
Research of the Autonomic Regulation in the Formation of the Brain
Microwave Radiation Restoration Processes during Rehabilitation of
the Stroke Patients
Study by Means of the Multifractal Analysis of the Radiophysical Complex
MRTHR Signals
Vladimir Kublanov
1
, Vasilii Borisov
1
, Yan Kazakov
2
and Alexander Azin
3
1
Ural Federal University, Mira 19, 620002, Yekaterinburg, Russian Federation
2
Ural State Medical University, Repina 3, 620028, Yekaterinburg, Russian Federation
3
Mari State University, Lenina 1, 424000, Yoshkar-Ola, Russian Federation
Keywords: Multifractal Cross-Correlation Analysis, Brain Microwave Radiation, Heart Rate Variability, Rehabilitation
Processes, Stroke Patients, DCASNS.
Abstract: The paper discusses the possibility of applying multifractal cross-correlation analysis method for the joint
processing of transient biomedical signals received via the Radiophysical complex MRTHR (Medical Radio-
Thermograph - Heart Rate) for rehabilitations estimations. The results of the multifractal cross-correlation
analysis application are shown for research the role of the autonomic regulation in the formation of the brain
microwave radiation (intrinsic electromagnetic radiation of the brain) in the treatment process. A pilot clinical
study obtained by the multichannel Radiophysical complex MRTHR had shown the dynamics discrepancies
of cross-correlation Hurst exponent coincides with the clinical data for patients after passing through the
course of rehabilitation using techniques of the dynamic correction activity of the sympathetic nervous
system.
1 INTRODUCTION
It is well known, that the main mechanism for
ensuring the constancy of the internal environment of
the body, is the autonomic nervous system (ANS).
The ANS adapts all regulation systems to
environmental changes (Guyton and Hall, 2011). The
ANS can be considered as the complex of structures
that are parts of the peripheral and central divisions of
the nervous system that regulate the functions of
organs and tissues. This regulation is aimed at
maintaining the body relatively constant internal
environment (homeostasis).
Among the main factors that contribute to changes
in regulation of cerebral circulatory system are:
the vascular tone change;
the intravascular pressure;
the shear stress on the vascular wall;
the streaming blood characteristics;
the chemical composition of the blood;
the blood viscosity
the activity of the autonomic regulation;
the dependence of the perfusion pressure in the
brain on the value of intracranial pressure
(Moskalenko, 1992).
The actuator in the regulation mechanism of the
cerebral circulation are the muscles of the vascular
wall. The muscles perceive irritation of specialized
receptor and chemical compounds released into the
bloodstream and the environment. In addition,
muscles perceive the mechanical stretching of the
intravascular blood pressure and are sensitive to a
variety of substances, which are the products of
cellular metabolism (Pocock and Richards, 2013).
According to the anatomical criteria the ANS is
divided into the segmental and suprasegmental
divisions (Schmidt and Thews, 1989). The segmental
division of the ANS provides the autonomic
innervation of the individual segments of the body
and internal organs, which belong to them. It is
divided into the sympathetic and parasympathetic
divisions (SNS and PSNS, respectively). The heart
rate variability signal (HRV) is an example of the
Kublanov V., Borisov V., Kazakov Y. and Azin A.
Research of the Autonomic Regulation in the Formation of the Brain Microwave Radiation Restoration Processes during Rehabilitation of the Stroke Patients - Study by Means of the
Multifractal Analysis of the Radiophysical Complex MRTHR Signals.
DOI: 10.5220/0006157102990306
Copyright
c
2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
standard instruments of functional diagnostics.
This choice in our study is not accidental. The
HRV signals are indicators of the ANS activity (Malik
et al., 1996). The role of the autonomic regulation of
the formation of functional processes in the brain
tissue is poorly understood. The suprasegmental
divisions of the ANS are involved in organisation
cerebral circulation. Although clinical trials of its
activity depends on the effectiveness of rehabilitation
of vascular lesions of the brain (Kublanov et al.,
2010). Particularly there is no data on the effect of the
autonomic regulation on the formation of the brain
microwave radiation.
Based on this, the aim of this paper is to apply the
multifractal estimates for the autonomic regulation in
the formation of brain microwave radiation
restoration processes during rehabilitation of the
patients.
2 MATERIALS AND METHODS
2.1 Radiophysical Complex MRTHR
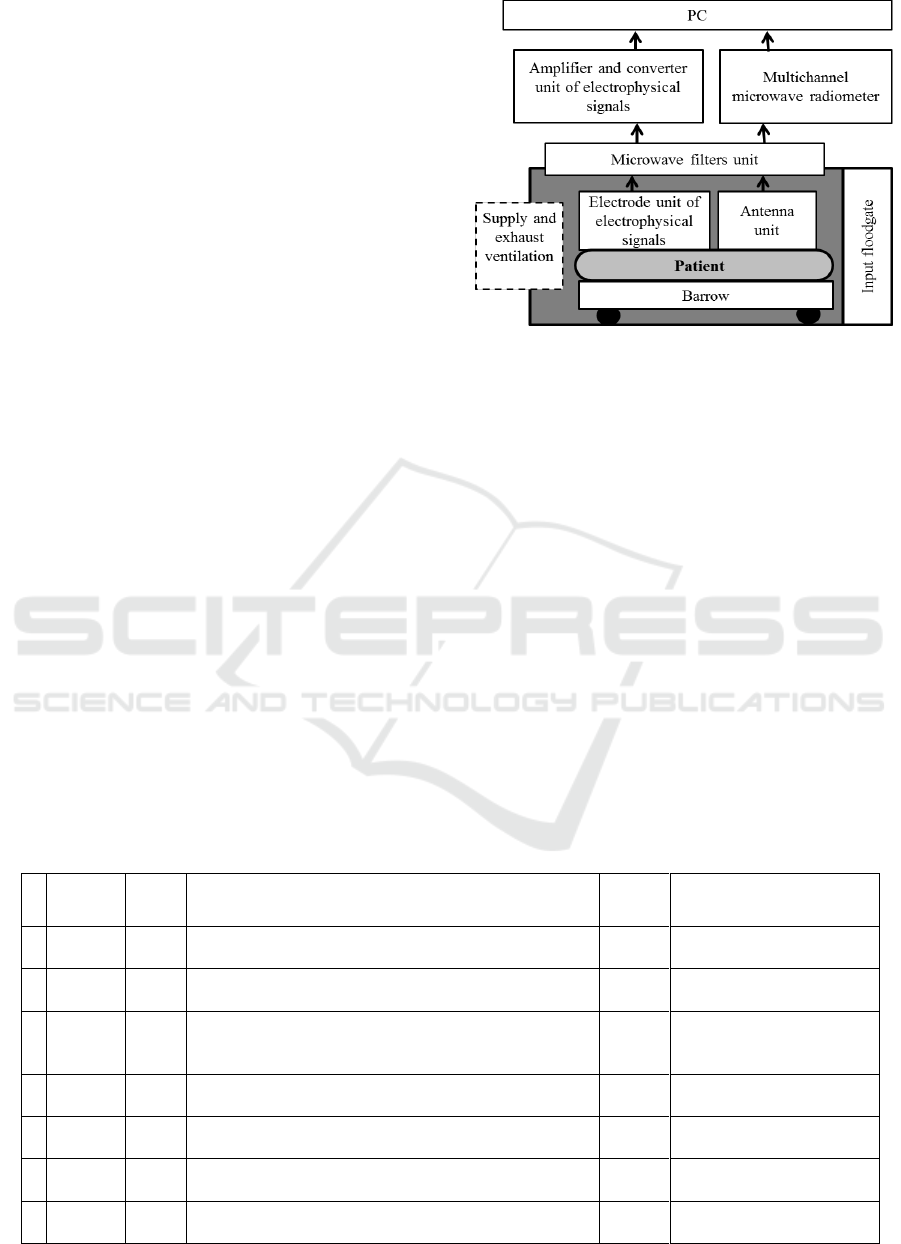
In this study two signals forms the information
channels of multichannel Radiophysical complex
MRTHR: the HRV and brain microwave radiation
(Kublanov, 2013). Figure 1: Structural diagram of the
Radiophysical complex MRTHR for examining
patients (Kublanov, 2013).
The HRV signals are obtained from the
electrocardiography registered by means of the
electrophysical signals channel. The microwave
radiometer registers the brain microwave radiation in
650-850 MHz range.
Figure 1: Structural diagram of the Radiophysical complex
MRTHR for examining patients.
2.2 Patients
Signal analysis was made based on studies conducted
in the Sverdlovsk regional clinical psycho-
neurological Hospital for War Veterans (SRCPNH,
Yekaterinburg). Investigations were carried out for
the group of seven patients suffering from ischemic
stroke (before and after rehabilitation treatment).
All patients gave their informed consent to
voluntary participate in the study. The study was
approved by the Ural State Medical University ethics
committee (protocol №8 from 16.10.2015). The
Table 1 shows the clinical data for group of patients.
The rehabilitation of patients after ischaemic
stroke was performed in accordance with Guidelines
for Management of Ischaemic Stroke and Transient
Ischaemic Attack 2008 (Ringleb et al., 2008).
Table 1: Clinical data of the studied patients group from the SRCPNH.
№
n
Patient/
sex
Age,
years
Stroke localization.
Clinical data.
ICD-10
Amount of the DCASNS
séances
1
T.V.S./
male
53
Left middle cerebral artery basin, with elements of
aphasia, early recovery period (up to the year)
I63.5
10
2
Z.I.G./
male
40
Ischemic stroke in Right Internal Carotid Artery basin
3 and 2 years ago. Arterial Hypertension III st.
I63.2,
I10
10
3
G.V.L./
male
76
Isсhemic stroke in Right middle cerebral artery 3
years ago, right hemiparesis. Diabetes mellitus.
Arterial Hypertension III st.
I63.5,
I10,
E11.6
10
4
K.M.F./
female
73
Isсhemic stroke in Left middle cerebral artery,
residual effect. Ischemic heart disease. Heart failure.
I63.5,
I25.8
10
5
D.L.I./
male
66
Chronic cerebral ischaemia III.
Arterial Hypertension III st.
I69,
I10
10
6
D.K.A./
female
71
Stroke in right internal carotid artery (1 month ago).
Arterial Hypertension III st.
I63.2,
I10
10
7
S.V.I./
male
49
Ischemic stroke in Right Internal Carotid Artery.
Arterial Hypertension III st.
I63.2,
I10
10
In addition, patients were treated with the neuro-
electrostimulation device – “SYMPATHOCOR-01”
course of the dynamic correction activity of the
sympathetic nervous system (DCASNS) (Kublanov
et al., 2015). For these patients clinically proven
improvement was observed after rehabilitation
course.
2.3 Multifractal Cross-correlation
Analysis
In our study, we propose to evaluate the information
characteristics of the signals of the brain microwave
radiation and HRV using method of multifractal
formalism. Nowadays, application of the multifractal
analysis is common in the brain research (Pavlov et
al., 2016; Whalley et al., 2016; Závodszky et al.,
2015). Registration and analysis of these biomedical
signals at the same time, gives a qualitatively new
features that allow one to define a new integral
indicator for the study of the functional changes in the
brain in a state of preclinical and clinical practice in
the early stages of development of these changes
(Kublanov et al., 2015).
Application of the multifractal cross-correlation
analysis (MFCCA) method on two signals should be
carried out at the same time windows (Podobnik and
Stanley 2008). Based on this, in further signal
analysis ten second time windows were considered. It
can be assumed that the important properties of the
signal, there are only in a certain range of scales,
where properties are most distinct characteristic of
multifractal structure (Di et al. 2015; Delignières et
al. 2016).
Generally, in analysis of HRV signals applied:
HF spectral component, which characterize
activity of the parasympathetic department of the
ANS and activity of the autonomic regulation loop;
LF spectral component, which mainly
characterize activity of the sympathetic vascular tone
regulation centre. (Malik M. et al., 1996).
The fluctuations of very low-frequency (VLF)
spectral component of the HRV signal in range
(25-300), sec are complex two- or three- formation
(Fleishman 2005). Because of that the dynamics of
changes in the aggregate analysis of signals obtained
estimates of the HRV and brain microwave radiation
signals is not advisable to carry out throughout the
VLF range. It is appropriate to carry out analysis on a
set of time windows.
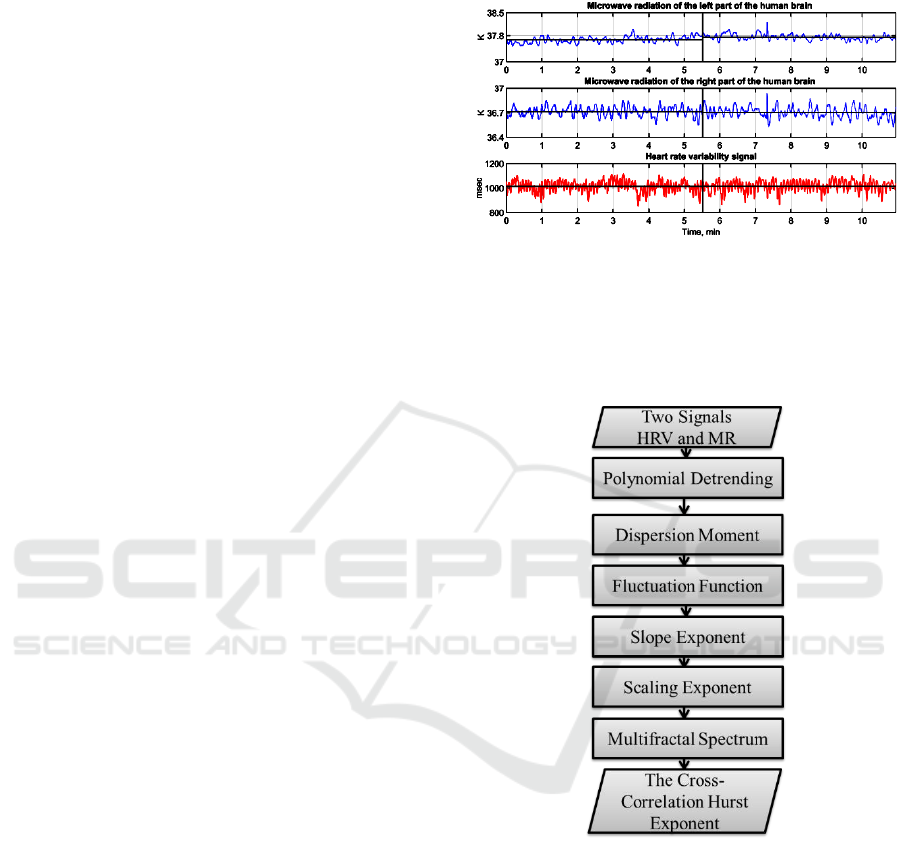
To acquire summary estimation of the microwave
radiation of biomedical signals, which indicate the
ANS variability, one must transform the original
biomedical signals to equidistant time series (TS)
with the same sampling frequency 10 Hz (Example of
signals is presented in Figure 2).
Figure 2: Simultaneously recorded signals of the Brain
Microwave Radiation and HRV.
After interpolation, the investigated TS are accessed
by the multifractal cross-correlation analysis. Stages of
MFCCA are shown in Fig.3 (Kublanov et al., 2016).
Figure 3: Stages of multifractal cross-correlation analysis.
The usage of multifractal analysis as an effective
tool to study the possibilities and identify short-term
series HRV was presented in (Kublanov et al., 2015).
There it was shown that one parameter – cross-
correlation Hurst exponent H
2
is enough for obtaining
information significant estimates of the autonomic
regulation in the formation of brain microwave
radiation.
In accordance with that article, simultaneous
analysis of TS for signals the brain microwave
radiation and HRV indicates the relationship between
multifractal parameters for group for healthy subjects.
It was determined that:
processes describing sympathetic activity of the
ANS with fluctuation periods in the range from 6.5 to
25, sec and transport dynamics of the fluid in the
intercellular and intracellular spaces brain tissue
fluctuation periods ranging from 20 to 40, sec are
similar.
processes that characterize the activity of the
central ergotrophic and humoral-metabolic
mechanisms of heart rate regulation, defined by VLF
fluctuations of the HRV in the range from 25 to 300,
sec and the thermodynamic processes in the
regulation of brain tissue fluctuations with range from
60 to 70, sec are similar.
As shown previously (Kublanov et al, 2016), the
diagnostic capability of the computed multifractal
characteristics in two functional states for the above
mentioned time windows can be determined by a
Bland-Altman's criteria (Bland and Altman, 1986) as
follows:
assessment of systematic differences calculated
as the difference between each measurement pair;
calculation of the mean and standard deviation
for these differences, characterizing the degree of
variation of results.
3 RESULTS AND DISCUSSIONS
Data analysis of multifractal estimates were provided
for the HRV and brain microwave radiation signals
obtained using the MFCCA method for the group of
patients (shown in the Table 1). For signals of the
HRV and brain microwave radiation multifractal
estimates obtained by the MFCCA, difference of the
Hurst exponents was calculated in two functional
states: at rest and during antiorthostatic load. The
analysis was conducted on time windows (20-30; 30-
40;
60-70, sec) as specified in the article (Kublanov et al.,
2015).
Obtained estimation are presented before and after
the course of rehabilitation using techniques of the
DCASNS. In all the tables below, negative values
indicate a “shift” of the cross-correlation in direction
of the antiorthostatic load, positive values – in
direction of rest (Fig. 4).
Figure 4: State F ─ functional rest [0,300] sec;
state A ─ antiorthostatic load (30
0
) [300,600] sec.
3.1 Patient One
The clinical data of the patient T.V.S. showed
reduction of the ataxia (instability) severity in
Romberg’s sign, decreased effects of motor aphasia,
rate of speech and articulation improvement. Blood
pressure and heart rate indices - have not changed.
During the period of treatment there were no
hemodynamic deterioration.
The DCASNS method mode function stellate
ganglion block (blocking the activity of the SNS) was
used for this patient. Clinical outcome was
accompanied by a decrease in LF / HF ratio from 2.64
(the predominance of sympathetic tone) to 1.56
(normal). This effect is associated with the SNS
predominant tone with respective pathogenesis and
clinical manifestations. Moreover, the duration of
disease is relatively low: early post stroke recovery
period - during the year.
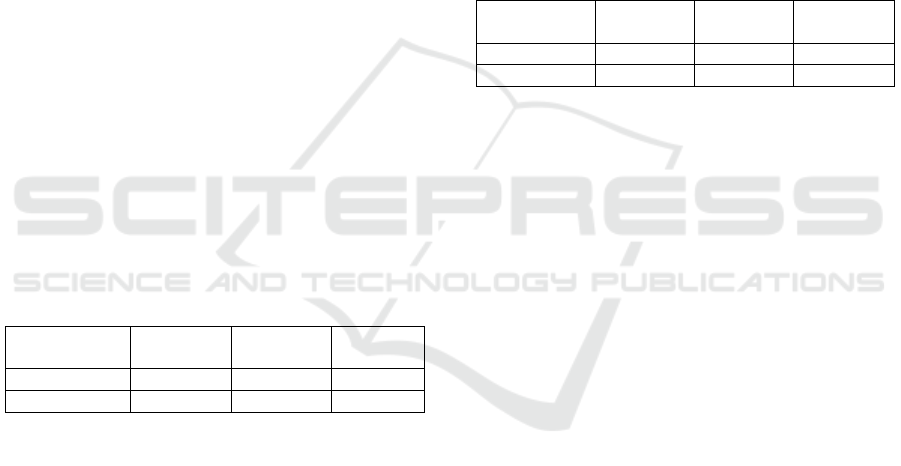
Table 2: Systematic discrepancy assessments of the cross-
correlation Hurst exponent for the HRV and brain
microwave radiation signals for patient T.V.S.
Time
window
20-30, sec
30-40, sec
60-70, sec
Before
-0,04460
-0,11771
-0,17561
After
0,02878
0,27910
0,00551
In accordance with the Table 2, the normalization
of autonomic balance for the segmental divisions of
the ANS was accompanied by an increase in
conjunction with oscillatory processes that reflect the
transport of tissue fluid in the matter of the brain at
rest and during antiorthostatic load.
Based on that it can be assumed that the
synchronization processes in the ANS (at the
segmental level) have a relationship with the
normalization of the function of suprasegmental
(brain) autonomic structures. Synchronization of
processes can be explained by activation
(normalization) process and neuroplasticity of the
nervous trophism, caused by the DCASNS method.
State F
State A
3.2 Patient Two
In accordance with the clinical data of the patient
Z.I.G. headaches decreased (frequency, duration,
intensity, reduced the number of analgesics taken to
anesthesia). Achieved target blood pressure (less than
120 mm Hg). Decreased subjective phenomena of
weakness. Decreased levels of anxiety (from 12 to 7
grades) (Boakye et al., 2016).
For this patient mainly the DCASNS stimulation
activity mode of the SNS was used. Initially, reduced
tone of the SNS was accompanied by headaches, and
anxiety disorders. As the result of the DCASNS tone
of the SNS increased. LF / HF ratio increased from
0.25 to 1.05.
All patient's clinical parameters were determined
by "shift" of autonomic regulation on the segmental
level – reduction of HF and LF, and suprasegmental
hypothalamic. The “shift” happened a long time
(three years) after vascular accident and manifested
itself in slowdown of the vascular tone regulation
process. The leading treatment effect was a slight
increase in power modulating effects of segmental
structures of the ANS (the nerves of the heart). The
disappearance of headaches was caused by the
expansion of the adaptation corridor of vascular tone
(in an increment of the total power spectrum of HRV
- total power index).
Table 3: Systematic discrepancy assessments of the cross-
correlation Hurst exponent for the HRV and brain
microwave radiation signals for patient Z.I.G.
Time window
20-30, sec
30-40, sec
60-70,
sec
Before
-0,18838
-0,24459
-0,12457
After
0,10135
0,03153
-0,05517
According to the data presented in the Table 3, the
normalization of autonomic balance in the segmental
divisions of the ANS in a state of rest was
accompanied by an increase of cross-correlation level
with oscillatory processes that reflect the transport of
tissue fluid in the brain substance alone. At the same
time, the relationship between the thermodynamic
processes in the brain and VLF component of the
spectrum of HRV increased. This finding indirectly
confirms the currently existing ideas about the nature
of VLF waves (as one that reflects the
thermoregulatory processes) (Fleishman, 2005).
3.3 Patient Three
Pursuant to the clinical data of the patient G.V.L.
systolic blood pressure decreased to target values
(less than 120 mm Hg for patients with diabetes).
Reflexes with limb asymmetry decreased. The
appearance of hemiparetic gait reduced. The
hemiparesis severity decreased from 3 to 2 grades.
The DCASNS stimulation biotropic field
parameters were individually selected with
predominant target – the activition of the SNS. It
resulted in balance normalization of the sympathetic
and parasympathetic regulation of the heart, coursed
by diabetes and diabetic autonomic neuropathy.
Improvement of the decreased tone of the SNS,
allowed to achieve the normalization of segmental
regulatory effects on vascular tone, and a significant
regression of neurological symptoms.
Table 4: Systematic discrepancy assessments of the cross-
correlation Hurst exponent for the HRV and brain
microwave radiation signals for patient G.V.L.
Time
window
20-30, sec
30-40, sec
60-70, sec
Before
-0,09742
0,04123
-0,09871
After
0,00758
0,06727
0,01680
According to the Table 4 for a patient with severe
organic lesion of segmental and suprasegmental
autonomic structures have achieved a certain
normalization of autonomic balance in segmental
divisions of the ANS in a state of rest. In other words,
the DCASNS influence preserved insufficient
regulation reserves by stimulating the processes of
transport of tissue fluid (mechanisms of trophism and
neuroplasticity) in the matter of the brain. This in turn
provided normalization of autonomic reactivity in
functional loads (within the stored reserves of the
regulation) (Kessner et al., 2016; Lundborg, 2005).
At the same time, a positive impact of the DCASNS
on segmental autonomic structures (the
hypothalamus) was indicated by some normalization
of reactivity of the thermodynamic processes in the
brain at antiorthostatic load.
3.4 Patient Four
In conformity with the clinical data of the patient
K.M.F. fatigue phenomenon decreased, disappeared
noise in the head, dizziness. The blood pressure
normalized - hypotension phenomena have
disappeared. The symptoms of anxiety scale reduced
(from 14 to 11 grades) (Hurley and Tizabi, 2013;
Stetler et al., 2014).
Application of the DCASNS method in the
stimulation mode managed to maintain an increased
tone of the SNS. Furthermore, it allowed maintaining
a normal perfusion of blood through the arterial bed
and the maintenance of normal values of blood
pressure. These values ensure the normalization of
blood flow through the brain and restoration of the
cerebral blood flow performance after stroke. Little
effect was associated with initially low levels of total
power of HRV – i.e low modulating effects on the
heart of segmental division.
Table 5: Systematic discrepancy assessments of the cross-
correlation Hurst exponent for the HRV and brain
microwave radiation signals for patient K.M.F.
Time window
20-30, sec
30-40, sec
60-70, sec
Before
-0,15419
0,03370
-0,06882
After
-0,04550
-0,02534
0,04625
In accordance with the Table 5 for this patient was
observeddecreased HRV correlation of signals in LF-
and of HF - bands with their brain microwave
radiation in the respective time windows. This
coincides with the target values of the blood pressure
- the necessity to maintain high tone of the SNS. At
the same time, there was a significant increase in
correlation, both at rest and during antiorthostatic, for
stress indicators of the brain microwave radiation
(thermoregulation) with VLF-component of the HRV
spectrum. This, in turn, may indicate a preferential
activation of the suprasegmental autonomic
structures (the hypothalamus) when this particular
mode the DCASNS method is selected.
3.5 Patient Five
In appliance with the clinical data of the patient D.L.I.
there was a normalization of elevated blood pressure.
The target blood pressure was achieved - less than
130/80 mm Hg. It was possible to reduce the tone of
the SNS by means of the DCASNS method in
blocking mode. Which, in turn, resulted in lowering
of blood pressure.
Table 6: Systematic discrepancy assessments of the cross-
correlation Hurst exponent for the HRV and brain
microwave radiation signals for patient D.L.I.
Time window
20-30, sec
30-40,
sec
60-70, sec
Before
-0,05011
-0,03088
-0,07643
After
0,18664
-0,19695
0,30650
According to the data presented in the Table 6, the
patient has a reduced correlation of HRV LF signals
in the range, the effect associated with initially
elevated tone SNS. At the same time, the relationship
of the thermodynamic processes in the brain and
VLF-component of the HRV spectrum increased
(Togo et al., 2006).
3.6 Patient Six
The clinical data of the patient D.K.A. provides
insight of achieved gradual reduction for high blood
pressure in the range of target values in the acute
phase of stroke. There was an increase caused by a
reduced stroke force of muscles on the left. At the
same time, there was a decrease of pathologically
elevated tone of the left limbs.
For the DCASNS method, biotropic parameters of
physical fields were selected to block the SNS. By
using that, it was possible to dramatically reduce
increased tone of the SNS and to normalize the
autonomic balance. This resulted in improvement of
blood perfusion on the arterial bed by reducing the
weakening of hypervasoconstriction degree. This, in
turn, ensured the normalization of blood flow through
the head brain and recovery rates of cerebral blood
flow after stroke.
Table 7: Systematic discrepancy assessments of the cross-
correlation Hurst exponent for the HRV and brain
microwave radiation signals for patient D.K.A.
Time window
20-30, sec
30-40, sec
60-70, sec
Before
-0,04999
-0,06435
-0,10949
After
-0,14435
0,25473
0,01954
In accordance with the Table 7 for a patient with
severe acute organic central nervous system disease
(acute ischemic stroke) achieved normalization of
autonomic maintenance - increase of the correlation
between HF indicators of the HRV and the brain
microwave radiation. Moreover, autonomic reactivity
was moted - increased correlation of the module LF
and the brain microwave radiation in a time window
of 60-70 for state of antiortostic load.
This confirms the restoration of suprasegmental
autonomic regulation processes in the brain. In other
words, activation of a fluid transport processes
(neuro-trophic, neuroplasticity), as thermoregulation
processes.
3.7 Patient Seven
According to the clinical data of the patient S.V.I.
high blood pressure failed to normalize after the first
course the DCASNS method. This can be explained
by the presence of comorbidity, in violation of the
mechanisms of autonomic regulation of vascular
tone. Also this complicates treatment and worsens the
prognosis – anxiety and depressive disorders.
Indicators of the Hospital Anxiety and Depression
Scale patient had evidence of clinically significant
depression (Varidaki et al., 2016)
After re-hospitalization and new selection of the
biotropic physical parameters for the DCASNS
method it was possible to normalize blood pressure.
The presence of depression, worsen cardiovascular
disease due to a persistent increase of the tone of the
SNS, were the factors that prolonged treatment and
made difficult to achieve positive clinical (Jeong et
al., 2016).
The patient required repeated the DCASNS
courses with individual selection of the biotropic field
parameters. As a result, moderate decline in the tone
of the SNS happened. The achievement of a
significant antidepressant effect revealed in reduction
of the severity of depressive symptoms at the hospital
anxiety and depression scale. Moreover, it achieved
normalization of blood pressure (Rial et al., 2016).
The effect can be associated with initially elevated
tone of the SNS.
Table 8: Systematic discrepancy assessments of the cross-
correlation Hurst exponent for the HRV and brain
microwave radiation signals for patient S.V.I.
Time window
20-30, sec
30-40, sec
60-70, sec
Before
-0,14729
-0,25288
-0,05091
After
-0,03984
-0,02991
-0,08195
The data presented in the Table 8 show that this
support of patient in the clinical observation of the
results and gave an explanation concerning the
difficulties to achieve a therapeutic effect. The patient
showed the initial expression violations of the
correlation between process of the segmental division
modulation of heart rate at rest and during exercise in
time windows. Which primarily reflects the
phenomena of transport of fluid in the brain and is
associated with the processes it neuro-trophic and
neuroplasticity. As it is currently known and shown,
these processes suffer significantly from patients with
depressive disorders (Arnaud and Di, 2016).
Thus, the data of the cross-correlation analysis
coincides with the clinical picture of the disease for
the patient and fits into this particular clinical case.
The data is the basis for predicting the difficulty in
achieving a clinical effect of the DCASNS, which is
associated with a profound impairment of nervous
trophic and neuroplasticity.
3.8 Discussion
The analysis of data presented in Tables 2-8, showed
that the dynamics of cross-correlation differences
Hurst exponent coincides with the clinical data in the
treatment of patients. The coincidence is
representative for the variety of clinical cases, and can
serve as a basis for forecasting and possible
correction of the treatment course of patients.
Obtained in this study estimations are consistent
with results received earlier. In (Kublanov et al.,
2016) it was found, that for the time windows 20–40
and 50–60 seconds in the functional rest and during
the passive orthostatic load, the systematic
discrepancy between the differences of the Hurst
exponent of biomedical signals is minimal for the
healthy patients. For patients suffering from ischemic
stroke prior to the rehabilitation treatment, these
values are greater.
4 CONLUSIONS
The article describes the pilot clinical study of the
brain microwave radiation and HRV signals obtained
by the multichannel Radiophysical complex
MRTHR. Analysis of the HRV and brain microwave
radiation signals, by means of the methods of the
cross-correlation multifractal analysis allowed to
obtain new knowledge about the studied biomedical
signals.
Application of multifractal formalism allowed
proving that at the minimum level of systematic
differences of the HRV and the brain microwave
radiation signals dynamic changes in these signals
occur like. In this case, we can assume that the role of
the autonomic regulation defined by characteristics of
the HRV in the formation of the brain microwave
radiation is high. The proposed approach can be used
to manage the medical process.
Dynamics of the cross-correlation Hurst exponent
differences coincides with the patients’ clinical data.
The treatment effectiveness depends on the duration
of the disease, more amenable to correction processes
arisen recently. Strokes to the three-year history and
were treatable worse.
ACKNOWLEDGEMENTS
The work was supported by Act 211 Government of
the Russian Federation, contract № 02.A03.21.0006.
REFERENCES
Arnaud, K. and Di, N., 2016. Choroid plexus trophic factors
in the developing and adult brain. Frontiers in Biology,
11 (3), 214–221.
Bland, J. M., Altman, D. G., 1986. Statistical methods for

assessing agreement between two methods of clinical
measurement. Lancet, 8476(1), 307-310.
Boakye, P. A., et al., 2016. A critical review of
neurobiological factors involved in the interactions
between chronic pain, depression, and sleep disruption.
Clinical Journal of Pain, 32 (4), 327–336.
Danilov, Y. P., et al., 2015. Non-invasive multi-channel
neuro-stimulators in treatment of the nervous system
disorders. BIODEVICES 2015 - 8th International
Conference on Biomedical Electronics and Devices,
Proceedings; Part of 8th International Joint
Conference on Biomedical Engineering Systems and
Technologie, 1, 88-94.
Deligniers, D., Almurad, Z.M.H., Roume, C., and
Marmelat, V., 2016. Multifractal signatures of
complexity matching. Experimental Brain Research,
234 (10), 2773–2785.
Di, I., Esteban, F. J., Grizzi, F., Klonowski, W., and Martín-
Landrove, M., 2015. Fractals in the neurosciences, part
II: Clinical applications and future perspectives.
Neuroscientist, 21 (1), 30–43.
Fleishman, A. N., 2005. The IV All-Russian Symposium on
Slow Oscillatory Processes in the Human Body and the
II School/Seminar on Nonlinear Dynamics in
Physiology and Medicine. Human Physiology, 32(2),
248-250.
Guyton, A. C. and Hall, J. E., 2011. Textbook of medical
physiology. Saunders Elsevier.
Hurley, L. L. and Tizabi, Y., 2013. Neuroinflammation,
neurodegeneration, and depression. Neurotoxicity
Research, 23 (2), 131–144.
Jeong, J. H., et al., 2016. Group-and home-based cognitive
intervention for patients with mild cognitive
impairment: A randomized controlled trial.
Psychotherapy and Psychosomatics, 85 (4), 198–207.
Kessner, S. S., Bingel, U., and Thomalla, G., 2016.
Somatosensory deficits after stroke: A scoping review.
Topics in Stroke Rehabilitation, 23 (2), 136–146.
Kublanov, V. S., 2013. Microwave radiation as interface to
the brain functional state. Proc. of the International
Conference on Biomedical Electronics and Devices, 6,
318–322.
Kublanov, V. S., Borisov, V. I. , Dolganov, A. Y., 2015.
The interface between the brain microwave radiation
and autonomic nervous system. Annual International
IEEE EMBS Conference on Neural Engineering, 7,
922-925.
Kublanov, V., Borisov, V., Dolganov, A., 2016. Summary
processing of Radiophysical complex MRTHR signals.
BIOSIGNALS 2016 - 9th International Conference on
Bio-Inspired Systems and Signal Processing,
Proceedings; Part of 9th International Joint
Conference on Biomedical Engineering Systems and
Technologies, l, 143-149.
Kublanov, V. S., Petrenko, T.S., Babich, M.V., 2015.
Multi-electrode neurostimulation system for treatment
of cognitive impairments. Presented at the Proceedings
of the Annual International Conference of the IEEE
Engineering in Medicine and Biology Society, EMBS,
2091–2094.
Kublanov, V. S., Sedelnikov, Ju. E., Azin, A.L., and
Syskov, A.M., 2010. The Nature of Fluctuations Own
Electromagnetic Radiation of the Brain. Biomedical
Radioelectronics, 9, 45-54.
Malik M. et al, 1996. Heart rate variability. Standards of
Measurement, Physiological interpretation and clinical
use. Circulation, 93, 1043-1065.
Moskalenko, Yu. E., 1992. Cerebral Circulation,
Cardiovascular Diseases [in Russian]. Meditsina, vol. 1.
Lundborg, G., 2005. Nerve Injury and Repair:
Regeneration, Reconstruction, and Cortical
Remodeling: Second Edition.
Pavlov, A. N., et al., 2016. Characterizing cerebrovascular
dynamics with the wavelet-based multifractal
formalism. Physica A: Statistical Mechanics and its
Applications, 442, 149–155.
Pocock, G., Richards, C. D., 2013. Human Physiology: The
Basis of Medicine. Oxford Core Texts.
Podobnik, B., Stanley, H. E., 2008. Detrended Cross-
Correlation Analysis: A New Method for Analyzing
Two Nonstationary Time Series. Physical Review
Letters, 100, art. no. 084102.
Rial, D., et al., 2016. Depression as a glial-based synaptic
dysfunction. Frontiers in Cellular Neuroscience, 9
(JAN2016), 1–11.
Ringleb, P. A., et al., 2008. Guidelines for Management of
Ischaemic Stroke and Transient Ischaemic Attack 2008.
Cerebrovascular Diseases 25(5), 457-507.
Schmidt, R. F., Thews G., 1989. Human Physiology.
Springer-Verlag. Berlin, Heidelberg, New York.
Stetler, R. A., et al., 2014. Preconditioning provides
neuroprotection in models of CNS disease: Paradigms
and clinical significance. Progress in Neurobiology,
114, 58–83.
Togo, F., et al., 2006. Unique very low-frequency heart rate
variability during deep sleep in humans. Biomedical
Engineering, 53, 28-34.
Varidaki, A., Mohammad, H., and Coffey, E.T., 2016.
Molecular Mechanisms of Depression. In: Systems
Neuroscience in Depression. 143–178.
Whalley, L. J., Staff, R.T., Fox, H.C., and Murray, A.D.,
2016. Cerebral correlates of cognitive reserve.
Psychiatry Research - Neuroimaging, 247, 65–70.
Závodszky, G., Károlyi, G., and Paál, G., 2015. Emerging
fractal patterns in a real 3D cerebral aneurysm. Journal
of Theoretical Biology, 368, 95–101.
