
Cross Examination of Atenolol and Canderstan Cilexetil on the
Treatment of Hypertension
Mingxuan Yang
BASIS International School Shenzhen, Shenzhen, Guangdong, 518067, China
Keywords: Hypertension (HTN), Atenolol, Canderstan Cilexetil/Canderstan, Beta-1 Adrenergic Receptor, Angiotensin
II Receptor (Type-1).
Abstract:
Hypertension is a serious medical condition that has led to approximately a total of 7.6 million deaths annually
throughout the globe. In retrospect of the entire medical history, many drugs had been used for the treatment
of hypertension, but none had presented a consummate solution that could eradicate or prevent hypertension
previously at all. Nowadays, with the fast-developing medical industries, people can gain access to more
medications targeting hypertension with a far wider range of scope and through more convenient facilitations.
Drugs such as atenolol and canderstan cilexetil had furthermore also became some of the most popular drugs
used to treat high blood pressure with the precondition of a prospering modern medical market. In order to
resolve one of the most difficult medical problems that hovered through the entire human history until now,
it is essentially necessary to understand what is the best equipment that can defeat the abhorrent enemy in the
entire medical field----hypertension.
1 INTRODUCTION
Hypertension (HTN), commonly known as high
blood pressure (HBP) by the public, is often
considered as one of the most dreadful causes of
cardiovascular dysfunction as it induces to
approximately 54% of all stroke diagnoses and 47%
of all coronary heart diseases discovered world-
widely (
J;, A. H. B. F. C, 2011)
. As the culprit
contributing to a total of 7.6 million deaths annually
throughout the globe, HTN has the highest mortality
rate in comparison to any other risk factors for
cardiovascular diseases or kidney failures (
J;, A. H.
B. F. C, 2011)
. Overall, 80% of diagnoses for HTN
were found in low- and middle-income countries (
J;,
A. H. B. F. C, 2011)
, making it a great struggle
related to poverty and population aging also since the
population of age 69 and older would have the
possibility to be diagnosed with HTN with a 50%
chance, much higher in comparison to a 38% for the
younger age group (
GL;, O. R. V. B. (n.d.)
. As
partially shown in Table 1, in China, an average of
23.2% of the adult population during 2012-2015 was
diagnosed with HTN, while another 41.3% of the
entire Chinese adult group were discovered to have
symptoms indicating pre-HTN, demonstrating a high
prevalence for HTN in China and throughout the
globe (
Wang, 2018)
.
Table 1: Trend of hypertension prevalence in Chinese adults from year 2007-2015 [3-4].
Years 2007 2009 2010 2011 2013 2015
Prevalence (%) of HTN in Chinese adult
population
26.6 29.6 33.5 22.8 24.5 37.2
According to the American College of
Cardiology/American Heart Association Guideline
for the Prevention, Detection, Evaluation, and the
Management of High Blood Pressure in Adults,
systolic HTN is confirmed once one’s blood pressure
has reached 130 mm Hg or higher, while diastolic
HTN would be confirmed once the patient’s blood
level has reached 80 mm Hg or higher (
Whelton,
2017)
. Patients diagnosed with HTN were often
found to be accompanied by symptoms including
extensive nose bleeding, dizziness, or shortness of
breath when their blood pressure has reached a high
life-threatening stage while demonstrating minor or
no symptoms during normal-day activities (
Mayo
Yang, M.
Cross Examination of Atenolol and Canderstan Cilexetil on the Treatment of Hypertension.
DOI: 10.5220/0011381300003443
In Proceedings of the 4th International Conference on Biomedical Engineering and Bioinformatics (ICBEB 2022), pages 1153-1163
ISBN: 978-989-758-595-1
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
1153
Foundation for Medical Education and Research,
2021)
. Although the essential etiology about a single
trigger causing HTN still remains to be unclear, a
lack of strong blood circulation, weakening of blood
vessel contraction, and an excessive force damaging
the internal structures of the blood vascular system
could all be the calmative causes for HTN
accompanied by external conditions especially
related to old age or bad physical circumstances (diet,
environment, etc.) (
Mayo Foundation for Medical
Education and Research, 2021)
.
Drugs such as Atenolol and Canderstan Cilexetil
acting as essential blockers had been commonly used
to treat HTN throughout the history of modern
medicine due to their dominance in the market.
Atenolol, a Beta-1 cardio-selective adreno-receptor
blocker (
Mayo Foundation for Medical Education
and Research, 2021)
, was originally developed by
the Imperial Chemical Industries (ICI) in 1976 and
has been approved by the public in 1981 in America
due to its effectiveness and safety as an anti-
hypertensive drug in its previous clinical trials
(
https://en.citizendium.org/wiki/National_Library
_of_Medicine.)
. Canderstan Cilexetil, an
angiotensin-receptor blocking agent treating HTN,
registered by its brand name as Atacand in the public,
was developed by the corporation Takeda in the
Medical field on the other hand with a more different
mechanism than Atenolol on a pharmaceutical scale
(
Candesartan Cilexetil)
. Overall, these two drugs
had all demonstrated their efficiency in treating
HTN.
In this literature review, these two most dominant
drugs in the medical market, atenolol and canderstan
cilexetil, will be cross-examined based on their
chemical properties, mechanism of action, and
modes of delivery from both a therapeutical and
economic standpoint in order to search for the most
optimal solution on the treatment of hypertension.
2
DESCRIPTION OF CHEMICAL
STRUCTURES OF DRUGS
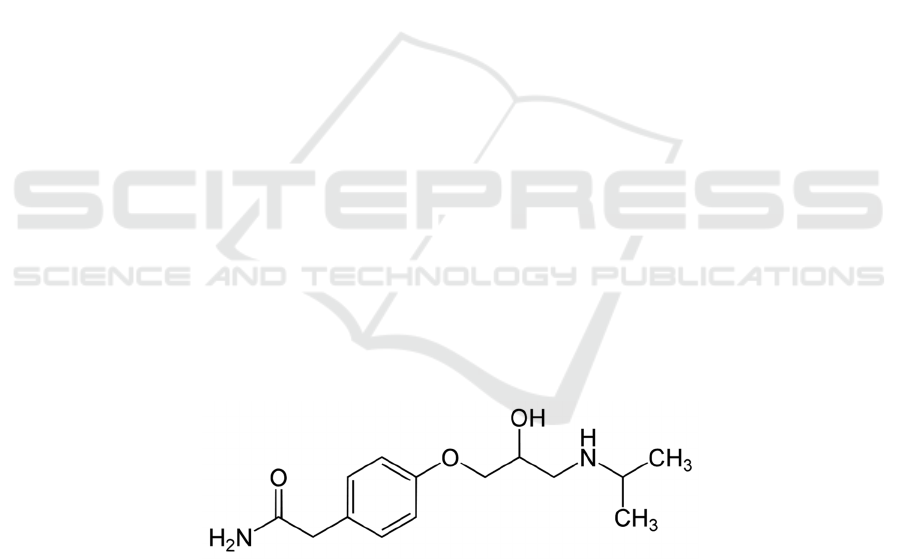
2.1 Atenolol (Generic Name)
Atenolol, commonly recognized by its brand name as
Tenoretic or Tenormin
(
https://pubchem.ncbi.nlm.nih.gov/compound/ate
nolol)
, has a molar mass of 266.336 g·mol−1 and is
solid in the form as white crystalline powder under
room temperature (
Libretexts, 2020);
(https://www.chem960.com/cas/29122687/)
. As
shown in Figure 1, Atenolol has a chemical
composition of C14H22N2O3
(
https://pubchem.ncbi.nlm.nih.gov/#query=C14H
22N2O3)
, and its IUPAC name is 2-(4-{2-hydroxy-
3-[(propan-2-yl) amino] propoxy} phenyl)
acetamide
(
https://pubchem.ncbi.nlm.nih.gov/compound/An
giotensin-II#section=Biologic-Description)
. On
the behalf of its chemical properties, Atenolol has an
approximate melting point ranging from 146-148°C
along with a pka value of 9.6 in its internal structure
(
https://go.drugbank.com/drugs/DB00335);
(Karaman, 2016)
. As a chemical substance that is
highly soluble in liquid including methanol and
hydrochloric acid, Atenolol also possesses a
solubility of 13300 mg/L at the temperature of 25°C
(
https://pubchem.ncbi.nlm.nih.gov/compound/ate
nolol#section=Solubility)
.
Figure 1: Chemical structure of Atenolol.
2.2 Canderstan Cilexetil (Generic
Name)
Canderstan Cilexetil, registered as Atacand as its
public brand name, has a common molar mass of
440.463 g·mol−1 in normal state
(
https://pubchem.ncbi.nlm.nih.gov/compound/Ca
ndesartan-cilexetil)
. As shown in Figure 2,
Canderstan Cilexetil has a chemical structure written
as C33H34N6O6 and was named in the form of
IUPAC nomenclature as 1-{[(cyclohexyloxy)
carbonyl]oxy}ethyl2-ethoxy-1-{[2'-(1H-1,2,3,4-
tetrazol-5-yl)-[1,1'-biphenyl]-4-yl]methyl}-1H-1,3-
benzodiazole-7-carboxylate (
Candesartan Cilexetil,
2021)
. Canderstan also has a strong acidic pka value
of 4.23 and a strong basic pka value of 1.45
(
https://chemaxon.com/products/calculators-and-
predictors#pka.
), along with a water solubility value
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
1154
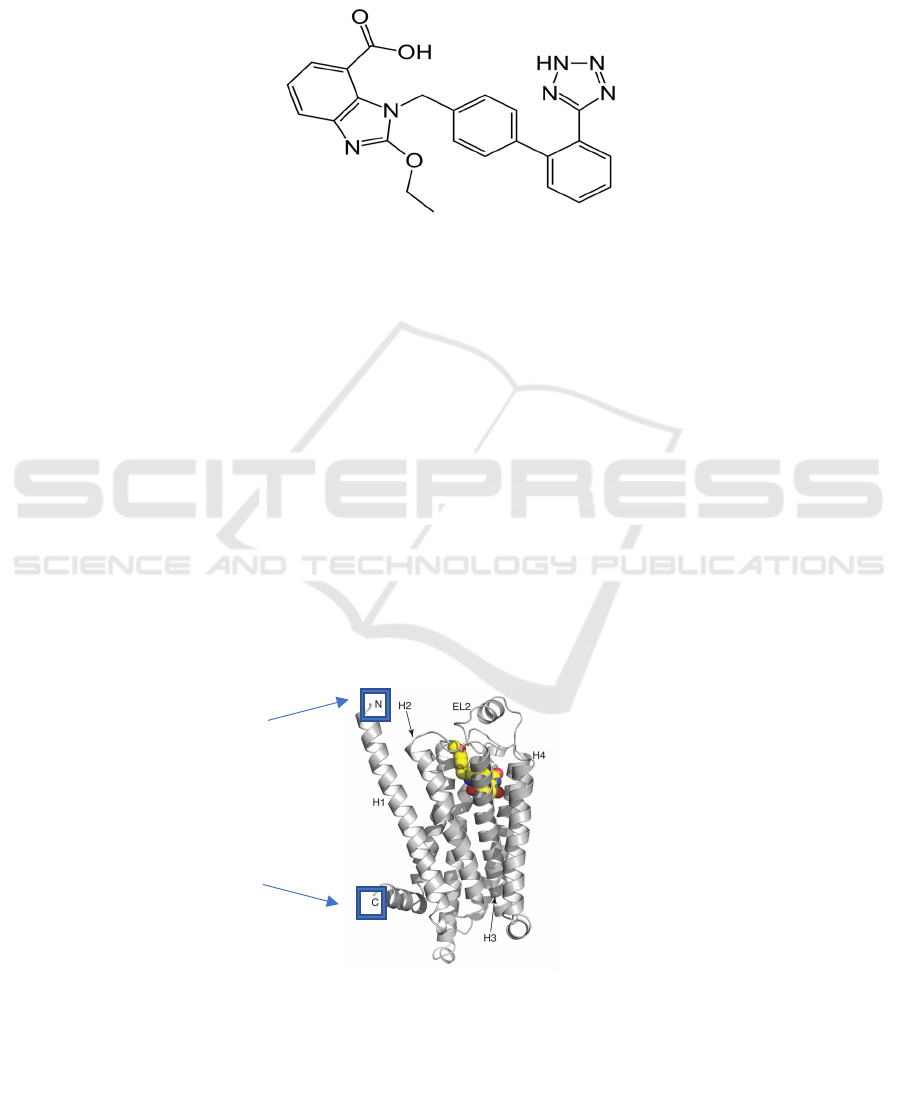
at 0.00204mg/ml under normal condition
(
http://www.vcclab.org/lab/alogps/);
(https://pubmed.ncbi.nlm.nih.gov/11749573/.)
.
Canderstan Cilexetil has a single chiral center at its
cyclohexyloxycarbonyloxy ethyl ester group,
indicating its specific characteristics as a chemical
compound acting as an angiotensin-receptor
blocking agent (
Pharmaceuticals, A. N. I., 2020)
.
Functions of its chemical structure on the behalf of
treating hypertension will be discussed furthermore
in the next section.
Figure 2: Chemical structure of Canderstan Cilexetil.
3
DISCUSSION OF DRUG
PHARMACOLOGY
3.1 Drug Targets Description and
Characteristics
(1) β-1 Adrenergic receptor & its corresponding
hormones
The Beta-1 receptor is a specific adrenergic
receptor primarily found within the body’s heart and
kidney cells (
CV;, A. S. P. (n.d.)
. As a receptor
responsible for the transportation of signals within
the sympathetic nervous system, the Beta-1
adrenergic receptor majorly passes signals through
the Gs alpha subunit that triggers the initiation of a
cAMP-dependent pathway and eventually amplifies
the Beta-1 receptor’s functions within the body
(
CV;, A. S. P. (n.d.)
. With the activation of beta-1
receptors through the cAMP-dependent pathway, the
beta-1 receptors inside the heart can thus perform
their tasks as receptors responsible of increasing the
contractions within the ventricular muscle, sinoatrial
node, and the atrioventricular node that amplify heart
rate and blood pressure in combination (
CV;, A. S.
P. (n.d.); (Steinberg SF)
. Based on its characteristics
to make use of the Gs alpha subunit as passageway,
the structure of Beta-1 receptor is specifically
classified as G protein-coupled receptor (GPCRs)
that has seven transmembrane regions with two
different terminal (N-terminus & C-terminus)
located both on the outside and inside of the cell
(
M.T., P. (n.d.)
.
Figure 3: Structure of the β-1 adrenergic receptor (
https://www.esrf.fr/news/spotlight/spotlight145/index_html).
Description of Figure:
Figure 4 has demonstrated the typical structure of
the Beta-1 receptor (as GPCR) located in heart cells
with labels of its structure: (extracellular N-terminus
& intracellular C-terminus). These receptors often
have the characteristics to be extremely dynamic and
easily conformational between its active state and
inactive state. These characteristics all eventually
Cross Examination of Atenolol and Canderstan Cilexetil on the Treatment of Hypertension
1155
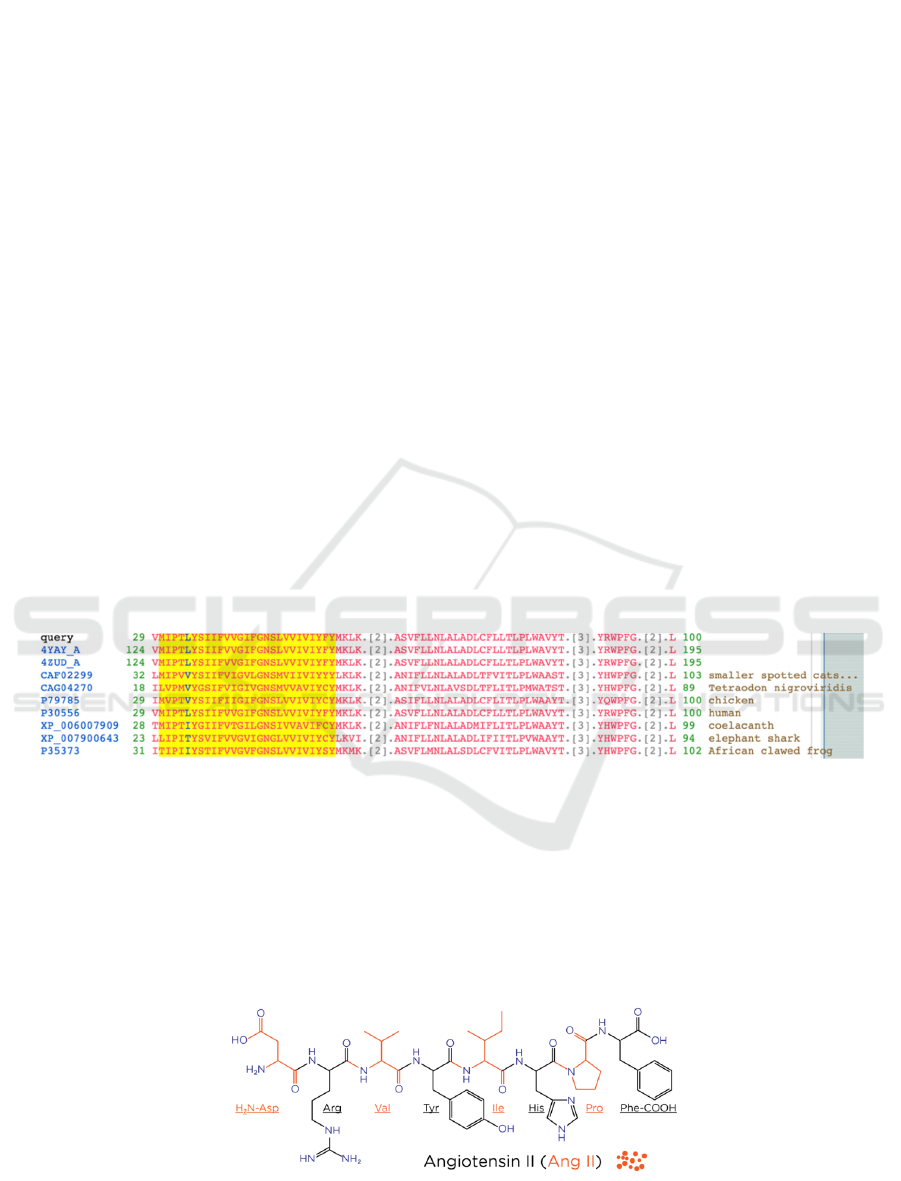
contributes to Beta-1 receptor’s extreme instability
on the performance of its job as a blood pressure
regulator and can easily be disruptive and has high
potential to trigger HTN
(
https://www.esrf.fr/news/spotlight/spotlight145/i
ndex_html.)
. (End of figure description)
A variety of hormones including dopamine,
epinephrine, and norepinephrine can bind to the
Beta-1 receptors within the heart, kidney, and
sympathetic nervous system. While dopamine and
norepinephrine have the affinity to target both Beta-
1 and Beta-2 receptor almost equally, the hormone
epinephrine has demonstrated the strongest affinity
toward the binding to Beta-1 receptor, making it the
most effective hormone in the Beta-1 pathway to
affect blood pressure and muscle contraction
amongst all the other hormones triggering the
activation of beta-1 receptor (
Lennarz, 2013)
.
(2) Angiotensin II (Ang II) & Type 1 (AT1)
Angiotensin II receptor
Angiotensin II (Ang II) is an organic peptide
hormone derived from Angiotensin I in the renin-
angiotensin system (RAAS) that can raise blood
pressure through causing contraction within blood
vessels and increasing sodium concentration within
the kidney (
I;, F. F. M. K. T. (n.d.)
. Thus, once too
much Ang II has accumulated within human organs
or in the RAAS system, it could potentially lead to
serious problems that would trigger HTN. Inside the
cardiovascular vessels, Ang II acts as one of the main
factors having a significant effect in the renin-
angiotensin system that regulates the cardiovascular
metabolism and homeostasis through the pathway of
its type 1 (AT1) and type 2 (AT2) receptors (
I;, F. F.
M. K. T. (n.d.)
.
The human AT1 Ang II receptor is specifically
encoded between the 29
th
to 10
th
position within the
protein sequence P30556, which has the conserved
feature of TM helix 1 that is classified to have a
seven-transmembrane helix domain
(
https://www.ncbi.nlm.nih.gov/Structure/cdd/cd1
5192.); (CDD Conserved Protein Domain Family:
7tmA_AT1R (nih.gov) (database)
). Based on this
domain’s specific function, the AT1 receptor
therefore can perform blood cell proliferation easily
due to its highly transmembrane feature (to pass
essential particles across cellular membrane) which
eventually contributes to the increase in blood
pressure with the multiplication of blood cells
(CDD
Conserved Protein Domain Family: 7tmA_AT1R
(nih.gov) (database)
. Thus, the activation of the
AT1 receptor domain through Ang II has become one
of the most evident features contributing to HTN on
a molecular scale.
Figure 4 Protein Sequences of AT1 Ang II receptor in various animals
(CDD Conserved Protein Domain Family:
7tmA_AT1R (nih.gov) (database).
Description of Figure:
Figure 5 has demonstrated a variety of protein
sequences encoding the AT1 receptor in RAAS
system responsible of receiving Ang II peptide
(CDD Conserved Protein Domain Family:
7tmA_AT1R (nih.gov) (database)
. The query
sequence P30556 represents for the protein sequence
in human that coded for the specific structure of AT1
receptor, while the highlighted yellow regions in all
these sequences represent the feature TM helix 1 in
the AT1 receptor coding sequence
(CDD Conserved
Protein Domain Family: 7tmA_AT1R (nih.gov)
(database)
. (End of figure description)
Figure 5 Chemical structure of Angiotensin II
(CDD Conserved Protein Domain Family: 7tmA_AT1R (nih.gov)
(database).
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
1156
3.2 Drug Effect on Targets Description
(1) Atenolol on β-1 Adrenergic receptor
Atenolol, a beta-1 selective agent, has been
widely used as an antihypertensive drug that
specifically targets the Beta-1 receptor to lower
blood pressure through competing with other
hormones for the binding site (extracellular N-
terminus) on the receptor (
Hasanah, Dwi Utari,
Pratiwi, 2019)
. Through connecting its methyl group
onto the extracellular N-terminus of the beta-1
receptors located in the myocardial regions, atenolol
thus inhibits their action to increase blood pressure
and cardio muscular contraction through producing
inotropic and negative chronotropic activities
(
Hasanah, Dwi Utari, Pratiwi, 2019);
(https://pubchem.ncbi.nlm.nih.gov/source/hsdb/6
526#section=Mechanism-of-Action-(Complete))
.
The negative chronotropic activities initiated by
atenolol within heart tissues such as the sinoatrial
node would eventually decrease the rate of electrical
signal discharges from the sinoatrial node and
gradually lowers heart rate by approximately 25-35%
(https://pubchem.ncbi.nlm.nih.gov/source/hsdb/6
526#section=Mechanism-of-Action-(Complete))
.
Atenolol would also reduce the regular cardiac
output by about 20% through its binding with the
Beta-1 receptor on a secondary position in
comparison to the decrease of heart rate and
myocardial muscular contraction
(https://pubchem.ncbi.nlm.nih.gov/source/hsdb/6
526#section=Mechanism-of-Action-(Complete))
.
Although atenolol trigger could possibly influence
the increase in oxygen requirements through
stimulating left ventricular fiber length to amplify
end-diastolic pressure especially in patients
diagnosed with cardiac failure, it generally would
reduce oxygen consumption through decreasing
myocardial contraction and eventually lead to pain-
relief of muscles in the myocardial region
particularly effective for patients diagnosed with
HTN-related angina pectoris
(https://pubchem.ncbi.nlm.nih.gov/source/hsdb/6
526#section=Mechanism-of-Action-(Complete))
.
A high dosage of the atenolol drug might possibly
lead to sinus arrest within patients in a life-
threatening stage. Moreover, atenolol could also lead
to increase in patient’s stroke index by about 10% as
one of its side-effects
(https://pubchem.ncbi.nlm.nih.gov/source/hsdb/6
526#section=Mechanism-of-Action-(Complete))
.
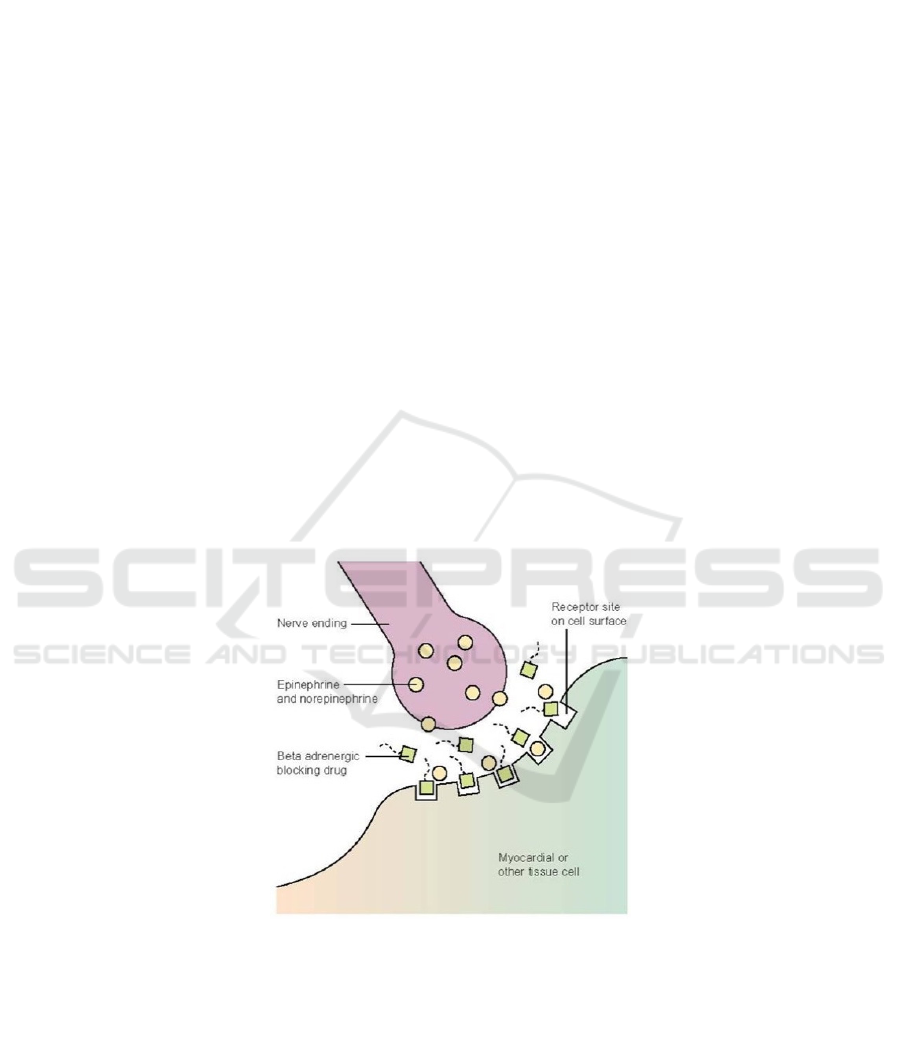
Figure 6: Mechanism of Beta-adrenergic blocking drug (atenolol) binding to receptor site (
http://dxline.info/diseases/beta-
blocker).
Description of Figure:
Figure 7 has demonstrated a simple illustration
for the process of atenolol competition with other
naturally occurring hormones for the binding site of
Beta-1 receptor on myocardial tissue cells. The
atenolol chemicals would reach the receptor site on
cell surface before hormones such as epinephrine or
norepinephrine in the sympathetic nervous system to
alter the receptor’s function with a high affinity
(
http://dxline.info/diseases/beta-blocker.)
. (End of
figure description)
(2) Canderstan Cilexetil on Type 1 (AT1)
Angiotensin II receptor
Canderstan Cilexetil has been commonly used as
an angiotensin-receptor blocker (ARB) medicine for
treating hypertension and many of its related
complications. Canderstan cilexetil, once rapidly
converted into its complete form as Canderstan
Cross Examination of Atenolol and Canderstan Cilexetil on the Treatment of Hypertension
1157

inside the body (see next section for further
details/reasons), will actively seek for AT1 Ang II
receptors and attaches itself onto the target. Once
Canderstan is attached to AT1 receptors, it will
restrain Ang II to connect to these receptors and thus
stops Ang II stimulating the AT1 receptors to
produce aldosterone that could lead to
vasoconstriction through reabsorbing water and
sodium which could eventually lead to HTN if the
pressure exerted by this action (vasoconstriction) is
too high
(
https://go.drugbank.com/drugs/DB11842)
.
In the whole process, as shown in Figure 8,
Canderstan cilexetil acts as an antagonist toward the
renin-angiotensin-aldosterone (RAAS) system that
would selectively competes for binding site with Ang
II and blocks the aldosterone secreting effects and
vasoconstrictor of Ang II in many parts of the human
body including the adrenal gland and vascular
smooth muscle (
Giacchetti G; Opocher G; Sarzani
R; Rappelli A; Mantero F; (n.d.))
. On a closer look,
the adrenal gland discussed in this process would
directly trigger the production of epinephrine within
itself that could furthermore initiates the binding
process to the beta-1 adrenergic receptor and raises
blood pressure if nothing acts to stop the reaction
(
Adrenal glands. Johns Hopkins Medicine. (n.d.))
.
Thus, Canderstan cilexetil’s blockade onto the Ang
II receptor would actually not only help stopping
blood pressure to be raised through processes within
the RAAS system, but it would also help to stop
epinephrine from binding onto the beta-1 receptor in
advance since once AT1 receptors in the adrenal
gland are inactivated, the adrenal gland would also
stop to produce the corresponding chemicals
required in the body. This process furthermore
proves this drug’s high efficiency in stopping HTN
since canderstan could has an effect in both systems
discussed (beta-1 adrenergic & Angiotensin II
receptor) in this specific paper.
Figure 7: Mechanism of angiotensin receptor blocking drug (canderstan) binding to receptor (
Aquarius, 2013).
3.3 Modes of Delivery and Related
Characteristics
(1) Atenolol
The most traditional way of absorbing atenolol
for treating hypertension is most directly related to
oral delivery. It is suggested that for an average adult
diagnosed with hypertension, atenolol should be
taken on an average day with 50-100mg three times
per day for a month’s period (
Choudhary, 2016)
.
Although constantly delivered to patients orally,
the bioavailability of absorbing atenolol through this
mode of delivery has actually been proven to be very
low with only an index of 50% which directly infers
that it would take almost 2 weeks for atenolol to
actually make an effect within the human body after
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
1158
taking it orally. Recently, studies had shown that the
process of transdermal delivery could actually be a
potential alternative to oral absorption since many
clinical studies has all demonstrated that transdermal
delivery of atenolol could actually increase the
therapeutic efficacy for atenolol to be dissolved in
the body. Since atenolol has a relatively high pka
value of 9.6 under normal circumstances, the
dissolution of atenolol within body through
transdermal iontophoresis could possibly be a better
solution than delivering atenolol to patients through
the mouth. Essentially, iontophoresis could reduce
the lag time of medical effect to happen, increase rate
of transportation of atenolol within the body, and
allow better control over the delivery of drugs
(
Ramkanth, 2018); (SM;, M.-D. S. N.-J. M. R. G.
(n.d.)
.
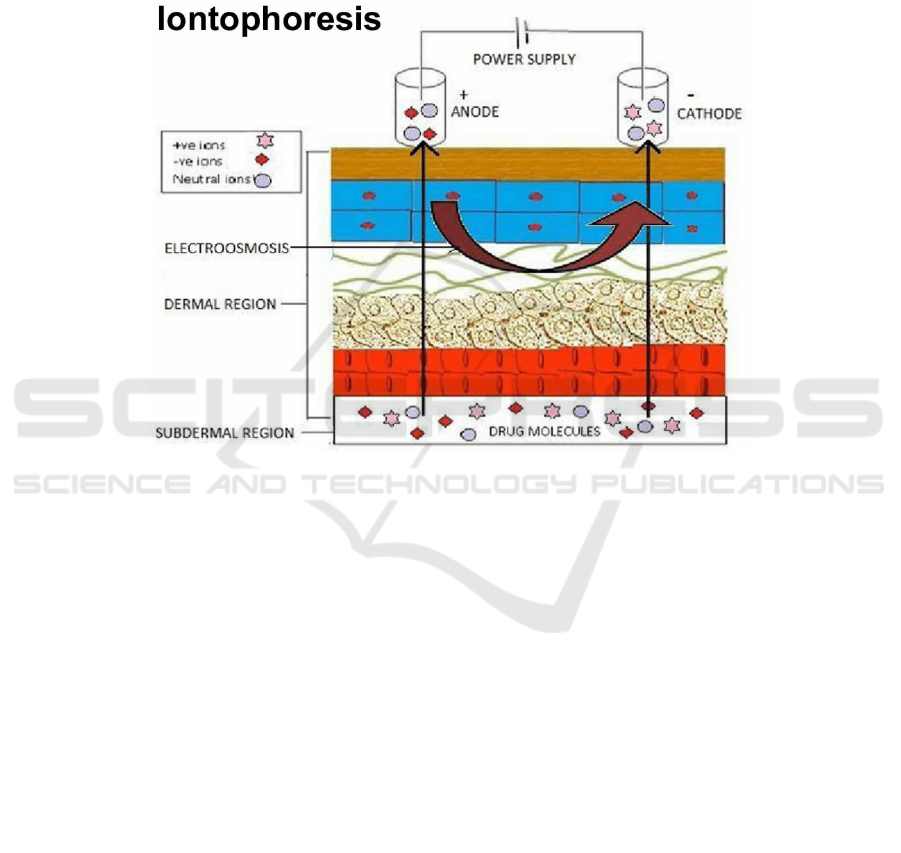
Figure 8: Illustration of Transdermal Iontophoresis (
Team, H. J., & Team, H. J. (2018).
Description of Figure:
Figure 9 has demonstrated a typical illustration
of the mechanism for iontophoresis on the skin
surface. On the surface, a simple battery powered
direct current (DC) has been connected with both the
anode (+ charge) and cathode (- charge) to transport
drug chemicals or macromolecules through the three
layers of the skin into the blood vessels and inner part
of the body through facilitating ions both charged
positively and negatively in the electrical current.
The transportation pathway of the drug particles
directly forms a loophole with the electrical power
supply in this way, giving drugs a faster rate to be
transported with electrical charges (
Team, H. J., &
Team, H. J. (2018)
. (End of figure description)
(2) Canderstan Cilexetil
Before absorbed by patients, canderstan cilexetil
is only a biological inactive compound (prodrug) that
still requires to be converted into its complete form
in order to make an impact to the targeted receptors
within the body. Once orally delivered, canderstan
cilexetil will directly enters the gastrointestinal tract
and become bioactivated through ester hydrolysis,
which will eventually convert canderstan cilexetil
into canderstan---the full selective AT1 receptor
antagonist/blocker. It is said that canderstan could
only be poorly absorbed after delivered to the patient
orally in its complete form, thus the ester prodrug
form of canderstan cilexetil must be prepared in
order to exert the maximum effect to the body as an
organic drug. After canderstan performs its function
inside the body, the drug chemical will mainly be
excreted unchanged outside the body via urine and
feces. The drug chemical would undergo minor
hepatic metabolism into the inactivate metabolite and
thus transport outside body in an approximate time
of 9 hours (roughly the half-life for canderstan). It is
suggested that canderstan cilexetil should be taken
orally per time for a monthly prescription time with
up to a 32 mg since 64% of the canderstan cilexetil
would be excreted outside the body during
absorption the form of feces, so a relatively large
amount of the prodrug is required to be taken in
(
Khawaja, 2011)
.
Cross Examination of Atenolol and Canderstan Cilexetil on the Treatment of Hypertension
1159

4 DISCUSSION OF DRUG
ECONOMICS
4.1 Atenolol
Atenolol was commonly sold in the current medical
market as both an antihypertensive, diuretic, and
anti-angina pectoris drug for customers (
Atenolol /
CHLORTHALIDONE Prices, coupons & savings
tips. GoodRx. (n.d.))
. In the market, Atenolol was
sold by many different pharmaceutical companies
ranging from the cheapest with a price of only $14.83
per prescription for a course of treatment sold by
GoodRx to an average retail price of $33.50 in each
distinct market dominated by different price
elasticity of demand value for medical products
(
Atenolol / CHLORTHALIDONE Prices,
coupons & savings tips. GoodRx. (n.d.))
. The price
elasticity of demand (PED) is a specific economic
index measuring the sensitivity of customer’s
willingness to purchase a specific product in respond
to the change of market price for that product, and in
the case of medical markets related to atenolol as an
inexpensive prescription drug, the PED value is
constantly changing in relationship to the amount of
atenolol products throughout the world, making the
price of atenolol hard to be standardized due to the
constant change in both the economic index and the
different private companies responsible for the
production of atenolol drug (
Price elasticity of
demand - harvard university. (n.d.))
.
4.2 Canderstan Cilexetil
Canderstan Cilexetil was often sold in the public
medical market with a relatively higher price in
comparison with atenolol. The standard GoodRx
price for canderstan cilexetil is around $23.54 per
prescription, and the average retail price for
canderstan cilexetil in the modern market is $90.79,
which is around 74% higher than the GoodRx
standard price. The high price for canderstan cilexetil
thus made it an infamous drug in the hypertension
market as most patient diagnosed with HTN often
lived in a low- and middle-income society where
they cannot afford so much money to purchase an
almost luxurious drug for the normal prescription
treatment (Candesartan prices, coupons & savings
tips. GoodRx. (n.d.).). However, a high price and low
purchase rate does not mean that canderstan cilexetil
has a poor quality over treating HTN. In comparison,
canderstan cilexetil do have a better effect over the
treatment of HTN than atenolol----their comparison
will be discussed furthermore in the next section.
5 DISCUSSION AND
CONCLUSION
From a therapeutical perspective, canderstan cilexetil
has demonstrated a higher efficiency in treating
hypertension than atenolol since it could bind to
receptors located in many different parts of the body
organs including the adrenal gland and smooth
cardiovascular muscle to cease hypertension through
both binding sites, while atenolol could only work to
stop the increase in blood pressure if it is bond to the
correct receptors inside the cardiovascular tissue
through the adrenergic pathway. These two drugs
are, essentially, very similar in their function
mechanism since they both acts as essential blockers
for receptors in order to stop high blood pressure, but
they still are working in two different systems as
atenolol makes its impact. Whereas atenolol
functions in the adrenergic system, canderstan works
in the renin-angiotensin system to stop both
aldosterone and the production of epinephrine to
cease hypertension which also marks one merit of
canderstan cilexetil on the treatment of hypertension
since it could eventually block the production of two
high blood pressure-triggering chemicals, while
atenolol could only stop the production of one
chemical channel in the angiotensin system.
From an economic standpoint, atenolol does
looks to have a better foreground than canderstan.
Whereas Atenolol has a cheaper price (lowest:
$14.83) than canderstan cilexetil (lowest: $23.54), it
also has a wider consumer population throughout the
globe because of its easy-accessibility and wide
production recognized by many medical private
companies. As mentioned previously in this
literature review, hypertensions most commonly
occur in low- and middle-income countries, so many
hypertensions diagnosed patients would actually be
more apt to choose a more inexpensive medicine for
treatment because many of them could not afford to
use such a costly medicine like canderstan cilexetil
to treat their diagnosed condition. Thus, in
conclusion, atenolol and canderstan all have
demonstrated their merits distinctively in the
perspective of pharmacology or in the field of
economy on the behalf of considering for the
treatment of hypertension.
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
1160

REFERENCES
Atenolol: 29122-68-7. 29122-68-7_ Atenolol CAS No.:
29122-68-7 / atenolol Chinese and English name /
molecular formula / structural formula – 960 chemical
network. (n.d.)
https://www.chem960.com/cas/29122687/.
(Chinese Source that specifies the solid-crystallite
powder form under room temperature)
Atenolol. Uses, Interactions, Mechanism of Action |
DrugBank Online. (n.d.).
https://go.drugbank.com/drugs/DB00335.
AE;, T. I. V. T. V. Y. K. T. N. V. (n.d.). Estimation of
aqueous solubility of chemical compounds using e-
state indices. Journal of chemical information and
computer sciences.
https://pubmed.ncbi.nlm.nih.gov/11749573/.
Angiotensin ii. Uses, Interactions, Mechanism of Action |
DrugBank Online. (n.d.).
https://go.drugbank.com/drugs/DB11842.
Adrenal glands. Johns Hopkins Medicine. (n.d.).
https://www.hopkinsmedicine.org/health/conditions-
and-diseases/adrenal-glands.
Aquarius. (2013, October 17). Hypertension. SlideServe.
https://www.slideserve.com/aquarius/hypertension-
1359807.
Atenolol / CHLORTHALIDONE Prices, coupons &
savings tips. GoodRx. (n.d.).
https://www.goodrx.com/atenolol-
chlorthalidone#:~:text=ATENOLOL%3B%20CHLO
RTHALIDONE%20is%20a%20combination%20of%
20a%20beta,55%25%20off%20the%20average%20re
tail%20price%20of%20%2434.01.
Bao, M., & Wang, L. (2020, August 19). The longitudinal
trend of hypertension prevalence in Chinese adults
from 1959 to 2018: A systematic review and meta-
analysis. Annals of Palliative Medicine.
https://apm.amegroups.com/article/view/49787/html.
Beta blocker. Beta Blocker. Causes, symptoms, treatment
Beta Blocker. http://dxline.info/diseases/beta-blocker.
Candesartan Cilexetil. Uses, Interactions, Mechanism of
Action | DrugBank Online. (n.d.).
https://go.drugbank.com/drugs/DB00796?__cf_chl_ca
ptcha_tk__=pmd_97bed8bfcba201ec7a6992afee46ee
3521a719a5-1628218821-0-
gqNtZGzNAvijcnBszQq6.
Candesartan Cilexetil. LGM Pharma. (2021, April 15).
https://lgmpharma.com/product/candesartan-cilexetil/.
Calculators and predictors. ChemAxon. (n.d.).
https://chemaxon.com/products/calculators-and-
predictors#pka.
CV;, A. S. P. (n.d.). Beta 1 receptors. National Center for
Biotechnology Information.
https://pubmed.ncbi.nlm.nih.gov/30422499/.
CDD Conserved Protein Domain Family: 7tmA_AT1R
(nih.gov) (database)
CDD Conserved Protein Domain Family: 7tmA_AT1R
(nih.gov) (database)
Candesartan prices, coupons & savings tips. GoodRx.
(n.d.). https://www.goodrx.com/candesartan.
Choudhary, D. D. (2016, September 2). Atenolol:
Therapeutic uses, Dosage & side effects. DoctorAlerts.
https://www.doctoralerts.com/atenolol/#:~:text=Ateno
lol%20is%20a%20adrenergic%20antagonist%20%28
%CE%B22-
selective%20blocker%29%2C%20used,hypertension
%20%26%20coronary%20artery%20disease.%20Dos
e%3A%2050-100%20mg.
Giacchetti G;Opocher G;Sarzani R;Rappelli A;Mantero F;
(n.d.). Angiotensin ii and the adrenal. Clinical and
experimental pharmacology & physiology.
Supplement.
https://pubmed.ncbi.nlm.nih.gov/8993850/.
GL;, O. R. V. B. (n.d.). Management of hypertension in the
elderly population. The journals of gerontology. Series
A, Biological sciences and medical sciences.
https://pubmed.ncbi.nlm.nih.gov/22913963/.
Hasanah, A. N., Dwi Utari, T. N., & Pratiwi, R. (2019, May
19). Synthesis of atenolol-imprinted polymers with
methyl methacrylate as functional monomer in
propanol using bulk and precipitation polymerization
method. Journal of analytical methods in chemistry.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6545
811/.
I;, F. F. M. K. T. (n.d.). Role of angiotensin ii in blood
pressure regulation and in the pathophysiology of
cardiovascular disorders. Journal of human
hypertension.
https://pubmed.ncbi.nlm.nih.gov/8583476/.
J;, A. H. B. F. C. (2011 Dec;29). Mortality patterns in
hypertension. Journal of hypertension.
https://pubmed.ncbi.nlm.nih.gov/22157565/.
Karaman, R. (2016, February 19). From conventional
prodrugs to prodrugs designed by molecular orbital
methods. Frontiers in Computational Chemistry.
https://www.sciencedirect.com/science/article/pii/B97
81608059799500056.
Khawaja, Z., & Wilcox, C. S. (2011, August). An overview
of candesartan in clinical practice. Expert review of
cardiovascular therapy.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3202
428/.
Libretexts. (2020, July 11). Atenolol. Chemistry
LibreTexts.
https://chem.libretexts.org/Under_Construction/Stalle
d_Project_(Not_under_Active_Development)/Walker
/Chemicals/Substance_A/Atenolol.
Lennarz, W. J. (2013). Encyclopedia of biological
chemistry. Elsevier Acad. Press.
Mayo Foundation for Medical Education and Research.
(2021, July 1). High blood pressure (hypertension).
Mayo Clinic. https://www.mayoclinic.org/diseases-
conditions/high-blood-pressure/symptoms-causes/syc-
20373410.
Mayo Foundation for Medical Education and Research.
(2021, July 1). High blood pressure (hypertension).
Mayo Clinic. https://www.mayoclinic.org/diseases-
conditions/high-blood-pressure/symptoms-causes/syc-
20373410.
Cross Examination of Atenolol and Canderstan Cilexetil on the Treatment of Hypertension
1161

M.T., P. (n.d.). THE PHARMACOLOGY OF
ADRENERGIC RECEPTORS. ADRENERGIC
pharmacology.
http://www.uky.edu/~mtp/OBI836AR.html.
National library of medicine. Citizendium. (n.d.).
https://en.citizendium.org/wiki/National_Library_of_
Medicine.
On-line Lipophilicity/Aqueous SOLUBILITY calculation
software. (n.d.). http://www.vcclab.org/lab/alogps/.
Pharmaceuticals, A. N. I. (2020, May 7). ATACAND HCT
(ANI Pharmaceuticals, Inc.): FDA package insert.
MedLibrary.org.
https://medlibrary.org/lib/rx/meds/atacand-hct-1/.
Price elasticity of demand - harvard university. (n.d.).
https://scholar.harvard.edu/files/alada/files/price_elast
icity_of_demand_handout.pdf.
Ramkanth, S., Chetty, C. M., Sudhakar, Y.,
Thiruvengadarajan, V. S., Anitha, P., & Gopinath, C.
(2018, March 15). Development, characterization &
invivo evaluation of proniosomal based transdermal
delivery system of atenolol. Future Journal of
Pharmaceutical Sciences.
https://www.sciencedirect.com/science/article/pii/S23
14724516301029.
Steinberg SF; Alcott S; Pak E; Hu D; Protas L; Möise NS;
Robinson RB; Rosen MR; (n.d.). beta (1)-Receptors
increase camp and induce Abnormal CA(I) cycling in
the German shepherd sudden death model. American
journal of physiology. Heart and circulatory
physiology.
https://pubmed.ncbi.nlm.nih.gov/11893550/.
SM;, M.-D. S. N.-J. M. R. G. (n.d.). Synthesis,
characterization, AND Atenolol Delivery application
of FUNCTIONALIZED Mesoporous
HYDROXYAPATITE NANOPARTICLES prepared
by Microwave-Assisted Co-precipitation Method.
Current drug delivery.
https://pubmed.ncbi.nlm.nih.gov/26996370/.
The molecular details of receptor-drug interactions in the
treatment of asthma and heart conditions. European
Synchrotron Radiation Facility (ESRF). (2016,
February 2).
https://www.esrf.fr/news/spotlight/spotlight145/index
_html.
Team, H. J., & Team, H. J. (2018, December 31).
Iontophoresis treatment, physical therapy, medication
& side effects. Health Jade.
https://healthjade.com/iontophoresis/.
U.S. National Library of Medicine. (n.d.). Atenolol.
National Center for Biotechnology Information.
PubChem Compound Database.
https://pubchem.ncbi.nlm.nih.gov/compound/atenolol
U.S. National Library of Medicine. (n.d.). PubChem.
National Center for Biotechnology Information.
PubChem Compound Database.
https://pubchem.ncbi.nlm.nih.gov/#query=C14H22N2
O3.
U.S. National Library of Medicine. (n.d.). Angiotensin ii.
National Center for Biotechnology Information.
PubChem Compound Database.
https://pubchem.ncbi.nlm.nih.gov/compound/Angiote
nsin-II#section=Biologic-Description.
U.S. National Library of Medicine. (n.d.). Atenolol.
National Center for Biotechnology Information.
PubChem Compound Database.
https://pubchem.ncbi.nlm.nih.gov/compound/atenolol
#section=Solubility.
U.S. National Library of Medicine. (n.d.). Candesartan
Cilexetil. National Center for Biotechnology
Information. PubChem Compound Database.
https://pubchem.ncbi.nlm.nih.gov/compound/Candesa
rtan-cilexetil.
U.S. National Library of Medicine. (n.d.). Cdd conserved
protein domain family: 7tma_at1r. National Center for
Biotechnology Information.
https://www.ncbi.nlm.nih.gov/Structure/cdd/cd15192.
U.S. National Library of Medicine. (n.d.). Hazardous
substances Data BANK (HSDB): 6526 - PUBCHEM.
National Center for Biotechnology Information.
PubChem Compound Database.
https://pubchem.ncbi.nlm.nih.gov/source/hsdb/6526#s
ection=Mechanism-of-Action-(Complete).
Wang, Z., Zengwu Wang Division of Prevention and
Community Health, Chen, Z., Zuo Chen Division of
Prevention and Community Health, Zhang, L., Linfeng
Zhang Division of Prevention and Community Health,
Wang, X., Xin Wang Division of Prevention and
Community Health, Hao, G., Hospital, G. H. F., Zhang,
Z., Zugui Zhang Christiana Care Health System, Shao,
L., Lan Shao Division of Prevention and Community
Health, Tian, Y., Ye Tian Division of Prevention and
Community Health, Dong, Y., Ying Dong Division of
Prevention and Community Health, Zheng, C., …
*The names of the the China Hypertension Survey
Investigators are listed in the online-only Data
Supplement.Sources of Funding. (2018, February 15).
Status of hypertension in China. Circulation.
https://www.ahajournals.org/doi/full/10.1161/CIRCU
LATIONAHA.117.032380.
Whelton, P. K., Search for more papers by this author,
Carey, R. M., Aronow, W. S., American Society for
Preventive Cardiology Representative. Search for
more papers by this author, Casey, D. E., ACC/AHA
Representative. Search for more papers by this author,
Collins, K. J., Lay Volunteer/Patient Representative.
Search for more papers by this author, Himmelfarb, C.
D., Preventive Cardiovascular Nurses Association
Representative. Search for more papers by this author,
DePalma, S. M., American Academy of Physician
Assistants Representative. Search for more papers by
this author, Gidding, S., Task Force Liaison. Search for
more papers by this author, Jamerson, K. A.,
Association of Black Cardiologists Representative.
Search for more papers by this author, Jones, D. W.,
MacLaughlin, E. J., … M., M. (2018, May 1). 2017
ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/A
SPC/NMA/PCNA guideline for the prevention,
detection, evaluation, and management of high blood
pressure In Adults: A report of the American College
OF CARDIOLOGY/AMERICAN Heart Association
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
1162

Task force on clinical practice guidelines. Journal of
the American College of Cardiology.
https://www.jacc.org/doi/full/10.1016/j.jacc.2017.11.
006?_ga=2.86879320.1182640551.1528306905-
1524800955.1528306905.
Cross Examination of Atenolol and Canderstan Cilexetil on the Treatment of Hypertension
1163
