
Wandering Analysis with Mobile Phones
On the Relation Between Randomness and Wandering
Agusti Solanas
1
, Edgar Batista
1
, Frederic Borras
1
, Antoni Mart
´
ınez-Ballest
´
e
1
and Constantinos Patsakis
2
1
Smart Health Research Group, Dept. of Computer Engineering and Mathematics,
Universitat Rovira i Virgili, Catalonia, Spain
2
Department of Informatics, University of Piraeus, Piraeus, Greece
Keywords:
Behaviour Analysis, Wandering, Randomness, Elderly.
Abstract:
Population pyramids have rapidly changed their shape worldwide. Specially in industrialised countries, where
a steady ageing process is taking place. Due to the ageing of the population, age-related illnesses such as
mild cognitive impairment (MCI) and dementia are becoming commonplace and healthcare systems struggle
to improve the quality of life of patients and carers. Wandering and disorientation are common symptoms
amongst patients with MCI, and they could lead to fatal outcomes. In this article we propose a wandering
detection technique based on the analysis of randomness in patients’ trajectories, which are gathered by means
of standard low-cost mobile phones with GPS.
1 INTRODUCTION
The average age of the world population has in-
creased progressively over the last 50 years as a re-
sult of the reduction of fertility and an increase in
life expectancy. The ageing of the population poses
a formidable challenge for public healthcare systems
since they have to face the rise of an aged and very de-
manding population and their associated health condi-
tions, namely chronic illnesses, injuries and disabili-
ties.
This demographic change results in a huge impact
on society and proper countermeasures have to be put
in place so as to cope with it in the years to come.
The aforementioned ageing of the population leads
to an increase in the cases of cognitive disorders like
Mild Cognitive Impairment (MCI), Parkinson’s dis-
ease (PD) and Alzheimer’s disease (AD), to name the
most common.
MCI is specially interesting because it can be un-
derstood as a precursor of early stages of AD and
PD and other types of early dementia that imply im-
paired memory function whilst the cognitive function
is generally preserved (Petersen et al., 2001). MCI
is a brain function syndrome involving the onset and
evolution of cognitive impairments beyond those ex-
pected based on the age and education of the indi-
vidual, but which are not significant enough to inter-
fere with their daily activities (Petersen et al., 1999).
Annual prevalence estimates for MCI in the United
States range from 3% to 4% in the eighth decade
in the general population. Amongst community-
dwelling African Americans, the estimated preva-
lence is 19.2% for those aged 65 − 74 years, 27.6%
for those aged 75 − 84 years, and 38% for those aged
85 years and older. The prevalence of mild cogni-
tive impairment increases with age. The prevalence
is 10% in those aged 70 − 79 years and 25% in those
aged 80 −89 years.
People suffering from MCI and early stages of dif-
ferent types of dementia might experience a decrease
in their cognitive capabilities that might affect their
mobility patterns but they still have considerably high
degrees of autonomy (i.e. they can live alone, walk,
exercise). The most apparent impairment is related
to their memory function: patients might become
spatially and temporally disoriented, and might have
problems in finding their way home, or they could
forget to accomplish tasks. As a result of the mem-
ory function impairment, patients suffering from MCI
might follow strange trajectory patterns and wander.
Amongst all symptoms related to MCI, namely
memory loss, disorientation, wandering, anxiety, etc.
Wandering is one of the most frightening for relatives
and carers. People that wander might easily get lost
and, as a result, they could put their lives in jeop-
168
Solanas A., Batista E., Borras F., Martínez-Ballesté A. and Patsakis C..
Wandering Analysis with Mobile Phones - On the Relation Between Randomness and Wandering.
DOI: 10.5220/0005329601680173
In Proceedings of the 5th International Conference on Pervasive and Embedded Computing and Communication Systems (PECCS-2015), pages
168-173
ISBN: 978-989-758-084-0
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

ardy. In this article, we focus on detecting wander-
ing/disorientation patterns in trajectories gathered by
GPS-enabled mobile phones.
The rest of the article is organised as follows:
Next, in Section 2 we provide some basic background
and an overview of related work. In Section 3 we
introduce our method to detect wandering and disori-
entation and show that there exists a relation between
the amount of randomness in trajectories and the ap-
pearance of abnormal patterns. Next, in Section 4 we
describe our initial experiments with real patients and
provide an illustrative example with real data. Finally,
the article concludes in Section 5 with some final re-
marks and lines for further research.
2 RELATED WORK
Research related to the provision of health services
by means of electronic devices is very wide. With the
aim to provide the reader with a basic background,
in Section 2.1 we elaborate on electronic health (e-
health) and mobile health (m-health), next in Sec-
tion 2.2 we recall the SIMPATIC Project to illustrate a
novel and recent initiative to provide intelligent mon-
itoring of people with MCI.
2.1 e-Health and m-Health
The healthcare sector has adopted the so-called in-
formation and communication technologies (ICT)
and, as a result, the concept of electronic health (e-
health) (Eysenbach, 2001) appeared. e-Health is con-
tributing to the reduction of costs and the increase
of efficiency. ICT might be used for a variety of
health-related tasks, namely communication between
patients, doctors and carers, distant provision of care,
remote support to diagnostic, EHR, medication adher-
ence control, etc. e-Health substantially reduces the
displacements of professionals and patients, globally
brings down the cost of medical resources, and makes
treatments and health watchfulness more comfortable
to patients.
After the consolidation of e-health, the general-
ized utilisation of mobile devices with GPS, or other
self-localisation capabilities, (e.g., smartphones) gave
birth to the idea of mobile health (m-health). There is
no doubt about the huge potential of m-Health since
it adds to the advantages of e-health all the benefits
related to the ubiquity of mobile devices (i.e., global
monitoring capabilities, wide availability and imme-
diacy).
Mobile health (m-health) can be defined as the
discipline founded on the use of mobile communi-
cation devices in medicine, or more specifically, the
delivery of healthcare services via mobile commu-
nication devices, or: “Emerging mobile communi-
cations and network technologies for healthcare sys-
tems” (Istepanian et al., 2006). The use of mobile
devices helps to perform tasks more efficiently. Espe-
cially the remote monitoring of patients and the com-
munication between professionals, relatives and pa-
tients will highly benefit from m-health. m-Health
extends the capabilities of indoor monitoring environ-
ments and it is a powerful tool that allows the ad-
vance of several lines of research, namely the con-
tinuous assessment of the state of patients, the early
detection of emergency situations, the detection of
changes in health conditions, the detection of abnor-
mal situations, the early detection of fragile situations,
etc. Some interesting examples of m-health applica-
tions can be found in (Solanas et al., 2013)(Postolache
et al., 2012)(Foundation, 2013).
2.2 The SIMPATIC Project
It is apparent that continuous surveillance can help
people with mild cognitive impairments (MCI) and
dementia but, current methods have several limita-
tions: (i) surveillance could be seen as a serious pri-
vacy invasion (Mart
´
ınez-Ballest
´
e et al., 2013), (ii)
monitoring is not autonomous and, (iii) abnormal be-
havioural patterns are neither analysed nor detected.
With the aim to avert some of these limita-
tions, the SIMPATIC project (Mart
´
ınez-Ballest
´
e and
Solanas, 2014), has developed a new intelligent and
autonomous system that monitors the location of pa-
tients, who suffer from MCI. Figure 1 shows some
screenshots of the SIMPATIC Project web-based con-
trol environment.
The system behaves autonomously (without the
need for user intervention) and also intelligently (i.e.
it learns from the users and adapts to their be-
haviours), also it is able to detect abnormal users’ be-
haviours. In addition, the system reacts to risky situa-
tions, namely the user is in a dangerous area (e.g. the
edge of a cliff), he/she is not moving for a long time,
he/she is wandering, etc. The SIMPATIC Project,
which is currently ongoing, is collecting location data
from several patients diagnosed with MCI. Specially,
it is focussed on people diagnosed with GDS-3 and
GDS-4
1
.
3 WANDERING ANALYSIS
The act of wandering is defined as walk or move in
1
Global Deterioration Scale (GDS)
WanderingAnalysiswithMobilePhones-OntheRelationBetweenRandomnessandWandering
169

Figure 1: Screenshots of the web-based control interface of
the SIMPATIC Project. From top to bottom: Users regis-
tration page, Trajectory monitoring and filtering page and,
alarms log page.
leisurely or aimless way or, travel aimlessly through
or over an area. This behaviour appears in people with
MCI and, if it is properly detected, it could alleviate
further risks of suffering serious injuries as a result of
the disorientation. Our main aim is to propose an au-
tomatic method that can detect wandering by means
of analysing the mobility patterns of monitored pa-
tients.
Our assumption, that we aim to discuss next, is
that trajectories that contain wandering patterns have
more randomness than trajectories free of wandering
or disorientation. Next, we discuss the rationale be-
hind this assumption and we propose a method to
analyse the degree of randomness of a trajectory by
means of graph cycles analysis.
3.1 Rationale
Impairments in memory function, typical in people
with MCI, could translate into abnormal mobility pat-
terns, for example, patients will follow strange paths
to reach their homes, or they will go to the supermar-
ket more frequently (because they forget to buy what
they need).
These abnormal mobility patterns can be seen as
short-length cycles present in the trajectories of pa-
tients (e.g. disoriented patients going home might
walk around their block until they find the right en-
trance). On the contrary, trajectories that are clearly
guided (i.e. without disorientation) will have long cy-
cles (e.g. patients leave their home, go to the cinema,
and go back home).
Thus, our goal is to design a system that allows
us to detect the percentage of short and long cycles in
the trajectories of patients. Then, if our system detects
short cycles it could raise a wandering alarm.
3.2 Wandering and Randomness
With the aim to shed some light over our assumption,
we have simulated several trajectories with a variable
amount of randomness, and then we have analysed
the number and length of the cycles found in those
trajectories.
Figure 2 shows three trajectories that we will use
as examples to illustrate our point. In the first trajec-
tory (Figure 2-left) we have defined three locations
and we have simulated a regular, deterministic way
to reach them and go back to the origin. Since we
are considering a regular squared grid, at every given
location, the next move is selected amongst 8 possi-
bilities so that the distance to the destination is min-
imised. In the second trajectory (Figure 2-centre), at
each step of the trajectory, we have a 0.5 probabil-
ity of choosing a random move and 0.5 probability of
moving like in the first trajectory. Finally, the third
trajectory is completely random (i.e. at every step of
the trajectory, the next move is chosen uniformly at
random from the possible eight options).
Once the three trajectories are simulated, they are
represented as a graph G = {V, E}. Where V , the ver-
texes, are the center of each cell of the grid and E, the
edges, are the transitions from one cell to the next.
After creating each graph, we apply an algorithm
to determine the number and length of Eulerian cy-
cles. This way, we detect cycles of length
2
2, 3, ... and
we count how many cycles of each length are found.
This information if plotted in Figure 3.
2
The lenght is measured as the number of nodes in the
cycle.
PECCS2015-5thInternationalConferenceonPervasiveandEmbeddedComputingandCommunicationSystems
170
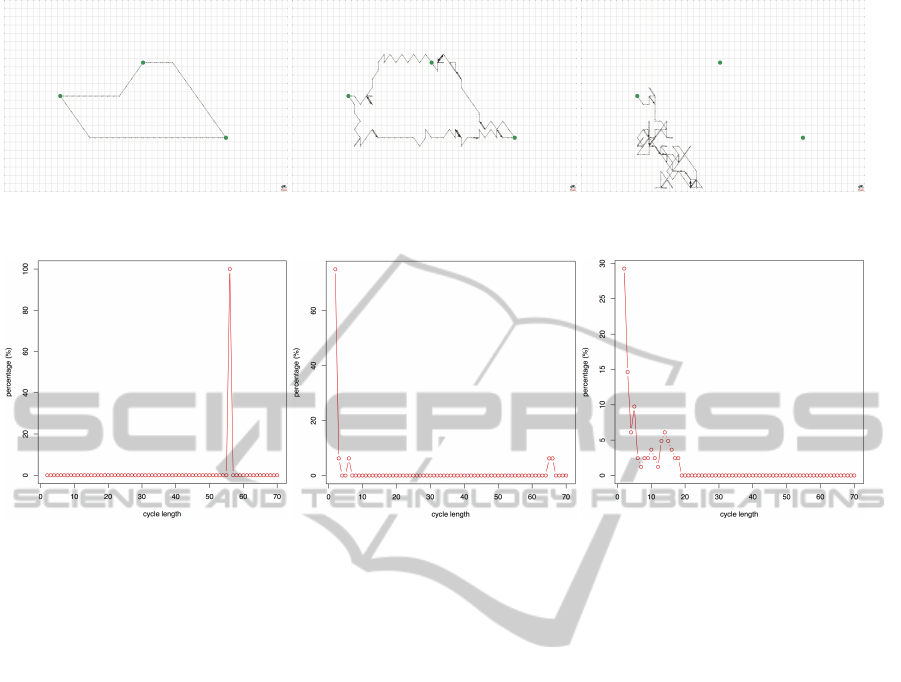
Figure 2: Simulated trajectories. From left to right: deterministic trajectory, semideterministic trajectory with 0.5 random
probability and, random trajectory.
Figure 3: Percentages of cycles depending on their length. From left to right: cycles for the deterministic trajectory, cycles
for the semideterministic trajectory and, cycles for the random trajectory.
It can be observed that the first trajectory (with 0
probability of randomness) has a single cycle with a
length of 56 steps. Thus, 100% of cycles are long.
In the second case (with 0.5 probability of random-
ness), there is a large number of cycles of short length
(90%), whilst only 10% are long. A similar result
is obtained with the third trajectory (with 1 probabil-
ity of randomness) and 100% of the found cycles are
short.
From these preliminary experiments, it could be
inferred that adding randomness to a guided trajec-
tory leads to an increase in the number of short cycles.
Thus, although it has not been proven with statisti-
cally sound experiments, we aim to use our assump-
tion to detect wandering by analysing the percentage
of short cycles in a graph.
4 INITIAL RESULTS WITH REAL
PATIENTS
With the aim to test our proposal with real patients
(within the SIMPATIC Project), we have collected
the trajectories of people diagnosed with MCI and we
have analysed their behaviour. To do so, we have se-
lected a group of 15 people aged from 65 to 83 di-
agnosed with MCI (GDS-3, GDS-4). Each patient
has been provided with a mobile phone equipped with
GPS and a data plan to send their data to our central
server every three minutes. The procedure illustrated
in Figure 4 works as follows:
First, our server receives raw data from the pa-
tients’ smartphones every three minutes and stores
them in a MySQL database. Each packet of data con-
tains the latitude and longitud provided by the GPS, a
time-stamp, the values of the accelerometers, the state
of the smartphone battery and the temperature. Next,
every 15 minutes the data are converted from the op-
erational MySQL database into a strategic PostGIS
database with a PHP script. Once we have the infor-
mation in the PostGIS database, we study it and we
find the number of cycles of the patient’s route with
a Java program and an API library (designed ad-hoc).
After obtaining the results, they are sent for visuali-
sation and further analysis to three different outputs,
namely a web viewer to use OpenStreetMaps, R to
plot the results of cycles and Pajek to plot the result-
ing graphs, G, of the trajectories.
For the sake of clarity we include an example of
the results obtained with a real patient. In Figure 5
(left) we show a trajectory followed by a patient dur-
ing 3 days in the area of Tarragona. Figure 5 (right)
depicts the graph created by our system. This graph is
analysed to determine the number and length of cycles
and the results are shown in Figure 6 (20x20 meters
cells are considered).
WanderingAnalysiswithMobilePhones-OntheRelationBetweenRandomnessandWandering
171
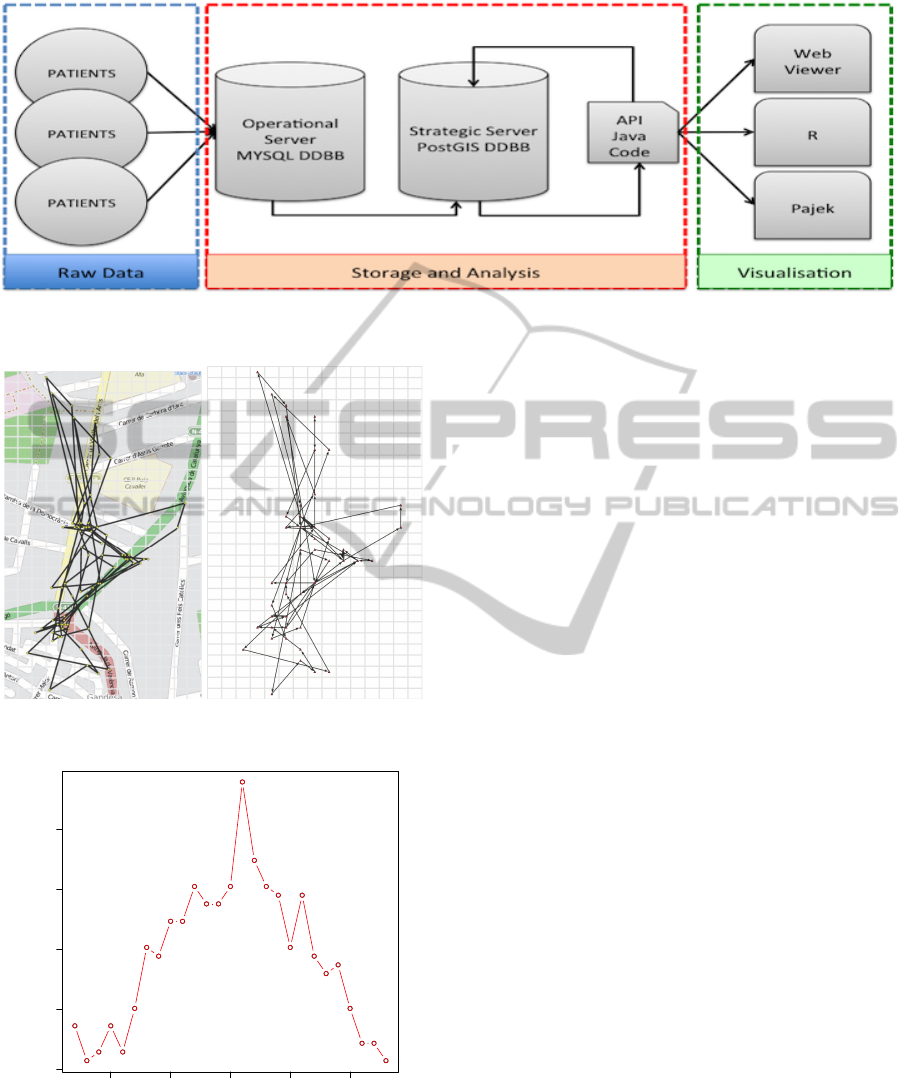
Figure 4: Data flow scheme of our proposal. First the raw data are collected from patients, then they are stored and analysed
in our servers, and finally the data are visualised in Open Street Maps, R and Pajek.
Figure 5: Trajectory and graph of a real volunteer patient of
the SIMPATIC project pilot test.
5 10 15 20 25
0 2 4 6 8
cycle length
percentage (%)
Figure 6: Results of the cycles analysis of the above trajec-
tory/graph.
It can be observed that the percentage of short cy-
cles (under 7, 8 steps) is very low and most of the
detected cycles have lengths between 12 and 18 cy-
cles. These results indicate that the patient behaved
normally during the analysed days, which was con-
firmed by directly asking the patient.
At the time of writing this article, we are still col-
lecting data and the pilot test is ongoing. However, to
the date, the system has been able to properly identify
alarms and the initial results for wandering detection
(as stated in this article) seem very promising.
5 CONCLUSIONS AND OPEN
RESEARCH LINES
Wandering is a serious problem for people suffering
from MCI and first stages of dementia. In this article
we have proposed the idea of studying the existence
of wandering behaviours by means of analysing the
randomness of the trajectories by counting the num-
ber of Eulerian cycles and their lengths.
Although there are still many techniques to be
studied and compared (Lin et al., 2014), the experi-
mental results support our claim that there is a rela-
tion between the amount of randomness and the pres-
ence of wandering. Also, it has been shown that there
is an initial evidence to think that the percentage of
short-cycles in a graph might be a good indicator of
the randomness of a trajectory.
Currently, the presented solution is used in a pi-
lot test within the context of the SIMPATIC project
with volunteers in the Tarragona area. Although the
project is already providing interesting results and a
good service to patients and carers, there are many
open research lines that will deserve further study in
the years to come and are briefly listed as follows:
• Tuning the System. Although the proposed solu-
tion is operative and is currently being tested with
real patients, there is still a lot of work to do to
improve its resilience. Also, there are a number
PECCS2015-5thInternationalConferenceonPervasiveandEmbeddedComputingandCommunicationSystems
172

of parameters that have to be carefully tuned. It
would be desirable to have an automatic system
that determines the values of these parameters and
adapts them to the needs of each patient.
• The Smart Health Paradigm. The process of
urbanisation is concentrating most of the pop-
ulation in cities. Those cities that are hosting
a very demanding population need to improve
their way of managing resources to guarantee a
proper and sustainable living. As a result, smart
cities have appeared (P
´
erez-Mart
´
ınez et al., 2013).
The use of ICT in smart cities aiming at im-
proving a variety of services and providing new
solutions has gained importance. It seems nat-
ural that also health services might be offered
within the context of a smart city: intelligent sys-
tems fed with data collected from sensors, users
and mobile devices, etc, pave the way for the
emergence of new services related to health and
well-being. Hence, the concept of smart health
(s-health) arises (Solanas et al., 2014). Using
the sensing and context-aware infrastructures of
smart cities allows the collection of personalised
data that will help to improve our system.
• Recommender Systems. Using the experience
of other users/patients to predict the behaviour of
new patients is an interesting new approach that
will be used by our system in the near future. Col-
laborative Filtering (Casino et al., 2013b)(Casino
et al., 2013a) systems are good candidates to be
studied and we plan to use them to predict possi-
ble erratic behaviour of patients.
• Psychological Analysis. Although our system is
centred in patients. We are very much interested
in the benefits that it can provide to carers and rel-
atives. At the time of writing this lines, we are
analysing which are the effects of using our sys-
tem on the reduction of anxiety and stress of car-
ers and relatives. Preliminary results indicate that
carers feel less stress because they trust the system
that allows them to locate patients if they get lost
or disoriented. Further studies have to be carried
out to confirm these initial findings.
ACKNOWLEDGEMENTS
The authors are partly funded by La Caixa through
project “SIMPATIC” RECERCAIXA’12, and by the
Government of Catalonia under grant 2014 SGR 537.
REFERENCES
Casino, F., Domingo-Ferrer, J., Patsakis, C., Puig, D., and
Solanas, A. (2013a). Privacy preserving collaborative
filtering with k-anonymity through microaggregation.
In ICEBE, pages 490–497.
Casino, F., Patsakis, C., Puig, D., and Solanas, A. (2013b).
On privacy preserving collaborative filtering: Current
trends, open problems, and new issues. In ICEBE,
pages 244–249.
Eysenbach, G. (2001). What is e-health? Journal of Medi-
cal Internet Research, 3(2):e20.
Foundation, U. N. (2013). mhealth alliance. Website.
http://www.mhealthalliance.org/about.
Istepanian, R., Laxminarayan, S., and Pattichis, C. S.
(2006). M-Health: Emerging Mobile Health Systems,
chapter Preface. Topics in Biomedical Engineering.
International Book Series. Springer.
Lin, Q., Zhang, D., Chen, L., Ni, H., and Zhou, X. (2014).
Managing elders wandering behavior using sensors-
based solutions: A survey. International Journal of
Gerontology.
Mart
´
ınez-Ballest
´
e, A., P
´
erez-Mart
´
ınez, P. A., and Solanas,
A. (2013). The pursuit of citizens’ privacy: A privacy-
aware smart city is possible. IEEE Communications
Magazine, 51(6).
Mart
´
ınez-Ballest
´
e, A. and Solanas, A. (2014). The SIM-
PATIC project. http://projecte-simpatic.cat.
P
´
erez-Mart
´
ınez, P. A., Mart
´
ınez-Ballest
´
e, A., and Solanas,
A. (2013). Privacy in smart cities - a case study of
smart public parking. In PECCS, pages 55–59.
Petersen, R., Doody, R., Kurz, A., Mohs, R., Morris, J.,
Rabins, P., Ritchie, K., Rossor, M., Thal, L., and Win-
blad, B. (2001). Current concepts in mild cognitive
impairment. Archives of Neurology, 58(12):1985 –
1992.
Petersen, R., Smith, G., Waring, S., Ivnik, R., Tangalos,
E., and Kokmen, E. (1999). Mild cognitive impair-
ment: clinical characterization and outcome. Archives
of Neurology, 56(3):303 – 308.
Postolache, G., Gir
˜
ao, P., and Postolache, O. (2012). Perva-
sive and Mobile Sensing and Computing for Health-
care - Technological and Social Issues, chapter Re-
quirements and Barriers to Pervasive Health Adop-
tion. Spriger.
Solanas, A., Martinez-Balleste, A., Perez, P. A., Fernan-
dez, A., and Ramos, J. (2013). m-carer: Privacy-aware
monitoring for people with mild cognitive impairment
and dementia. Selected Areas in Communications,
IEEE Journal on, 31(9):19–27.
Solanas, A., Patsakis, C., Conti, M., Vlachos, I. S., Ramos,
V., Falcone, F., Postolache, O., P
´
erez-Mart
´
ınez, P. A.,
Pietro, R. D., Perrea, D. N., and Mart
´
ınez-Ballest
´
e,
A. (2014). Smart health: A context-aware health
paradigm within smart cities. IEEE Communications
Magazine, 52(8):74–81.
WanderingAnalysiswithMobilePhones-OntheRelationBetweenRandomnessandWandering
173
