
Health Information Systems
Investigating Greek Hospital Employees’ Intention to Use Electronic
Health Records
Prodromos D. Chatzoglou, Leonidas L. Fragidis, Argiro Nestoridou and Vassilios P. Aggelidis
Democritus University of Thrace, Department of Production and Management Engineering, Xanthi, Greece
Keywords: Paper Records, Health Information Systems (HIS), Electronic Health Records (EHR).
Abstract: This research examines the factors affecting Greek hospital employees’ intention to use Electronic Health
Records (EHR). The findings indicate that perceived ease of use and perceived usefulness are very
significant drivers in the adoption of the EHR. Moreover, the intention to use EHR by employees is also
affected by management support and subjective norms.
1 INTRODUCTION
Although, the need for innovative health information
systems is a fact (Knaup et al., 2006), Greek
hospitals are still on a primary stage regarding the
use of Electronic Health Records (EHR) with the
implementation of only minor scale EHR systems in
small regions to have been completed so far
(Observatory on the Information Society, 2007).
This study intends to shed some light on the factors
that affect Greek hospital employees’ intention to
use EHR. For that purpose a version of the TAM
(Technology Acceptance Model), differentiated to
fit the needs of computer acceptance in Greek
hospitals, has been used.
2 LITERATURE REVIEW
Information Technology (IT) is considered to be the
second “industrial revolution” after that of the 19th
century (Sistrom, 2005). Even though it has brought
about many changes in various fields, in the
healthcare there has been a delay in the adoption of
the IT (Ash and Bates, 2005 cited in Callen, 2007).
According to Ovretveit et al. (2007), despite the
fact that many countries and health service providers
have established policies for the implementation of
health information systems and Electronic Medical
Records (EMR), there is still a large distance to be
covered from theory (policy) to practice. A
collection of various types and definitions of HER is
provided by Hayrinen et al, 2008, p. 295.
2.1 Paper Records vs Electronics
Health Records
Even though EMRs have been implemented in many
hospitals around the globe, still, personnel such as
doctors and nurses, continue to take handwritten
notes for the observation and treatment of the
patient, writing prescriptions and radiology orders
(Atreja et al., 2008).
It is true that the majority of Hospital personnel
find it easier and more time saving them using a
computerized system during the clinical sessions.
Another important reason for the supporters of
paper-based records is their durability as well as
their accessibility by sight. However, there are also
many negative aspects regarding the paper records.
Most of the patient’s records that are kept in paper
usually “stay” within the healthcare facility.
On the other hand the implementation and use
of an EHR in health care institutions, helps staff
reduce the time spent for many actions of their
daily routine (Hier, 2005). This could include the
retrieval of a patient’s data and history, immediate
access to his laboratory or other exams needed and
the entry of new medical data during his treatment
inside the facility.
As Bakker (2007) points out, the fundamental
difference between the electronic systems and the
commonly used paper records is the field of security.
Not only EHRs offer different levels of authorization
187
D. Chatzoglou P., L. Fragidis L., Nestoridou A. and P. Aggelidis V..
Health Information Systems - Investigating Greek Hospital Employees’ Intention to Use Electronic Health Records.
DOI: 10.5220/0004232901870192
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2013), pages 187-192
ISBN: 978-989-8565-37-2
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

to their multiple users, but also, it is possible to
know which user had access to where and when
through the electronic trails of the system.
2.2 Global Efforts for EHR
Implementation
EHR have been developed by countries such as UK
(Atlantis and Vidavo, 2007), Australia (Thompson
and Brailer, 2004), Canada (Sherman, 2001).
Finland (Trade Partners, 2002) and Germany (Cross,
2000) where a similar system, based on the smart
card technology, is in use.
In the United States a decision has been made (in
2003) to have an EHR system by 2013 (Medicare
Prescription Drug Improvement and Modernization
Act MMA), estimating that 90% of the physicians
and 70% of the hospitals will be “meaningful users”
by 2019. Also Canada, aims to meet its target of
delivering EHR to 100% of all Canadians by 2015
(Shaw, 2010).
Further, in Australia the HealthConnect program
was initiated in 2001 and it was separated into three
stages (HealthConnect, 2004), with the aim to cover
80% of Queensland Health activity by 2012.
The European Commission (EC) has been
funding research activities concerning the use of
Information and Computer Technology (ICT) in the
Health Sector for the last two decades (European
Commission Information Society, 2010).Greece is a
country with a very different Healthcare
infrastructure compared to other developed countries
(Orfanidis et al., 2004).
The initial attempt for the introduction and use of
ICT in the Health sector in Greece started with the
Integrated Mediterranean Programs and Community
Support Framework (CSF) I (1986 – 1993), and was
continued in the CSF II (1994-1999), CSF III (2000-
2006) and CSF IV (2007-2013).
2.3 Technology Acceptance Model
Technology Acceptance Model (TAM) (first
introduced by Davis, 1986) best describes IS usage
and IS acceptance behaviors (Dasgupta et al., 2002,
Holden and Karsh, 2008).
In this model, “attitude” and “intention” are
influenced by “Perceived usefulness” and
“Perceived ease of use” (for definitions look at
Davis, 1985 p.320 and Holden and Karsh, 2008,
who have used TAM to study the adoption of health
IT). Their findings support the high predictive power
of TAM concerning the use and the acceptance of
health IT though with the need of some “add-ons”.
Apart from the standard features of the TAM model,
Holden and Karsh (2008) suggest the use of some
more parameters such as system quality, and
standardization. Moreover, they found strong
evidence that perceived ease of use will result in
greater acceptance and use of IT health systems by
clinicians. On the other hand, ease of use may not
affect acceptance in a great extent but appears to
correlate with usefulness. Finally, it is stated that no
matter how useful and easy to use a health IT is,
effort is needed to ensure that clinicians will be able
to use it (self-efficacy), that using the system will be
under their control (controllability) and they will be
provided with every kind of support (facilitating
conditions).
Aggelidis and Chatzoglou (2007), used a
modified TAM to study the acceptance of health
information systems (HIS) by Greek hospital
personnel. Their findings point out that personnel’s
behavioral intention to use HIS is positively affected
by perceived usefulness, ease of use of the system,
social influence, attitude, facilitating conditions and
self-efficacy. Moreover, an indirect relationship
among training and behavioral intention was
detected. Finally, positive effects between social
influence and self-efficacy, perceived usefulness and
anxiety, facilitating conditions and social influence
were supported by the results.
3 RESEARCH FRAMEWORK
AND METHODOLOGY
Tο achieve the main targets of this research a new
conceptual framework has been developed based on
the work of Aggelides and Chatzoglou (2007) and
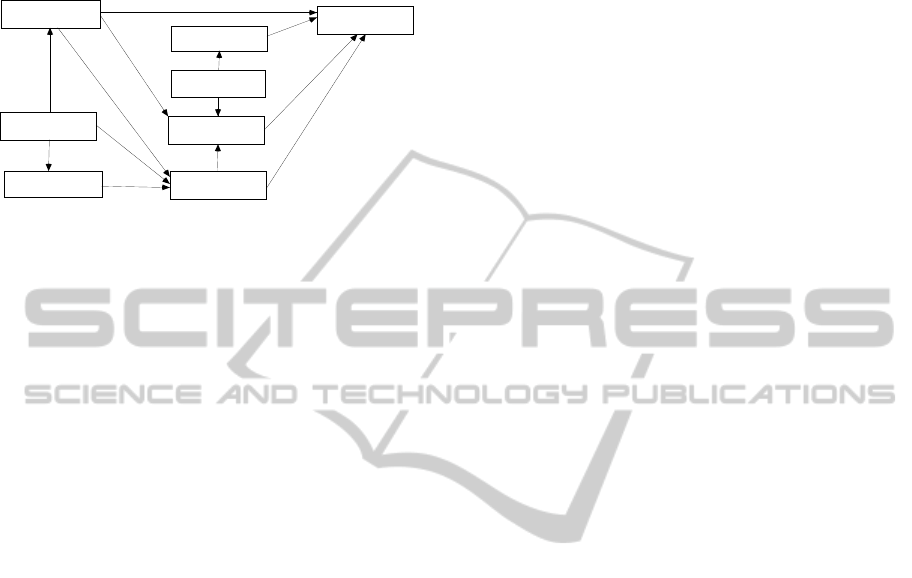
Chatzoglou et al. (2008). This framework (figure 1)
is adequate to measure intention to use EHR since it
is a version of TAM, and part of it has already been
tested in Greek companies.
3.1 Hypotheses Development
In order to test the model, a number of hypotheses
are developed, based on the technology acceptance
model, which is altered in such a way to fit the needs
of this research.
Primarily, the intention to use the electronic
patient records is, according to Chatzoglou et al
(2008), positively affected by perceived ease of use
and perceived usefulness. It is logical, therefore, to
claim that the friendlier and easier it is for an
employee to use a system in general, and the EHR in
specific, the higher the chances he/she is going to
HEALTHINF2013-InternationalConferenceonHealthInformatics
188
use it. Similarly, it is normal to assume that the more
useful an IT system is to employees for assisting
them to complete their daily tasks, the higher the
chances that they will be using it.
Figure1: The proposed model.
Finally, it also make sense to assume that
perceived usefulness and perceived ease of use are
closely related to one another. The ease of using an
IT system enhances users’ perception of its
usefulness.
H.1 The intention to use electronic health records
is positively affected by perceived ease of use.
H.2 The intention to use electronic health records
is positively affected by perceived usefulness.
H.3 Perceived usefulness of electronic health
records is positively associated with perceived
ease of use.
Next, it is well documented that, under specific
circumstances, management support motivate
hospital employees to look at a new system from a
different, more positive, angle. According to
literature (Karahanna et al., 1999), management
support could be considered as an extension of the
original TAM. It was also proven that organizations
lacking management support would not easily
persuade their employees to use the technology
required for the case (Venkatesh et al., 2003).
H.4 There is a positive relationship between
Management support and perceived usefulness
H.5 There is a positive relationship between
Management support and perceived ease of
use
Further, it is suggested that the more nervous
someone feels towards using computers, the lower
the chances for him/her to understand its usefulness.
H.6 Computer anxiety has a negative impact on
perceived usefulness
H.7 Computer anxiety has a negative impact on
perceived ease of use.
Computer self-efficacy is also a key factor
influencing intention to use EHR. It is assumed that
if an employee is a computer expert, he will
probably be much more interested in getting to know
the new system.
H.8 Self efficacy has a positive impact on
perceived usefulness.
H.9 Self efficacy has a positive impact on
perceived ease of use.
H.10 Self efficacy has a negative impact on
computer anxiety.
Another crucial factor affecting intention to use
an IT system is enjoyment. It has been statistically
proven that the more a person enjoys using
computers, the more willing he/she would be to
learn new things, especially if it has to do with their
professional occupation. Scholars also believe that
there is a positive association between enjoyment
and perceived usefulness (Davis et al., 1992;
Venkatesh et al., 2002), as well as between
enjoyment and perceived ease of use (Moon and
Kim, 2001; Venkatesh, 1999, 2000; Yi and Hwang,
2003). These findings also apply in the case of EHR.
Finally, the more a person enjoys using these EHR,
the more confident he becomes. Previous research
(Offodile and Abdel-Malek, 2002) has shown that
the attitude towards computers in general can play a
key role in whether to adopt new technologies
within the working environment..
H.11 Enjoyment of using and intention to use EHR
are positively associated.
H.12 Enjoyment of using and perceived usefulness
of EHR are positively associated.
H.13 Enjoyment of using and perceived ease of use
of EHR are positively associated.
H.14 Enjoyment of using electronic health records
and self-efficacy are positively associated.
Finally, another factor that may affect intention
to use EHR is subjective social norms. Social
subjective norms reflect the influence of important
people on a person as far as the use of EHR is
concerned. The importance of this factor is
highlighted in previous literature (Taylor and Todd,
1995; Venkatesh and Davis, 2000; Venkatesh et al.,
2003; Yu et al., 2005).
H.15 Top Management positively influences a
person’s subjective social norms about using
electronic health records.
H.16 Social subjective norms positively influence
the intention to use electronic health records.
Intention
to Use
Perceived
Ease of Use
Perceived
Usef ulness
Self
Efficacy
Management
Support
Computer
Anxiety
Subjective
Norms
Enjoyment
HealthInformationSystems-InvestigatingGreekHospitalEmployees'IntentiontoUseElectronicHealthRecords
189
3.2 Data Collection Process and
Sample Characteristics
The research instrument used to collect data is a
structured questionnaire divided into eight sections.
The first section included general questions referred
to each participant and his/her organization, while
the other seven sections referred to each of the
construct included in the proposed research model.
The second section of the questionnaire measured
the intention to use the EHR and is based on the
TAM (Yu et al., 2005; Premkumar and
Bhattacherjee, 2008). All items used are measured
on a 7 point Likert scale.
Questionnaires were distributed to 10 Greek
hospitals from where 437 usable questionnaires was
received. Apart from the questionnaires,a small
number of interviews were held in every hospital
with people in key positions (manager of the IT
department, director of the administrative personnel,
Head of nursing staff and Leader of the medical
staff).
All respondents were health staff in these
hospitals and their average age were the 38 years.
4 RESULTS
Initially, since the items used were adopted by other
similar researches, a confirmatory factor analysis is
performed to test the validity of the scales used.
4.1 Reliability Analysis
The Cronbach’s alpha is adopted for measuring the
reliability of each factor. As seen in Table 1, all
Cronbach’s alpha measurements are above the
critical value of 0.5, which show that the reliability
of all factors is high.
Table 1: Reliability and Factor Analysis.
Items Crombach’sα KMO Bartlett’s
Construct
reliability
Variance
extracted
Computer
anxiety
4 0,888 0,82 0,000 0,87 64,17%
Enjoyment 3 0,923 0,73 0,000 0,79 58,31%
Intention
to use
5 0,895 0,80 0,000 0,80 58,76%
Management
Support
3 0,871 0,74 0,000 0,84 64,03%
Perceived
ease of use
4 0,908 0,75 0,000 0,83 61,82%
Perceived
usefulness
4 0,816 0,74 0,000 0,81 59,88%
Self efficacy 10 0,961 0,94 0,000 0,88 64,88%
Subjective
norms
11 0,958 0,93 0,000 0,94 70,70%
4.2 Factor Analysis
Other aspects that should be taken into account are
the values of KMO and the Bartlett’s test of
sphericity Table 4.1presents the results drawn from
this analysis (Kaiser-Meyer-Olkin measure of
sampling adequacy).
The results of the test for the KMO and the
Bartlett’s test show that the indices are greater than
the acceptance levels (KMO>0.5 while the
Sig<0.05).
Another important aspect in the factor analysis is
the construct reliability and the variance extracted. It
can be noticed that construct reliability for all objects
exceeds the critical value of 0.7, i.e. while for all
factors the variance extracted values are all above
50%, indicates that the latent variables explain the
determination variables at an adequate level.
Further, Table 2 presents the goodness of fit
statistics for every factor. The results are above the
desired level for all CFI, GFI and AGFI, while the
values of RMR and RMSEA are all below the level
of 0.1, and the ratio of chi square/df is also below
the accepted threshold (5). These results indicate
that the factors show good fit for the SEM analysis.
Table 2: Goodness of fit statistics for every factor.
CFI GFI AGFI RMSEA RMR
Chi
Sq.
df
Computer anxiety
(CA)
0.94 0.91 0.93 0.033 0.037 9.04 6
Enjoyment(EN) 0.93 0.91 0.94 0.017 0.021 4.42 2
Intention to use (IU) 0.92 0.88 0.91 0.074 0.042 9.53 4
Management Support
(MS)
0.92 0.95 0.93 0.065 0.022 17.64 5
Perceived ease of use
(PEU)
0.97 0.91 0.93 0.055 0.037 8.44 3
Perceived
usefulness(PU)
0.93 0.89 0.92 0.029 0.018 8.72 5
Self efficacy(SE) 0.95 096 0.93 0.017 0.010 12.41 9
Subjective norms(SN) 0.93 0.95 0.95 0.015 0.044 343.00 115
4.3 Evaluation of the Structural
Models
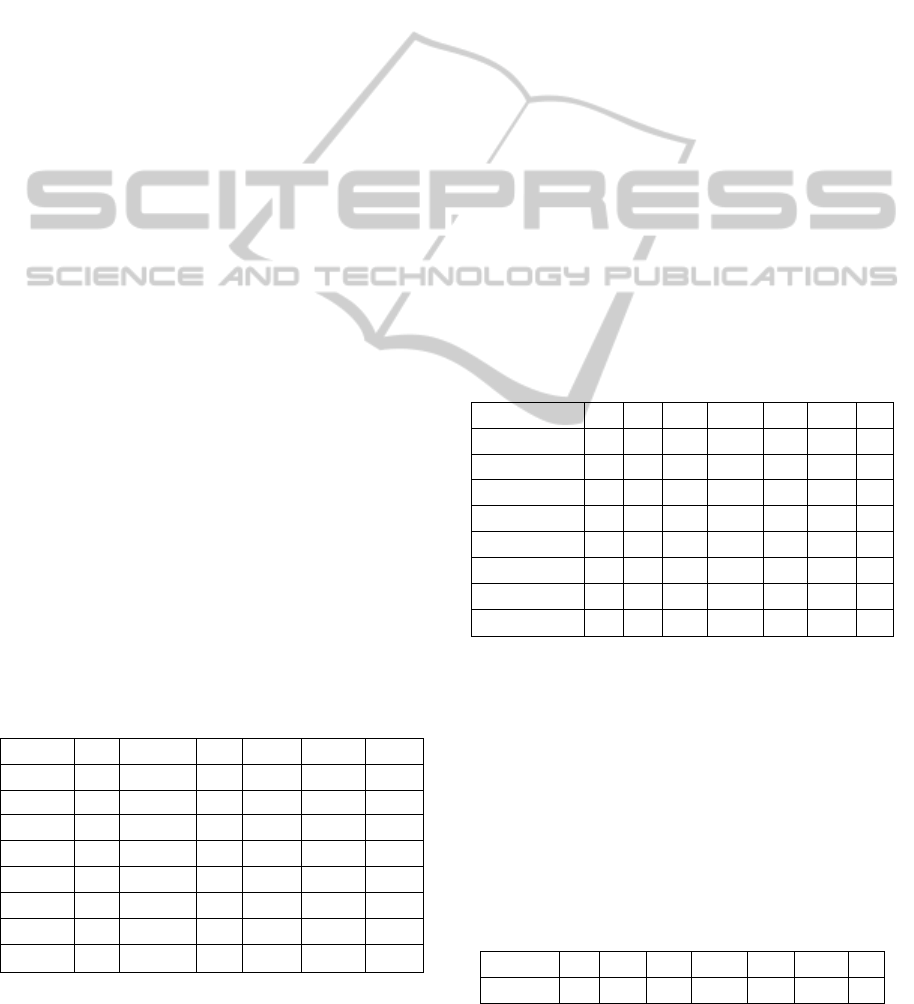
Figure 2 presents the results of the Structural
Equation Modeling analysis while table 3 shows the
goodness of fit statistics of the proposed model. It is
worthwhile noticing that all the fit indices (CFI,
GFI, AGFI) are all above the desired value of 0.9,
and as the RMSEA and RMR values are below the
critical limit of 0.1.
Table 3: Overall Model fit.
CFI GFI AGFI RMSEA RMR Chi Sq. df
Computer
anxiety
0.92 0.91 0.93 0.078 0.068 332.45 221
HEALTHINF2013-InternationalConferenceonHealthInformatics
190

Figure 2: Final structural model.
The results of the research indicate that
perceived ease of use (.88) plays a more important
role in the adoption of EHR than perceived
usefulness (.47). These findings imply that if EHR
incorporates various features and technical
characteristics which make its use easy then not only
users’ will be motivated to use it but also will affect
their perception about the usefulness of the system.
In addition, findings imply that perceived ease of use
affect perceived usefulness. Thus, top management
should focus on software that is simple and easy to
use, in order to enhance staff performance and
productivity.
Moreover, the results indicate a strong
relationship between management support and
perceived ease of use and a less strong but
significant relationship with perceived usefulness.
Another strong relationship found between
intention to use EHR and social subjective norms. It
makes sense to say that in a working environment,
social relationships are evolved. People that care for
one another would give an advice to use the specific
software in order for their colleagues to achieve
better results at work.
Computer anxiety also plays an important role in
the acceptance of the EHR in hospitals. All three
hypotheses concerning the negative relationship
between computer anxiety and perceived ease of
use, perceived usefulness and self-efficacy are
confirmed. Top management should consider
fighting this phenomenon, since it is holding back
the progress of the hospital. This can be also proven
by the confirmation of the hypotheses regarding the
skills of each and every employee and perceived
usefulness and ease of use of the EHR.
Another key finding of this research is that
enjoyment is strongly related to intention to use,
perceived usefulness and perceived ease of use. It is
clear that once employees enjoy using computers in
their jobs, will be more determined to use EHR,
even if they have not used similar software in the
past.
5 CONCLUSIONS
AND LIMITATIONS
This research has focused on measuring the intention
to use EHR Greek hospital employees, designing
and empirically testing a new conceptual framework
(research model), which is an integrated version of
the initial technology accepted model (TAM).
Results show that intention to use the EHR is a
function of many factors which are interconnected to
one another. People intend to use EHR once they are
persuaded that these systems are easy to use and
very useful for their daily working life.
Although the sample of respondents is rather
large, the results cannot be generalized, since most
of these hospitals are using different (bespoke)
systems.
REFERENCES
Aggelidis V. P. and Chatzoglou P. D. (2008), “Using a
modified technology acceptance model in hospitals”,
International Journal of Medical Informatics, Vol. 78,
pp. 115-126.
Atlantis and Vidavo (2007), “Study on the use of
technology information technology and
communications in area health and welfare -
Deliverable P2: Recording and Analyzing the Current
Situation”, Observatory on the Information Society,
Athens
Atreja A., Gordon S. M., Pollock D. A., Olmsted R. N.,
Brennan P. J.& the Healthcare Infection Control
Practices Advisory Committee(2008), ‘Opportunities
and challenges in utilizing electronic health records for
infection surveillance, prevention, and control’,
Association for Professionals in Infection Control and
Epidemiology Inc., Vol. 36, pp. 37-46. Available
from:http://www.emeraldinsight.com/0024-2535-htm
Bakker A. R. (2007), “The need to know the history of the
use of digital patient data, in particular the HER”,
International Journal of Medical Informatics, Vol. 76,
p.p.438-441.
Callen J. L., Braithwaite J. and Westbrook J. I. (2007),
“Cultures in hospitals and their influence on attitudes
to, and satisfaction with, the use of clinical
information systems”, Social Science & Medicine,
Vol. 65, pp. 635-639.
Chatzoglou P. D., Sarigiannidis L., Vraimaki E. and
Diamantidis A. (2009), “Investigating Greek
Intention
to Use
Perceived
Ease of Use
Perceived
Usefulness
Self
Efficacy
Management
Support
Computer
Anxiety
Subjective
Norms
Enjoyment
0.83
0.27
0.52
0.28
0.42
0.47
-0.75
0.88
0.38
0.26
0.35
0.31
-0.75
-0.36
0.34
HealthInformationSystems-InvestigatingGreekHospitalEmployees'IntentiontoUseElectronicHealthRecords
191

employees’ intention to use web-based training”,
Computers & Education, Vol. 53, pp. 877-889.
Cross M. (2000), “Europe’s wrestling with electronic
patient record”, Doc. World 5.1, pp. 30-33
Dasgupta S., Granger M. and McGarry N. (2002), “User
acceptance of e collaboration technology: an extension
of the technology acceptance model”, Group Decision
and Negotiation, Vol. 11, No. 2 pp. 87–100.
Davis, F. D. (1986), “A technology acceptance model for
empirically testing new end-user information systems:
Theory and results.” Doctoral Dissertation, MIT Sloan
School of Management, Cambridge, MA.
European Commission Information Society (2010), “The
right prescription for Europe’s eHealth”, Europe’s
Information Society Thematic Portal [Online],
Available: http://ec.europa.eu/information
_society/activities/health/policy/index_en.htm
Greek National Healthcare System Reform Act 2001.
(N2889/2001 / FEK-Α/37/02.03.2001), Athens: Greek
Government Printing Office
Hayrinen K., Saranto K., Nykanen P. (2008), “Definition,
structure, content, use and impacts of electronic health
records: A review of the research literature”,
International Journal of Medical Informatics, Vol. 77,
pp. 291-304.
HealthConnect (2004), “Interim Research Report and
Draft Systems Architecture”, Federal Privacy
Commissioner Submission, Canberra
Hier D. B., Rothschild A., LeMaistre A., Keeler J. (2005),
“Differing Faculty and housestaff acceptance of an
electronic health record”, International Journal of
Medical Informatics, Vol. 74, pp. 657-662.
Jalal-Karim A. and BalachandranW. (2008), “The
National Strategies for Electronic Health Record in
three developed countries: General Status”, Proc. 12th
IEEE International Multitopic Conference, pp. 132-
138
Karahanna E., W. Detmar, J. Straub, L. Norman and M.
Chervany (1999), “Information Technology Adoption
Across Time: A Cross-Sectional Comparison of Pre-
Adoption and Post-Adoption Beliefs”, MIS Quarterly
Vol. 23, No 2.
Knaup P., Garde S., Merzweiler A., Graf N., Schilling F.,
Weber R. and Haux R. (2006), “Towards shared
patient records: An architecture for using routine data
for nationwide research”, International Journal of
Medical Informatics, Vol. 75, No. 3 pp.191-200.
Moon, J. W., and Kim, Y. G. (2001), “Extending the TAM
for a world-wide-web context”, Information &
Management, Vol.38, Issue 4, pp. 217-230.
Observatory on the Information Society (2007), “Study on
the use of technology information technology and
communications in area health and welfare – Survey
of international best practices”, Athens.
Orfanidis L., Bamidis P. D. and Eaglestone B. (2004),
“Data Quality Issues in Electronic Health Records: An
Adaptation Framework for the Greek Health System”,
Health Informatics Journal, vol. 10, pp. 23-36
Ovretveit J., Scott T., Rundall T. G., Shortell S. M.,
Brommels M. (2007), Implementation of electronic
medical records in hospitals: two case studies, Health
Policy, Vol. 84, pp.181-190.
Premkumar G. and A. Bhattacherjee (2008), “Explaining
Information Systems Usage: A Test of Competing
Models,” Omega, Vol. 36, No. 1, pp. 64-75.
Queensland Clinical Senate (2009), “Response to
Queensland Clinical Senate Recommendations”,
Queensland Government
Sistrom C. (2005), “The Socioeconomic Aspects of
Information Technology for Health Care with
Emphasis on Radiology”, Academic Radiology, Vol.
12, No 4, pp.232-256.
Shaw N., (2010), “Medical education & health
informatics: Time to join the 21st century?”, Cape
Town
Sherman G. (2001), “Toward electronic health records”,
Office of Health and Information Highway Health
Canada [Online], Available: http://www.hc-sc.gc.ca
Thompson T. G. and Brailer D. J. (2004), “The Decade of
Health Information Technology: Delivering
Consumer-centric and Information-rich Health Care”,
Department of Health and Human Services, United
States, Framework for Strategic Action
Trade Partners (2002), “Health and Medical Market in
Finland”, [Online] Available:
http://www.tradepartners.gov.uk/healthcare/finland/pr
ofile/overview.shtml
Venkatesh, V. (1999), “Creation of favourable
perceptions: exploring the role of intrinsic
motivation”, MIS Quarterly, Vol.23, Issue 2, pp. 239-
260.
Venkatesh, V. (2000), “Determinants of perceived ease of
use: integrating control intrinsic motivation and
emotion into the thechnology acceptance model”,
Information Systems Research, Vol.11, Issue 4, pp.
342-365
Venkatesh V., Morris M. G., Davis G. B. and Davis F. D.,
(2003), “User acceptance of Information Technology:
Towards a Unified view”, MIS Quarterly, Vol. 27, No
3, pp, 425-478.
Yi, M. Y., and Hwang, Y. (2003), “Predicting the use of
web-based information systems: self-efficacy,
enjoyment, learning goal orientation and the
technology acceptance model, Internation Journal of
Human-Computer Studies, Vol.59, Issue 4, pp. 431-
449.
Yu J., Ha I., Choi M. And Rho G. (2005), “Extending the
TAM for a t-commerce, Information & Management”
Vol. 42, No. 4, pp. 965–976.
HEALTHINF2013-InternationalConferenceonHealthInformatics
192
