
Modular Health Kiosk based on Web Technologies
João Silva, Pedro Brandão and Rui Prior
Instituto de Telecomunicações, Faculdade de Ciências da Universidade do Porto, Portugal
Keywords:
Health Kiosk, Personal Health Devices, Data Collection, Autonomous Measurements, Health Monitoring.
Abstract:
We describe a modular and easily reconfigurable Health Kiosk based on common, off-the-shelf Personal
Health Devices and a computer with a touchscreen interface. The Kiosk is implemented in standard web tech-
nologies (JavaScript, HTML and CSS) on top of the Electron platform. It is intended to be used autonomously
by the patients. It is highly modular, can easily be adapted and reconfigured by health professionals with little
to no computer expertise, using a graphical interface, to adapt to different groups of patients and use cases.
We document our findings, identifying problems faced throughout the development and solutions to those
problems.
1 INTRODUCTION
With the increase of the population at a worldwide
level, the expenses associated with health care are
proportionally increasing. Despite that fact there are
still some gaps that need to be fulfilled since the re-
sources are mainly allocated in central areas that most
of the time are not easily accessible to all the pop-
ulation. Moreover, due to that centralization of re-
sources, the ratio of patients for each health profes-
sional is expected to increase, making it more diffi-
cult for them to proper assess all patients that use a
medical facility.
There is a clear demand for alternatives to visit-
ing a medical facility, due to the expenses associated
with it, not only financial but also in terms of time.
Due to the high demand and a low offer in terms of
medical professionals available, there is a chance that
when visiting a medical facility a patient may not be
evaluated by a professional. This situation can lead to
a delay in finding abnormal biometric values, causing
a later treatment start.
Health has always been a field with a high-level of
acceptance of innovation, and using technology with
the intent of improving patients health is something
that has been evolving over the time. This evolution
allowed for the development of medical devices ac-
cessible not only to hospitals but also for personal use
at home. (Suggs, 2006) There was an evolution from
different types of devices that facilitated the access to
health information. The phone acted as a way to solve
simple questions for the patients, which, when the In-
ternet access was globalized, was made easier through
forums or e-mails.
A shortage of these types of devices or technolo-
gies in rural areas is visible and due to that fact, it
should be a main goal of our society to try to reduce
the discrepancy between these areas and others more
developed. In rural areas where the offer in terms of
medical services is low, the impact of a system that
can make evaluation of the patients without taking
time from the medical professionals can be extremely
relevant. (Das and Padhy, 2014)
Creating a system such as the health kiosk would
allow the patients, without the requirement of allo-
cating human resources in these areas, hospitals or
other possible locations, to obtain information on
their health, ultimately saving time and resources to
the user, and in the case of the hospital both to the pa-
tient and to the health professional that has access to
the information without having to collect it.
Possible applications of this system are hospitals
or health centers, but it is not limited to those as the
system is being developed in order to adapt to the
needs of the situation. This is accomplished by having
a configuration that allows for modifications. With the
right configuration it can be deployed in rural areas,
based on the needs of those areas, or elderly commu-
nities in which its inhabitants require constant medi-
cal attention.
In this work, the possibilities of improving an ex-
isting health kiosk are analyzed, what modifications
were made, what benefits those modifications bring
to the table, as well as the difficulties faced on the
Silva J., BrandÃ
ˇ
co P. and Prior R.
Modular Health Kiosk based on Web Technologies.
DOI: 10.5220/0006297705170525
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

development and milestones that are to be reached in
order to have a fully functional system, capable of be-
ing deployed in different areas.
2 RELATED WORK
Using computers or other internet capable devices has
always been of great help in health related develop-
ments, not only with respect to machines used, the
type of devices available in hospitals but also in the
way the general population has access to health infor-
mation.
The evolution of technology made possible the
adaptation of several of those developments to health
areas, such as the phone, video, clarification of doubts
via e-mail, medical websites, and the creation and us-
age of electronic health records. (Verma et al., 2008)
With the increase in the variety and offer of medi-
cal devices, it rose the idea of grouping a set of these
devices associated with an application in order to cre-
ate a system capable of taking measurements of its
users to provide some feedback on their vital signs,
which otherwise would not be possible if its users
lacked the resources to acquire these devices or to
make visits to health centers. Currently the health
kiosk is a system capable of collecting data from a
blood pressure monitor, a weighing scale and a pulse
oximeter. Nonetheless, it is not limited solely to these
devices as new ones can easily be added to the system.
The idea of a system capable of collecting bio-
metric data from its users and show them the re-
sults is not new, as it can be seen in public locations,
where most of the time static, offline systems with
a small set of instructions provide the user valuable
information. In parallel some other types of kiosks
can be seen in some locations such as the informa-
tion kiosks that serve the purpose of disseminating in-
formation throughout the population (Nicholas et al.,
2003; Leeman-Castillo et al., 2010), they can be in-
ternet connected with the intent of remotely changing
the available information.
A more approximated system to our proposal is
the Multi-User Health Kiosk developed in a joint ef-
fort of the University of Pittsburgh and Carnegie Mel-
lon University. (Courtney et al., 2013) Their findings
provided helpful information on how to tackle the de-
velopment of a health kiosk. Creating a modular ar-
chitecture, to change in accordance to what is needed
or providing helpful, step by step, instructions on how
to use the devices, is information that, despite being
simple, has a major impact on the usability of the sys-
tem.
Since our aim with this system is to deploy it at
communities, public locations or medical facilities, a
multi-user approach must be made instead of creat-
ing a simple collection tool for a single user to use at
home. This has to take into account that the system
will be used by different users, with different charac-
teristics and different health needs.
A specific application case of this type of system
are elderly communities, as the need for attention on
their vital signs is higher due to the increased fragility
of human health over time. This type of deployment
has proven to be very positive with a high-level of
acceptance from its users. (Demiris et al., 2013)
The system is being developed making use
of commercially available Personal Health Devices
(PHDs). With the increased availability of these types
of devices, the price is more accessible, reducing the
total cost of assembling a system with these require-
ments. Some of the devices that are already working
with this system, and possible new devices, communi-
cate under a standardized form, which allows adding
new devices in a simpler way since the communica-
tion module handles all the devices.
The ISO/IEEE 11073 Personal Health Data (PHD)
Standards allow for the intended interoperability be-
tween some of the different devices that make up the
system. This standard appeared as a merge of differ-
ent standards such as ISO TC215, CEN TC251, IEEE
1073. (Nam et al., 2011) The Continua Health Al-
liance has a major impact both in the standard as well
as in the health care industry, trying to standardize
health devices in an orderly process, and also to make
it easier for developers to work around with these de-
vices.
Not having this standardization in some devices is
a problem since it means that an individual approach
must be made in order to interact with the devices. A
way to establish the communication has to be created,
as well as an interpretation of the messages sent by
the devices, and if needed to the devices.
The objective of reducing consultation times, and
keeping a more detailed patient’s history is achieved
by having access to these records. This implies that
the health kiosk in the future must be able to add
data to the patient’s Electronic Health Record (EHR)
this would improve the view the health professional
has on the patient’s history since the number of mea-
surements taken outside a medical facility should be
higher than inside one. Despite its benefits, it is not
an easy task to converge the user’s medical data of a
user and make it available at all medical facilities that
the user could visit. (Kalra, 2006) For now, a local
database serves the purpose of giving the patients the
possibility of saving and evaluating their history.
It is now possible, when using the health kiosk to

make use of a smart card reader, this option makes
it possible to extract data from the Portuguese Citi-
zenship card. This function helps not only to avoid
human error when inserting personal data, but also
as a way of reducing usage time of the application.
Further testing needs to be made in order to establish
the true value of this feature. The data available for
collection is public data that is visible in the physi-
cal card, no private data is accessible without a Per-
sonal Identification Number (PIN) that only the user
has knowledge of, besides text data it is also possible
to extract the picture of the user.
With the objective of being used in an autonomous
way by the patients, the usability of the health kiosk is
a concern. The current version of this system is an im-
provement to an existing version, which was assessed
in respect of the usability of the application. The dif-
ferences between the two versions will be address in
the next section. (Soares et al., 2016) Little changes
were made relative to the execution flow of the appli-
cation in order to take advantage of the information
that was collected regarding the usability. This eval-
uation of the application was based on observer-filled
questionnaires alongside the option of keeping track
of user clicks on the screen in order to evaluate the
number and position of clicks per screen to see the
changes to be made in the presented content.
3 OVERVIEW OF THE SYSTEM
An example of a health kiosk physical deployment is
visible in Figure 1, which has three devices associated
with it, a blood pressure monitor, a pulse oximeter and
a weighing scale that is not visible in the figure. The
interaction from the user is made through the use of
the touchscreen, if the user chooses to, it can insert
the citizenship card onto the smart card reader. After
the exams are finished, the results are printed in the
printer that is also visible in the figure.
Figure 1: Physical health kiosk.
Relative to the system architecture a representa-
tion is visible in Figure 2. The system has two possi-
ble types of devices, Continua Alliance Certified and
Non Certified Devices, at the moment all the devices
communicate via Bluetooth. Nonetheless, the devel-
opment of a way to communicate with the devices
takes one of two possible approaches, either the de-
vice is Continua Alliance certified and communicates
with an Antidote IEEE 11073 PHD interface, or it
is not certified and an individual approach must be
made in order to communicate with that specific de-
vice. The process of creating a way of communicat-
ing with a non-certified device can be applied to other
devices, creating a skeleton that is the base for the
development. Consequently, reducing the time of de-
velopment.
In the future we intend to have a connection to a
central EHR system, in order to make the patient’s
data available in different health kiosks, as well as to
health professionals. By sharing data along all differ-
ent locations that the users visit the impact the col-
lected information has is higher.
Figure 2: Overview of the System.
4 IMPLEMENTATION
The current development of the health kiosk has been
based on a previous existing version that, despite al-
ready having a functional flow, did not have the tools
for a proper continuous development. With that came
the idea of developing a version of the health kiosk
that used web technologies. The previous version
was developed using JavaFX, where some challenges
were found before the transition into the use of web
technologies. This transition came as an alternative
that could replace the existing version and at the same
time take advantage of features that are available with
the usage of this type of technologies, such as Web
Real Time Communication (WebRTC).
The application was developed on top of Electron,
a framework for building cross-platform applications
based on JavaScript, HTML and CSS. The Electron
1
framework was selected because it makes it possible
to communicate with the operating system directly us-
ing Node.js, while providing all the advantages of us-
ing web technologies (including the vast amount of
JavaScript libraries for building web applications).
The previous version was already assessed in
terms of usability (Soares et al., 2016). With that in
mind, the development of the new interface was made
trying to keep the same flow of interaction.
Some changes had to be made, either because of
the advantages of using web technologies, or because
the creation of new modules such as the smart card
reader implied new screens that the user has to inter-
act with. In the following subsections the adaptations
made to the system will be addressed.
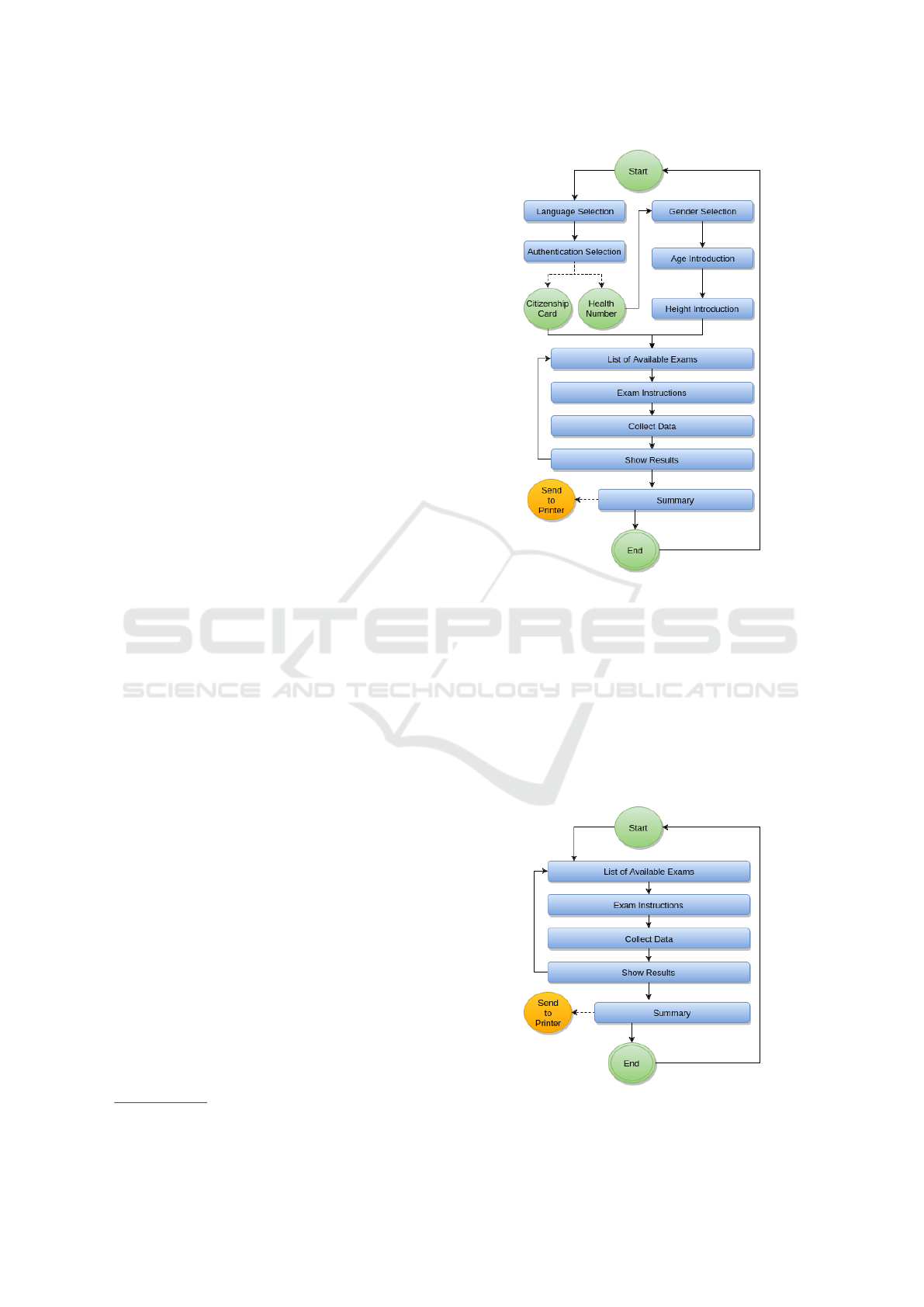
Regarding the usage of the application, there are
several possible cases of use due to the modularity of
the application. Figure 3 represents a full usage of
the application, this includes language selection, au-
thentication selection, performing exams and an end
summary. Figure 4 represents a smaller application
case, where no user data is collected, just the exams to
be performed and a summary with respect to the col-
lected data. These variations allow for different field
applications since what is intended is to adapt the ap-
plication to the users and/or scenario and not the other
way around.
The flows visible in the figures goes through sev-
eral steps, these steps being optional in some cases.
By configuring the system to follow the flow visible
in Figure 3 it gives the users the possibility of tak-
ing full advantage of all the features. Starting with
the language selection, the user is presented flags rep-
resenting all available languages. After selecting the
language, all texts and voice instructions to be pre-
sented to the user are in the selected language. The
user is presented now with the authentication method
selection, if the user chooses to use the citizenship
card all the necessary personal data is collected au-
tomatically. If not the user is presented with several
screens in order to insert the data by himself. After
having all the data, the user is presented with a screen
showing all exams that are to be performed. Subse-
quently the user iterates over each exam, following a
set of instructions, either by image or video, and eval-
uating the collected information on an intermediary
results page. In the end a table is shown presenting the
final results, and it is also visible in the screen a QR
Code containing all the information of that table that
is inserted as a calendar entry, all this is printed out to
give out to the user. After that, the system restarts and
is ready for a new user.
1
http://electron.atom.io/
Figure 3: Example of the flow of execution.
What is intended with this system is not only to
have the ability to collect data, process it and present
the results, but to give the option to the responsible
person to adapt the health kiosk in order to fulfill the
needs of its users. There are different use cases to the
health kiosk, some differences are related to the type
of data that is intended to be collected, other to the
necessity or not to collect user personal data, for that
the health kiosk must be modular and easily adaptable
to the circumstances.
Figure 4: Example of a simpler flow of execution.

4.1 User Interface
The usage of this system can be divided upon three
different stages, collecting personal data from the
user, collecting data from the devices, presenting re-
sults to the user.
When the patient starts the process of using the
health kiosk, it has the choice of either inserting a cit-
izenship card, and the application itself collects rele-
vant data from the card, or the user can himself insert
its personal data, such as the national health identifi-
cation number, gender, height and age.
After having all the user data collected, the next
step is to go through all the defined exams, after each
exam the user is presented with the results and a
chronological chart with all the measurements taken
with that device associated with the user. The col-
lected measurements are displayed in a bar, colored
green on what are considered default values for that
measurement with a gradient to red as it increases
the distance to those values. The intermediary re-
sults screen are visible in Figure 5, which represents
what it looked like in the older version of the health
kiosk, and Figure 6 represents the newer version of
that screen.
The proposed changes included an usage of
chronological graph, with the x axis being a time se-
ries, which means that the points take into considera-
tion the distance between the presented dates; center-
ing the next button and using a green color instead of
blue.
Figure 5: Blood Pressure Results on the previous version.
Figure 6: Blood Pressure Results on the new version.
In the final screen a table is presented with all col-
lected data, as well as a QR Code that upon reading
by a smartphone inserts in the default calendar app an
entry with all the collected data.
A page is also printed containing the user personal
data, the collected data and the QR Code. It also con-
tains a logo on the top that can be configured to fit the
needs of the situation.
The idea of using a QR Code to share data serves
not only the purpose of saving the data in the users
smartphones, but can also be used in the future as a
way of transmitting data to a health kiosk smartphone
application that if developed can act as a place where
the user can evaluate at any moment their vital signs
registry and even add other measurements that were
not made in the health kiosk.
The printing of the results, as well as the genera-
tion of a QR Code are optional functions that can be
disabled by the person responsible for the configura-
tion. This goes along with the idea of creating a sys-
tem that is highly configurable and capable of dealing
with the needs of its users.
4.2 Application Modularity
From the beginning one of principles of the develop-
ment of this health kiosk was the idea of modularity.
By creating a system that is based on this idea, adding
or removing elements, changing their order or using
the system with different configurations is a goal eas-
ier to achieve.
With that in mind, one of the main focus when
developing this application is the possible configura-
tions that the application should have. The use cases
can increase by creating a modular application. As
such, a configuration file was created, in which all
the possible options of the system are inserted. The
configuration file allows for the definition of which
screens to show, which exams are to be performed and
in which order to show them.
When having the possibility of choosing which
screens to be used, or which exams to perform, the
system is easily adapted to different use cases, from a
situation where no user data is needed such as a spe-
cific event where only a specific parameter is being
evaluated in a population to detect anomalies, to cases
where the system is deployed in a local place where
all the population can access it, and a record specific
to each user has more meaning.
A approach was made, when the system was being
developed, to try and simplify the process of adding
new exams or devices. A skeleton, based on web
components, is created for adding new exams to the
application, and if the device is certified, it can easily
be added to the system, needing only specific codes
for the parameters being read from the device.
Figure 7 represents an exam component, this com-
ponent can be reused in different cases, the compo-
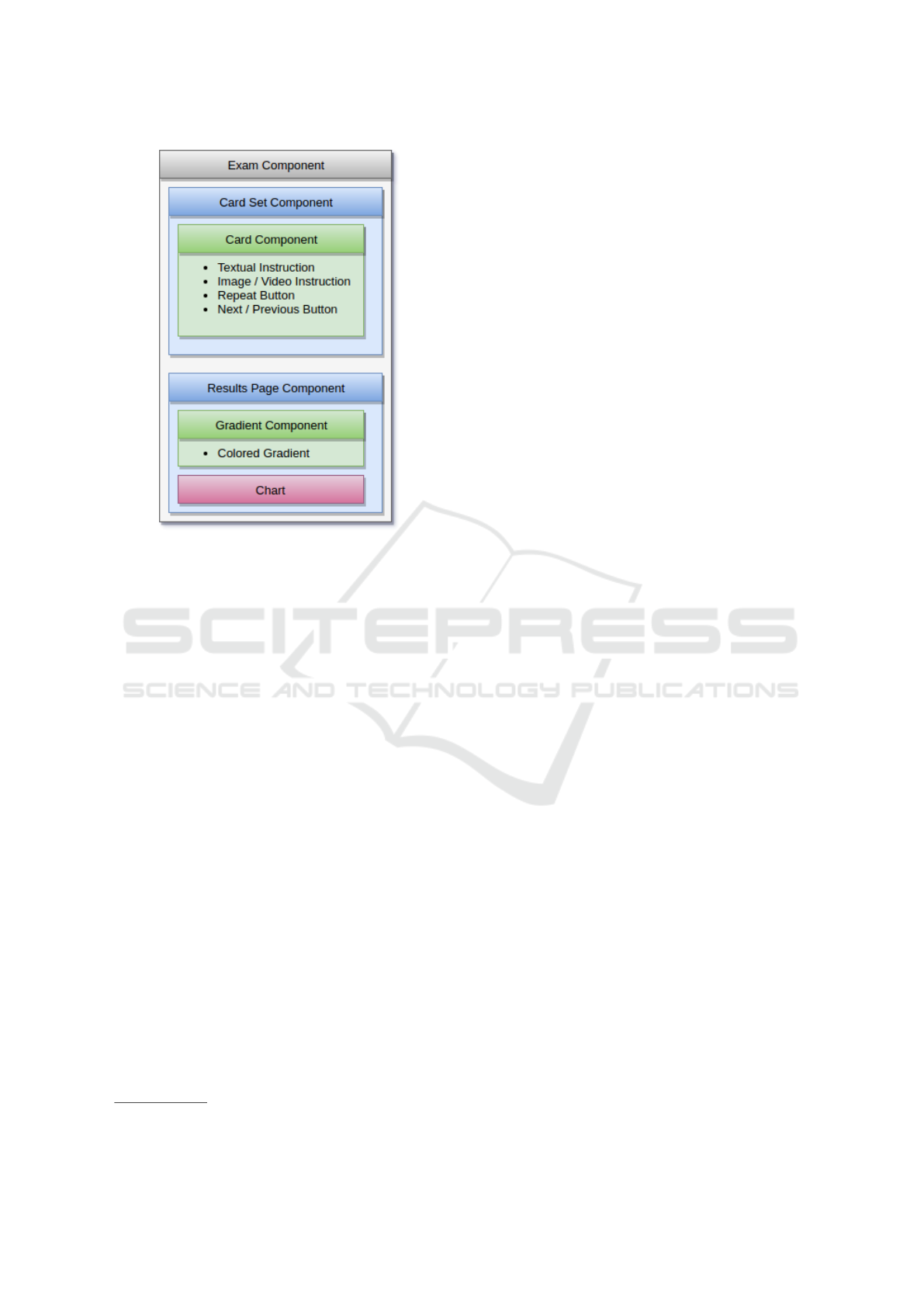
Figure 7: Representation of an Exam Component.
nent itself contains two different components, the card
set that is shown to the user with the instructions,
and the results component that is shown after the user
has passed through all the instruction cards. This ap-
proach was made throughout all the application in or-
der to facilitate adding new screens or elements to ex-
isting ones.
4.3 Internationalization
Although at the moment the smart card component
collects only data from Portuguese Citizenship cards,
and the national health identification number asked
is also the Portuguese one, this will not always be
the case, and the wide range of possible users of the
health kiosk must be taken into consideration. With
that in mind, we implemented in the system the pos-
sibility of using different languages, making use of an
internationalization framework
2
.
Having each text component associated with an id,
and for each language a set of ids with the respec-
tive text values, the process of making the application
available in new different languages was made easy.
As for adding a new language the development pro-
cess passes only through creating a file with all the id
and values pairs and the system is capable of dealing
with that information.
Although the previous version of the health kiosk
already had voice instructions, these were recorded
2
See http://i18next.com/.
by a person. This has some limitations in terms of
development. This initial approach made possible a
first development and evaluation on how sound in-
structions can help the user take the available exams.
However, it has several problems associated with it,
for perfect instructions no noise in the sound would
be preferable and this is not possible to achieve with
low cost recording devices. Another fact to take into
account is that even small changes to the audio in-
structions imply that a new recording session has to
be made.
To tackle these issues, we added digital voice in-
structions to the application. These voice instructions
are generated making use of the text-to-speech tech-
nology and saved into files to ensure that the produced
speech is the same across all systems. The process of
creating these instructions is the same as for the text
instructions, a set of values associated with an Id have
to be created, and then all these values are read and
a file for each available language is generated. Since
the voice’s used are the available ones on the operative
system, and new ones can be added, it is easily possi-
ble to add voice instructions in different languages.
4.4 Hardware
Currently the prototype of the health kiosk is de-
ployed in an all-in-one PC with a 22” touchscreen.
This prototype is capable of collecting from any pos-
sible combination of a blood pressure monitor, a
weighing scale, and a pulse oximeter. This system
has connected to it a printer in order to handout the
results to its users and a smart card reader to extract
data from the citizenship card.
The current supported and tested devices in the
system are two Continua Alliance Certified devices,
a blood pressure monitor (AND A&D Medical UA-
767 Plus BT-Ci) and a weighing scale (AND A&D
Medical UC-351PBT-Ci), and a non-certified device,
a pulse oximeter (Nonin 3230), this device commu-
nicates via Bluetooth Low Energy (BLE). Although
Nonin has a Continua Alliance compliant device we
used this one to develop and test the integration of non
Continua devices. Moreover, we also experimented
with the differences for a BLE device.
4.4.1 Device Communication
During the development of the new version, we cre-
ated modules to communicate with the devices. By
using Electron to develop the application, Node.js can
be used in order to access the operating system di-
rectly, which would not be possible if a browser ap-
plication were to be developed.

Using a Node.js module (node-dbus), made it
possible to develop a new module capable of commu-
nicating with the existing Continua Alliance certified
devices, and to easily add new devices as long as in-
formation about the devices is previously given to the
developers in order to properly extract relevant infor-
mation produced by the device.
Continua Alliance certified devices, generate data
in eXtensible Markup Language (XML) format, hav-
ing the relevant medical data associated with a spe-
cific Id for the parameter, it also provides information
relative to the date of the measurement. It also con-
tains parameters that can hold information about the
physical device.
Since the objective of the application is to adapt to
the users and not the other way around a decision had
to be made in order to support non certified devices
since there is a possibility of these types of devices
being cheaper for some possible use cases. This deci-
sion goes along with the idea of creating an adaptive
system that is not closed in terms of compatible de-
vices.
For the case of the Nonin Oximeter 3230, as it
is not a Continua Alliance certified device a different
approach had to be made. Since this device commu-
nicates via BLE it was decided that taking advantage
of a Node.js modules (Noble) was an appropriate way
to develop the means to communicate with these types
of devices. For that a module was created that takes
the MAC Address of a device, starts scanning until
the device is found, after connecting to the device it
has to activate the characteristic of the device respon-
sible for sending data via Bluetooth, when that is done
a stream of continuous data is received by the appli-
cation, being decided that upon a number of repeti-
tions that value was to be considered and the stream
stopped.
The development of these new modules will allow
a simpler development in the future since the base of
the communication is already implemented and what
is required is to adapt it to the new devices is an eval-
uation of the device in order to proper assess what
messages it sends, how it sends them and what is the
best way to extract information from them.
4.5 Usability
Being an application that evolved from an existing
one, and since the previous version had an usability
evaluation, what was made when developing this ap-
plication was to follow the flow of interaction pro-
vided in that application. The usability of the pre-
vious version was studied in different scenarios, at
the university open days (by 195 users), at a health
day in one of the university schools (46 users), during
a week at a local city hall (127 users) and for thir-
teen days in thirteen different villages in Brazil (465
users). This covered different age groups, and usage
information was retrieved not only from the applica-
tion but also from the evaluation on how people used
the system. The evaluation used observer-filled ques-
tionnaires and user click tracking. The evaluation did
not use the standard user questionnaires as we per-
ceived them as either too long or less appropriate than
a researcher observing the usage. More details can be
seen in (Soares et al., 2016).
At the moment the usability of the current system
has not been tested by a large population. The tools
for assessing time spent on each screen and where the
user has clicked throughout the usage are developed
and will soon be tested. This will allow us to evaluate
if the interface is easily usable, if the user has the abil-
ity to use the application from start to finish without
any assistance, or if so which screens are taking more
time from the flow of interaction.
The collection of time spent on each screen can
help us determine if the instructions on the screen are
easy to understand, and for instance, if having the
ability to use a citizenship card is quicker and more
adopted than introducing the data manually.
By also collecting the coordinates of the clicks and
group all clicks made in a single screen presenting
them on top of a screen representation it is possible to
determinate if the screen is usable, and if it is being
used in the most correct way. If a large group of peo-
ple click somewhere in the screen that is not intended
to be clicked then something is not right about that
screen and must be evaluated.
More consideration has to be made in order to
proper evaluate the usability by using these methods,
such as the elimination of outliers that could affect the
visualization of the problems on the screen. A small
amount of users could make excessive clicks in wrong
places or spent too much time in certain screens and
with that alert for a non existing problem.
The usability of a previous version of the health
kiosk has been tested (Soares et al., 2016) with the
same idea of representing clicks on a screen represen-
tation, which is visible on Figure 8.
Figure 8: Weight measurement result screen usage pattern.

In Figure 8 it is possible to evaluate that users try
to interact with the color gradient before clicking on
the button to show the new screen. This type of infor-
mation allow us to consider what steps to take to make
the application more fluid, with quicker and better re-
sponses from the users.
4.6 Configuration Tool
Both on the previous version as well as in the new
version there was a unique point in the system that
was responsible for the configuration of the system.
The configuration file is currently responsible to
allow for the definition of which screens to be shown
or wich personal data to collect, if features such as QR
Code, printing, voice instructions should be used or
not in the application among other different options.
For easier configuration, all possible configurable
values must be in this file. At this moment it is under
development a tool that will allow for non-technical
users to configure the health kiosk. A preview of the
application interface is visible in Figure 9, this appli-
cation will be divided in several blocks of configu-
ration grouped by what is being configured, such as
available languages, what type of authentication is to
be used, what exams are to be performed. The de-
velopment of this tool is not only important to make
the health kiosk configurable without technical help
but also to evaluate what truly is configurable in this
system.
Figure 9: Current status of the Configuration Tool.
5 CONCLUSIONS
A system such as the health kiosk could have a major
impact in different possible scenarios, such as rural
areas lacking medical resources or health centers with
higher attendance than the one they can process. De-
ploying this system in these locations, makes it pos-
sible for the population to, by themselves, measure
their vital signs.
The current prototype makes use of a simple
weighing scale, a portable blood pressure monitor and
pulse oximeter, an evaluation of possible changes to
this setup is undergoing, with the idea in mind of hav-
ing devices simpler to use and that possibly collect
more data. One example is going from a normal blood
pressure monitor that the user has to set up and adjust,
to one where the user simple introduces the arm in the
fixed device and waits for the results. Also, weighing
scales capable of evaluating body fat are also an al-
ternative to the current existing ones. One point that
has to be considered is relative to the powering of the
devices, presently all the devices are battery powered,
which is not feasible in large scale.
At it was already referred, the configuration of
the health kiosk is made by editing an existing con-
figuration file with the desired values, but a Graphi-
cal User Interface (GUI) is being integrated into the
health kiosk system soon that will allow for anyone
responsible for the health kiosk to edit the configura-
tion without knowledge of the technical details.
It is also being developed under a master’s the-
sis project a module that will allow the establishment
of a video conference, using WebRTC, in which the
patient can get help on how to use the device or ask
for a medical opinion on the collected data. Due to
the possibilities of WebRTC, the health professional
is not only able to establish a video conference, but it
is also able to have access to data from the applica-
tion, and to send data to the application. This creates
the possibility of having remote instructions that can
change the status of the application.
ACKNOWLEDGEMENTS
This article is a result of the project NanoS-
TIMA Macro-to-Nano Human Sensing: Towards In-
tegrated Multimodal Health Monitoring and Ana-
lytics, NORTE-01-0145-FEDER-000016, supported
by Norte Portugal Regional Operational Programme
(NORTE 2020), through Portugal 2020 and the Euro-
pean Regional Development Fund.
REFERENCES
Courtney, K. et al. (2013). Designing the community multi-
user health kiosk. Enabling Health and Healthcare
Through ICT: Available, Tailored and Closer, 183:79.

Das, R. and Padhy, H. M. (2014). Health monitoring kiosk:
An effective system for rural health management. In-
ternational Journal of Innovations in Engineering Re-
search and Technology, IJIERT, 1(2).
Demiris, G., Thompson, H., Boquet, J., Le, T., Chaudhuri,
S., and Chung, J. (2013). Older adults’ acceptance of
a community-based telehealth wellness system. Infor-
matics for Health and Social Care, 38(1):27–36.
Kalra, D. (2006). Electronic health record standards. IMIA
Yearbook of Medical Informatic, pages 136–144.
Leeman-Castillo, B., Beaty, B., Raghunath, S., Steiner, J.,
and Bull, S. (2010). LUCHAR: Using computer tech-
nology to battle heart disease among latinos. Ameri-
can Journal of Public Health, 100(2):272–275.
Nam, J.-C., Seo, W.-K., Bae, J.-S., and Cho, Y.-Z. (2011).
Design and development of a u-Health system based
on the ISO/IEEE 11073 PHD standards. In The 17th
Asia Pacific Conference on Communications, pages
789–793. IEEE.
Nicholas, D., Huntington, P., and Williams, P. (2003). Three
years of digital consumer health information: A lon-
gitudinal study of the touch screen health kiosk. Inf.
Process. Manage., 39(3):479–502.
Soares, E., Oliveira, C., Maia, J., Almeida, R., Coimbra,
M., Brandão, P., and Prior, R. (2016). Modular health
kiosk for health self-assessment. In Computers and
Communication (ISCC), 2016 IEEE Symposium on,
pages 278–280. IEEE.
Suggs, L. S. (2006). A 10-year retrospective of research in
new technologies for health communication. Journal
of health communication, 11(1):61–74.
Verma, A., Dhand, H., and Shaha, A. (2008). Healthcare
kiosk next generation accessible healthcare solution.
In e-health Networking, Applications and Services,
2008. HealthCom 2008. 10th International Confer-
ence on, pages 194–199. IEEE.
