
Querying Social Practices in Hospital Context
John Bruntse Larsen
1
, Virginia Dignum
2
, Jørgen Villadsen
1
and Frank Dignum
3
1
DTU Compute, Technical University of Denmark, 2800, Kongens Lyngby, Denmark
2
Faculty of Technology, Policy and Management, Delft University of Technology, Delft, The Netherlands
3
Department of Information and Computing Sciences, Utrecht University, Utrecht, The Netherlands
Keywords:
Social Practices, Hospital Staff Planning, Multi-Agent Goals, Decision Support.
Abstract:
Understanding the social contexts in which actions and interactions take place is of utmost importance for
planning one’s goals and activities. People use social practices as means to make sense of their environment,
assessing how that context relates to past, common experiences, culture and capabilities. Social practices can
therefore simplify deliberation and planning in complex contexts. In the context of patient-centered planning,
hospitals seek means to ensure that patients and their families are at the center of decisions and planning of
the healthcare processes. This requires on one hand that patients are aware of the practices being in place at
the hospital and on the other hand that hospitals have the means to evaluate and adapt current practices to the
needs of the patients. In this paper we apply a framework for formalizing social practices of an organization
to an emergency department that carries out patient-centered planning. We indicate how such a formalization
can be used to answer operational queries about the expected outcome of operational actions.
1 INTRODUCTION
The importance of developing shared meaning and
understandings is one of the main aspects of main-
taining an organization. Hospital organizations are
no different and tend to develop their own ways of
doing things which need to be shared with novices.
Moreover, as vision and strategy change, new prac-
tices need to be implemented to ensure that medical
staff and users are able to function properly in the new
model of operation.
In recent years, ensuring patient satisfaction in
hospitals is becoming increasingly important, requir-
ing hospitals to develop means to continuously as-
sess and adapt their processes and practices. Patient-
centered planning is a way of thinking and doing
things that sees the patients in health and social ser-
vices as equal partners in planning, developing and
monitoring care to make sure the treatment meets
their needs. The patients and their families are put
at the center of decisions and seen as experts in their
own condition, working alongside professionals to
get the best outcome. Traditional planning technolo-
gies are typically designed to produce complete plans
that handle all situations given a well defined set
of goals. This approach is not suitable for patient-
centered planning, which involve human agents, as it
leads to a combinatorial explosion if the actions of the
human agents are not predictable or limited. Social
practices provide a mean to deal with the complexity
by considering the social and physical constructs that
shape and constrain the interaction.
A hospital can be seen as the embodiment of on-
going social practices of many different forms (in-
cluding, for example, nursing, diagnosing, operating,
office working, drug dispensing). It is also materi-
ally bound up in those practices (and their success-
ful performance), and in how these are changing over
time. For example, as patient-centered planning (in-
cluding how it is organized, managed and monitored)
becomes the practice in hospital management, exist-
ing processes and roles may become less functional
and need to adapt in order to stay fit for that pur-
pose [Walker et al., 2014].
This work contributes with frameworks to help
with understanding of how patient-centered planning
relates to the changing practices of hospital work and
understandings of what constitutes a well-working
hospital. In particular we consider the emergency de-
partment and how the social practices that govern it
have consequences across the hospital. In the present
paper we propose our approach for applying a frame-
work for formalizing social practices of the emer-
gency department and how such a formalization can
Larsen, J., Dignum, V., Villadsen, J. and Dignum, F.
Querying Social Practices in Hospital Context.
DOI: 10.5220/0006580904050412
In Proceedings of the 10th International Conference on Agents and Artificial Intelligence (ICAART 2018) - Volume 2, pages 405-412
ISBN: 978-989-758-275-2
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
405

be used for answering operational queries about the
expected outcome of operational actions. The emer-
gency department is also the focus of [Larsen and Vil-
ladsen, 2017] which proposes an approach for model-
ing it as a multi-agent organization.
2 SOCIAL PRACTICES
Social interactions are the focus of Social Sciences
and have also long been discussed in Multi-Agent
Systems (MAS) where there are many formalizations
and theories that describe specific aspects of inter-
actions [Van Den Broek et al., 2005, Dignum and
Dignum, 2011, K
¨
ohler, 2007].
Social practices are accepted ways of doing
things, contextual and materially mediated, that
are shared between actors and routinized over
time [Reckwitz, 2002]. They can be seen as patterns
that are filled in by a multitude of single and often
unique actions. Through (joint) performance, the pat-
terns provided by the practice are filled out and repro-
duced. Each time a social practice is used, elements
of the practice, including know-how, meanings and
purposes, are reconfigured and adapted [Shove et al.,
2012]. Actors learn from the use of social practices,
and the more one uses a social practice with satis-
factory results, the more that actor will tend to use
that practice. Social practices are shared which means
that individuals playing a role in a social practice will
know what to do and will expect certain behavior and
reactions of the other participants. Success enforces
the social practice.
Related research on work practices and cognitive
architectures are the closest to our proposal. Work
practice research recognizes the inherent difference
between the work flows as described and prescribed
by the organization and employee behavior. The work
practice model Brahms enables to define the behav-
ior of entities by means of activities and workframes,
amongst others [Sierhuis et al., 2009] but lacks learn-
ing capabilities to adjust priorities, and means to dis-
tinguish between context and action preconditions.
Cognitive architectures [Sun, 2009] use drives as ba-
sis to dynamically derive goals during agent interac-
tions. As such, it can capture the motivational com-
plexity of the human mind [Newell, 1994], but it takes
an agent perspective rather than a societal one, such as
the one we propose. Our approach with social prac-
tices also shows some resemblance to agent organiza-
tions (see e.g. [Dignum, 2004]) as they both provide
structure to the interactions between the agents. How-
ever, the structure provided by social practices arises
from the bottom up from components that define ex-
pected behavior in a given context rather than being
an imposed (top-down) organizational structure.
In [Dignum and Dignum, 2015] an initial formal
representation of social practices is presented that
allows for its incorporation in agent deliberation
architectures. It is based on modal logic and extends
work on agent organizations and landmarks. In
particular, it extends work on the Logic for Agent
Organizations (LAO) [Dignum and Dignum, 2011]
which formalizes notions of capability, stit [P
¨
orn,
1974], attempt and responsibility. For the purpose of
this paper, we suffice with the informal definitions of
the symbols in table 1 and the components of a social
practice as follows:
• Context
– Roles describe the competencies and expecta-
tions about a certain type of actors [Sunstein,
1996]. Thus a lecturer is expected to deliver
the presentation.
– Actors are all people and autonomous systems
involved, that have capability to reason and (in-
ter)act. This indicates the other agents that are
expected to fulfill a part in the practice.
– Resources are objects that are used by the ac-
tions in the practice such as — in case of a lec-
ture — seats, projector, screen, etc. So, they
are assumed to be available both for standard
actions and for the planning within the practice.
– Affordances are the properties of a resource, a
place or a context that indicate the action pos-
sibilities that are readily perceivable by an ac-
tor. E.g. any flat surface at approximately knee-
length can afford the action ‘sit’. Affordances
permit social actions and depend on the match
between context conditions and actor character-
istics [Gaver, 1996].
– Places indicate where all objects and actors are
usually located relatively to each other, in space
or time.
• Meaning
– Purpose determines the social interpretation of
actions and of certain physical situations.
– Promotes indicate the values that are promoted
(or demoted, by promoting the opposite) by the
social practice.
– Counts-as are rules of the type “X counts as Y
in C” linking brute facts (X) and institutional
facts (Y) in the context (C) [Searle, 1995]. E.g.,
in a voting place, filling out a ballot counts as a
vote.
ICAART 2018 - 10th International Conference on Agents and Artificial Intelligence
406

• Expectations
– Plan patterns describe usual patterns of ac-
tions [Bresciani et al., 2004] defined by the
landmarks that are expected to occur.
– Norms describe the rules of (expected) behavior
within the practice, using the ADICO grammar
proposed by Ostrom [Crawford and Ostrom,
1995]. ADICO statements are formed using
five components: Attribute (or Acting entity),
Deontic, aIm (or Intention), Condition, and Or
else (or sanction). Norms are statements that
include the acting entity, deontic, intention, and
condition (ADIC) and possibly also a sanction
(ADICO).
– Strategies indicate the possible activities that
are expected within the practice. Not all activ-
ities need to be performed! They are meant as
potential courses of action. Strategies are spec-
ified as AIC statements in ADICO.
– Start condition, or trigger, indicating how the
social practice starts.
– Duration, or End condition, indicating how the
social practice ends.
• Activities
– Possible actions describe the expected actions
by actors in the social practice.
– Requirements indicate the type of capabilities
or competences that actors are expected to have
in order to enact roles and perform activities
within the social practice.
It is also important to note that social practices can
be described at different levels of abstraction. Ab-
stract practices are generic and do not give much de-
tails on the specifics of a context. Concrete social
practices apply to more specific domains, roles or ac-
tors and typically provide more details about the pos-
sible plans. E.g. an abstract social practice ‘greeting’
just indicates when a greeting gesture is expected,
but given a more specific context or actors it also de-
scribes how it should be performed; for example, by
‘bowing’ if context is Japan, or ‘hugging’ if actors are
good friends.
Finally, social practices relate to each other and
to the current situation. Depending on the features
of a situation individuals will choose (a set of) social
practices to explore. Moreover, social practices can
be composed or contain other social practices. E.g. a
handshake can be the start of a meeting. So it forms
part of the meeting social practice. On the other hand
the handshake is one type of greeting. So, handshake
is a specialization of greeting and a part of a meet-
ing. In fact, most classification relations that apply to
processes (specialization, part-of, is-a, ...) can also be
applied to social practices.
3 PATIENT-CENTERED
PLANNING
Advance care planning is a process “whereby a pa-
tient, in consultation with health care providers, fam-
ily members and important others, makes decisions
about his or her future health care, should he or she
become incapable of participating in medical treat-
ment decisions” [Singer et al., 1996]. The process of
advance care planning informs and empowers patients
to have a say about their current and future treatment.
Patient-centered planning is a process in which
the hospital plans are made with needs of the patient
in center. A social practice approach to modeling
patient-centered planning can accommodate societal
requirements of patient-centered planning, including:
• respecting patients values and putting patients at
the center of planning.
• taking into account patients preferences and ex-
pressed needs.
• coordinating and integrating care planning.
• working together to ensure good communication,
information and education.
Social practices have both a social and a func-
tional purpose, which determines how they are used
by the different actors. To regard patient care as a so-
cial practice puts an appropriate emphasis on the rea-
sons why people take part in it and how they choose
to interpret the various expectations. Young doctors
value the hospital regulations and formal workflows
because they assume it serves efficiency and patient
care. Experienced doctors care for patients but often
less for formalisms. Phoning a specialist directly is
seen by senior doctors as a good social practice, be-
cause they know that the reaction of the specialist is
direct and will result in a quick treatment of the pa-
tient. Delays caused for other patients are not consid-
ered, because the overall hospital perspective is less
important for experienced doctors. Identifying and
understanding these differences in perceiving hospi-
tal policy is important for hospital managers and can
be used to redefine processes and policies. In this
project, we will develop simulation models that en-
able hospital managers to analyze the consequences
of different social practices from the perspective of
patients and medical staff.
In the remainder of this section, we first introduce
a simple scenario and then illustrate the use of so-
Querying Social Practices in Hospital Context
407
Table 1: Symbols of the social practice formal representation where O(γ) and F(γ) have standard dynamic deontic logic
semantics.
Symbol Meaning
Activities
Basic actions {α
1
, ..., α
n
} A finite number n of basic actions in the social
practice. Entails notion of a complex action γ.
Actors {a
1
, ..., a
m
} A finite number m of actors in the social practice.
Context {c
1
, ..., c
n
} A finite number n of special context constants. A
subset of these are social practice identifiers SP.
Capabilities Capability(a) A function that returns the set of actions that ac-
tor a is capable of performing.
Cap(a, α) True iff actor a is capable of performing action a
i.e. Cap(a, α) ≡ α ∈ Capability(a).
DO(a, α) Actor a performs action α next. Additionally as-
sumes that DO(a, α) → Cap(a, α)
Beliefs and Assumptions
purpose(a, α, c) = φ ≡
CB
A
c
(Salient(a, α, c) ∧
DO(a, α) → Goal(a, φ) ∧
B
a
([α(a)]φ)
It is common belief among the agents in context
c that if actor a performs action α in context c
then φ is a goal of a and a believes it can achieve
it by performing α.
Meanings
play(a, r) Indicates that actor a enacts role r.
promote(sp, α(a), v) Indicates that in the social practice sp, the action
α(a) performed by actor a promote value v. For
a more formal characterization of the promotes
relation see [Weide, 2011].
Expectations
O(r, φ, γ) O(r, φ, γ) ≡ ∀a : play(a, r) ∧ B
a
(φ) → O(γ(a)).
F(r, φ, γ) O(r, φ, γ) ≡ ∀a : play(a, r) ∧ B
a
(φ) → F(γ(a)).
strategy(φ, DO(B, γ), sp) Indicates that if all actors (involved in the social
practice sp) believe that B believes the condition
φ then they all believe that all actors in B will
perform their part of γ next.
cial practices modeling to represent the situation de-
scribed in the scenario.
3.1 Scenario: Specialist Consults
In this paper, we consider the case of scheduling spe-
cialist consults for emergency ward patients. These
patients arrive at the hospital unscheduled and the at-
tending doctor may decide that a specialist opinion is
needed. However, these specialists follow a regular
consult plan and emergency patients will need to be
placed in between the regular patients. Several strate-
gies can be used for this, depending on the severity
of the case, the knowledge the emergency doctor has
about hospital procedures and informal strategies or
workarounds, and the overall culture of the hospital
location.
In particular, we will consider the following sce-
nario: A man arrives at the emergency ward with
very bad headache. The patient is not critically ill but
the doctor fears that his condition can deteriorate and
needs a second opinion from a specialist. Depending
on the seniority and expertise of the attending doctor,
two different plans will be followed:
• A junior doctor, not aware of the hospital’s infor-
mal processes and networks, will file a request for
a specialist consult through the formal channels
and wait for the specialist to make the time to at-
tend to this patient.
• A senior doctor, knowing how things work, will
directly call a specialist who will directly attend to
this request, delaying her consult with a scheduled
regular patient.
These two different practices lead to different re-
sults. In the first case, the acute patient will need
to wait, which depending on his condition may have
serious health consequences. On the latter case, the
ICAART 2018 - 10th International Conference on Agents and Artificial Intelligence
408

scheduled patients will need to wait longer than their
appointed times, leading to irritation and possibly
complaints to the hospital administration.
As both of the situations above illustrate, the deci-
sions that the emergency ward doctors make depend
a lot on their experience with “how things work” in
the hospital. The junior doctor looks for an avail-
able specialist whereas the experienced doctor finds
a specialist who is scheduled for a checkup that they
agree can wait. The experienced doctor can do this
as they know that there is usually a specialist who has
an appointment with a patient who is otherwise do-
ing fine. The experienced doctor is aware of how the
patient depends on the specialist; the junior doctor is
not. There is no clear cut “best” outcome as there are
both satisfied and dissatisfied patients in both cases
but it is clear that the interaction between the acute
doctors and the specialists influence the outcomes.
Overseeing the entire operation, the hospital man-
agement people are tasked with ensuring that there is
a balance between taking care of the scheduled pa-
tients and the acute patients. They are capable of ex-
ecuting operational actions that have either an imme-
diate effect during operation or long term actions with
effects in future operations.
Depending on the local culture and social expecta-
tions, delays to regular consults may require the hos-
pital to reschedule all patients to another day or offer
some kind of compensation, rather than expect those
regular patients to wait patiently to their consult. De-
pending on the frequency and number of emergency
ward patients, long term adaptation of existing proto-
cols may be required which demands well informed
management, as discussed in the next section.
3.2 Scenario as Social Practice
As described in Section 2, social practices can be de-
scribed at several levels of abstraction, resulting in a
graph structure that represents differentiation in terms
of context specialization, inclusion and salience. In
the case of the Specialist Consults scenario, practices
vary for senior and junior doctors and also for the so-
cietal expectations on how to deal with delays. Figure
1 gives an overview of these relations between social
practices.
We provide a basic formal representation of the
scenario as an abstract social practice as follows.
• Context
– Roles are identified from the actors that are
mentioned in the scenario: the junior doctor,
the senior doctor, the regular patient, and the
acute patient. We consider each actor as a role.
We also consider both the acute patient and the
regular patient as a patient role:
jd, sd, d, rp, ap, p : ap, rp ∈ p ∧ jd, sd ∈ d
– Actors are defined by the play-predicate. We
use it to state that four people have the roles
above:
play( j, jd), play(s, sd), play(r, rp), play(a, ap)
– Resources include the room in which the doc-
tor diagnoses the patient, the scheduling sys-
tem, and other objects that we leave vague on
purpose for this abstract social practice:
o
1
, ..., o
m
– Places are the three main areas of the scenario:
the hospital as a whole, an MRI room (where
the specialists carry out their diagnosis), and
the emergency ward:
hospital, MRI-room, ER
• Meaning
– Purpose is defined by purpose-predicate. We
use it to state that the purpose of the consult
action for acute patient a is to get a diagnosis,
and for a junior doctor j is to learn and gain
experience:
purpose(a, consult, sp) = diagnosis(a)
purpose( j, consult, sp) = learn( j)
– Promoted Values are defined by the promote-
predicate. We use it to state that for the junior
doctor, tending patients promotes learning. We
also state that for the patient, getting a treatment
promotes awareness about their condition and
staying long in the ER demotes timeliness:
promote(sp, tendPatient( j), Learning)
∀p : promote(sp, diagnosis(p), Awareness)
∀p : promote(sp, longStay(p), ¬Timeliness)
• Expectations
– Plan Patterns are the sequences of abstract ac-
tions that models the general procedure as de-
scribed in the scenario. We use α
i
for the ab-
stract actions in the sequences. The sequence
models the two different approaches for the ab-
stract social practice to take place depending on
which of the two doctors take care of the acute
patient, as described in the scenario:
α
1
(arrive); α
2
(checkup); (α
5
(get2Op)+
(α
3
(plan2op); α
4
(wait);α
5
(get2Op)))
Querying Social Practices in Hospital Context
409
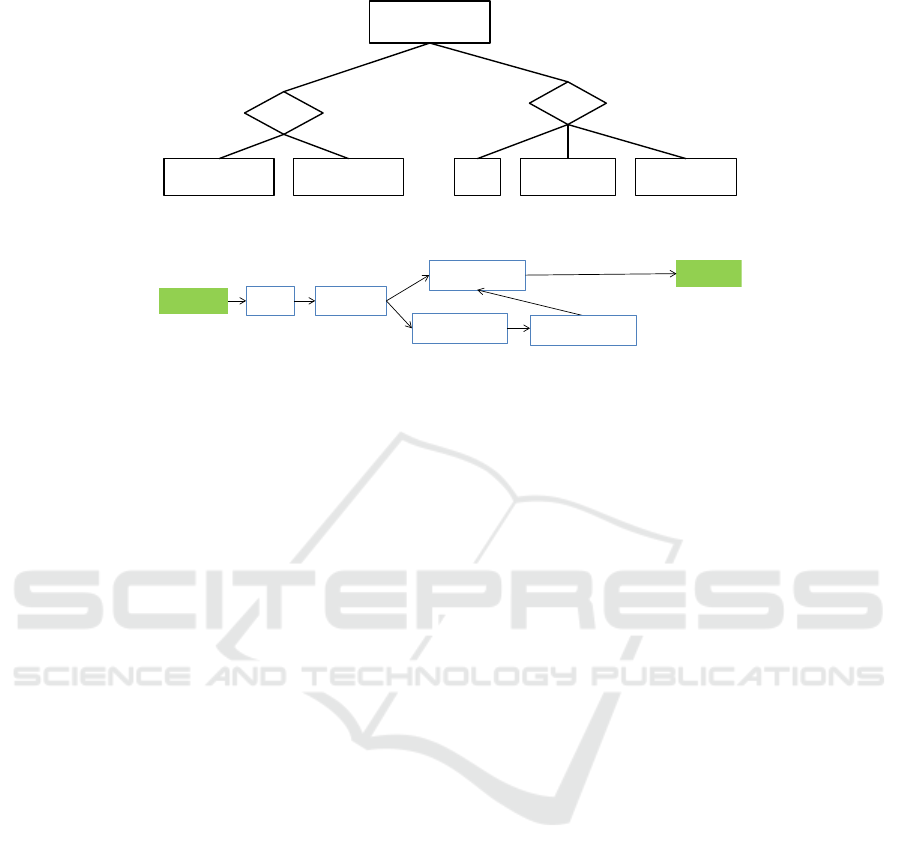
emergency
patient consult
society
doctor
find specialist wait specialist wait reschedule compensate
context context
abstract SP
concrete SP concrete SP concrete SP concrete SP concrete SP
senior
junior
a
b
c
Figure 1: Contextual variations on social practices.
start
end
checkup
get 2
nd
Op
plan 2
nd
Op
arrive
wait @home
Figure 2: Plan pattern.
– Norms are stated as deontic logic predicates.
We state that junior doctors are obliged to treat
acute patients first, and that junior doctors are
forbidden from giving a diagnosis:
O( jd, plays(a, ap), prioritize( jd, a))
F( jd, plays(a, ap), diagnose( jd, a))
– Strategies are defined by the strategy-predicate.
We use strategies to state that the patient waits,
that a senior doctor calls for help from a spe-
cialist by phone, and that a junior doctor waits
for help from a specialist:
strategy(>, DO(p, wait), sp)
strategy(diagnose(d, p),
DO(senior(d), phone), sp)
strategy(diagnose(d, p),
DO( junior(d), wait), sp)
– Start Condition & Duration/End are respec-
tively that the acute patient arrives and that the
acute patient has a treatment plan. As we only
consider this particular abstract social practice
we do not state them explicitly.
• Activities
– Possible Actions includes waiting, calling on
phone, and stating a diagnosis, among others:
wait(), phone(), diagnose(X, p), ...
– Requirements are stated with formulas using
the cap-predicate. We use it to state that the
doctors have medical expertise, and that pa-
tients wait:
∀a
i
, play(a
i
, d) : cap(a
i
, medicalexpertise)
∀a
i
, play(a
i
, p) : cap(a
i
, wait)
In Table 2 we provide a summary of the above. We
provide a more detailed description of the play-, pur-
pose-, promote-, strategy-, and cap-predicates. We
are working on the full specification of the patient-
centered scenario as a validation of this formal repre-
sentation language.
4 OPERATIONAL QUERIES
Operational actions are generally considered risky
in the sense that they can have far reaching effects
and that it can be difficult to estimate the conse-
quences. Immediate actions compromise the sched-
ule greatly and can turn up much more expensive than
first thought. Long term actions that change the pro-
tocols may lead to immediate dissatisfaction among
staff but can be beneficial in the long run. As an ex-
ample in the Specialist Consults scenario, the man-
agement may choose to have the specialists prioritize
acute patients over regular patients so that the junior
doctors will have an easier time finding an available
specialist. Such a change can cause dissatisfaction in
the specialized wards and it is unclear if it would actu-
ally be beneficial in the long run. For that reason they
need insight into the expected outcome of the current
situation, and insight into how an operational action
can change the expected outcome. We consider an
approach for giving such insight by the way of opera-
tional queries that can answer questions such as:
• How many acute patients do we expect in the near
future?
• How long will the average waiting time be for
acute patients?
• What are the expected behavior of the senior doc-
ICAART 2018 - 10th International Conference on Agents and Artificial Intelligence
410
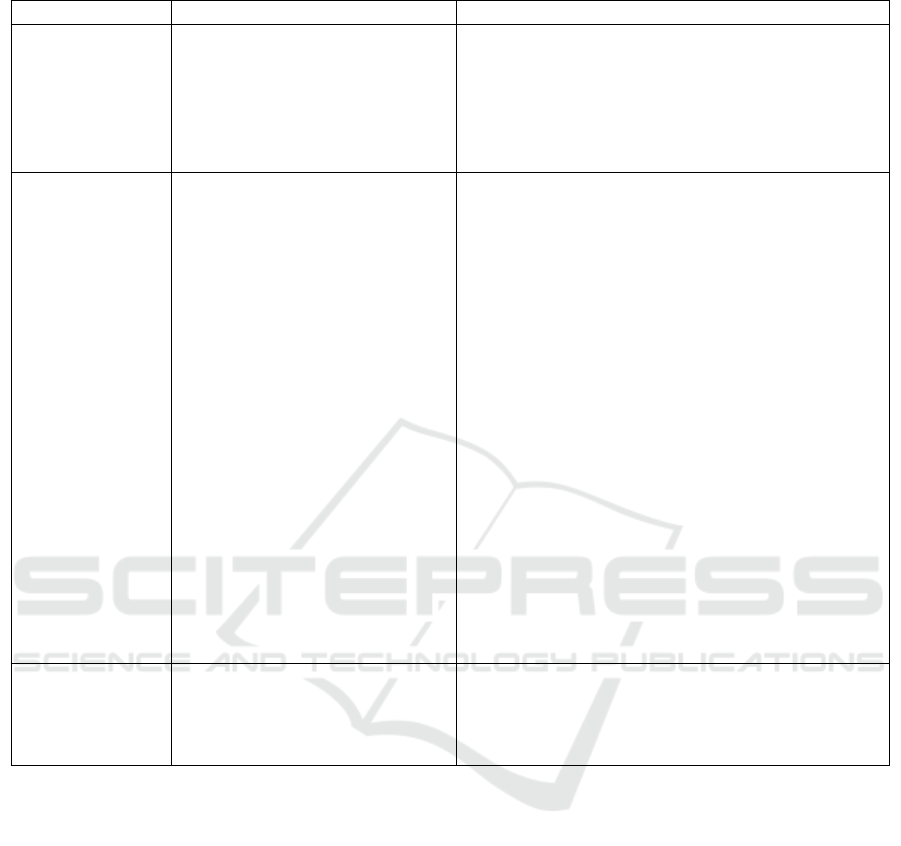
Table 2: A social practice application.
Social Practice A: Hospital SP (informal) B: Hospital SP (formal)
Context
Roles
junior doc, senior doc, regular
patient, acute patient, patient
jd, sd, d, rp, ap, p : ap, rp ∈ p ∧ jd, sd ∈ d
Actors
j, s, r, a
play( j, jd),play(s, sd), play(r, rp),play(a, ap)
Resources
rooms, scheduling system...
o
1
, ..., o
m
Places
hospital, MRI-room, ER... hospital, MRI-room, ER
Meaning
Purpose
diagnosis of patient purpose(a, consult, sp) = diagnosis(a)
teach junior doctor
purpose( j, consult, sp) = learn( j)
Promoted Values
tending patients promotes learn-
ing
promote(sp, tendPatient( j), Learning)
getting a diagnosis promotes
awareness
∀p : promote(sp, diagnosis(p), Awareness)
a long stay demotes timeliness ∀p : promote(sp, longStay(p), ¬Timeliness)
Expectations
Plan Patterns
the plan pattern graph in figure 2.
α
1
(arrive); α
2
(checkup); (α
5
(get2Op)+
(α
3
(plan2op); α
4
(wait);α
5
(get2Op)))
Norms
acute patients must be prioritized O( jd, plays(a, ap), prioritize( jd, a))
junior doctors cannot give diag-
nosis
F( jd, plays(a, ap), diagnose( jd, a))
Strategies
patients wait strategy(>, DO(p, wait), sp)
senior doctors find available spe-
cialist
strategy(diagnose(d, p), DO(senior(d), phone), sp)
junior doctors wait for available
specialist
strategy(diagnose(d, p), DO( junior(d), wait), sp)
Start Condition
acute patient arrives
Duration/End
patient has plan
Activities
Possible Actions
wait, phone, diagnosis, ...
wait(), phone(), diagnose(X, p), ...
Requirements
doctor: medical expertise
∀a
i
, play(a
i
, d) : cap(a
i
, medicalexpertise)
patient: wait ∀a
i
, play(a
i
, p): cap(a
i
, wait)
tors?
• What are the expected behavior of the junior doc-
tors?
These queries are hard to answer analytically, but by
simulating the situation with artificial agents that act
according to our formalization of the social practices,
we can provide sufficiently accurate answers about
the expected outcome. For the simulation we con-
sider having the agents include their knowledge about
social practices when they decide on an action. The
operational query is then answered by simulating the
actions of the agents within the immediate future, re-
turning a list of pairs of outcomes together with their
expectancy. In this way, operational queries and sim-
ulation can provide insight into how decisions and
changes to hospital work practices influence expected
developments and potential bottlenecks.
5 CONCLUSION AND FUTURE
WORK
The social practice approach shows promise as a way
to augment agents with social reasoning. The hos-
pital context provides a good scenario for validating
this approach. The social practice approach supports
decision making. In the scenario we considered, the
operational queries can trigger long term operational
actions that change the protocols. If social context is
known then protocols can be designed to be in line
with social expectations.
In the future we would like to investigate to which
extent operational queries can trigger short term op-
erational actions with an immediate effect. Our next
step towards an evaluation is to implement the for-
mal representation in an agent simulation framework
Querying Social Practices in Hospital Context
411

that shows how changes to the social practice model
influence agent decisions. Furthermore, we intend to
investigate the work in the recent PhD thesis by Chris-
tian Michel Sørup on a generic performance mea-
surement model for an emergency department [Sørup,
2015]. We consider that work highly relevant as it
investigates performance measurement and decision
support in the emergency department scenario and
was done in close collaboration with the emergency
department at one of the hospitals in the Danish cap-
ital region. We hope that our approach using social
practices can add to that work.
ACKNOWLEDGEMENTS
This work is part of the Industrial PhD project Hos-
pital Staff Planning with Multi-Agent Goals between
PDC A/S and Technical University of Denmark. We
are grateful to Innovation Fund Denmark for funding
and the governmental institute Region H, which man-
ages the hospitals in the Danish capital region, for be-
ing a collaborator on the project. We would like to
thank PDC A/S for providing feedback on the ideas
described in this paper. We would also like to thank
Anders Schlichtkrull for comments on a draft.
REFERENCES
Bresciani, P., Perini, A., Giorgini, P., Giunchiglia, F., and
Mylopoulos, J. (2004). Tropos: An agent-oriented
software development methodology. Autonomous
Agents and Multi-Agent Systems, 8(3):203–236.
Crawford, S. E. S. and Ostrom, E. (1995). A grammar
of institutions. American Political Science Review,
89(03):582–600.
Dignum, V. (2004). A Model for Organizational Interac-
tion: based on Agents, founded in Logic. SIKS Dis-
sertation Series 2004-1. Utrecht University. PhD The-
sis.
Dignum, V. and Dignum, F. (2011). A logic of agent orga-
nizations. Logic Journal of IGPL.
Dignum, V. and Dignum, F. (2015). Contextualized plan-
ning using social practices. In Ghose, A., Oren, N.,
Telang, P., and Thangarajah, J., editors, Coordination,
Organizations, Institutions, and Norms in Agent Sys-
tems X, pages 36–52. Springer.
Gaver, W. W. (1996). Situating action II: Affordances for
interaction: The social is material for design. Ecolog-
ical Psychology, 8(2):111–129.
K
¨
ohler, M. (2007). A formal model of multi-agent organi-
sations. Fundamenta Informaticae, 79(3-4):415–430.
Larsen, J. B. and Villadsen, J. (2017). An approach for
hospital planning with multi-agent organizations. In
Polkowski, L., Yao, Y., Artiemjew, P., Ciucci, D., Liu,
D., Slezak, D., and Zielosko, B., editors, Rough Sets -
International Joint Conference, IJCRS 2017, Olsztyn,
Poland, July 3-7, 2017, Proceedings, Part II, volume
10314 of Lecture Notes in Computer Science, pages
454–465. Springer.
Newell, A. (1994). Unified theories of cognition. Harvard
University Press.
P
¨
orn, I. (1974). Some Basic Concepts of Action, pages 93–
101. Springer Netherlands, Dordrecht.
Reckwitz, A. (2002). Toward a theory of social practices.
European Journal of Social Theory, 5(2):243–263.
Searle, J. R. (1995). The construction of social reality. Si-
mon and Schuster.
Shove, E., Pantzar, M., and Watson, M. (2012). The Dy-
namics of Social Practice. Sage.
Sierhuis, M., Clancey, W. J., and van Hoof, R. J. J. (2009).
Brahms: An agent-oriented language for work prac-
tice simulation and multi-agent systems development.
In El Fallah Seghrouchni, A., Dix, J., Dastani, M.,
and Bordini, R. H., editors, Multi-Agent Program-
ming: Languages, Tools and Applications, pages 73–
117. Springer.
Singer, P. A., Robertson, G., and Roy, D. J. (1996).
Bioethics for clinicians: 6. advance care plan-
ning. CMAJ: Canadian Medical Association Journal,
155(12):1689.
Sørup, C. M. (2015). Development of a Generic Perfor-
mance Measurement Model in an Emergency Depart-
ment. PhD thesis, Department of Management Engi-
neering, Technical University of Denmark.
Sun, R. (2009). Motivational representations within a com-
putational cognitive architecture. Cognitive Computa-
tion, 1(1):91–103.
Sunstein, C. R. (1996). Social norms and social roles.
Columbia Law Review, 96(4):903–968.
Van Den Broek, E. L., Jonker, C. M., Sharpanskykh, A.,
Treur, J., et al. (2005). Formal modeling and analysis
of organizations. In International Conference on Au-
tonomous Agents and Multiagent Systems, pages 18–
34. Springer.
Walker, G., Shove, E., and Brown, S. (2014). How does
air conditioning become ‘needed’? A case study of
routes, rationales and dynamics. Energy Research &
Social Science, 4:1–9.
ICAART 2018 - 10th International Conference on Agents and Artificial Intelligence
412
