
TheraDrive in a Robot Gym
Toward Stroke Rehabilitation beyond Inpatient Rehabilitation Settings in USA and
Mexico
Michelle J. Johnson
1-3
, Sandra Montes
4
and Karla Bustamante
3,4
1
Department of Physical Medicine and Rehabilitation, University of Pennsylvania, Philadelphia, PA, U.S.A.
2
Department of Biomedical Engineering, University of Pennsylvania, Philadelphia, PA, U.S.A.
3
Department of Biomedical Engineering, Marquette University, Milwaukee, WI, U.S.A.
4
Biomedical Engineering, ITESM, Campus Chihuahua, Heroico Colegio Militar, 4700,Chihuahua, Mexico
Keywords: Game Therapy, Haptics, Motivation, Stroke Rehabilitation, Robotics, Upper Limb.
Abstract: Affordable stroke rehabilitation approaches can maximize the functional independence of stroke survivors
discharged after inpatient and outpatient services and improve access to rehabilitation for low-resource
environments. This paper briefly describes the evolution of the Theradrive system and its novel use in a
robot therapy gym in Mexico, where it was one of 6 devices aimed at improve motor function after stroke.
Results from testing with TheraDrive in Mexico in a robot gym suggest it is an effective affordable solution
for upper limb stroke rehabilitation whether alone or in a suite with other devices.
1 INTRODUCTION
Fifty percent of stroke survivors who are six months
post stroke and post rehabilitation have residual
impairments in their upper and lower limbs. Greater
than 30% are unable to walk without some
assistance and 26% remain dependent in activities of
daily living (Rosamond et al., 2008). Affordable
stroke rehabilitation approaches can maximize the
functional independence of stroke survivors
discharged after inpatient and outpatient services
and improve access to rehabilitation for low-
resource environments (Howitt et al., 2010). New
affordable assistive/robotic devices for home and
outpatient environments are needed for areas staffed
by a few therapists. For example, Colombo and
colleagues (Colombo et al., 2007) and Hesse and
colleagues (Hesse et al., 2005) in separate efforts
developed affordable robot devices for upper limb
therapy and showed that they were motivational and
useful for rehabilitation. Johnson and colleagues
(Johnson et al., 2004); (Johnson et al., 2005);
(Johnson et al., 2007) developed Driver’s SEAT and
Theradrive and later proposed the use of low-cost
devices such as Theradrive in a device suite tied to
Unitherapy, a unifying custom software that allowed
stroke survivors to play therapeutic games (Feng and
Winters, 2009). Recently, Buschfort and colleagues
showed that a suite of four simple robotic devices
(from Reha-STIM) can provide effective seated
‘hands on’ therapy to acute and sub-acute patients
(Arm Studio) inside the Charite’ Rehabilitation
Hospital in Berlin, Germany. Arm Studio can deliver
effective therapy to patients under the supervision of
a single therapist (Buschfort et al., 2010).
This paper briefly describes the evolution of the
Theradrive system and its novel use in a robot
therapy gym in Mexico, where it was one of 6
devices aimed at improving motor function after
stroke. We suggest it is an effective affordable
solution for upper limb stroke rehabilitation whether
alone or in a suite with other devices (Johnson et al.,
2007); (Bustamante and Johnson, 2012).
2 TheraDrive
TheraDrive, initially sponsored by the American
Heart Association, was developed as an affordable
stroke therapy system. It uses commercial force-
feedback wheels mounted on novel height adjustable
frames to provide a therapy environment for the
upper limb (Johnson et al., 2007). Figure 1 shows an
example of the original system. The main
307
J. Johnson M., Montes S. and Bustamante K..
TheraDrive in a Robot Gym - Toward Stroke Rehabilitation beyond Inpatient Rehabilitation Settings in USA and Mexico.
DOI: 10.5220/0004934603070311
In Proceedings of the International Conference on Biomedical Electronics and Devices (TPDULL-2014), pages 307-311
ISBN: 978-989-758-013-0
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

components of the TheraDrive system are a pair of
modified, commercial force-feedback steering
wheels, commercial gaming software as well as a
customized software called Unitherapy (Feng and
Winters, 2009). The system can be utilized in
several training modes; these are unilateral steering
utilizing the Logitech force-feedback wheel in the
front or on the side and bilateral steering utilizing
the two steering wheels mounted in the front in a bus
driving configuration (Paranjape et al., 2006).
TheraDrive can be used with or without an
autonomous mobile robot that can move about the
perimeter. The robot can monitor arm and torso
movements and provide visual feedback on activities
(Johnson et al., 2011). Therapy with Theradrive
consists of subjects playing off-the-shelf driving
games such as Need for Speed or completing custom
tracking tasks such as circle tracking or complex
sine wave tracking. As subjects completed tracking
tasks using the wheel, they experienced spring like
assistive or resistive forces on the wheel; the
magnitude of the force-feedback was proportional to
the tracking error. The proportional gain was pre-
adjusted according to a subject’s tracking ability.
The custom tracking tasks and the force-feedback
experience were created via the Unitherapy program.
Theradrive was used in a pilot study where data
were collected from ten stroke subjects who used the
device in twenty-four, one-hour therapy sessions
(Ruparel et al., 2009). Results showed that the
device was useful for stroke rehabilitation of the
upper limb [no hands], increasing range of motion in
the shoulder and elbow flexion/extension degrees of
freedom. The Theradrive system proved most suited
for subjects with moderate-to-high function. The low
torque output of the commercial wheels and the non-
adaptive force-feedback algorithm applied during
therapy made it difficult for stroke subjects with low
motor function due to severe hemiparesis to
experience a great benefit. The wheels were unable
to apply sufficient assistive forces for these users.
The system’s inability to support very low-
functioning subjects lead to a re-design effort to
improve its usefulness to them. The design efforts
lead to the creation of Haptic Theradrive, a low-cost
robot that is stronger in that it is able support larger
forces. Custom adaptive control algorithms allow
forces to be applied at the wheel that can adapt to a
user’s functional ability. The system also includes a
novel mechanism for creating variable compliance
and torque limits at the wheel; this enables safe use
of the system (Theriault et al., 2014). Figure 2
shows a prototype of the newest Theradrive, Haptic
Theradrive, with the custom crank arm capable of
applying torques stronger than the commercial
force-feedback wheel (45Nm versus 1.5Nm).
Figure 1: Theradrive original in front and side drive.
Figure 2: Haptic Theradrive.
2.1 TheraDrive in Mexico
Simultaneous to the Haptic Theradrive development,
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
308

the original Theradrive was recreated in Mexico by
Co-PI, Karla Bustamante with specifications given
by PI Johnson. As in the USA stroke survivors in
Mexico are discharged from rehabilitation still
having residual disabilities and needing access to
services in the community. Unfortunately, in
developing countries such as Mexico a disproportion
number of the population is without easy access to
rehabilitation services (Lozano-Ascencio et al.,
1996); (Kurland, 1977). Access is very limited by, 1)
economics: rehabilitation services and associated
technologies may not exist outside of major urban
areas and many times are not affordable by low
income patients; 2) training: skilled therapists and
physiatrists are often not available in large numbers
inside or outside of cities; and 3) technology: access
to state of art rehabilitation technologies may be
limited and gaining access may be too costly.
The Mexican version of the Theradrive system
essentially mimicked the original version with
commercial force-feedback steering wheel and a
height adjustable frame (Bustamante and Johnson,
2012). Several custom games were used with the
Mexican system. Figures 3 and 4 show the
Theradrive Mexican version. The Mexican version
of the system maintained the key features of a height
adjustable frame and a variety of mounting positions
for the force-feedback wheel. It improved upon the
seating by creating a rail-mounted seating system
that made adjusting patients easier. The Unitherapy
custom software was also used. Therapy with this
system was similar and consisted of stroke survivors
playing off-the-shelf games and custom tracking
tasks.
Figure 3: Theradrive the version in Mexico.
Figure 4: Mexico Theradrive with user.
2.2 Robot Gym Study
The Mexican Theradrive was deployed in a novel
concept, we develop and called the robot gym
(Bustamante and Johnson, 2012). The robot gym
offered therapy based on circuit training where
patients could rotate to 6 stations under a clinician’s
supervision; each station used a custom or
commercially built robot/mechatronic rehabilitation
technology. On four machines subjects did activities
of daily living (ADLs), cycling, or game-based
visuomotor tracking tasks using the upper limb and
on two machines, cycling and gait training using the
lower limb.
The long-term goal of the robot gym is to
provide therapy for the upper and lower extremities
of stroke patients in an environment where limited
supervision is available. Our main objective in this
pilot study was to determine if the robot gym can
deliver comparable care as standard therapy
administered at CREE, the only low-cost public
rehabilitation healthcare center located in
Chihuahua, Mexico. Seventeen patients with right
hemiparesis due to a stroke were randomized to
either a standard therapy group (Control
Group:N=7) or the robot gym group (Robot
Group:N=10). All patients had 24, 1-hour therapy
sessions for the upper and/or lower limb. Patients in
the standard therapy group experienced 1-on-1
manual therapy. Patients in the robot therapy group
rotated through the six stations with an engineer and
therapist as supervisors that assist with set-up and
use of the devices.
All patients were evaluated pre- and post-
therapy for arm/hand motor impairment using the
Fugl-Meyer (Fugl-Meyer et al., 1975). Their
engagement in the therapy was assessed using the
intrinsic motivation scale (Wilson et al., 1984).
Unpaired t-tests determined significant differences
with p≤0.05 as threshold.
TheraDriveinaRobotGym-TowardStrokeRehabilitationbeyondInpatientRehabilitationSettingsinUSAandMexico
309
3 RESULTS AND DISCUSSION
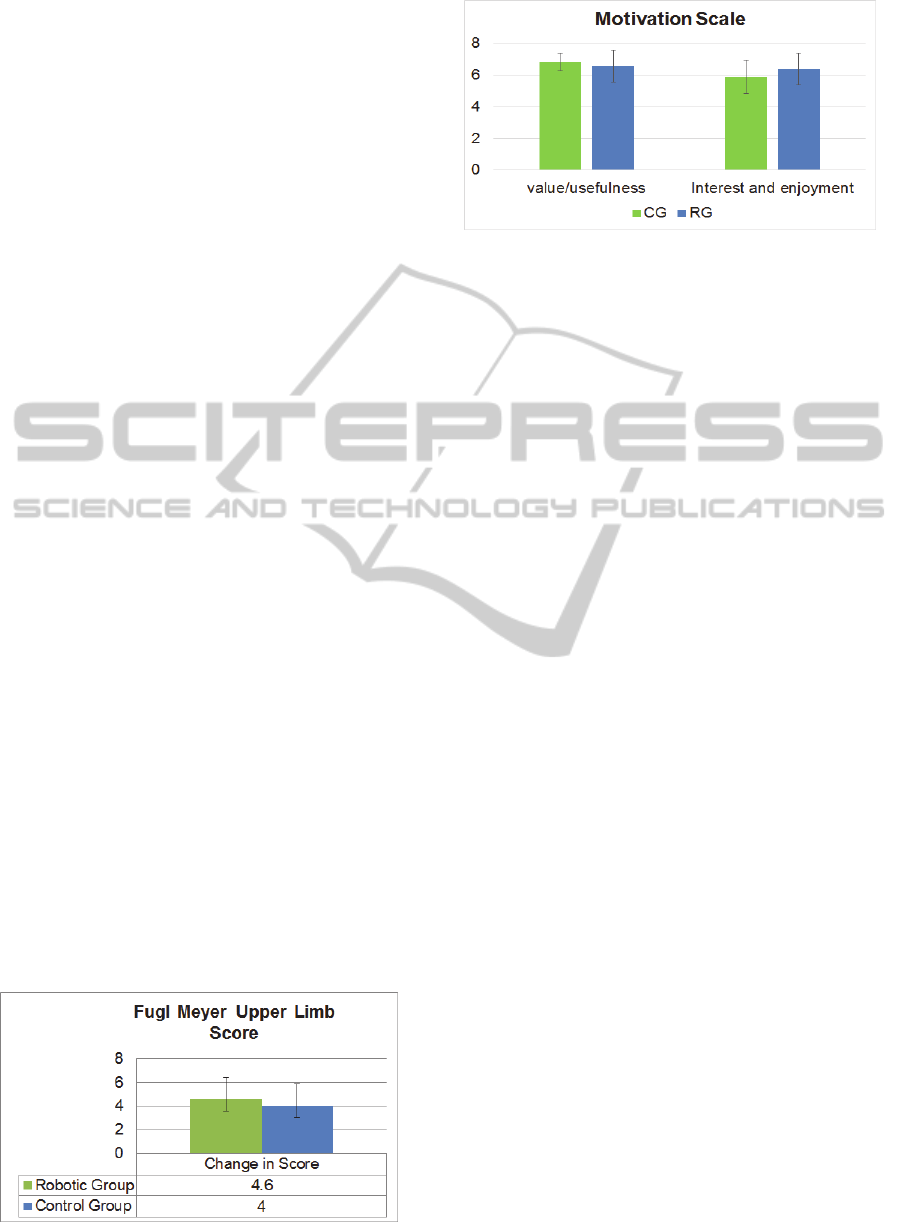
Both Control Group (CG) and Robot Group (RG)
experienced a mean 4 point change in the Fugl-
Meyer motor control scores (RG: 4.6±1.23 and CG:
4±1.85: p=0.79), representing a more than 20%
increase over baseline (Figure 5). On average both
CG and RG perceived the therapy received as
valuable (RG: 6.83±0.56 and CG: 6.57±1.04:
p=0.14) and engaging (RG: 6.36±1.23 and CG:
5.89±1.6: p=0.27) (Figure 6). The differences in
upper limb outcomes and engagement were not
significant suggesting comparable therapy (Johnson
and Bustamante, 2014). Figures 5 and 6 summarize
the FM and motivation results.
The Mexican study shows that TheraDrive was
effective in concert with the other upper limb
devices. The impact of TheraDrive alone on motor
recovery cannot be separated from the Bioness
device or the Motormed upper limb. However, the
previous pilot data in the USA suggested TheraDrive
main contribution would be in shoulder and elbow
flexion and extension improvements (Ruparel et al.,
2009) and (Johnson et al., 2007).
Our overall goal for the pilot study in Mexico
was to determine if a low-cost system of
robot/computer-driven devices under limited
supervision by clinicians could improve motor
function of stroke survivors. The pilot study
demonstrated that the robot gym was effective and
was just as good as the control group. This is a
successful outcome given our goal and suggest that
we could potentially address issues of access to
rehabilitation services in more rural locations in
Mexico. The results suggest that creating a robot
gym in more rural Mexico where access to
rehabilitation is limited and staffing it with both a
remote supervisor and at least one skilled clinician
could not only provide access to rehabilitation for
stroke survivors in these locations but also given
them ways of further improving their rehabilitation
outcomes.
Figure 5: Fugl-Meyer score.
Figure 6: Motivation scores.
3.1 Lesson Learned
There is a need for appropriate rehabilitation
technologies. Except for one of the machines used,
all other devices were commercial products that
were not developed with Mexico in mind or
developed to be deployed in a resource poor
environment. As a result, when the devices
developed issues, getting technical help was difficult
and getting replacement parts were a challenge.
There is a need for low-cost solutions that are
rugged and simple to use. Problems with the
technology were sometimes complex and greater
than a clinician could troubleshoot and therefore, the
reliance on the engineer for assistance with the use
of the equipment was more than anticipated.
There is a need for reliable metrics that are able
to be administered, analysed and interpreted quickly.
We found that post assessment of changes after
therapy was difficult to obtain quickly. Clinical,
motion, and engineering analyses were done by the
clinician or an engineer and required many hours of
analysis. As a result, meaningful changes in function
were not feedback to patients in a timely manner.
4 CONCLUSIONS
We briefly presented the TheraDrive, its evolution,
and a feasibility study of its use in robot gym with
five low-cost therapy devices. Our overall goal was
to test the concept of affordable technology-
mediated care delivery in Mexico. Since access to
rehabilitation services and associated technologies
may not exist outside of major urban areas and many
times are not affordable to low income patients, our
robot gym is an innovative solution that has the
potential to augment the delivery of rehabilitation
care.
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
310

ACKNOWLEDGEMENTS
This work was supported in part by the American
Heart Association under the grant #0635450Z
entitled “Robot-Assisted Motivating Rehabilitation
after Stroke”, by departmental funds of the Physical
Medicine and Rehabilitation of the Medical College
of Wisconsin, and by the Mexican government
grant# CHIH-2009-C02-127781 entitled “Gimnasio
Robotica”. We would also like to extend our thanks
to all the members of Rehabilitation Robotics
Research and Design Lab in USA and the gait lab in
Mexico. Please direct all correspondence to Dr.
Michelle J. Johnson.
REFERENCES
Buschfort R., Brocke J., Heb A., Werner C., Waldner A.,
Hesse S., 2010. Arm Studio to intensify upper limb
rehabilitation after stroke: Concept, acceptance,
utilization, and preliminary clinical results. J Rehabil
Med 42:310-314.
Bustamante K., Johnson M. J., 2012 Low cost gymnasium
for robotic rehabilitation of stroke survivors. In 7th
International Conference on Appropriate Healthcare
Technologies for Developing Countries, pp.21, UK
Colombo R., Pisano F., Mazzone A. et al., 2007. Design
strategies to improve patient motivation during robot-
aided neuroRehabilitation. J NeuroEngineering and
Rehabil, 4(6): open access
Feng X. and Winters J. M., 2009. A pilot study evaluating
use of a computer-assisted neurorehabilitation
platform for upper extremity stroke assessment.
Journal of NeuroEngineering and Rehabilitation, open
access.
Fugl-Meyer AR, Jaasko L, Leyman I, Olsson S, Steglind
S. 1975. The post-stroke hemiplegic patient: A method
for evaluation of physical performance. Scand J Rehab
Med 7:13
Hesse S., Werner C., Pohl M., S. Rueckriem, J. Mehrholz,
and M. L. Lingnau. 2005. Computerized arm training
improves the motor control of the severely affected
arm after stroke: A single-blinded randomized trial in
two centers. Stroke. 36:1960-1966
Howitt P., Darzi A., Guang-Zhong Y. et al., 2010.
Technologies for global health, the Lancet, 380:507-
535
Johnson M. J., Bustamante K., 2014. Affordable
technology-mediated rehabilitation of stroke survivors
in a global context. In Unite For Sight 11th Annual
Global Health & Innovation Conference, Yale
University, April 12-13. Abstract. Accepted. In press.
Johnson M. J., Feng X., Johnson L. M., Winters J. M.,
2007. Potential of a suite of robot/computer-assisted
motivating systems for personalized, home-based,
stroke rehabilitation. J NeuroEngineering and Rehabil
Mar 1; 4(6) (open access)
Johnson M. J., Shakya Y., Strachota E., Ahamed S. I.
2011. Low-cost monitoring of patients during
unsupervised robot/computer assisted motivating
stroke rehabilitation. Biomed Tech (Berl). 56(1): 5-9
Johnson M. J., Trickey M., Brauer E., F. Xin, 2004.
TheraDrive: A new stroke therapy concept for home-
based computer-assisted motivating rehabilitation. In
Conf Proc IEEE Eng Med Biol Soc. 2: 4844-47.
Johnson M. J., Van der Loos H. F. M., Burgar C. G., Shor
P., and Leifer L. J., 2005. Experimental results using
force-feedback cueing in robot-assisted stroke therapy.
IEEE Transactions on Neural Systems and
Rehabilitation Engineering. 13(3):335–348.
Kurland L. T., 1977. Twenty five years of
neuroepidemiology in the Americas. Neurol Neurocir
Psychiatr. 18 (2-3): 129-144.
Lozano-Ascencio R., Frenk Mora J., Gonzalez-Block M.
A., 1996. Burden of disease in the aged, México,
1994.
Sal Pub Mex 38 (6): 419-429.
Paranjape R. P., Johnson M. J., Ramachandran B., 2006.
Assessing impaired arm use and learned bias after
stroke using unimanual and bimanual steering tasks. In
Conf Proc IEEE Eng Med Biol Soc. 1:3958-61.
Rosamond W., Flegal K., Furie K. et al. 2008. Heart
Disease and Stroke Statistics_2008 Update: A report
from the American Heart Association statistics
committee and stroke statistics subcommittee,
Circulation 117;e25-e146.
Ruparel R., Johnson M. J., Strachota E., Tchekanov G.,
McGuire J., 2009. Evaluation of the TheraDrive
system for robot/computer assisted motivating
rehabilitation after stroke. In Conf Proc IEEE Eng
Med Biol Soc. 811-4
Theriault, A. R., Nagurka, M. L., Johnson, M. J., 2014.
Design and Development of an Affordable Haptic
Robot with Force-Feedback and Compliant Actuation
to Improve Therapy for Patients with Severe
Hemiparesis. Transactions on Haptics. IEEE
Computer Society In Press.
Wilson D. J., Baker L. L. et al., 1984. Functional test for
the hemiplegic upper extremity. American Journal of
occupational therapy. 38: 159-164.
TheraDriveinaRobotGym-TowardStrokeRehabilitationbeyondInpatientRehabilitationSettingsinUSAandMexico
311
