
Prediction and Management of Readmission Risk for Congestive
Heart Failure
Senjuti Basu Roy and Si-Chi Chin
Center for Web and Data Science, Institute of Technology, The University of Washington - Tacoma,
1900 Commerce Street, Tacoma, WA 98402-3100, U.S.A.
Keywords:
Hospital Readmission Risk Prediction, Readmission Risk Management, Predictive Modeling.
Abstract:
This position paper investigates the problem of 30-day readmission risk prediction and management for Con-
gestive Heart Failure (CHF), which has been identified as one of the leading causes of hospitalization, espe-
cially for adults older than 65 years. The underlying solution is deeply related to using predictive analytics
to compute the readmission risk score of a patient, and investigating respective risk management strategies
for her by leveraging statistical analysis or sequence mining techniques. The outcome of this paper leads to
developing a framework that suggests appropriate interventions to a patient during a hospital stay, at discharge,
or post hospital-discharge period that potentially would reduce her readmission risk. The primary beneficia-
ries of this paper are the physicians and different entities involved in the pipeline of health care industry, and
most importantly, the patients. This paper outlines the opportunities in applying data mining techniques in
readmission risk prediction and management, and sheds deeper light on healthcare informatics.
1 INTRODUCTION
Early readmission is a profound indicator of the qual-
ity of care provided by the hospitals. The Centers
for Medicare & Medicaid Services (CMS) recently
began using readmission rate as a publicly reported
quality metric. The estimated cost of unplanned read-
mission was 17.9 billion in 2004 (Jencks et al., 2009),
and more than 27% of them were considered avoid-
able (Walraven et al., 2011). Readmission can result
from a variety of reasons, including early discharge
of patients, improper discharge planning, and poor
care transitions. Studies have shown that appropri-
ate interventions during the hospital stay, during or
post-discharge plans like home based follow up, and
patient education can improve the health outcome of
the patients and reduce the readmission likelihood, es-
pecially in elderly patients, and decrease the overall
medical costs (Naylor MD, 1999; Rich et al., 1995;
Schneider et al., 1993; Phillips CO, 2004; Koelling
et al., 2005).
To that end, this position paper focuses on investi-
gating analytical techniques to mitigate the readmis-
sion risk of the individuals and improve their over-
all health outcome. While our vision is generic and
applicable to any disease, for the purpose of illus-
tration, our primary investigation hinges on Conges-
tive Heart Failure (CHF), in particular. CHF is one
of the leading causes of hospitalization, and stud-
ies show that many of these admissions are readmis-
sions within a short window of time. Based on the
2005 data of Medicare beneficiaries, it has been es-
timated that 12.5% of Medicare admissions due to
CHF were followed by readmission within 15 days,
accounting for about $590 million in healthcare costs
(Krumholz HM, 1997). More specifically, this paper
emphasizes the 30-day readmission problem for CHF,
as this time window is considered clinically mean-
ingful by different healthcare services and standards.
Identifying patients who have greater risk of readmis-
sion can guide implementation of appropriate inter-
ventions to prevent these readmission. The primary
objective of this work is to investigate a comprehen-
sive framework to address the problem of readmission
risk prediction and management for CHF. We summa-
rize the state of the art on the general problem of CHF
risk prediction, identify their limitations, and outline
future opportunities.
Readmission is common and costly. It can re-
sult from a variety of reasons, including early dis-
charge of patients, improper discharge planning, and
poor care transitions. Appropriate interventions or
pre-discharge planning (Schneider et al., 1993) , and
post discharge plans like home based follow up (Nay-
523
Basu Roy S. and Chin S..
Prediction and Management of Readmission Risk for Congestive Heart Failure.
DOI: 10.5220/0004915805230528
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2014), pages 523-528
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

lor MD, 1999) and patient education (Koelling et al.,
2005) can reduce the readmission rates considerably
and improve the health outcome of the patients. In
particular, studies have shown that targeted inter-
ventions during the hospital stay, during or post-
discharge, can reduce the readmission likelihood, es-
pecially in elderly patients, and decrease the overall
medical costs (Naylor MD, 1999; Rich et al., 1995).
However, to the best of our knowledge, there does
not exist any effort that proposes an iterative analyti-
cal framework to predict 30-day readmission risk for
CHF and to recommend appropriate personalized in-
tervention strategies to the patients at different phases,
which is the primary focus of our work.
This paper has two primary objectives: 1) first,
summarize current research on predicting the 30-day
readmission risk score (or percentage) of CHF pa-
tients; 2) second, outline the challenges and oppor-
tunities in designing personalized intervention strate-
gies to assist decision making, such that the read-
mission risk of the patients gets reduced by a certain
percentage. While the former task is risk prediction,
the latter objective is referred to as risk management.
Interestingly, suggesting appropriate interventions is
tightly integrated with a patient’s current phase – for
example, the post-discharge interventions may only
be limited to appropriate follow-ups or patient educa-
tion, while physicians could suggest different proce-
dures or surgery, if the intervention is being adminis-
tered during her hospital stay. Existing research has
studied different clinical risk prediction problems in
silos. This paper is one of the first efforts to study the
risk prediction and management problem in conjunc-
tion.
Our vision is to design the solution strategies us-
ing statistical and data mining techniques. For ex-
ample, the risk prediction problem could be designed
as a statistical classification or a regression (Han and
Kamber, 2006) problem, with the objective to learn
a mathematical function that correctly outputs the as-
sociated probability of an individual’s 30-day risk of
readmission, or correctly outputs the actual number
of days until the next readmission will take place for
the individual, using different factors that causes CHF
readmission. On the other hand, the risk manage-
ment problem could also be studied using statistical
and data mining techniques. Given a set of possi-
ble interventions, if the risk prediction problem is de-
signed as a regression problem, then to achieve a tar-
geted (lower) risk score, the risk management prob-
lem could be solved by: 1) learning the reverse regres-
sion or calibration (Johnson and Wichern, 1988) of
the intervention parameters that results in the intended
targeted risk score, and 2) performing sequence min-
ing (Han and Kamber, 2006) to suggest appropriate
interventions.
2 RISK PREDICTIONS
In this section, we summarize current studies in pre-
dicting risk of hospital readmission and discuss the
limitations of the field.
2.1 Applying Extensive Data
Preprocessing to Improve Quality of
Prediction
The quality of data determines the quality of predic-
tions. This paper suggests to incorporate a wide va-
riety of data preprocessing and predictive modeling
techniques, i.e. missing value imputation, clustering,
and classification (Han and Kamber, 2006), for im-
proving the prediction of 30-day readmission risk for
CHF patients. Real world clinical data are noisy and
heterogeneous in nature, severely skewed, and con-
tain hundreds of pertinent factors. They contain in-
formation on patients’ socio-demographical charac-
teristics, such as marital status and ethnicity; clinical
data such as diagnosis, discharge information; and co-
morbidity factors
1
; other cost related factors pertain-
ing to a particular hospital admission; lab results; pro-
cedures. The proposed solution relies on data mining
and predictive analytics. Current research has investi-
gated a wide range of techniques to that end – starting
from simple Naive Bayes’ Classifier, Support Vector
Machine (Zolfaghar et al., 2013b; Zolfaghar et al.,
2013a), Regression models (Kansagara D, 2011), to
Ensemble of Multilayer classifier (Zolfaghar et al.,
2013c).
A sophisticated and effective predictive model of-
ten requires a large set of attribute values that may
not all be available (or known) at the time when a pa-
tient or a healthcare provider uses the risk assessment
tool. To transform the limited inputs to the complete
set of attribute values on which the predictive model
is trained, the first task of the risk prediction model is
to map the input values to a group (i.e., cluster) of pa-
tients who are most similar to the provided user pro-
file. The model pre-computes the clusters based on
different permutations of input attributes using the k-
mode algorithm (Han and Kamber, 2006). To accom-
modate all possible scenarios, the model constructs
k ∗ 2
n
clusters, where n is the number of factors (i.e.,
1
Comorbidities are specific patient conditions that are
secondary to the patient’s principal diagnosis and that re-
quire treatment during the stay.
HEALTHINF2014-InternationalConferenceonHealthInformatics
524

attributes) used in the predictive model and k is the
predetermined number of clusters. The model effi-
ciently matches the given set of input attribute values
to its closest cluster centroid using the index-based
matching algorithm (Zolfaghar et al., 2013a). The
pre-computed cluster centroids are used to complete
the remaining missing attribute values.
Then the problem of computing risk score is stud-
ied as a classification problem, or as a regression
problem. The primary objective is to design a math-
ematical function that learns the relationship between
the attributes and the risk score. The relationship
could be linear or non-linear. The risk could be some
categories (High risk, Medium Risk, Low Risk), or
it could be a positive real number. Given n factors,
the task is to learn the function, which generates the
appropriate risk score y.
y = f (x
1
, x
2
, . . . , x
n
)
2.2 Limitations of Current Risk
Prediction Research
There are two primary limitations of current research
on risk of readmission predictions. The first is the lack
of intervention recommendations based on the results
of risk predictions. The second limitation is the lack
of customization of care management strategies for
individual patients and for different healthcare sys-
tems. While most research has invested largely in pre-
dicting risk of readmission, these aspects are scarcely
unexplored.
The value of risk prediction is massively limited if
there is no guidance about selecting proper interven-
tions to manage the risk. The knowledge of prediction
results is only actionable if predictive modeling also
enables the decision making about the interventions.
Extensive number of studies investigate risk factors
contributing to risk of readmission (Kansagara D,
2011). However, many primary factors, such as age,
gender, and prior hospitalization history, can not be
manipulated. The knowledge that age contributes to
higher risk of readmission is not actionable since it
is impossible to alter one’s age to reduce the read-
mission risk. Therefore, predictive modeling should
aim to enable intervening on different stages of care:
upon admission, during the hospitalization, and at dis-
charge.
Currently, most care managers in the hospitals
adopt a holistic approach to intervene based on sim-
ple categorization of patients (e.g. high risk versus
low risk patients). However, intervention strategies
could be more effective if they were tailored to indi-
vidual patients. For example, while patient have no
family or other caregiver at home may benefit from
home care and home visit, other patients may ben-
efit more from medication review and prescriptions
to lower their sodium level. Furthermore, interven-
tion strategies should also be customized based on the
needs of different hospitals and healthcare systems.
For example, while some hospital may wish to over
predict the number patients with risk of readmission
in order to decrease the readmission rate, other hos-
pitals may aim at precise predictions to efficiently al-
locate care resource and can afford to tolerate some
instances of false negatives. Therefore, the problem
of risk management intervention prediction and rec-
ommendation should be studied in conjunction with
the cost of interventions and available resource in a
hospital or a healthcare system.
The limitations provide the opportunities to ex-
pand the scope of the applying predictive modeling
to the problem of readmission reduction. We outline
some possible solutions to address the first limitation
in Section 3.
3 OUR VISION: FROM RISK
PREDICTION TO RISK
MANAGEMENT
This section describes our vision of applying statis-
tical and data mining techniques for readmission risk
management. We first present a framework that incor-
porates predictive modeling to risk management feed-
back loop. We then suggest two methods – calibration
and sequential mining – to design a sequence of inter-
ventions for risk management.
3.1 Incorporating Predictive Modeling
to Risk Management Feedback loop
The objective of risk management is to develop ap-
propriate medical interventions and care management
strategies to reduce the risk score of an individual. In-
terventions could take place during hospitalization, at
discharge time, or post-discharge. Patients should be
treated and/or reached in a unique way in order to
minimize the risk score. From the factors described
above, our proposed solution identifies and selects
a subset of intervention factors that are actionable,
either during hospitalization, at time of discharge,
or post discharge. Additionally, the model consid-
ers post-discharge interventions, including medica-
tion review and counseling by clinical pharmacist, di-
etary and social service consultation, coordination of
home care and home visits, follow up with patients
via telephone, use of tele-health in patient care, etc.
PredictionandManagementofReadmissionRiskforCongestiveHeartFailure
525
A. Patients are
admitted to the
hospital
B. Is CHF a
possible active
diagnosis?
C. Preidct
readmission risk
D. Display and
visualize risk
factors
G. Is it a risk
reduction
opportunity?
E. Predict optimal
interventions that
can reduce the risk
F. Display the
effect of various
interventions
H. Initiate the
selected
interventions
I. Collect the
updated patient
data
J. Usual care
Yes
YesNo
No
K. Patients are
discharged from
the hospital
Risk Prediction and Management Feedback Loop
L. Risk Prediction
and Management
Feedback Loop
Pre-admission
At-admission
Care
At-discharge
Post-discharge
Patient Time Series
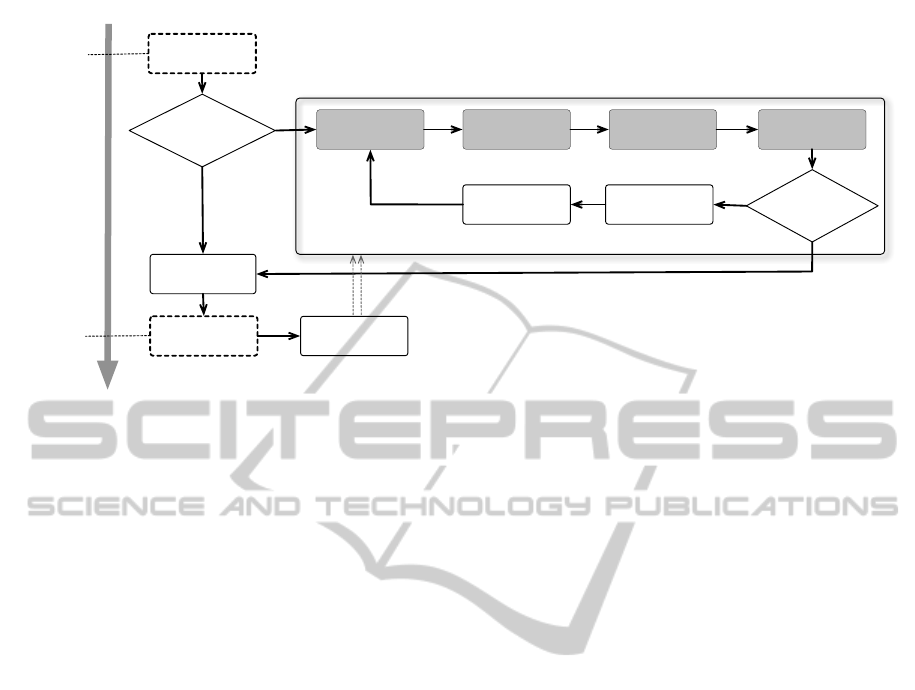
Figure 1: Feedback loop for predicting and managing risk of readmission. The shaded steps describe how the project fits in
the process of care.
In Figure 1, steps A-J illustrate how analytics can
be integrated into the feedback loop in clinical prac-
tice to reduce risk of readmission. After identifying
admitted patients with CHF (steps A,B), we first esti-
mate the risk of readmission and analyze risk factors
for patients of different characteristics (steps C, D).
Then, our analysis also suggests interventions that can
reduce the risk and their relative effect on risk reduc-
tion (steps E, F). Healthcare providers may then deter-
mine whether to initiate interventions and capture the
outcome of the interventions (steps G-I). The outcome
of the interventions produces a new risk estimate (step
C). Given the updated risk assessment (steps C-F),
healthcare provider could then re-evaluate whether
the risk is minimized and whether further opportu-
nity for risk reduction exists (step G). This way, the
proposed framework contributes to the prediction and
management of readmission risk for CHF patients.
3.2 Predictive Modeling Solutions to
Risk Management
This section describes the adopted procedure to solve
the risk prediction and the management problem, and
the evaluation methods of the solutions. Imagine that
the risk score of a patient is expressed as a function of
different interventions. Table 1 describes three imag-
inary patient records with only five interventions. To
manage patients’ 30-day readmission risk, our over-
all process relies on understanding the respective risk
score first, followed by learning the best interventions
to reduce it.
As discussed in Section 2, the risk prediction
problem could be solved using many different predic-
tive analytics techniques. For the purpose of illustra-
tion, here, we consider a specific and effective model,
namely multiple linear regression (Han and Kamber,
2006) and describe the risk management methodol-
ogy using that.
A general additive multiple linear regression
model relates the risk score of a patient as the de-
pendent variable or outcome (y), to a set of k in-
dependent or predictor variables (i.e., interventions),
x
1
, x
2
, . . . , x
k
. The model is expressed by the equation
y = α + β
1
x
1
+ β
2
x
2
+ . . . + β
k
x
k
(1)
From the patient data, using x
1
, x
2
, ....., x
k
and the ob-
served risk score, multiple linear regression learns
the coefficients α, β
1
, . . . , β
k
. That is, the objective is
to learning the dependency between the independent
variables and the outcome. Given a patient and a set
of possible interventions, the task is, which subset of
interventions to administer, such that her readmission
risk score gets reduced (e.g., to 45%)? We propose
two different techniques to that end.
3.2.1 Inverse Regression/Calibration
Given a regression equation such as Equation 1, the
intended reduced risk score y’ (e.g., to 45%), the
coefficients α, β
1
, . . . , β
k
and the function is known.
The objective is to output the value of the indepen-
dent variables x
1
, x
2
, ....., x
k
that results in y’. Note
that this is inverse regression or the “multivariate cal-
ibration”(Johnson and Wichern, 1988; Hardin et al.,
HEALTHINF2014-InternationalConferenceonHealthInformatics
526

Table 1: A set of 3 simple patient data with 5 interventions
Ejection Fraction Blood Pressure Depression Diabetes Cardiac CT Risk Score (y)
<40 160/100 Yes Yes No 75%
58 140/90 No Yes Yes 55%
51 170/110 Yes Yes No 87%
2003) problem in statistics. The proposed research
applies the Bayesian Approach for calibration. Equa-
tion 1 above for the n-sample calibrating data can be
written as,
Y = B
0
X +E
where Y (nx1) is the response matrix, X(nx(k + 1)) is
a fixed matrix of dependent factors, and B are the co-
efficients, and E is the error matrix.
A particular risk outcome follows the same as-
sumption and could be expressed as,
y
0
= B
0
X
∗
+ α
0
Finding appropriate interventions here is analogous to
finding the marginal posterior distribution of X
∗
. To
do that, the process first calculates the joint prior, ex-
pressed as,
p(B, Σ, X
∗
) = p(B, Σ)p(X
∗
)
Furthermore, it is assumed that p(X
∗
|Y ) = p(X
∗
).
Then the posterior distribution of X
∗
could be ex-
pressed by the joint density function. We omit further
details for brevity, and refer to (Plessis and Merwe,
2004) for detailed discussion. The output of this
method outputs the different predictors (i.e., interven-
tions) which give rise to the desirable lower risk score.
3.2.2 Sequence Mining
An alternative investigation is to study the problem
from the sequential pattern mining (Han and Kamber,
2006) perspective. The objective is to output the ap-
propriate sequence of the interventions which leads
to a desirable lower risk score. Many frequent item-
set mining algorithms (such as Apriori or FP-Growth
(Han and Kamber, 2006) ) with appropriate adapta-
tions could be applied to solve the problem. The basic
idea is to treat patient history (such as provided in Ta-
ble 1) and consider frequency of co-occurrence of the
interventions (considering their ordering) and the out-
comes (i.e., associated risks) to generate association
rules between the likely outcome and the suggested
interventions. The output would generate rules of the
form “if a patient is treated and cured for diabetes fol-
lowed by depression, and then her Ejection fraction =
58”, she is likely to have risk score 45%.
Trade-offs exist between the two suggested meth-
ods described above. The former strictly relies on a
specific function and probability distribution assump-
tion to estimate the posterior. It introduces challenges
as real world patient data exhibits severe randomness
over the time. The latter is computationally expen-
sive, especially when the attributes are continuous and
the generated rules are required to have orders, such
as ours. We explore both these paths and choose the
winning approach for validations.
4 CONCLUSIONS
This position paper investigates the problem of 30-
day readmission risk prediction and management for
Congestive Heart Failure (CHF), which has been
identified as one of the leading causes of hospitaliza-
tion. Although current research has demonstrated the
effort of predicting risk of readmission in silos, those
solutions are mostly not applicable to design inter-
vention strategies for personalized risk management.
In this position paper, we envision that a horizon of
opportunity could be unveiled, if these two problems
are studied in conjunction and in an iterative manner.
We believe that the solutions could be largely adapted
from the computing domain, in particular by applying
data mining and statistical analysis techniques. We
note that novel solutions could be designed with such
adaptations to support clinical and care management
decision making processes to reduce the risk of read-
mission and improve the quality of care.
REFERENCES
Han, J. and Kamber, M. (2006). Data mining: concepts and
techniques. Morgan Kaufmann.
Hardin, J. W., Schmeidiche, H., and Carroll, R. J. (2003).
The regression-calibration method for fitting general-
ized linear models with additive measurement error.
Stata Journal, 3(4):361–372.
Jencks, S. F., Williams, M. V., and Coleman, E. A. (2009).
Rehospitalizations among patients in the medicare
fee-for-service program. New England Journal of
Medicine, 360(14):1418–1428.
Johnson, R. A. and Wichern, D. W., editors (1988). Applied
multivariate statistical analysis. Prentice-Hall, Inc.,
Upper Saddle River, NJ, USA.
Kansagara D, E. H. (2011). Risk prediction models for
hospital readmission: A systematic review. JAMA,
306(15):1688–1698.
PredictionandManagementofReadmissionRiskforCongestiveHeartFailure
527

Koelling, T. M., Johnson, M. L., Cody, R. J., and Aaronson,
K. D. (2005). Discharge education improves clinical
outcomes in patients with chronic heart failure. Cir-
culation, 111(2):179–185.
Krumholz HM, P. E. (1997). Readmission after hospitaliza-
tion for congestive heart failure among medicare ben-
eficiaries. Archives of Internal Medicine, 157(1):99–
04.
Naylor MD, B. D. (1999). Comprehensive discharge plan-
ning and home follow-up of hospitalized elders: A
randomized clinical trial. JAMA: The Journal of the
American Medical Association, 281(7):613–620.
Phillips CO, W. S. (2004). Comprehensive discharge plan-
ning with postdischarge support for older patients with
congestive heart failure: A meta-analysis. JAMA:
The Journal of the American Medical Association,
291(11):1358–1367.
Plessis, J. L. D. and Merwe, A. J. V. D. (2004). Inferences
in multivariate bayesian calibration. JSTOR.
Rich, M. W., Beckham, V., Wittenberg, C., Leven, C. L.,
Freedland, K. E., and Carney, R. M. (1995). A mul-
tidisciplinary intervention to prevent the readmission
of elderly patients with congestive heart failure. New
England Journal of Medicine, 333(18):1190–1195.
Schneider, J. K., Hornberger, S., Booker, J., Davis, A., and
Kralicek, R. (1993). A medication discharge planning
program measuring the effect on readmissions. Clini-
cal Nursing Research, 2(1):41–53.
Walraven, C. v., Bennett, C., Jennings, A., Austin, P. C.,
and Forster, A. J. (2011). Proportion of hospi-
tal readmissions deemed avoidable: a systematic
review. Canadian Medical Association Journal,
183(7):E391–E402.
Zolfaghar, K., Agarwal, J., Sistla, D., Chin, S.-C., Roy,
S. B., and Verbiest, N. (2013a). Risk-o-meter: an in-
telligent clinical risk calculator. In KDD, pages 1518–
1521.
Zolfaghar, K., Meadem, N., Sistla, D., Chin, S.-C., Roy,
S. B., Verbiest, N., and Teredesai, A. (2013b). Explor-
ing preprocessing techniques for prediction of risk of
readmission for congestive heart failure patients. In
Data Mining and Healthcare Workshop.
Zolfaghar, K., Verbiest, N., Agarwal, J., Meadem, N.,
Chin, S.-C., Roy, S. B., Teredesai, A., Hazel, D.,
Amoroso, P., and Reed, L. (2013c). Predicting risk-
of-readmission for congestive heart failure patients: A
multi-layer approach. CoRR, abs/1306.2094.
HEALTHINF2014-InternationalConferenceonHealthInformatics
528
