
Aingeru: an Innovating System for Tele
Assistance of Elderly People
Alberto Tablado, Arantza Illarramendi, Miren I. Bag¨u´es
?
, Jes´us Berm´udez,
and Alfredo Go˜ni
??
University of the Basque Country, Donostia, Spain
Abstract. In this article we present the main features of Aingeru, a
system that provides a new kind of tele assistance service. The purpose
of developing Aingeru has been to overcome the main constraints that
tele assistance services nowadays present: they are passive (they react
only when the user requires it); their coverage is limited; and, they do
not monitor automatically vital signs.
By contrast, Aingeru, by using PDAs (Personal Digital Assistants),
wireless communications and semantic web and agent technologies, pro-
vides a service with the following features: it is active (it reacts auto-
matically in the face of anomalous situations); it can work anywhere and
anytime; and, it can monitor vital signs and generate an alarm when nec-
essary. Furthermore Aingeru permits physicians and relatives concerned
with Aingeru users to consult data about them through the web.
The main focus of the paper is on presenting the architecture of Aingeru
and three asp ects that are used in its development: agent technology,
semantic web techniques and web services which constitute the pillars to
obtain the new tele assistance features provided by Aingeru.
1 Introduction
It is a reality that the numb er of elderly people is growing and so, the number
of these people that live alone. Although many of them can manage themselves,
it is also true that they feel a kind of defenceless situation and many of them
sign a contract with companies that offer a tele assistance service.
These tele assistance services, although they accomplish an interesting and
necessary function, present the following main constraints: they are passive, their
coverage is limited and they do not monitor vital signs.
Having as a goal to overcome the previous constraints, we are developing
the system Aingeru
1
, that is our proposal for a new way of tele assistance
?
This work is supported by a grant of the Basque Government.
??
All authors are members of the Interoperable DataBases Group, online at
http://siul02.si.ehu.es. This group is part of the Department of Computer Lan-
guages and Systems, at the University of the Basque Country in Spain. This work
is mainly supported by the University of the Basque Country and Diputaci´on Foral
de Gipuzkoa (cosupported by the European Social Fund).
1
Aingeru is the word in the Basque language for expressing the notion of guardian
angel.
Tablado A., Illarramendi A., I. Bagüés M., Bermúdez J. and Goñi A. (2004).
Aingeru: an Innovating System for Tele Assistance of Elderly People.
In Proceedings of the 1st International Workshop on Tele-Care and Collaborative Virtual Communities in Elderly Care, pages 27-36
DOI: 10.5220/0002681100270036
Copyright
c
SciTePress

for elderly people. Hence, apart from supporting the functionalities provided
by current tele assistance services, Aingeru also offers: an active assistance by
using stationary agents that behave in the face of anomalous situations without
a direct intervention of the user; an anywhere and anytime assistance by using
wireless communications and PDAs; and the monitoring of vital signs by using
sensors that capture the values of those signs and feed a decision supp ort system
that analyzes them and generates an alarm when necessary.
Concerning related works, we classify tele assistance systems in two groups.
In the first group, we include those systems that provide limited coverage, such
as existing tele alarms. The main features of those systems are the following: they
use wired phone communications to contact tele assistance services providers,
their coverage is restricted usually to the user’s home and their activation is
triggered by the user, generally using a button. Therefore, they do not support
an active anywhere and anytime assistance. In the second group we include more
advanced systems. Some of them focus their efforts on offering an active assis-
tance (e.g. TeleCare [1]) while others use PDAs and take advantage of wireless
communications to provide anywhere and anytime assistance (e.g. doc@HOME
[2] and TeleMediCare [3]). In the majority of the last kind of systems, PDAs are
used only as intermediary elements and their goal is merely reduced to transmit
data from sensors to a central computer where data analysis is made. They do
not take advantage of the ability of the PDAs to carry out a certain pre-analysis
before sending data to the central computer. Notice that wireless communica-
tions are slow, expensive and unstable so, analysis made in the PDA can save
communication costs and can permit to detect anomalies earlier. Other related
works use different “devices” to provide anywhere and anytime assistance (e.g.
Sensatex [4] and SILC [5]).
Aingeru goes one step further by providing not only anywhere and anytime
assistance using wireless communications and PDAs, but also a high quality
assistance. The combined use of three technologies: agents, semantic web and
web services constitutes the core that differentiates Aingeru from other related
works.
In the rest of this paper we first present a brief introduction to the global
architecture of Aingeru. Then, we explain the main features of: the agents that
take part in Aingeru, the semantic web tools developed, and the web services.
Next, we show some performance features and we finish with the conclusions.
2 Overview of the Global Architecture of Aingeru
The goal of this section is to present briefly the main features of the Aingeru
architecture. As can be observed in Fig. 1, there are five different types of com-
ponents:
–
User PDA. Each person monitored by Aingeru carries a PDA. Its main
goal is twofold, first to monitor the user and then, when special circum-
stances require, to be the link between the person and the center (Control
28
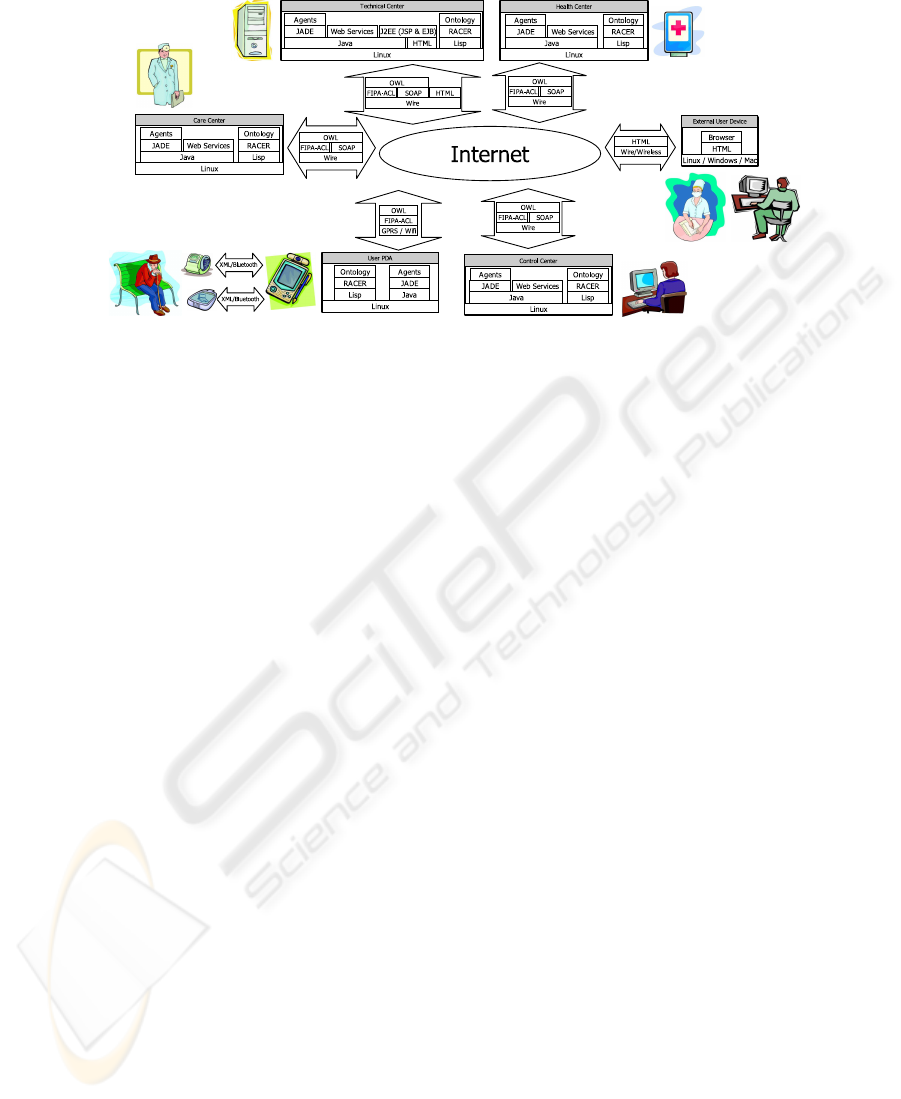
Fig. 1. Architecture of .
Center) resp onsible for monitoring her/him. Three are the basic functions
of PDAs: manual activation of an alarm (when the user feels bad, or some-
thing is happening in his environment and he wants to notify it, he presses
the button that appears in the interface and an alarm is activated in the
Control Center), automatic activation of an alarm (the PDA receives data
sent by sensors related to pulse, mobility, etc., and an agent situated at the
PDA analyzes these data in order to activate an alarm when an anomalous
situation is detected) and agenda services (PDAs provide their users with
classical agenda services, such as remembering when they have to visit the
doctor, etc.). In each PDA two ontologies are incorporated: MedOnt and
OperOnt (they are described in Sect. 3) and several agents.
– Control Centers are the centers in charge of monitoring people. Their
main task is to react in the presence of user alarms and to take the ade-
quate actions. In a computer of each Control Center are incorporated: the
OperOnt ontology, several agents, web services and a database that contains
data about monitored users. The OperOnt ontology permits the agents to
communicate at a semantic level.
–
Care Centers are the public health centers for primary assistance. Part
of the application must run in Care Centers in order to provide
users with new functionalities such as: accessibility of physicians
to data stored in the user PDA, direct insertion of medical appointments
in the PDA, etc. In a computer of each Care Center are incorporated: the
OperOnt ontology, several agents, web services and a database that contains
clinical data.
–
Health Centers correspond to hospitals. In order to interoperate with
system, in a computer of each Health Center are incorporated:
the OperOnt ontology and some deployed web services.
–
Technical Center. The goal of this center is the development and support
of the application. For example, there is an agent in this center,
29

in charge of sending new software releases and activating them, in the cor-
responding component of the global architecture.
Concerning communication aspects among the components, in
Fig. 1 we can observe the different levels that are used. At the physical level,
the wired or wireless communication appears. At the transp ort level, FIPA is
used for inter agent communications and SOAP for web services. At the appli-
cation level, agents and web services communicate through terms described in
ontologies written in OWL
2
.
3 Distinctive technologies of Aingeru
3.1 Agents in Aingeru
As we have mentioned in the introduction, one pillar of is the use of
agents. There are software agents working in the various elements that take part
of its architecture (i.e., in the PDA, Control Centers, etc.). Moreover, all kinds
of agents that take part in the system are described in the OperOnt
ontology (explained in Sect. 3.2), with the goal of making them interoperable
with external applications.
For the implementation of those agents, we have selected the JADE Agent
System platform [8, 9] for the following reasons among others: standards com-
pliant, it adheres to the latest FIPA standards; lightweight, as some parts of
must run in PDAs (JADE has versions that can run on J2ME/MIDP
compliant devices, like phones and watches); flexibility, it allows us to use dif-
ferent transport drivers to convey messages among agencies; Moreover, we make
use of the authentication mechanism supported by JADE and the SSL proto-
col to transmit sensitive data among agents. If additional security is required,
message content is also encrypted.
There are other systems that also promote applying agents in Health Care
[1, 10, 11, 12, 13]. However, as far as we know, they do not put special emphasis
on combining the agent technology with the use of PDAs.
3.2 Semantic Web Techniques
Two formal logic-based ontologies that are machine understable have been de-
fined for the system: MedOnt and OperOnt (see [14] for more details).
Medical Ontology (MedOnt).
To offer a high quality assistance is one of the
aims of the system. This means that not only will generate an
alarm when the user requires it, but also when the system autonomously detects
anomalous situations. Thus, its behaviour is reactive when the user’s health is
in danger. In our opinion, the latter feature is a step forward in the field of tele
2
OWL [6, 7] is an ontology representation language from the Semantic Web forum.
30
assistance applications. In order to accomplish the goal of detecting anomalous
situations, two components are necessary: first, sensors that capture users’ vital
signs values such as temperature, pulse, etc. and then, a decision support system
that analyses the captured values. Knowledge for the decision support system
is represented by a formal domain ontology called MedOnt. Ontology terms
describe states of illnesses that elderly people can suffer from as well as states
generated by the values captured by the sensors.
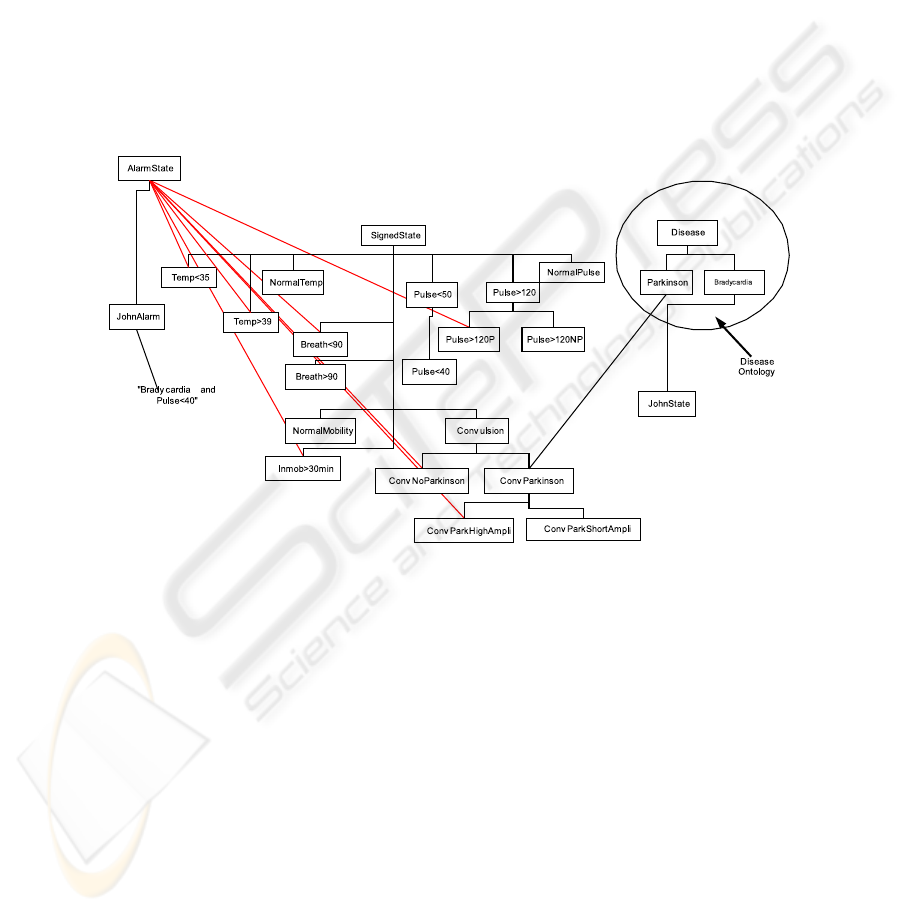
So far, to build the prototype, we deal with a “toy” MedOnt on-
tology that we have built with the collaboration of physicians (see Fig. 2). For
example, in this ontology we can observe the Pulse>120 term. This term de-
scribes that the pulse of the user is above 120 beats per minute.
Fig. 2. Graphic representation of a fragment of a personalized MedOnt.
The JohnAlarm term illustrates the desirable customization of the MedOnt
ontology loaded into each user’s PDA. The JohnAlarm term is a kind of
AlarmState that subsumes the potential anomalous situations of the user John.
We consider customization a very interesting feature because every single person
has peculiarities added to general symptoms.
There are also some terms in the MedOnt ontology that describe situations
combining signs detected by sensors with states of diseases. For example, the
term Convulsion describes the situation when the Mobility Sensor reports shak-
ing over a certain threshold and ConvParkinson describes the state of the kind
of Convulsion of a person who suffers from Parkinson disease.
31

Operational Ontology (OperOnt). Another goal that we planned to reach
when developing the system was to have a semantic representation
of the agent communications framework. Such a formal representation facili-
tates: (i) the interoperability of with other related systems, (ii) the
understanding of features by external actors, and (iii) the
evolution.
So far, the OperOnt ontology
3
is basically divided into three interrelated
areas of descriptions: (i) actors, which interact using various kinds of messages,
(ii) messages with different purposes and dealing with different kinds of contents
and (iii) subjects representing the kinds of message contents. Next we outline
each area, but we want to stress that there are axioms in the OperOnt ontology
that describe their interrelationships.
– Actors. We divide this area into human agents, software agents and
web services. Human agents are classified into two groups: on one hand
users and, on the other hand all those people who are concerned
with the user assistance, from sanitary people to relatives. Software agents
are described taking into account their location and their goals (for instance,
whether they work in a PDA or in a computer, if they are attending a sensor
or interacting with an ontology, and so on). Web services are described on
the basis of their functionality.
–
Messages. Considering the standards-compliant principle in , we
have included descriptions of messages according to their functionality in
FIPA [15] protocols. Message descriptions are based on three FIPA proto-
cols: FIPA Request Interaction Protocol, FIPA Subscribe Interaction Pro-
tocol and FIPA Query Interaction Protocol. Kinds of messages that appear
in OperOnt are: Agree, Cancel, Failure, Refuse, Query, Subscribe and
Inform.
–
Subject of Messages. This area describes terms about the subject or the topic
concerning the message. For example, InputOutput, Location, Urgency,
Emergency, Sensor, Hospital, Appointments, Medicines and Dump de-
scribe different subjects of messages.
Both ontologies — MedOnt and OperOnt — are specified in OWL to take
advantage of semantic web technology and its richer primitives for class and
property descriptions. Furthermore, OWL supports datatype descriptions using
XML Schema [16], so we are able to deal with properties with integer values or
with structured values such as HL7
4
[17] rows.
Moreover, for the reasoning process we selected the RACER [18] system,
which covers all the OWL constructors we need; in particular, it deals with
reasoning about individuals of classes, which is crucial in our framework.
3
See http://siul02.si.ehu.es/Aingeru/OperOnt.owl for an OWL specification of
the OperOnt ontology.
4
HL7 is the first health care data interchange standard.
32

3.3 Web Services
One interesting feature that can be incorporated to the tele assistance services
is the possibility of allowing external persons (relatives, physicians) to consult
data about monitored persons (only authorized users will be allowed to consult)
through Internet. The goal of this feature is accomplished in by web
services that have been developed using JAX-RPC and specified by WSDL. As
examples of those web services we can mention:
– Vital Signs: A web service exported by the Care Center. It provides infor-
mation about user vital signs in real-time. Authorized actors (physicians,
for example) can obtain data about the current values of the sensors that
monitor the user.
– Location: A web service exported by the Technical Center. It provides in-
formation about the current location of the user. Location information is
managed by the Location Agent residing in the User Agency.
Moreover, the architecture of allows the incorporation of public
web services such as those that provide information about sports, weather fore-
casts, etc. Web Services are described in the OperOnt ontology in order to be
discovered and accessed by different actors.
4 Feasibility Features of Aingeru at Work
As is being implemented, we cannot test it yet in a real environment.
For this reason, in this section we show some tests that we did in order to check
its feasibility in particular: (i) influence of the bandwidth in the time needed to
respond to alarms and (ii) capacity of the PDAs to support all the requirements
defined in . Moreover, we compared, in one concrete scenario, local
data analysis versus remote data analysis.
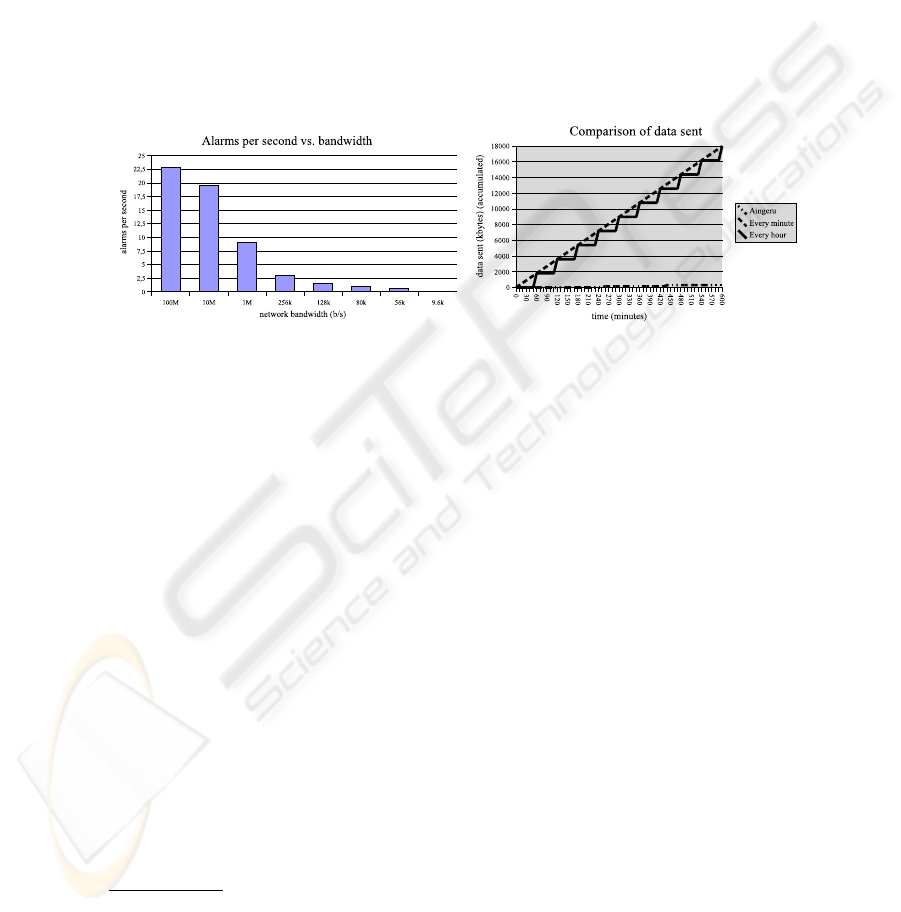
Influence of the Bandwidth in the Time Needed to Respond the
Alarms.
In this test, we show how network communications severely reduce
the number of alarms that can be managed simultaneously (see Fig. 3.a). On
one hand, nowadays GPRS wireless communications provide around 80 kb/s
bandwidth, so each PDA can send only one alarm per second
5
. On the other
hand, a Control Center connected to internet using a 10 Mb/s link can handle
20 alarms per second. Therefore, the Control Center will b e able to cop e with
20 users simultaneously, a number greater than that supported by current tele
assistance services.
5
This frequency of alarms widely exceeds the actual behavior of the users of tele
assistance services as experts told us.
33
Capacity of the PDAs. In the PDA we need to run in a Java virtual machine,
Linux, RACER reasoner and JADE agent platform. Except for RACER (there
is not a version for PDAs yet
6
), all the others run in our test. More than this,
we also tested JADE, and we verified that it could manage up to 60 agents in
the PDA. Taking into account that so far we have developed only eleven agents
for the PDA, we concluded that will be able to operate in the PDA.
As RACER cannot be tested on a PDA, we run it in a normal computer and
we registered how much memory it consumed. In our tests, RACER never went
beyond 10 MB of RAM and, even when all other software was running in the
PDA, about 40 MB of RAM remained free. This means that RACER could be
run in the PDA.
(a) (b)
Fig. 3. Data sent by different models and .
Local Analysis versus Remote Analysis.
Finally, we compared our ap-
proach of making local data analysis at the PDA with the other approaches that
advocate external data analysis. The comparison is based on communication
costs (how many bytes must be sent) in the following scenario: a user has to be
monitored via a 2-lead ECG sensor. It sends 250 samples of a byte every second.
In short, this configuration sends 30 KB per minute. And, to perform this task,
we defined three configurations. The first one was , equipped with a
wireless ECG sensor and a wireless thermometer. The second and third ones had
the same sensors, but did not perform local analysis of the data received. These
two differ in that they sent data at different intervals: one (A) every minute and
the other (B) every hour.
Figure 3.b shows the data sent as time goes on. We simulated an alarm
at 260 minutes (four hours and twenty minutes) and 440 minutes (after seven
hours). The first and most relevant fact is that the line that lies over X axis,
which represents , sends hardly any data, even though is
configured to send five minutes of ECG data within the alarm notification.
6
We are working in collaboration with the authors of RACER to port it to the PDAs.
34

Related to communications costs, needs to send data only twice, in
contrast to other configurations. The A configuration sends 30 KB of data every
minute (600 times) and the B configuration, 1,8 MB every hour (10 times) for
a total of 18 MB. only sends 300 KB in the same interval and offers
better assistance.
Furthermore, we analyzed the latency, that is, how long it takes since the risk
situation arises until the system knows about it. In A or B, the average time is
half of the time between data arrival, i.e., half a minute for A or half an hour for
B. can report the alarm in less than a second (only the time needed
to send the alarm over the network, because software components have response
times much slower). To finish, we want to mention that savings communication
costs implies also savings in battery consumption, which is relevant when working
with PDAs.
5 Conclusions
In this article we have presented the system, which main contribu-
tions can be summarized under two different perspectives: one related to the
application domain; and, the other related to the technical issues.
Concerning the application domain, goes one step further in the
tele assistance service by providing: (i) anywhere and anytime assistance using
PDAs and wireless communications; and, (ii) a high quality assistance reacting
in the face of anomalous situations, mainly due to the use of agents and semantic
web technology.
With respect to technical issues, for the development of we have
built: (i) agents that are specialist in different tasks, that can be executed in
the PDA and in other servers and that can communicate among them at the
semantic level using OperOnt ontology; (ii) two ontologies that allow sharing
knowledge, medical and operational, with other systems; and (iii) web services
that bring closer to physicians and relatives concerned with the users
of .
So far we have got only a limited prototype and as future work we plan to
work in the following directions: (i) defining a mechanism that allows us to do
a semiautomatic customization of the domain ontology MedOnt, (ii) analyzing
the interest of changing the agent platform to another one that supports agent
mobility and (iii) incorporating the WSAI technology to improve the integration
of agents and WebServices.
6 Acknowledgements
The authors would like to thank Volker Haarslev and Ralf M¨oller for their help
in carrying RACER to PDAs.
35

References
[1] (2004, Feb.) Telecare, a multi-agent tele-supervision system for elderly care.
[Online]. Available: http://www.uninova.pt/
∼
telecare
[2] (2004, Feb.) doc@HOME. [Online]. Available: http://www.docobo.com
[3]
(2004, Feb.) TelemediCare. [Online]. Available: http://www.telemedicare.net
[4] (2004, Feb.) Sensatex. [Online]. Available: http://www.sensatex.com
[5] (2004, Feb.) Supporting Independently Living Citizens. [Online]. Available:
http://www.fortec.tuwien.ac.at/silcweb/SILC.htm
[6]
OWL Web Ontology Language Reference, World Wide Web Consortium
W3C Candidate Recommendation, Aug. 2003. [Online]. Available: http:
//www.w3.org/TR/owl-ref
[7] (2004, Feb.) Web-ontology (webont) working group. [Online]. Available:
http://www.w3.org/2001/sw/WebOnt/
[8]
(2004, Feb.) JADE. [Online]. Available: http://jade.cselt.it
[9] F. Bellifemine, A. Poggi, and G. Rimassa, “Developing multi-agent systems with
JADE,” in 7th International Workshop on Agent Theories, Architectures, and
Languages, 2000, pp. 85–99, Boston, MA.
[10] H. Mouratidis, G. Manson, P. Giorgini, and I. Philp, “Modelling an agent-based
integrated health and social care information system for older people,” in 15th
European Conference on Artificial Intelligence, 21 July 2002.
[11] S. L. Mabry, S. J. Kollmansberger, T. Etters, and K. L. Jones, “IM-Agents for
patient monitoring and diagnostics,” in 15th European Conference on Artificial
Intelligence, 22 July 2002.
[12]
A. Moreno and D. Isern, “Offering agent-based medical services within the
AgentCities project,” in 15th European Conference on Artificial Intelligence, 22
July 2002.
[13]
L. M. Camarinha-Matos and H. Afsarmanesh, Advances in Automation, Multi-
media and Video Systems, and Modern Computer Science. WSEAS Press, 2001,
ch. Virtual Communities and Elderly Support, pp. 279–284, ISBN: 960 8052 440.
[14]
M. I. Bag¨u´es, J. Berm ´udez, A. Illarramendi, A. Tablado, and A. Go˜ni, “Us-
ing ontologies in the development of an innovating system for elderly people
tele-assistance,” in Proceedings of the International Conference on Ontologies,
Databases and Applications of SEmantics, ser. Lecture Notes on Computer Sci-
ence, vol. 2888. Springer-Verlag, Nov. 2003, pp. 889–905, Sicily, Italy.
[15]
(2004, Feb.) Foundation for Intelligent Physical Agents. [Online]. Available:
http://www.fipa.org
[16] XML Schema Working Group, XML Schema Part 0: Primer, World Wide Web
Consortium Std., 2 May 2001.
[17] (2004, Feb.) Health Level Seven. [Online]. Available: http://www.hl7.org
[18]
R. M¨oller and V. Haarslev. (2004, Feb.) RACER: Renamed ABox and Concept
Expression Reasoner. [Online]. Available: http://www.fh-wedel.de/
∼
mo/racer/
36
