
COMPANION: SOCIAL SUPPORT NETWORKING
TECHNOLOGY FOR SURVIVORS OF SUICIDE
Elizabeth M. LaRue, Ann M. Mitchell
School of Nursing, University of Pittsburgh, 415 Victoria Buildingt, Pittsbirgh, PA, 15261 U.S.A.
Hassan Karimi, Piyawan Kasemsuppakorn and Duangduen Roongpiboonsopit
Geoinformatics Laboratory School of Information Sciences
University of Pittsburgh, 713 IS Building, Pittsburgh, PA, 15261 U.S.A.
Keywords: Mobile phones, Communication, Information dissemination, Survivors of suicide, Social support networks.
Abstract: This position paper presents a conceptualization of a model of a survivor of suicide’s (SOS) social support
network. By knowing the actors in a SOS’s social support network, information can be customized and
delivered directly to them at the time of their greatest need. This has the potential to improve the current
treatment available for survivor’s of suicide and positively influence the bereavement process, bereavement-
related outcomes, and health-related quality of life for everyone in the social support network. We will
briefly describe suicide survivorship, present our model of the social support network, and COMPANION –
our location based mobile support system designed to connect social support network members. We believe
this will enable use to describe the communication use and patterns of the SOS’s social support network and
positively impact their health related quality of life.
1 INTRODUCTION
In the United States, suicide is the eleventh leading
cause of death, accounting for about 30,000 to
32,000 deaths annually (McIntosh, 2008). For each
person who completes suicide, there may be, a
minimum of 7-10 survivors (persons close to the
suicide victim) left to cope with the loss. While there
is no need for immediate medical treatment for most
of the estimated 300,000 survivors, there is a need
for social support for those individuals close to the
suicide victim (Mitchell et al., 2004). Without social
support, these survivors may be at an increased risk
for developing anxiety, depression, complicated
grief, and post-traumatic stress symptoms.
The current support services available for
survivors of suicide (SOS) include counselling and
bereavement support groups. Only those survivors
who seek out support services are receiving care. In
times of sudden crisis, e.g., suicide, multiple people
experience the feeling of losing control and
diminished faith. The actual number of people
suffering from this type of crisis is unknown.
During the bereavement process and times of
sudden crisis the strength of relationships are tested
and various people within the network of friends
take on roles of support in the relationship (e.g.,
friend, cousin, therapist, faith leader, etc.). By
analyzing the natural social support system that
establishes itself to help persons through these
difficult times, we will better understand the type of
support requested and offered, as well as the timing
for social support services available for these
vulnerable individuals. This paper will present our
proposed model of a SOS’s social support network
and an overview of COMPANION. COMPANION
is a location based mobile support system designed
to connect social support network members. It is
expected to discover and enhance the flow of
communication, recognize the survivor’s geographic
location when requesting support and requiring
information, as well as the dissemination of
information among a SOS’s social support network.
COMPANION will test the validity of the model.
357
M. LaRue E., M. Mitchell A., Karimi H., Kasemsuppakom P. and Roongpiboonsopit D. (2009).
COMPANION: SOCIAL SUPPORT NETWORKING TECHNOLOGY FOR SURVIVORS OF SUICIDE.
In Proceedings of the International Conference on Health Informatics, pages 357-362
DOI: 10.5220/0001774003570362
Copyright
c
SciTePress

2 BACKGROUND
The introduction of mobile technologies is changing
and influencing the way society communicates as
well as the entire framework of society. The primary
determinants of communication, space and time, are
quickly disappearing as the introduction of mobile
phones into society keeps people available for
contact wherever they are at any time of day.
Patterns of communication that were shaped by a
person’s central geographic position in respect to the
social network they participated in, as well as their
ability to share information, are no longer restricted
by human relocation or geographic boundaries
(Hossain et al., 2007). They are now configured and
arranged by the relevancy of the information one has
to give to the network. This shared information is
only relevant if it fits the needs of the users within a
social network, the available operating system in the
technology used to communicate, and the geo-
graphic environment of the user at the time of their
communication/information needs.
A social network is the structure existing among
a set of people and their relationships that act as a
source of social support. Social support has been
defined as all or part of the following: the act of
providing a resource; the outcome of support (such
as having a sense of well-being or being cared for);
and as a relationship between the recipient and
provider. While different from the concept of social
support, social networks and social support are inter-
related.
Social support networks can occur naturally or
can be created by commonality of circumstances. It
has been theorized that social support creates an
interpersonal environment that alleviates
accumulated stress that might overwhelm the
individual's ability to cope while also contributing to
the adaptive capacity of the individual. It has been
argued that the main effects of social support
influences health by way of the social network
(Cohen, 1991). When a SOS does not utilize a social
support network, the likelihood of experiencing
complicated grief symptoms is increased.
As part of the social support network, family
members and friends of the deceased may also
experience devastating psychological effects when a
death by suicide occurs. Affective, behavioral, and
cognitive changes may occur during the period of
bereavement. If they go untreated, the possibilities
for severe psychological changes increase. To
illustrate the experience of survivors following a
death by suicide, the theory of social impact can be
used. With this theory the affective, behavioral, and
cognitive changes in a person occur because of the
impact of an information source (e.g., a person, a
document, a movie, etc.) with respect to: the number
of others recommending the information; who gives
the information; the geographic closeness of the
person giving the information, and the strength of a
particular individual within the network. By building
new utilities and manipulating the available
functions, short text messages services (SMS), short
multi-media messages services (MMS), etc…, on
mobile phones and applying the social impact
theory, there is the potential to prevent a
bereavement-related crisis in survivors of suicide.
Communication establishes structure for society.
Methods of communication vary from hand signals,
to verbal exchanges, to reading the written word, or
viewing pictures. Mobile phones are a tool that
increases the ability to communicate with voice,
text, and images at any time and in any geographic
environment. Following the patterns of information
sharing in social networks, a SOS’s network will
have an inner-network of people in close proximity,
either geographically, physically, or emotionally,
and an outer-network of people, either geo-
graphically, physically, or emotionally. Each person
within the network may be conceptualized as being
an actor, playing a role within the support system.
The relationships established by the actors in the
network are built on the amount of time spent
communicating, the emotional intensity among the
actors, mutual confiding, and the offering of
reciprocal services. Figure 1 illustrates our proposed
model of a SOS’s social support network. Depicted
are the possible actors in the social support network.
The actors have been divided into two resource
groups, personal and clinical, revealing the role they
play within the social network and their role within
the support system (throughout the bereavement
process).
At this time, there is no published literature
defining a survivors’ of suicide social support
network, their communication patterns, or their
information needs. We propose that by using
COMPANION and providing appropriately tailored
information, it will be possible to enhance the
health-related quality of life (QOL) for survivors,
and inhibit severe psychological changes in
survivors of suicide as they live through the
bereavement process.
HEALTHINF 2009 - International Conference on Health Informatics
358
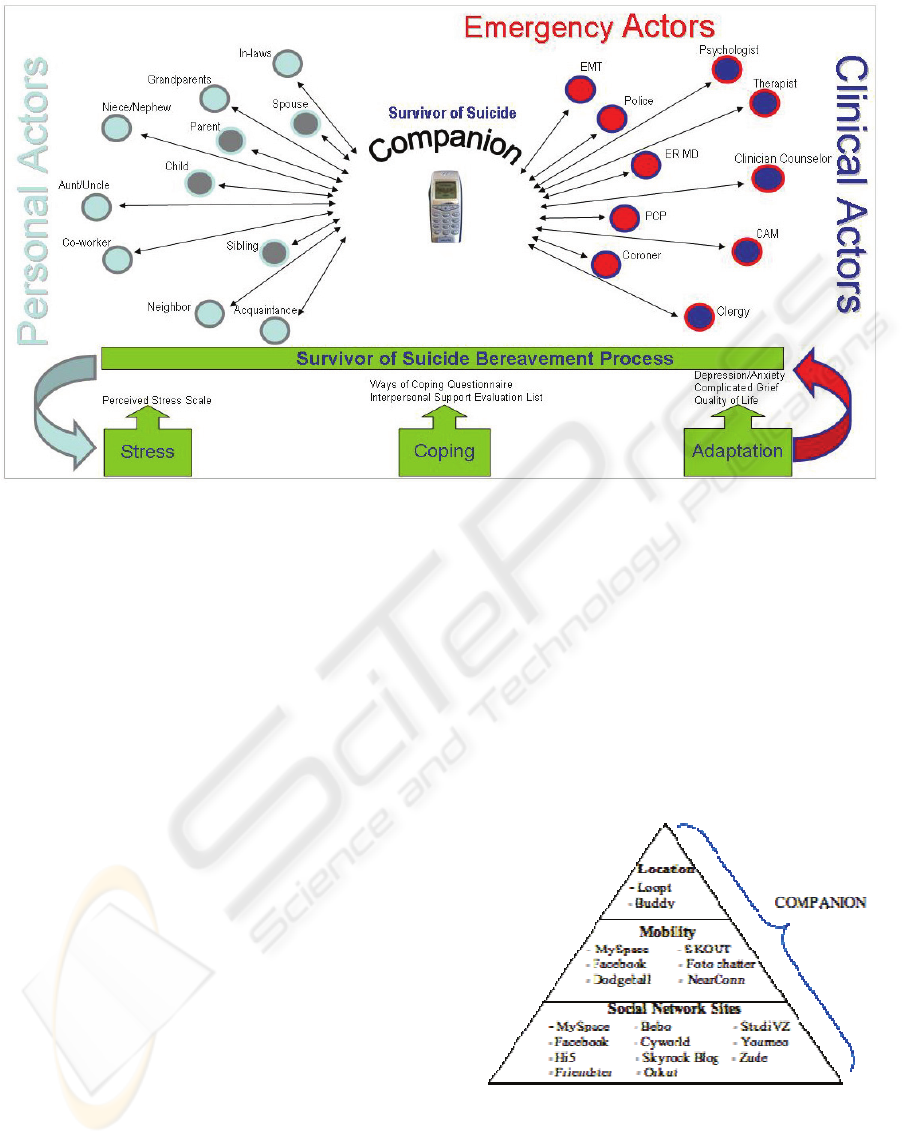
Figure 1: Survivor of Suicide Social Support Network.
3 COMPANION ENVIRONMENT
Human communication has changed substantially in
recent years due to rapid technological
developments such as the Internet and wireless
networks. Both of these tools have promoted a
change in social networks. Technology has played a
primary role in changing the way society
communicates through the development of a social
network services. This type of service is a web-
based technology providing a virtual community for
people with similar interests or activities to
communicate and share information. Figure 2 shows
an overview of our proposed location-based social
networking by highlighting the relationships
between the three categories of social networks.
Presently, the majority of existing social network
applications falls under the first category, social
network sites. Boyd and Ellison (2007) define social
network sites as “web-based services that allow
individuals to (1) construct a public or semi-public
profile within a bounded system, (2) articulate a list
of other users with whom they share a connection,
and (3) view and traverse their list of connections
and those made by others within the system. The
nature and nomenclature of these connections may
vary from site to site.”
The second type of social network is mobility.
These are social networks that permit interaction
with another person that has similar interests or
activities using mobile devices (e.g., cellular
phones). The inclusion of this technology has been
slowly incorporated and only included in a few
social network applications since 2006 (Boyd and
Ellison, 2007). Even since then, the modes of
communications are limited within the network.
The third type of social network is location
based. This category provides users the ability to use
mobile devices equipped with geo-positioning
technologies (e.g., GPS) to find locations of places
and social network members
Figure 2: Location-Based Social Networks.
COMPANION, as a social network environment,
combines all three categories of the social network
technologies by using such services as SMS, and
MMS, e-mail, photos, video, maps, and the Internet
on GPS-based cellular phones. COMPANION will
COMPANION: SOCIAL SUPPORT NETWORKING TECHNOLOGY FOR SURVIVORS OF SUICIDE
359
have the capability to connect information resources,
personal resources, and clinical resources, through
location-based features. This will provide survivors
of suicide with various options for obtaining
information such as searching for points of interests
and route directions – either walking or driving in
real-time
3.1 Architecture and Components
We will develop COMPANION in two versions to
test this model. The first version of
COMPANION_v1, will be capable of performing
generic and basic functions to facilitate common
social, clinical, and professional tasks. This specific
information will allow COMPANION to gain
knowledge about survivor’s behavior as well as to
understand specific needs of each survivor. The
second version of COMPANION_v2, will utilize
knowledge gained from the first version in order to
personalize, learn, and predict survivors’ behaviors
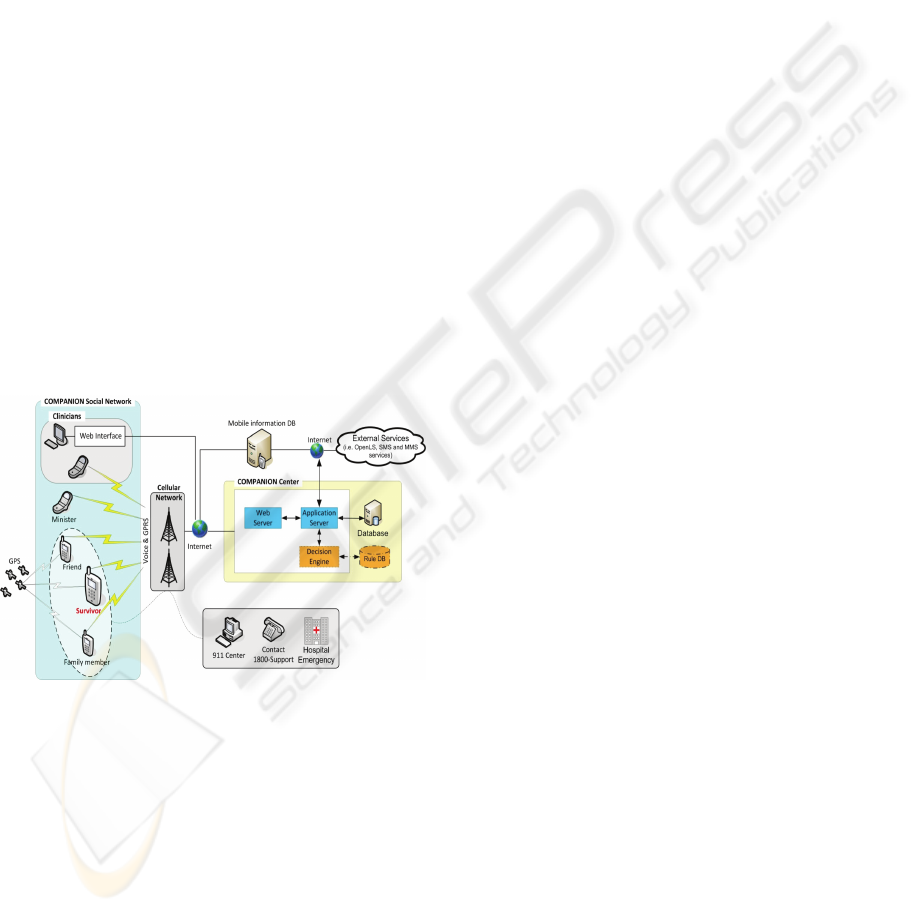
and interests and information needs. Figure 3
illustrates the high-level concept of COMPANION.
COMPANION is based on a three-tier
architecture: client, middle tier server, and database
server. There are two components: COMPANION
social network and the COMPANION center.
Figure 3: COMPANION Architecture.
3.1.1 COMPANION Social Network
The COMPANION social network consists of
clients, which are mobile units and stationary units
(workstations), in the three-tier design as depicted in
Figure 3. The mobile units are cellular phones
equipped with GPS and be capable of such
functionalities as: voice, SMS, and MMS. By
providing professional members (such as spiritual
leaders or clinicians) with these cellular phones, they
can provide medical and spiritual support via a voice
call before or after the system communicates with
them through SMS and MMS messages.
The COMPANION phones will exchange
information with the COMPANION center via the
Internet. The COMPANION phones will feature
speed dials to local emergency services, contact
services 1-800-support (local suicide hotlines),
emergency numbers for local hospitals, include
sensors allowing the COMPANION center to
monitor and query specific information, such as the
users reported emotional status, URL access, and
call history. When utilizing the GPS unit on the
social support member’s phone, COMPANION will
assist the user in locating other members and
geographically direct the user to predetermined
activities or spontaneous activities.
By collecting personal information on each
survivor through COMPANION and transferring it
to the COMPANION center, the system will
construct knowledge for the next generation of
COMPANION (i.e., COMPANION_v2).
The stationary units in the COMPANION social
support network, provide authorized clinicians
access to review a survivor’s information through a
secure web page. COMPANION_v1 will provide
only a high-level summary of the survivor’s reported
emotional state, frequency of cell phone use, and
utilization of location data. COMPANION_v2 will
be able to provide combined information to reveal
spatial patterns that are found to impact a survivor’s
emotional state and suggest locations that the
survivor should avoid because of psychological
effects (e.g., bridges). Moreover, COMPANION_v2
will feature a set of rules that the system should
respond to for each individual’s actions – such as a
text alert to the survivor’s social support network if
the survivor does not communicate in anyway with
COMPANION over a period of time.
3.1.2 COMPANION Center
The COMPANION center consists of two main
components: middle tier server and database server.
The middle tier server includes a web server and an
application server. The web server provides HTTP
portal services for web clients. This server is
responsible for data integrity and the conversion of
data into a format that can be viewed on a client
screen. The application server provides the core
functionalities of COMPANION, the logic, and the
data access. This server also will be capable of
requesting additional services from external
providers such as mapping services, and pre-
programmed support text messages (push
technology). The application server will be able to
retrieve communication transactions (such as call
history, SMS and MMS messages, and URL access)
HEALTHINF 2009 - International Conference on Health Informatics
360

located in a mobile information database from each
survivor’s COMPANION phone. This mobile
information could be accessed through a service
provided by the designated network provider or a
third-party software provider that is able to handle
the personal information of cellular phone usage
confidentially and securely.
The second component of the COMPANION
center is the database server. The database server is
responsible for data storage and management. Two
types of data will be contained in this database,
spatial and non-spatial data. Spatial data include
historical trajectories of each survivor, locations of
the social network members, and tagged locations.
Non-spatial data include user profiles (i.e., personal
notes, emotional status), a list of website information
for support materials, and a list of book
recommendations. All information in the database
server will be kept confidential and revealed only to
authorized users. The application server will grant
permission to access data in accordance to each
user’s role. Data will be de-identified as necessary
for confidentiality and security.
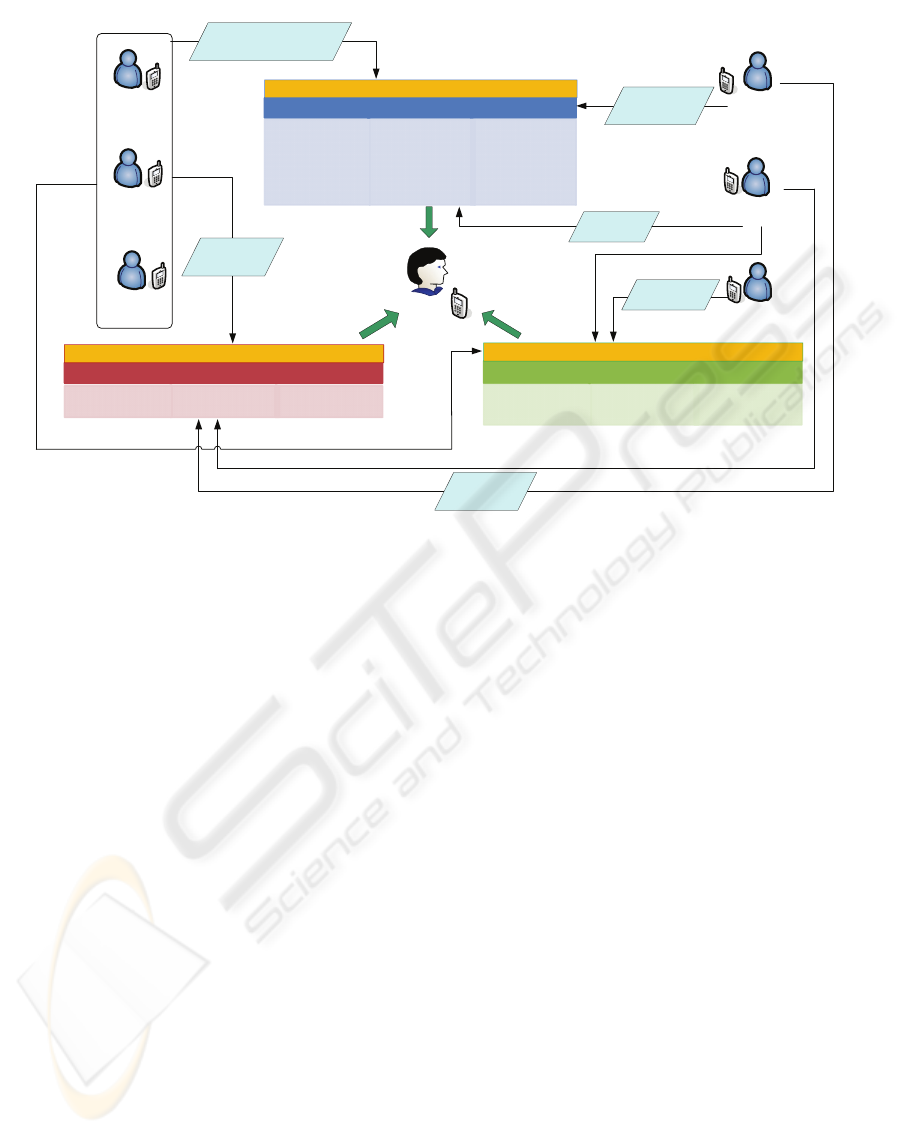
3.2 Functions
As shown in Figure 4, social support network
members provide a different type of support than
those clinical members who rely mostly on their
specialized skills. Three support actions composed
of social, clinical, and emergency actions are
considered so survivor’s of suicide can receive
support from each of these categories of people, in
order to assist them in coping with their loss. Each
action is a form of tangible support, confidant
support, and validation support. For example, the
validation support that both personal members and
clinical members can provide is companionship,
social interaction, and positive information. These
forms of support can occur as a SMS, MMS or voice
messages.
It is true that COMPANION cannot offer all
supporting functions for suicide survivors however,
COMPANION can provide a means for human
communication with respect to location, context, and
time, which can then lead to more face-to-face
tangible support.
To enhance the health-related QOL,
COMPANION will feature a reminder system and
six unique functions to facilitate communication or
interactions between suicide survivors and their
caregivers, family and friends. These functions
mainly utilize spatial data, temporal data, and
preference information for each user.
Find People- A group member can use this function
to search for a location and personal information
(i.e., availability) for finding people with some
criteria. Example queries are: Where is Lyn? Who is
within 1 mile of me and able to meet? Is anyone
with Sue? The query results could be presented as a
point on a map with a description.
Find Place- A member in the group can use this
function to search for a place that meets a specific
set of desired criteria. For example, are there support
group meetings near? What are the top three
restaurants visited by Sue? In addition, when two or
more members are involved in the search process
COMPANION can provide an optimal solution to
satisfy the users while maximizing the criteria. For
example, what library is located between Sue and
Lyn’s current locations?
Navigation- This function provides step-by-step
directions, estimated travel time and arrival time
from a requesting user’s current location to a
specific destination (static) or to another user’s
current location (dynamic). The route and instruction
will be calculated according to a method of travel
defined by the user. In this research, transportation is
limited only to ground transportation, i.e., driving,
walking, or taking public transportation.
Geofence- This function triggers an event whenever
someone enters or leaves a pre-defined geographical
region. For example, Sue sets COMPANION to send
a SMS to notify her that Ann is within 0.5 mile of
her location, and Lyn sets COMPANION to notify
her spouse when she leaves the support group
meeting.
Geotag- This function allows members to post
messages at a particular location. For example, Lyn
wants to describe her feelings and express anxiety to
her sister when shopping. She can accomplish this
by entering a score into the phone representing her
emotional state. The posted geotag could be set as a
personal or sharable piece of information.
Information Service- This function provides
information resources including websites, books and
services related to coping with suicide. It also
provides information about specific interests for
each user.
4 CONCLUSIONS
Through the development, testing and application of
the COMPANION system, the model for a SOS’s
social support network will be modified if necessary,
retested until correct, and then validated. By
knowing the actors and the roles that they play in a
survivor’s social support network, information can
be customized and made readily available to support
COMPANION: SOCIAL SUPPORT NETWORKING TECHNOLOGY FOR SURVIVORS OF SUICIDE
361
Tan gibleSupport
•FinancialAssistance
•HouseholdGoods
•Providestransportation
• Assistancewith cooking
andcleaning
ConfidantSupport
•Expressionoffeelings
•Expressionofconcerns
•Expressionofsympathy
•Expressionofcari ng‐
acceptanceand
approval
Validatio nSupport
•Providescompanionship
•Providessocial
interaction
•Providespositive affect
andreinforcement
•AllowsforTime/
Recuperation
SocialActions
TangibleSupport
•Providesforphysical
assessmentandcare
ConfidantSupport
•Providesmentalstatus
assessment‐ care
Validatio nSupport
•Providessocial
comparison‐ feedback
ClinicalActions
TangibleSupport
•EmergencyMedical
Service‐ Police
ConfidantSupport
•EmergencyPh one
Hotline–Contact1800‐
Support
Validatio nSupport
•EmergencyDrop‐In
Center‐ Shelter
EmergencyActions
Family
Friends
Neighbors
Suicide
Survivors
Counselor
Professional
Emergency
Professional
Healthcare
Professional
Social
Members
Professional
Members
Whowithin
thefence?
Whereisthe
survivorsor
friends?
Whereare
thesensitive
locations?
Howtogetto
themeeting
location?
Howtoget
tosurvivors?
Whatarethe
importantnotesof
thespecificlocations?
Figure 4: Social Support Network of COMPANION.
individuals in times of crisis. Through the
discoveries made with COMPANION and it’s
utilization within a survivor’s social support network
there is potential to positively affect the bereavement
processes and impact the health-related QOL of
many individuals currently not treated.
REFERENCES
Boyd, D. M. & Ellison, N. B. (2007) Social Network
Sites: Definition, History, and Scholarship. Journal of
Computer-Mediated Communication, 13, 210-230.
Cohen, S. (1991) Social supports and physical health:
Symptoms, health behaviors and infectious disease. IN
CUMMINGS, E. M., GREENE, A. L. &
KARRAKER, K. H. (Eds.) Lifespan Developmental
Psychology: Perspectives on Stress and Coping.
Hillsdale, NJ, Erlbaum.
Hossain, K., Chung, K. & Murshed, S. (2007) Exploring
Temporal Communication Through Social Networks.
INTERACT 2007. Rio De Janeiro, Brasil, IFIP.
Mcintosh, J. L. (2008) U.S.A. Suicide: 2005 Official Final
Data. Washington, DC, American Association of
Suicidology.
Mitchell, A. M., Kim, Y., Prigerson, H. & Mortimer-
Stephens, M. (2004) Complicated grief in survivors of
suicide. CRISIS, 25, 12-18.
HEALTHINF 2009 - International Conference on Health Informatics
362
