
REAL-TIME INTELLIGENT DECISION SUPPORT IN
INTENSIVE MEDICINE
Filipe Portela, Manuel Santos, Marta Vilas-Boas
Departamento de Sistemas de Informação, Universidade do Minho, Guimarães, Portugal
Fernando Rua, Álvaro Silva
Hospital de Santo António, Porto, Portugal
José Neves
Universidade do Minho, Departamento de Informática, Braga, Portugal
Keywords: Real-time, Knowledge Discovery in Databases, Intensive Care, INTCare, Intelligent Decision Support
Systems.
Abstract: Daily, a great amount of data that is gathered in intensive care units, which makes intensive medicine a very
attractive field for applying knowledge discovery in databases. Previously unknown knowledge can be
extracted from that data in order to create prediction and decision models. The challenge is to perform those
tasks in real-time, in order to assist the doctors in the decision making process. The Data Mining models
should be continuously assessed and optimized, if necessary, to maintain a certain accuracy. In this paper
we present the INTCare system, an intelligent decision support system for intensive medicine and the way it
was adapted to the new requirements. Some preliminary results are analysed and discussed.
1 INTRODUCTION
Intensive care units (ICU) are a particular
environment where a great amount of data related to
the patients’ condition is daily produced and
collected. Physiological variables such as heart rate,
blood pressure, temperature, ventilation and brain
activity are constantly monitored on-line (Mahmoud
2003). Due to the complex condition of critical
patients and the huge amount of data, it can be hard
for physicians to decide about the best procedure to
provide them the best health care possible. The
human factor can lead to errors in the decision
making process; frequently, there is not enough time
to analyze the situation because of stressful
circumstances; furthermore, it is not possible to
continuously analyze and memorize all the data
(Pereira et al. 2007) .
1
The INTCare project is financially supported by FTC
(PTDC/EIA/72819/2006).
Care of the critically ill patients requires fast
acquisition, registering and availability of data
(Gardner et al. 1991). Accordingly, rapid
interpretation of physiological time-series data and
accurate assessment of patient state is crucial to
patient monitoring in critical care. The data analysis
allows supporting decision making through
prediction and decision models. Algorithms that use
Artificial Intelligence (AI) techniques have the
potential to help achieve these tasks, but their
development requires well- annotated patient data
(Ying, Silvers and Randolph 2007, Morik 2003).
We are developing a real-time and situated
intelligent decision support system, called INTCare
1
,
whose main goal is to improve the health care,
allowing the physicians to take a pro-active attitude
in the patients’ best interest (Santos et al. 2006,
Gago et al. 2006).
INTCare is capable of predicting organ failure
probability, the outcome of the patient for the next
hour, as well as the best suited treatment to apply.
44
Portela F., Santos M., Vilas Boas M., Rua F., Silva Á. and Neves J..
REAL-TIME INTELLIGENT DECISION SUPPORT IN INTENSIVE MEDICINE.
DOI: 10.5220/0003098200440050
In Proceedings of the International Conference on Knowledge Management and Information Sharing (KMIS-2010), pages 44-50
ISBN: 978-989-8425-30-0
Copyright
c
2010 SCITEPRESS (Science and Technology Publications, Lda.)

To achieve this, it includes models induced by
means of Data Mining (DM) techniques (Santos et
al. 2006), (Gago and Santos 2008, Gago, Silva and
Santos 2007, Silva et al. 2003, Silva et al. 2004).
This paper is organized as follows. Section 2
presents some background relating to Intelligent
Decision Support Systems (IDSS), Knowledge
Discovery in Databases (KDD) and intensive
medicine. In section 3 it is presented the INTCare
system, focusing on its features, the information
architecture and the latest DM models developed.
Section 4 and 5 conclude this paper, presenting a
discussion, a conclusion and pointing to future work.
2 BACKGROUND
2.1 Intelligent Decision Support
Systems
According to Turban (Turban, Aronson and Liang
2005), a Decision Support System (DSS) is an
interactive, flexible and adaptable information
system, developed to support a problem solution and
to improve the decision making. These systems
usually use AI techniques and are based on
prediction and decision models that analyze a vast
amount of variables to answer a question.
The decision making process can be divided in
five phases: Intelligence, design, choice,
implementation and monitoring (Turban et al. 2005).
Usually it is used in the development of rule based
DSS (Arnott and Pervan 2004). However, these DSS
are not adaptable to the environment in which they
operate. To address this fault, Michalewicz
(Michalewicz et al. 2007) introduced the concept of
Adaptive Business Intelligence (ABI). The main
difference between this and a regular DSS is that it
includes optimization that enables adaptability. An
ABI system can be defined as “the discipline of
using prediction and optimization techniques to
build self-learning decisioning systems. ABI
systems include elements of data mining, predictive
modelling, forecasting, optimization, and
adaptability, and are used to make better decisions.”
(Michalewicz et al. 2007).
As it is known, predictive models’ performance
tends to degrade over time, so it is advantageous to
include model re-evaluating on a regular basis so as
to identify loss of accuracy (Gago and Santos 2008)
and enable their optimization.
There is a particular type of DSS, the real-time
DSS. Ideally, the later includes adaptive behaviour,
supporting the decision making in real-time.
To achieve real-time DSS, there is a need for a
continuous data monitoring and acquisition systems.
It should also be able to update the models in real
time without human intervention (Santos et al.
2006). In medicine, most systems only use data
monitoring to support its activities, without
predictive behaviour and with poor integration with
other clinical information.
2.2 Knowledge Discovery
from Databases
KDD is one of the approaches used in Business
Intelligence (BI). According to Negash (Negash and
Gray), BI systems combine data gathering, data
storage, and knowledge management with analytical
tools to present complex and competitive
information to planners and decision makers. KDD
is an interactive and nontrivial process of extracting
implicit and previously unknown and potentially
useful and understandable information from data
(Frawley, Piatetsky-Shapiro and Matheus 1992).
The KDD process is divided in 5 steps:
Selection, pre-processing, transformation, data
mining and interpretation/evaluation (Fayyad,
Piatetsky-Shapiro and Smyth 1996). This process
starts with raw data and ends with knowledge.
The automation of the knowledge acquisition
process is desirable and it is achieved by using
methods of several areas of expertise, like machine
learning (Gago et al.). The knowledge acquisition
takes advantage of KDD techniques, simplifying the
process of decision support (Gago and Santos).
Knowledge discovery is a priority, constantly
demanding for new, better suited efforts. Systems or
tools capable of dealing with the steadily growing
amount of data presented by information system, are
in order (Lourenco and Belo 2003).
2.3 Intensive Medicine
Intensive medicine can be defined as a
multidisciplinary field of the medical sciences that
deals with prevention, diagnosis and treatment of
acute situations potentially reversible, in patients
with failure of one or more vital functions (Silva
2007). These can be grouped into six organic
systems: Liver, respiratory, cardiovascular,
coagulation, central nervous and renal (Hall,
Schmidt and Wood 2005).
ICU are hospital services whose main goal is to
provide health care to patients in critical situations
and whose survival depends on the intensive care
(Ramon et al. 2007), (Rao and T. 2003). In the ICU,
REAL-TIME INTELLIGENT DECISION SUPPORT IN INTENSIVE MEDICINE
45

the patients’ vital signs are continuously monitored
and their vital functions can be supported by
medication or mechanical devices, until the patient
is able to do it autonomously (Ramon et al. 2007).
Clinical intervention is based on the degree of
severity scores like the SOFA (Sequential Organ
Failure Assessment) score, that allow the evaluation
of the patient’s condition according to a predefined
set of values (Vincent et al. 1996).
The assessment of these severity scores are based
on several medical data acquired from bedside
monitors, lab results and clinical records.
2.4 Real-time
A system that aims to support decision making must
analyze many parameters and output in short real-
time and consider online monitoring (Morik,
Brockhausen and Joachims). It is known that in the
ICU setting, there is a huge amount of noisy, high
dimensional numerical time series data describing
patients. Consequently, such systems must go
beyond classical medical knowledge acquisition,
since they have to handle with high dimensional data
in real-time.
Data acquisition in real-time implies the need for
a system responsible for collecting the relevant data
to the DSS. This process can be divided in two
phases: monitoring and acquisition and storage.
Initially, the required data (variables) for the project
is identified for further being monitored by sensors
or other technology. Subsequently, data is acquired
and stored in DB. This is a critical phase, for
technical, human and environment factors are
involved and may condition the quality of the data
acquired by a gateway, for example, and its storage
on a DB. Usually, the monitoring is continuous and
there is a small percentage of failures. Although they
may occur, they are relatively easy to correct. The
biggest problem occurs in the communication
between the monitoring system and the storage
system.
In conclusion, monitoring in real-time is relatively
easy; usually, problems arise in the data storage
process.
3 THE INTCARE SYSTEM
INTCare is an IDSS for intensive medicine that is
being developed in the ICU of the Hospital Santo
António (HSA) in Porto, Portugal. It makes use of
intelligent agents (M. F. Santos M.F.) (Abelha et al.)
that are capable of autonomous actions in order to
meet its goals (Gago et al. 2006), (Jennings 2000).
3.1 System Features
In order to model the information for KDD
processing, the system attends some requirements:
Online Learning. The system acts online, i.e., the
DM models are induced using online data in
opposition of an offline approach, where the data is
gathered and processed afterwards;
Real-time. The system actuates in real-time, for the
data acquisition and storing is made immediately
after the events take place to allow that decisions are
taken whenever an event
occurs;
Adaptability. The system has the ability to,
automatically, optimize the models with new data
when needed. This information is obtained from
their evaluation results;
Data Mining Models. The success of IDSS
depends, among others, on the acuity of the DM
models, i.e., the prediction models must be reliable.
These models make it possible to predict events and
avert some clinical complications to the patients;
Decision Models. The achievement of the best
solutions depend heavily on the decision models
created. Those are based in factors like
differentiation and decision that are applied on
prediction models and can help the doctors to choose
the better solution on the decision making process;
Optimization. The DM models are optimized over
time. With this, their algorithms are in continuous
training so that increasingly accurate and reliable
solutions are returned, improving the models acuity;
Intelligent Agents. This type of agents makes the
system work through autonomous actions that
execute some essential tasks. Those tasks support
some modules of the system: Data acquisition, data
entry, knowledge management, inference and
interface. The flexibility and efficiency of this kind
of system emerges from the intelligent agents and
their interaction (Gago et al. 2006).
In order to accomplish these features, the system
has some requirements:
• Fault tolerance capacities;
• Processing to remove null and noisy data;
• Continuous data acquisition process;
• Time restrictions for the data acquisition and
storage;
• Online learning mode;
KMIS 2010 - International Conference on Knowledge Management and Information Sharing
46
• Digital data archive in order to promote the
dematerialization of paper based processes (e.g.,
nursing records);
• Database extension to accommodate the data
structures;
• Correct usage of the equipment that collects the
vital signs.
3.2 Information Architecture
Patient management is supported by complex
information systems, which brings the need for
integration of the various types and sources of data
(Fonseca, Ribeiro and Granja 2009).
In order to follow the requirements enumerated
above, an information model was drawn, regarding
the data acquisition module which includes three
types of information sources:
• Bedside Monitors (BM);
• Lab Results (LR); and
• Electronic Nursing Records (ENR).
All sources can produce information to the system
and that information can be used to develop
predicting models in Intensive Care (knowledge).
The development of an automated information
system for ICU has to be in harmony with the whole
information system and activities within the unit and
the hospital (Fonseca et al. 2009).
The first type of sources relates to data
acquisition from BM. This acquisition is in real-
time, the data is received by a gateway, and it is
stored on a DB table by an agent. Automatic
acquisition eliminates transcription errors, improves
the quality of records and allows the assembly of
large electronic archives of vital sign data (Fonseca
et al. 2009)
The second type of sources (LR) is the one that
contains the less frequent observations, because the
patient normally does this type of clinical analysis
once or twice per day, except in extraordinary
situations. With this method we can collect the data
related with some clinical analysis, such as: number
of blood platelets, creatinine, billirubin, SOFA
scores, partial pressure of oxygen in arterial blood
and fraction of inspired oxygen.
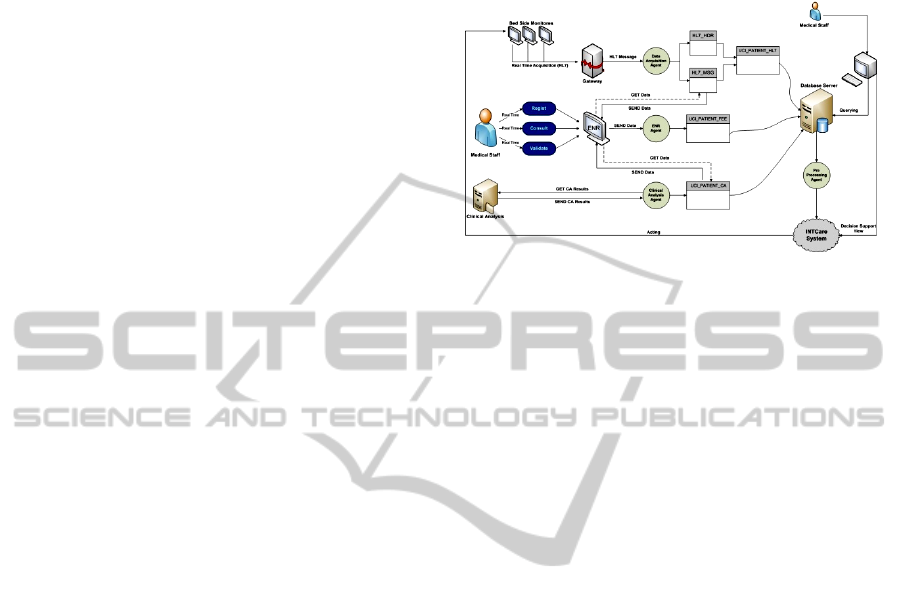
3.3 INTCare Sub-systems
Functionality
The INTCare System (Gago et al. 2006, Santos et al.
2006) is divided into five subsystems, represented in
Figure 1: data acquisition, data entry, knowledge
management, inference and interface. Figure 1
shows a model that is a part of INTCare system and
represents an evolution of two subsystems: data
acquisition and data entry.
Figure 1: The INTCare system.
This subsystem is responsible for all activities of
data acquisition and data store and will gather all
required data into a data warehouse (Santos M.F.
and J. 2009, Santos 2009, Santos et al. 2009). The
evolution of this architecture is prominent.
Formerly, most of the data was registered in paper
format, and it was necessary to manually put it in
electronic format, i.e., the information was rarely
stored in computers, except the information from the
BM, which was automatically collected and stored
in electronic format.
The new architecture (Santos M.F. and J. 2009,
Santos 2009, Santos et al. 2009) contemplates the
data acquisition from three sources and, regarding
the information input, it is done either automatically
(BM, LR) or automatically and manually (nursing
records). The adjustment made to the system was the
addition of one more data source and the creation of
two more agents that enable storing information in
the database (DB).
This modification is in course and it is the most
important, because it makes possible the data
acquisition in electronic and automatic mode for all
data sources through multi-agent system. Whit this
change, we will have all the necessary information
in electronic format for the DM models and the
decision support process, addressing the timing
requirements of critical tasks.
How These Subsystems Work. The first type of
data sources is the BM, which collects the patients’
vital signs (VS). The gateway is connected to the
monitors, reads the information and stores it on a
DB through the data acquisition agent. This agent
splits a HL7 (Hooda, Dogdu and Sunderraman)
message in two, one with the header information and
another with patient data. The second source is the
ENR (Santos M.F. and J. 2009). It was developed
with the objective of registering electronically the
REAL-TIME INTELLIGENT DECISION SUPPORT IN INTENSIVE MEDICINE
47
paper-based nursing records. With the ENR, the
medical and nursing staff can register various types
of data, like confirming if some therapeutic was
performed or not, and they may consult all the
present and past data about the patients. The last
type of data sources is the LR, which is controlled
by the clinical analyses agent that automatically
stores all the LB from the patients.
All the data is stored in one DB and it can be
accessed by the medical staff through a computer.
The integrated data will be used by the INTCare
system to create prevision and decision models.
The DM agent belongs to the sub-system
knowledge management and it is in charge of
retrieving the required data to feed the DM models
and to train new models whenever their performance
becomes unsatisfactory.
3.4 Data Mining Models
3.4.1 Data Description
The data used to generate the DM models originates
from three distributed and heterogeneous sources:
LR, BM and paper-based nursing records, presented
and explained previously. Additionally, variables
containing the case mix (information that remains
unchanged during the patient’s stay - age, admission
from, admission type) were also considered. It was
also included some calculated variables: Critical
Events (CE), SOFA scores and a set of ratios
relating the previous variables to the patients’ length
of stay. The data was gathered in the ICU of HSA
and it was collected in the first five days of stay of
thirty two patients. The construction of the dataset
was not automatically, the data from the LB and
nursing records was manually registered, for the new
adjustments of the system regarding the data
acquisition and data entry were not developed at the
time the models were generated
3.4.2 Features Selection
For the prediction of the dysfunction/failure of each
organic system and outcome, three scenarios were
explored regarding the inclusion of the variables
mentioned above – M1, M2, and M3 – where
M1 = {Hour, Case Mix, CE}
M2 = {Hour, Case Mix, CE, Ratios}
M3 = {Hour, Case Mix, CE, SOFA}.
For each model, the techniques applied were
Artificial Neural Networks, Decision Trees,
Regression and Ensemble methods.
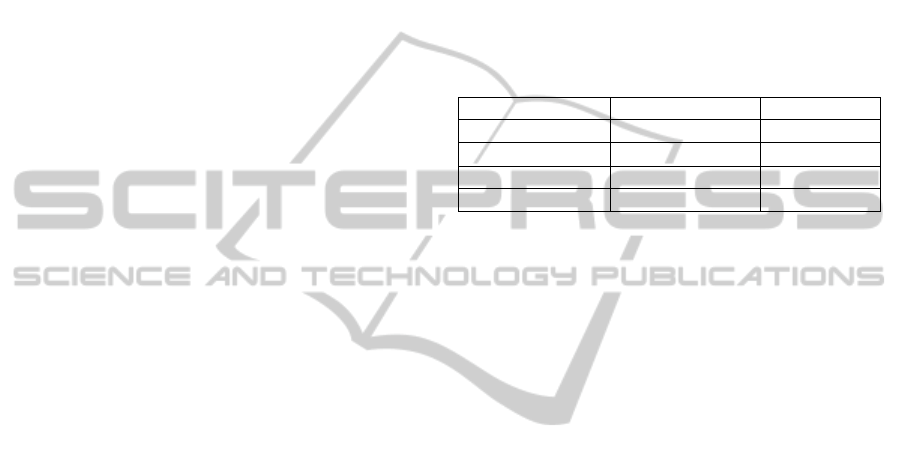
3.4.3 Results
Table 1 shows the best results achieved for
cardiovascular, respiratory, renal, liver, coagulation
and neurological systems and outcome in terms of
sensibility (i.e. percentage of failure and death
correctly classified as such) as well as the scenario
that produced the best results. The models were
developed for hourly prediction with the intent to
make predictions as fast as possible, in the patients
best interest.
Table 1: Sensibility of the DM models by system and
outcome.
System Sensibility (%) Scenario
Cardiovascular 93.4 M3
Respiratory 96.2 M2
Renal 98.1 M3
Coagulation 97.5 M2
4 DISCUSSION
In this paper we presented the INTCare system,
which is an IDSS for intensive medicine. It relies on
the KDD process and AI algorithms to apply DM
techniques for predicting outcomes that might
support the course of action of doctors’ decision.
Relying on intelligent agents, the system in divided
into five sub-systems (data acquisition, data entry,
knowledge management, inference and interface)
that guarantee its functionality.
Since its beginning, INTCare has evolved towards
using real-time and online clinical data so that the
predictions can be as accurate and as soon as
possible. As an IDSS, INTCare uses continuous data
monitoring and acquisition systems that make
possible for all information being available at the
right time. This allows doctors to have a proactive
attitude in patients’ care.
The development of an ENR allows the integration
of all necessary information regarding the patients’
condition to be collected and integrated in just one
application, which is a great gain in time and
performance for the medical staff operating in the
ICU. In addition to the patients’ vital signs, data
regarding their LR, procedures, medication, is also
available by the time it is generated.
Moreover, the INTCare system is designed to
address know issues of the ICU setting, such as
noisy, high dimensional numerical time series data
in real-time (Morik et al.), as well as the data
KMIS 2010 - International Conference on Knowledge Management and Information Sharing
48

acquisition in real-time, storage, integration and
rapid availability of all clinical information.
5 CONCLUSIONS AND FUTURE
WORK
The main concern in ICU is to avoid or reverse
organ failure, in order to preserve the patients’ lives.
The INTCare system is being developed for hourly
prediction of the patients’ clinical condition, i.e. the
prediction of dysfunction/failure of the organ
systems (cardiovascular, respiratory, renal,
coagulation and liver systems) and outcome. We
believe that, with this fine grained prediction, it will
be possible for the healthcare professionals to have a
timely intervention and a proactive attitude so that
worst complications for the patients may be avoided.
Further work will encompass the test of the DM
models generated so far, with online and real-time
data from the ICU of HSA, in order to guarantee
their accuracy or, in case their performance decays,
to optimize them. The models presented used data
manually entered and the next step is to use them
with the new adjustments of the system, i.e., online
and in real-time. Prediction, optimization and
adaptability are features that make INTCare an ABI
system, whose maid goal it to allow the medical
staff to make better decisions, at the right time and
place, improving quality in health care.
The integration with the various data sources and
with the rest information systems of the hospital has
been supported by the development of an ENR and
further related work include its test in the ICU and
subsequently, its optimization.
REFERENCES
Abelha, A., J. Machado, M. Santos, S. Allegro, F. Rua, M.
Paiva & J. Neves. Agency for Integration, Diffusion
and Archive of Medical Information.
Arnott, D. & G. Pervan. 2004. A critical analysis of
decision support systems research. In Conference on
Decision Support Systems, 67-87. Prato, ITALY:
Palgrave Publishers Ltd.
Fayyad, U. M., G. Piatetsky-Shapiro & P. Smyth (1996)
From data mining to knowledge discovery: an
overview.
Fonseca, T., C. Ribeiro & C. Granja (2009) Vital Signs in
Intensive Care: Automatic Acquisition and
Consolidation into Electronic Patient Records. Journal
of Medical Systems, 33, 47-57.
Frawley, W. J., G. Piatetsky-Shapiro & C. J. Matheus
(1992) Knowledge Discovery in Databases: An
Overview. AI Magazine, 13, 57-70.
Gago, P. & M. F. Santos. 2008. Towards an Intelligent
Decision Support System for Intensive Care Units. In
18th European Conference on Artificial Intelligence.
Greece.
Gago, P., M. F. Santos, Á. Silva, P. Cortez, J. Neves & L.
Gomes (2006) INTCare: a knowledge discovery based
intelligent decision support system for intensive care
medicine. Journal of Decision Systems.
Gago, P., A. Silva & M. F. Santos. 2007. Adaptive
decision support for intensive care. In 13th Portuguese
Conference on Artificial Intelligence, ed. J. S. M. F.
M. J. M. Neves, 415-425. Guimaraes, PORTUGAL:
Springer-Verlag Berlin.
Gardner, R. M., W. L. Hawley, T. D. East, T. A. Oniki &
H. F. W. Young (1991) Real time data acquisition:
recommendations for the Medical Information Bus
(MIB). International journal of clinical monitoring
and computing, 8, 251-258.
Hall, J. B., G. A. Schmidt & L. D. H. Wood. 2005.
Principles of Critical Care. McGraw-Hill's
AccessMedicine.
Hooda, J. S., E. Dogdu & R. Sunderraman. Health Level-7
compliant clinical patient records system. 259-263.
ACM.
Jennings, N. R. (2000) On agent-based software
engineering. Artificial Intelligence, 117, 277-296.
Lourenco, A. & O. Belo (2003) Promoting agent-based
knowledge discovery in medical intensive care units.
WSEAS Transactions on Computers, 2, 403-408.
M. F. Santos M.F., V.-B. M., Machado and A. A. J.,
Neves J., Silva A., Rua F., Salazar M., Quintas C.,
Cabral A.F. Intelligent Decision Support in Intensive
Care Units - Nursing Information Requirements.
Mahmoud, M. 2003. Real-time data acquisition system for
monitoring patients in intensive care unit., 320-326.
Multisensor, Multisource Information Fusion:
Architectures, Algorithms and Applications.
Michalewicz, Z., M. Schmidt, M. Michalewicz & C.
Chiriac. 2007. Adaptive Business Intelligence
.
Springer.
Morik, K. (2003) Data analysis and knowledge validation
in intensive care monitoring.
Morik, K., P. Brockhausen & T. Joachims. Combining
statistical learning with a knowledge-based approach-a
case study in intensive care monitoring. 268-277.
Citeseer.
Negash, S. & P. Gray Business intelligence. Handbook on
Decision Support Systems 2, 175-193.
Pereira, M., A. Curra, R. Rivas, J. Pereira, G. Banos, J.
Teueiro & A. Pazos (2007) Computer aided
monitoring system of intensive care unit patients.
WSEAS Transactions on Information Science and
Applications, 4, 78-84.
Ramon, J., D. Fierens, F. Güiza, G. Meyfroidt, H.
Blockeel, M. Bruynooghe & G. Van Den Berghe
(2007) Mining data from intensive care patients.
Advanced Engineering Informatics, 21, 243-256.
REAL-TIME INTELLIGENT DECISION SUPPORT IN INTENSIVE MEDICINE
49

Rao, S. M. & S. T. (2003) Organization of intensive care
unit and predicting outcome of critical illness. Indian
J. Anaesth, 47 (5), 328-337.
Santos M.F., P. F., Vilas-Boas M., Machado & A. A. J.,
Neves J., Silva A., Rua F., Salazar M., Quintas C.,
Cabral A.F.,. 2009. Intelligent Decision Support in
Intensive Care Units - Nursing Information
Requirements. In WSEAS Transactions on
INFORMATICS, ed. Springer.
Santos, M. F., P. Cortez, P. Gago, Á. Silva & F. Rua.
2006. Intelligent decision support in Intensive Care
Medicine. In 2nd International Conference on
Knowledge Engineering and Decision Support, 401-
405. Lisbon, Portugal.
Santos, M. F., F. Portela, M. Vilas-Boas, J. Machado, A.
Abelha, J. Neves, A. Silva & F. Rua. 2009.
Information Modeling for Real-Time Decision
Support in Intensive Medicine. In Proceedings of the
8th Wseas International Conference on Applied
Computer and Applied Computational Science -
Applied Computer and Applied Computational
Science, eds. S. Y. Chen & Q. Li, 360-365. Athens:
World Scientific and Engineering Acad and Soc.
Santos, M. F., Portela, F., Vilas-Boas, M., Machado, J.,
Abelha, A., Neves, J. 2009. Information Architecture
for Intelligent Decision Support in Intensive Medicine.
In 8th WSEAS International Conference on APPLIED
COMPUTER & APPLIED COMPUTATIONAL
SCIENCE (ACACOS '09). Hangzhou, China,:
WSEAS.
Silva, A. 2007. Modelos de Inteligência Artificial na
análise da monitorização de eventos clínicos adversos,
Disfunção/Falência de órgãos e prognóstico do doente
critico. Tese de doutoramento, ciências médicas,
universidade do Porto.
Silva, Á., P. Cortez, M. F. Santos, L. Gomes & J. Neves.
2004. Multiple organ failure diagnosis using adverse
events and neural networks. In 6 th International
Conference on Enterprise Information Systems, 401-
408. Springer.
Silva, Á., J. Pereira, M. Santos, L. Gomes & J. Neves.
2003. Organ failure prediction based on clinical
adverse events: a cluster model approach. 3th
International Conference on Artificial Intelligence and
Applications: ACTA Press.
Turban, E., J. E. Aronson & T.-P. Liang. 2005. Decision
Support Systems and Intelligent Systems. Prentice
Hall.
Vincent, J. L., R. Moreno, J. Takala, S. Willatts, A. De
Mendonca, H. Bruining, C. K. Reinhart, P. M. Suter &
L. G. Thijs (1996) The SOFA (Sepsis-related Organ
Failure Assessment) score to describe organ
dysfunction/failure. Intensive care medicine, 22, 707-
710.
Ying, Z., C. T. Silvers & A. G. Randolph. 2007. Real-
Time Evaluation of Patient Monitoring Algorithms for
Critical Care at the Bedside. In Engineering in
Medicine and Biology Society, 2007. EMBS 2007.
29th Annual International Conference of the IEEE,
2783-2786.
KMIS 2010 - International Conference on Knowledge Management and Information Sharing
50
