
Ambient Assisted Living Technologies, Systems and
Services: A Systematic Literature Review
Alexandra Queirós
1
, Anabela G. Silva
1
, Joaquim Alvarelhão
1
, António Teixeira
2
and Nelson Pacheco da Rocha
3
1
Health Sciences School, University of Aveiro, Campo Universitário, 3810 Aveiro, Portugal
2
Electronics, Telecommunications and Informatics Department, IEETA, University of Aveiro
Campo Universitário, 3810 Aveiro, Portugal
3
Health Sciences Department, IEETA, University of Aveiro
Campo Universitário 3810 Aveiro, Portugal
Abstract. This paper intends to demonstrate that it is possible to classify
Ambient Assisted Living (AAL) services using the International Classification
of Functioning, Disability and Health (ICF), in particular its components
activities, participation and environmental factors. For this purpose a systematic
review of the literature on AAL services was undertaken and existing AAL
services summarized and characterized. To be included in this review articles
must have defined innovative concepts or characterized innovative
technologies, products or systems that can contribute to the development of the
AAL paradigm, with the aim of enabling people with specific demands (e.g.
elderly) to live longer in their natural environment. Results indicate that most
publications regarding AAL are technology-oriented with only a few articles
describing applications and scenarios. Results also indicate that it is possible to
link tasks to categories of the ICF components activities, participation and
environmental factors.
1 Introduction
1.1 Ambient Assisted Living
A digital environment with a pervasive and unobtrusive intelligence that is able to
proactively support people in their daily lives is the fundamental idea of the Ambient
Intelligence (AmI) concept [1]. AmI deals with new paradigms where computing
devices are spread everywhere (ubiquity) to allow intelligent and natural interactions
between the human being and the physical environment.
Within the AmI concept, AAL emerges as one of the most important developing
areas. The general goal of AAL solutions is to apply the AmI concept and
technologies to enable people with specific needs (e.g. elderly) to live longer in their
natural environment. In technological terms, the AAL comprises a heterogeneous
field of systems ranging from quite simple devices such as intelligent medication
Queirós A., G. Silva A., Alvarelhão J., Teixeira A. and Pacheco da Rocha N..
Ambient Assisted Living Technologies, Systems and Services: A Systematic Literature Review.
DOI: 10.5220/0003859400140026
In Proceedings of the 2nd International Living Usability Lab Workshop on AAL Latest Solutions, Trends and Applications (AAL-2012), pages 14-26
ISBN: 978-989-8425-93-5
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

dispensers, fall sensors or bed sensors to complex systems such as networked homes
and interactive systems.
The automation in an AAL environment can be viewed as a cycle that goes from
perceiving the state of the environment, to reasoning about it in order to achieve a
specific goal or anticipate outcomes of possible actions, and acting upon the
environment to change its state [2].
Like all intelligent agents, a smart environment relies on sensory data collected
from the real world. The perception of the environment requires that devices are
embedded in the environment with the purpose to allow the interaction of the
occupants with the technology.
When using the sensory data, the technological structure is able to perform
reasoning processes to select actions that can be taken to change the state of the
environment. Therefore, the data collected by the sensors have to be transmitted by a
communication network and pre-processed by a complex technological structure,
which collates and harmonizes data from different devices (it processes the raw data
into more useful knowledge such as models or patterns). To make that information
useful to the occupants of the environment, AAL systems must have a high level of
reasoning and decision-making abilities in order to arrive at a diagnosis and advice or
assist the human beings accordingly [2].
Action execution flows top-down. The action is transmitted by the communication
network to the physical actuators. These change the state of the surrounding
environment according to the instructions received.
Therefore, sensing, communicating and acting are crucial issues in the AAL
paradigm [3, 4]: i) sensing - a sensorial network is indispensable to obtaining accurate
information about the environment and its users; ii) communicating - all the
components of an AAL environment have to be interconnected in order to
communicate among them; iii) acting - any AAL environment must be able to act,
through various types of actuators, in order to achieve its objective.
Furthermore, AAL systems must be able; i) to properly distinguish the people
present in the environment; ii) to recognize the individual roles, needs, preferences
and limitations; iii) to recognize situational context; iv) to allow different answers
according to personal needs and situational contexts; v) to anticipate desires and
needs without conscious mediation.
Having all this information about its users, the AAL technological structure will
then be able to decide which services to provide, when and how to provide them and
to whom. This means, that the AAL technological structure should present a broad
range of intelligent functions for user management interface and context awareness
[5].
The existence of a variety of devices, such as sensor or video cameras, poses a set
of complex problems in terms of privacy and security, which require additional
developmental efforts.
An AAL environment comprises numerous invisible devices and ubiquitous
systems. Effective architectures are required to mask the effects of heterogeneous
physical devices, communication networks and intelligent components and systems.
Last but not least, the acceptance of the AAL paradigm is, obviously, closely
related to the quality of the available systems (e.g. private houses and home-care
assistance in the presence of users with different abilities and needs).
15

1.2 International Classification of Functioning, Disability and Health (ICF)
One of the objectives of AAL services is to improve the performance of a person in
their daily life. The AAL services use advanced technology to make that possible.
However, the focus of these services should be in the task that the person needs to
perform rather than in the technology used to perform it. As mentioned above, the
development of these services intends to give more autonomy and independency and
to increase the quality of life of the elderly. This development should be user-
centered.
The user-centered paradigm is also present in the care delivery where the
International Classification of Functioning, Disability and Health (ICF) will have an
important role [6]. The ICF offers a framework for conceptualizing functioning
associated to health conditions [7] and it considers that there are many factors that
affect and have influence on the individual’s performance and thereby on the
decisions made on the type of service needed or how it should be delivered (e.g. care
staff, relatives, aid appliances and technology).
The ICF structure distinguishes between the body, activities, participation and
contextual factors [8] and considers that they are all part of the individual's
functioning. Additionally, it considers the context (environmental factors and
personal factors) as components that can either enhance or hinder the performance of
the individual, depending on how he or she experiences limitations (e.g. due to
possible weakness, illness and/or handicap).
The environmental factors can have a positive (i.e. be facilitators) or negative
impact (i.e. be barriers) on the individual’s performance as a member of society, on
the individual’s capacity to execute actions or tasks, or on the individual’s body
functions or structures. When coding an environmental factor as a facilitator, issues
such as the accessibility of the resource, and whether access is dependable or
variable, of good or poor quality, should be considered.
In the case of barriers, it might be relevant to take into account how often a factor
hinders the person, whether the hindrance is great or small, or avoidable or not. It
should also be kept in mind that an environmental factor can be a barrier either
because of its presence (e.g. negative attitudes towards people) or its absence (e.g. the
unavailability of a needed service).
The ICF contains 1,424 codes organized according to an alphanumeric system.
Each code begins with a letter that corresponds to its component domain: b (Body
Functions), s (Body Structures), d (Activities and Participation) or e (Environmental
Factors). The letter is followed by between one and five numeric digits. Items are
organized as a nested system so that users can telescope from broad to very detailed
items depending upon the needs presented by particular applications of the ICF. The
broadest descriptor of functioning is represented by the chapter (domain) in which the
item appears. For example, chapter 5 of the Activities and Participation (d)
component of the ICF is Self-care. The next level of coding is what the ICF refers to
as the second level of detail or specification. These codes consist of the letter
indicating the component domain (b, s, d, or e) followed by three numeric digits. The
first numeric digit always corresponds to a chapter in that component domain in
which the code is found. Within the Self-care chapter, the code d540 (Dressing)
represents the second level of detail.
16

Assuming that AAL services intend to highlight environmental factors, i.e.
technology, to improve participation and quality of life it should be possible to
classify these services, taking into account how they impact on the user activities and
participation, particularly on his/her quality of life [9]. It can also be considered that
the AAL services may be classified as environmental factors, because they are
embedded in the context where a person performs the activities and they may either
facilitate or hinder to the individual’s performance.
2 Methods
The objective of this paper is to review the AAL literature and classify the existing
AAL services and to link these services to ICF activities, participation and
environmental factors. In order to achieve these aims, a systematic review of the AAL
literature published after 2007 was undertaken. The main features and areas of the
products and systems described in the literature reviewed which interlink and
improve new or existing technologies and systems were described. The methodology
used to conduct this systematic review is detailed in the following sections.
2.1 Data Sources and Searches
Studies were sought using health databases (PubMed, Web of Science, Academic
Search Complete and Science Direct) and Engineering and Technology databases
(Cite Seer and IEEE Xplore). Two key words were used without language restriction:
Ambient Assisted Living, as this was the main focus of this review, and Ambient
Intelligence because AAL is a sub-area of AmI. This means that technologies such as
user interaction or context awareness that are classified as AmI technologies are also
used in the AAL. However, not all the AmI systems are considered AAL systems.
The search was performed on the 23rd of February of 2011 and included all
references published since the 1st of January 2007. This data limit was established as
2007 was the year the Joint Programme “Ambient Assisted Living” from the
European Union was proposed [10].
2.2 Study Selection
After the initial screening, abstracts were sub classified by AQ, AGS and NPR into
one of 7 areas: i) architectures and frameworks; ii) physical devices; iii) context
awareness; iv) user interaction; v) privacy and security; vi) systems; vii) conceptual
articles. The operational definitions used in this review for each one of these areas
are:
Architectures and frameworks - abstraction of the structure and rules needed to
reason about AAL systems and how to implement them, including different
middleware approaches. In this class, we also included the articles describing
methodologies required to enable efficient, engineering deployment and runtime
management of ALL systems [11];
17

Physical devices - the hardware components required for the implementation of an
AAL system, including networks of sensors and actuators required to collect and
disseminate a range of environmental data [12];
Context awareness - technologies and methodologies to abstract and model the
situation of a person, place or object considered relevant to the interaction between a
user and a system [13];
User interaction - technologies and methodologies that enhance the effectiveness
and usability of a system and its interfaces [14];
Privacy and security - privacy and security challenges imposed by the AAL
implementation [15, 16];
Systems - practical AAL systems applied in a specified context and with a well
defined aim [17];
Conceptual articles - innovative concepts related to the AAL or that may
contribute to its development.
Considering that the final aim of AAL is to develop systems to enhance people’s
quality of life, it was decided to do a more detailed analysis of the articles included in
the sub-area systems. These articles were characterized in terms of: objectives, users,
settings, domains, developmental status and whether could be considered as real AAL
services. The activities that the services aimed to facilitate and the environmental
factors considered were also linked to categories from the ICF components activities
and participation and environmental factors, respectively-
3 Included and Excluded Articles
The databases searches resulted in 2427 references, of which 462 were duplicates and
1067 did not meet the inclusion criteria and, therefore, were excluded. Thus, a total of
845 references were included in this review (Figure 1).
Among the excluded articles, there were 28 that, despite not meeting the
previously defined inclusion criteria, were related to AAL and we decided to include
their references for further reading. These were on topics concerning ethical and legal
issues (n=18), market studies (n=8) and assessment of AAL systems (n=2).
3.1 Included Articles
Of the 845 included studies, 192 (23%) were classified as architectures and
frameworks, 130 (15%) as physical devices, 246 (29%) as referring to context
awareness, 113 (13%) as user interaction, 34 (4%) as related to privacy and security,
88 (11%) as systems and 42 (5%) as conceptual papers defining innovative concepts.
The higher number of publications on context awareness may be related to the
knowledge that the individual performance is not only affected by the individual
abilities but also by the characteristics of the environment, which can either facilitate
or hinder the individual performance [8].
18
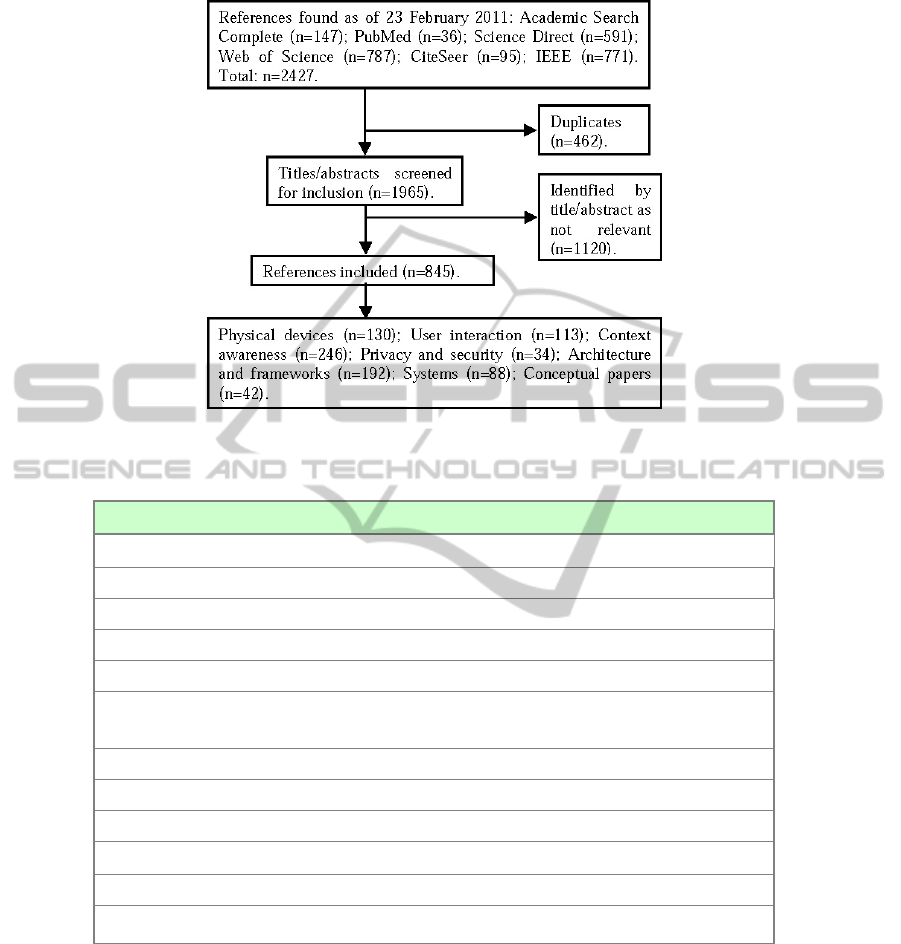
Fig. 1. Flow chart for the systematic review.
Table 1. Number of articles in each area and sub-area.
Area and Sub-area
Architecture and Framework (192):
Architecture (152); Design and Development Methodologies (37); Safety (3).
Physical Devices (130):
Sensors Network (75); Robotic (32), New technologies (23).
Context-awareness (246):
Environment (18); Location / Tracking (32); Identity Management (12); Identity Management and
Location (8); Detection of Specific Events and Situations (18); Activity / Interactions (41); Human
Behavior (25); Emotions (10); Reasoning (82).
User Interaction (113):
New Interfaces (52); Personalized Information (7); Design (44); Evaluation (10).
Privacy and Security (34).
Systems (88).
Conceptual papers (42):
Sensors network (2); User Interaction (6); Technology Development (6); Context awareness (2); Living
Lab (5); Future Challenges for the AAL Systems (21).
It was necessary to sub-divide the major 7 areas identified in the study selection
because the areas they covered very broad subjects. Thus, the main area of
architectures and frameworks was sub-divided into architecture, design and
developmental methodologies and safety. The main area of physical devices was sub-
divided into sensors networks, robotics and new technologies. Context-awareness
technologies were sub-classified into environment, identity management and location,
19

location/tracking, detection of specific events and situations, activity/interaction,
human behavior, emotions and reasoning. User interaction included the sub-areas of
new interfaces, personalized information, design and evaluation of user interfaces.
AAL systems included the issues of security and privacy related to the individual and
to the context so that the user receives adequate support. However, there were not
clearly distinct areas of research within this topic and, consequently, the articles were
not sub-classified. A total of 42 articles were classified as conceptual papers on the
following sub-areas: sensors network, user interaction, technology development,
context awareness, living lab and future challenges for the AAL systems. A total of
88 articles were classified as systems. The Table 1 shows the number of articles
identified by area and sub-area.
4 Results and Discussion
As AAL is related to the complex interaction of a variety of technology and system
components that aim to enhance people’s life we decided to perform a more detailed
analysis of the articles classified as systems as referred in the methodology.
Most systems were intended for use both indoor and outdoor in any environment
or at home. This may be related with an attempt to improve people’s life in their
natural environment. The system described by Chuan-Jun and Bo-Jung [18] is to be
used in outdoor environment and allows the location of the elderly anywhere in the
community. Caregivers may locate care-receivers easily in a community with RFID
while a Mobile Agent furnishes timely and accurate information for care provision.
Systems were conceived to be used in a variety of areas with the general aim of
directly or indirectly improve the individuals’ quality of life. Most systems were
conceived to help care delivery either by health professionals or by any formal or
non-formal caregiver. Most of these aimed at monitoring and controlling biological
signs and behaviors’ such as heart rate or falls. The ultimate goal is to provide the
caregiver with accurate, up to date information so that the right care can be delivered
at the right time. The remaining systems are on very diverse areas with very diverse
objectives such as security, information, domotics, user interface, entertainment,
mobility, shopping, self-care, culture, tourism, involvement in community events,
physical activities and education.
The World Health Organization (WHO) defined Health, Participation and
Security as the three pillars of a policy framework for active ageing. The ALLIANCE
Project supported by the European Commission, that aimed to coordinate a European
AAL Community, also defends that this three areas are very important to the elderly
[19]. When considering the scope of the analyzed systems, one was classified as
Security, while the others were classified as Health or Participation. Interestingly, a
high percentage of articles describe systems that aim to enhance fundamental
activities such as involvement in community events, self-care or mobility. This may
indicate that the priority of existing systems is to facilitate the fundamental activities
of an individual. However a few studies also describe systems that aim to facilitate
activities more related to quality of life (e.g. physical activities or tourism). These
studies use technologies that take advantage of existing knowledge on context
20
awareness. For example, the research presented by Ahn [20] is a novel approach to
evaluate customer aid functions with agent-based models of customer behavior and
evolution strategies that builds on existing knowledge on context-awareness
technology. Agent-based modeling is used to imitate users' rational behavior at
Internet stores with regard to browsing and collecting product information.
Of the 88 abstracts classified as systems, 77 described systems that use existing or
new technologies to solve very specific problems (e.g. a robot to assist elderly in a
particular daily activity). The other 11 articles (Table 2) describe systems showing a
higher level of complexity and aggregating functions to answer to a broad range of
needs in daily life situations [21]; [22]; [23]; [24]; [25]; [26]; [27]; [28]; [29]; [30];
[31]. An example is the system described by Bravo et al. [23] that is to be used in a
day centre or at home to monitor the behavior of patients with Alzheimer disease as
well as their vital signs. This information is then sent to caregivers and allows them to
identify emergency situations and provide the appropriate care. However, the system
is also used to assist patients in daily activities in order to promote their autonomy.
Table 2. Objectives of the AAL systems found.
Objective Article
Diagnose, prevent and treat patients with diabetes mellitus [21].
Personal assistant [22].
Complement and support daily activities [23]; [24]; [25]
Promote well-being and health [26]; [30].
Monitor and collect vital signals [27].
Promote autonomy [28].
Promote participation [29].
Assist tourism [31].
One of the objectives of this paper was to analyze the 11 articles considered as
real AAL services and describe the activities and participation that these services aim
to improve. As mentioned above, it is possible to link the tasks involved in the AAL
services and categories of the ICF component activities and participation. The
activities and participation found in the articles were linked to the following
categories: Focusing attention (d160); Reading (d163); Writing (d170); Calculating
(d172); Solving problems (d175); Caring for body parts (d520); Looking after for
one’s health (d570); Caring for household objects (d650); Assisting others (d660);
Informal social relationship (d750); Family relationship (d760); Community life
(d910); Recreation and leisure (d920); and Religion and spirituality (d930).
Table 3 shows the activities and participation presented in the articles linked to the
ICF categories.
As referred in the introduction, external factors can contribute to improve person’s
performance (i.e. the context where the tasks are completed may influence the
performance of a person). The concept of AAL can be defined as the use of
technologies to improve a person’s performance in a specific life situation. Thus, it is
possible to link the AAL services to ICF’s environmental factors.
21
Table 3. ICF’s activities and participation described in the articles classified as real AAL
systems.
Activities and Participation Articles
d160, d163, d166, d170, d172, d175 [27].
d520 [21].
d570 [21]; [22]; [26]; [28]; [29].
d650 [22]; [28].
d660 [23]; [24]; [27].
d750, d760, d930 [29].
d910 [22]; [26]; [29].
d920 [21]; [22]; [26]; [29]; [31].
When analyzing the 11 articles classified as AAL services, it was possible to
identify 10 environmental factors, according to the ICF: Products and technology for
personal use in daily living (e115); Design, construction and building products and
technology for gaining access to facilities in buildings for private use (e1551);
Immediate family (e310); Extended family (e315); Friends (e320); Acquaintances,
peers, colleagues, neighbours and community members (e325); Health professionals
(e355); Transportation services (e5400); Social security services (e5700); and Health
services (e5800). Table 4 presents the environmental factors classified according to
the ICF.
Table 4. ICF’s environmental factors described in the articles classified as real AAL systems.
Environmental Factors Articles
e115 [21]; [22]; [26]; [27]; [29]; [31].
e1551 [21]; [22]; [26]; [27].
e310 [24]; [29].
e315, e320, e325, e5700 [29].
e355 [23]; [24].
e5400 [31].
e5800 [21]; [23]; [24]; [26]; [27].
It is clear from Tables 3 and 4 that the activities, participation and environmental
factors described in real AAL systems are only a small part of those described in the
ICF.
5 Conclusions
The results of this systematic review indicate that there is a great amount of literature
on AAL encompassing very diverse areas.
Most of the literature on AAL is technology-oriented, what is reflected in the high
number of articles on specific components (89%) when compared to only 88 articles
(11%) on complete systems. In addition, a considerable number of these 88 articles
22

on systems focus on how the technology can be used in the AAL context instead of
looking at the users’ needs and proposing ways in which the technology can be used
to solve them. The focus is on the technology rather than on the person.
A high number of systems are conceived to help care delivery either by health
professionals or any formal or non-formal caregiver. This is probably related to the
continuous ageing of the population. With ageing there is a decrease in functioning
associated with an increase in a variety of chronic diseases which leads to a higher
consumption of healthcare services [32]. This challenges the traditional healthcare
system. It is likely that the scarcity and costs of health resources compromise the
ability of the health system to appropriately respond to a population that not only
wants to live longer, but to live with autonomy and quality of life [33]. Furthermore,
AAL systems can contribute to the reorientation of health systems that are currently
organized around acute, episodic experiences of disease, by allowing the
development of a broad range of systems promoting care prevention and care
promotion and home-caregiver support [34]. A considerable number of
technologies/systems are developed for elderly users or users with disabilities, what
may be related with the previously referred demographic changes and constitute an
attempt to answer to the specific needs of these users. However, the emphasis needs
to shift from specific groups of users to the general user/population by developing
intelligent systems with the technology embedded in the environment that can
automatically select the output and input information and mode according to the
specific needs and characteristics of the users, in line with the principles of the
Design for All [35]. Therefore, AAL technologies would be usable by all people,
independently of their abilities, age or health condition. This will contribute to
decrease the price of this technology which is one of the main barriers to its
widespread use. Interestingly, an important step towards this direction is being given
by using the intelligent AAL component (e.g. context awareness and user interaction)
to develop technologies that consider not only the person, but the activity being
performed and the context in which it is taking place. This is in line with the WHO
International Classification of Functioning, which sees the environment as a crucial
factor modulating the person’s activity and participation as a member of the society
[8].
The activities and participation considered in the AAL systems indicate that these
services are directly related to the Health and Participation areas of the WHO’s
definition of active ageing. Only one activity and participation was found related to
the Security area. This can be explained because one of the main objectives of AAL
is to improve the active ageing what requires the creation of services adapted to the
needs of the elderly using advanced technology, like sensors, monitoring devices or
communication technologies. Most of the activities and participation that were
implicit in communication or participation in society can also be seen as a way to
promote health. For example, Busuoli [26] describes a service that is related to the
virtual communities and aims to improve the knowledge on diabetes; Dadlani [27]
uses computer games to cognitively stimulate the elderly. In what concerns security it
is more difficult to identify activities and participation that can translate the feeling of
security by the point of view of the caregiver. Services that refer to security were
linked to the category d660 (Assisting others) of the component activity and
23

participation. Other possibility would have been to link it to a personal factor related
to emotions, personality and personal characteristics of a person.
Considering the presence of environmental factors in AAL services it was clear
that technologies and services that use actuators, sensors, and cameras may be
classified as e115 (Products and technology for personal use in daily living) or e1551
(Design, construction and building products and technology for gaining access to
facilities in buildings for private use). These two environmental factors were present
in all the articles describing AAL services. One explanation for this is, as argued by
Bravo [24], “the idea is that the user should focus on the task and that technology
should disappear”. The other environmental factors that were identified are related to
the activities and participation and aimed to improve relationship, community life,
recreation and leisure. Obviously, social support networks (formal or informal) have a
major impact in these activities and according to the ICF can be classified as
environmental factors.
To summarize, this review of existing literature on AAL highlights the need to
rethink the future research approach on the development of AAL systems in order to
take advantage of already existent technologies and systems. The difficulty found
when classifying the articles also suggests the need for a common classification that
could be used to characterize existing AAL systems. Furthermore, according to what
was described in the previous sections, the needed requirements to deliver viable,
adaptative and personalized AAL systems are still not fulfilled. There is a general
tendency to develop AAL systems from the scratch with specific solutions. Therefore,
there is a need for a normalized and coherent technological sub-stratum over which
AAL systems could be developed to answer the real demands of the users.
Acknowledgements
This work is part of the COMPETE - Program Operacional Factores de
Competitiviade and the European Union (FEDER) under QREN Living Usability Lab
for Next Generation Networks (LUL) (http://www.livinglab.pt) and QREN Primary
Healthcare ALL Services (AAL4ALL) (http://www.aal4all.org/).
References
1. Ramos, C.: Ambient Intelligence - A State of the Art from Artificial Intelligence
Perspective. EPIA 2007 (2007), 285-295.
2. Cook, D., and Das, S.: How smart are our environments? An Updated Look at the State of
the Art. Pervasive and Mobile Computing 3 (2007), 53-73.
3. Camarinha-Matos, L., and Vieira, W.: Intelligent Mobile Agents in Elderly Care. Robotics
and Autonomous Systems 27 (1999), 59-75.
4. Costa, R., Carneiro, D., Novais, P., Lima, L., Machado, J., Marques, A. and Neves, J.:
Ambient Assisted Living. 3rd Symposium of Ubiquitous Computing and Ambient
Intelligence (2008), 86-94.
5. Hoareau, C., and Satoh, I.: Modeling and Processing Information for Context-Aware
24

Computing: A Survey. New Generation Computing 27 (2009), 177-196.
6. Whiteneck, G., Dijkers, M.: Difficult to Measure Constructs: Conceptual and
Methodological Issues Concerning Participation and Environmental Factors. Archives of
Physical Medicine and Rehabilitation. Vol. 90, Issue 11, Supplement (2009), S22-S35.
7. Peterson, D. B.: International Classification of Functioning, Disability and Health: An
Introduction for Rehabilitation Psychologists. Rehabilitation Psychology. Vol. 50, No. 2
(2009), 105–112.
8. World Health Organization: International Classification of Functioning, Disability and
Health (ICF), (2001).
9. Queiros, A, Alvarelhão, J., Silva, A., Amaro, A., Teixeira, A. Rocha, A.: The International
Classification of Functioning, Disability and Health as a Conceptual Framework for the
Design, Development and Evaluation of AAL Services for Older Adults. Proceedings of
the 1
st
International Living Usability Lab Workshop on AAL Latest Solutions, Trends and
Applications, AAL 2011, in conjunction with BIOSTEC 2011 (2011), 46-59.
10. European Union: Opinion of the European Economic and Social Committee on the
Proposal for a Decision of the European Parliament and of the Council on the Participation
by the Community in a Research and Development Programme Aimed at Enhancing the
Quality of Life of Older People through the Use of new Information and Communication
Technologies (ICT), undertaken by several Member States COM(2007) 329 final -
2007/0116 (COD) (2007).
11. Bavafa, M., and Navidi, N.: Towards a Reference Middleware Architecture for Ambient
Intelligence Systems. Knowledge Engineering, 8th International Conference on ICT
(2010), 24-25.
12. Snijders, F.: Ambient Intelligence Technology: An Overview. In Ambient Intelligence,
edited by W. Weber, J. Rabaey and E. Aarts. Berlin: Springer (2005).
13. IST Amigo Project: Deliverable D2.2 - State of the Art Analysis including Assessment of
System Architectures for Ambient Intelligence (2005).
14. IST Amigo Project: Deliverable D2.3 Specification of the Amigo Abstract System
Architecture (2005).
15. Al Bouna, B., Chbeir, R. and Marrara, S.: A Multimedia Access Control Language for
Virtual and Ambient Intelligence Environments. Sws'07: Proceedings of the 2007 ACM
Workshop on Secure Web Services (2007), 111-120.
16. Bogdan, R., Ancusa, V. and Vladutiu, M.: Fault Tolerance Issues in Non-traditional Grids
Implemented with Intelligent Agents. ICCCE 2008, International Conference on Computer
and Electrical Engineering (2008), 912-917.
17. Sun, H., De Florio, V. Gui, N. and Blondia, C.: Promises and Challenges of Ambient
Assisted Living Systems. ITNG '09, Sixth International Conference on Information
Technology: New Generations. (2009), 27-29.
18. Chuan-Jun, S. and Bo-Jung, C.: Ubiquitous Community Care Using Sensor Network and
Mobile Agent Technology. Ubiquitous Intelligence & Computing and 7th International
Conference on Autonomic & Trusted Computing (UIC/ATC) (2010).
19. Broek, G. V. D., Cavallo, F. Odetti, L. and Wehrmann, C.: Ambient Assisted Living
Roadmap, AALIANCE - The European Ambient Assisted Living Innovation Alliance
(2008).
20. Ahn, H. J.: Evaluating Customer Aid Functions of Online Stores with Agent-based Models
of Customer Behavior and Evolution Strategy. Information Sciences 180 (2010), 1555-
1570.
21. Bal, N., and Schwarz, M.: Ambient Assisted Living for Type 2 Diabetic Patients. 4th
Internat. Conference on Pervasive Computing Technologies for Healthcare (2010), 22-25.
22. Boll, S., Heuten, W. Meyer, E. M. and Meis, M.: Development of a Multimodal Reminder
System for Older Persons in their Residential Home. Informatics for Health & Social Care
35 (2010), 104-124.
25

23. Bravo, J., Fuentes, C., Hervas, R., Casero, G., Gallego, R. and Vergara, M.: Interaction by
Contact for Supporting Alzheimer Sufferers. 3rd Symposium of Ubiquitous Computing and
Ambient Intelligence (2009), 125-133.
24. Bravo, J., Lopez-de-Ipina, D., Fuentes, C., Hervas, R., Pena, R., Vergara, M. and Casero,
G.: Enabling NFC Technology for Supporting Chronic Diseases: A Proposal for Alzheimer
Caregivers. Ami 2008, Ambient Intelligence Conference (2008), 109-125.
25. Casas, R., Marin, R. B., Robinet, A., Delgado, A. R., Yarza, A. R., McGinn, J., Picking, R.
and Grout, V.: User Modelling in Ambient Intelligence for Elderly and Disabled People.
11th International Conference on Computers Helping People with Special Needs (2008),
114-122.
26. Busuoli, M., Gallelli, T., Haluzik, M., Fabian, V., Novak, D. and Stepankova, O.:
Entertainment and Ambient: A new OLDES' View. Conference on Universal Access in
Human-Computer Interaction: Applications and Services (2007), 511-519.
27. Dadlani, P., Sinitsyn, A., Fontijn, W. and Markopoulos, P.: Aurama: Caregiver Awareness
for Living Independently with an Augmented Picture Frame Display. AI & Society 25
(2011), 233-245.
28. Niemela, M., Fuentetaja, R. G., Kaasinen, E. and Gallardo, J. L.: Supporting Independent
Living of the Elderly with Mobile-centric Ambient Intelligence: User Evaluation of three
Scenarios. Ami 2008, Ambient Intelligence Conference (2007), 91-107.
29. Romero, N., Sturm, J., Bekker, T. Valk, L. and Kruitwagen, S.: Playful Persuasion to
Support Older Adults' Social and Physical Activities. Interacting with Computers 22
(2010), 485-495.
30. Tocino, A. V., Gutierrez, J. J. A., Navia, I. A., Penalvo, F. J. G., Castrejon, E. P. and Giner,
J.: Personal Health Monitor. New Directions in Intelligent Interactive Multimedia Systems
and Services. (2009), 465-475.
31. Vansteenwegen, P., Souffriau, W., Berghe, G. V., and Van Oudheusden. D.: The City Trip
Planner: An Expert System for Tourists. Expert Systems with Applications 38 (2011),
6540-6546.
32. World Health Organization: Active Ageing: A Policy Framework (2002).
33. Kairy, D., Lehoux, P., Vincent, C. and Visintin, M.: A Systematic Review of Clinical
Outcomes, Clinical Process, Healthcare Utilization and Costs Associated with
Telerehabilitation. Disability and Rehabilitation, 31(2009), 427–447.
34. PERSONA: PERceptive Spaces prOmoting iNdependent Aging, Deliverable 2.1.1 - Report
Describing Values, Trends, User Needs and Guidelines for System Characteristics in the
AAL Persona Context (2008).
35. Bühler, C., and Placencia-Porrero, I.: eEurope - Participation for All Action Line:
Networking Centres of Excellence in Design-for-All and Developing an EU curriculum in
Design for All - Final Report. Brussels: European Comission (2002).
26
