast cells which cause neurogenic
inflammation (Basavaraj, 2011), (Cohen, 2007),
(Coimbra, 2014). Psychological stress causes
phenotypic changes in circulating lymphocyte and
considered as important trigger for T-helper1 cell-
polarized inflammatory in psoriasis (Basavaraj,
2011).
Measurement of mean stress score was 10.81 ±
10.00 and mean DLQI score was 10.74 ± 6.44. Stress
score had moderate correlation with DLQI, r=0.53;
p<0.05 which showed that higher DLQI score
indicated higher patients’ stress level measured by
DASS-21. In this study, positive correlation between
stress and quality of life variables such as symptoms
and feelings (r=0.41; p<0.05) and daily activities
(r=0.38; p<0.05) were identified. Those results
showed that higher stress level had greater effect on
both symptoms and feelings and daily activities
variables in psoriasis vulgaris patients.
4 CONCLUSION
Stress affected quality of life in psoriasis patients.
This study found higher stress level had greater effect
on patients’ quality of life, particularly in symptoms
and feelings, and daily activities variables. According
to the results of this study, it is concluded that
screening for stress as triggering factor of psoriasis
vulgaris is essential, thus prompt treatment for stress
can be performed which eventually leads to increased
quality of life in psoriasis vulgaris patients.
ACKNOWLEDGEMENT
We gratefully thank all of the patients for agreeing to
participate in our study.
REFERENCES
Al-Shobaili, H.A., Shahzad, M., Marshood, A.A., Khalil,
A., Settin, A., & Barrimah, I., 2010. Genetic
Correlation between Stress and Dermatology Life Quality Index in Psoriasis Vulgaris Patients
33

Background of Psoriasis. International Journal of
Health Sciences, 4, 23-29.
Basavaraj, K.H., Navya, M.A., & Rashmi, R., Stress and
quality of life in psoriasis: an update. International
journal of dermatology, 50(7), 783-792.
Bhosle, M.J., Kulkarni, A., Feldman, S.R., Balkrishnan, R.,
2006. Quality of life in patients with psoriasis. BioMed
Central, pp. 1-7.
Cohen, S., Deverts, D., Miller, G., 2007. Psychological
Stress and Disease. Journal American Medical
Association, 298, pp. 1485-1487.
Coimbra, S., & Silva, A., 2014. Biomarker of psoriasis
severity and therapy montoring. World Journal
Dermatology, 3, 15-20.
Griffiths, C., Barker, J.N.W.N., Psoriasis. In: Burn T,
Stephen B, Cox N. Editors. Rook’s Textbook of
Dermatology. 8th ed. Brithis: Wiley-Blackwell; 2010.
p. 20.1-.60.
Gudjonsson, J.E., Elder, J.T., Psoriasis. In: Goldsmith LA,
Katz SI, Gilchrest BA, editor. Fitzspatrick's
Dermatology in General Medicine. 8 th ed. New York:
McGraw-Hill; 2012. p. 197-231.
Kenari, M.A., 2014. A prospective study on the assessment
of level of depression, anxiety and stress among
teaching faculties of a Nursing college. American
Journal of Nursing Science, 3, pp. 43-47.
Nasren, S., Ahmed, I., Effendi, S., 2008. Frequency and
magnitude of anxiety and depression in patients with
psoriasis vulgaris. Journal of The College of Physicians
and Surgeons Pakistan, 18, pp. 397-400
Oei, T.P.S., Sawang, S., Goh, Y.W., Mukhtar, F., 2013.
Using the Depression Anxiety Stress Scale 21 (DASS-
21) across cultures. International Journal of
Psychology, pp. 1-24.
Parisi, R., Deborah, P.M., Christopher, E.M., Ashcroft,
D.M., 2013. Global epidemiology of psoriasis: A
Systematic review of incidence and prevalence. Journal
of Invest Dermatology, 133, pp. 377-385.
Sharma, S., Bassi, R., Singh, A., 2011. A comparative study
of depression and anxiety in psoriasis and other chronic
skin disease. Journal of Pakistan Association of
Dermatologists, 21, pp. 235-240.
Tseng, H.W., Lin, H.S., Lam, H.C., 2013. Co-morbidities
in psoriasis: a hospital based case control study Journal
of the European Academy of Dermatology and
Venereology, 27, pp. 1411-1425.
Wu, Y., Lu, Z., Chen, Y., Xue, F., Chen, X., Pan, M., &
Zheng, J., 2013. Association of IL-12B Gene
rs6887695 Polymorphism with Hereditary
Susceptibility and Clinical Characterization of Psoriasis
Vulgaris in the Chinese Han Population. Archives of
Dermatological Research, 305, pp.477-482.
RCD 2018 - The 23rd Regional Conference of Dermatology 2018
34
