
IoT-based Health Monitoring System for Intensive Care Units
Adriana Collaguazo
a
, Rebeca Estrada
b
and Nestor Arreaga
Escuela Superior Politcnica del Litoral, ESPOL,
Electrical Engineering and Computer Science and Technology Information Center,
Campus Gustavo Galindo Km. 30.5 Via Perimetral, P.O. Box 09-01-5863, Guayaquil, Ecuador
Keywords:
Mobile App, Intensive Care Unit, Smart Environment, IoT Health Application.
Abstract:
Due to the critical condition and unique treatments required by ICU’s patients, their vital signs should be
continuously and reliably monitored. In this paper, we present a system to address this problem including the
design considerations. Our system has three components: i) a mobile application to present the collected data
from the hospitals server, ii) a database server with patients data and iii) a transactional server that manages
and keeps the connection between the other two components. The mobile application implements a vital signs
monitor for each patient including an underlying emergency notification system. After several simulations,
we were able to identify that the proposed solution takes around 3 seconds to generate the notification after
an emergency alarm occurs. Moreover, the application uses an average of 2.11 Kb/s of traffic data and a
maximum of 250Mb of RAM. This system is a feature that will help to track the ICU patients status, allowing
doctors and ICU managers to work outside the unit and to determine when their presence is required. Results
show that relevant and accurate notifications can effectively reduce the time response in cases of emergency
and consequently increases the likelihood of the patients’ recovery.
1 INTRODUCTION
The Intensive Care Unit (ICU) is a specialized area
of a hospital that provides care to patients with se-
vere or life-threatening illnesses and injuries. This
area requires constant and close supervision from life
support equipment and medication to ensure normal
bodily functions (National Health Service, ). A con-
tinuous physician supervision is recommended for pa-
tients under these conditions, however, treating physi-
cians cannot remain in the ICU unit all the time to take
care of these patients. Instead, resident doctors re-
main in the area to constantly monitor each patient. In
the event of an emergency, resident physicians should
contact the treating physicians, either by using a com-
munication devices (e.g., phone or beeper) or by per-
sonally searching for them, leading to higher response
time in emergency cases.
This paper proposes the design and implementa-
tion of an automated alert system to tackle the above
problem. For instance, a case study was carried out
in the ICU of Guayaquil Hospital, in Ecuador. In
this hospital, the ICU unit has 21 places for criti-
a
https://orcid.org/0000-0002-0707-0226
b
https://orcid.org/0000-0003-3957-9294
cal care, of which 7 places are for isolated patients,
and serves approximately 15 patients (Ministerio de
Salud, 2018). The proposed system have several com-
ponents, such as: 1) a mobile application to present
the collected data from the hospitals server, 2) a
database server with patients data and 3) a transac-
tional server that manages and keeps the connection
between the other two components.
The mobile application shows the vital signs of
patients and each doctor can login into the applica-
tion, then, they can see the area with several win-
dows and the sectors of the ICU and their respec-
tive beds. Accelerometer sensors are used to monitor
the patients’ movement. In the event of any strange
movement, the physicians can get an idea of patients’
position through the report patients’ physical status.
Moreover, alerts are automatically generated to notify
doctors when a patient’s vital signs are outside the es-
tablished range. This type of emergency is displayed
in the application by changing the buttons of the sec-
tor, the bed and the parameter to a red color.
This work implements a solution that is able to:
• Report constantly the vital signs of patients by
means of non traditional systems.
• In case of emergency, alert are sent to the respec-
Collaguazo, A., Estrada, R. and Arreaga, N.
IoT-based Health Monitoring System for Intensive Care Units.
DOI: 10.5220/0011339800003286
In Proceedings of the 19th International Conference on Wireless Networks and Mobile Systems (WINSYS 2022), pages 101-106
ISBN: 978-989-758-592-0; ISSN: 2184-948X
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
101

tive staff in a hierarchical manner.
• Reduce the current average response time.
This paper is organized as follows: Section 2 de-
scribes the prior investigation of the equipment and
materials used to design the system. In section 3 we
presents the proposed system with the connection be-
tween the different modules. Section IV shows the
results of the application tests. Finally, section 5 con-
cludes our research work.
2 RELATED WORK
Researchers of the preliminary studies have managed
the real-time data over networks to be available to
clinicians in the Intensive Care Unit (ICU) anywhere
on the web with appropriate software and privileges.
Considering the IoT applications covers smart en-
vironments in domains such as emergency, health
care, and user interaction(Dr. Ovidiu Vermesan et al.,
2017).
According Thibaud (Thibaud et al., 2018), iden-
tifies that in the near future (within 5 years) several
theoretical or pilot projects will tackle different is-
sues such as better integration of pervasive health-
care services with general health care services in a lo-
cal database environment that ensures data availabil-
ity and that performs intelligent processes to deliver
quicker preliminary information without compromis-
ing the energy-efficiency of sensor networks.
In (Lamberti and Montrucchio, 2003), the medical
staff equipped with Personal Digital Assistant (PDA)
devices both inside and outside the hospital have mo-
bile access to the electronic patient’s clinical record.
Using a framework for ubiquitous monitoring in an
ICU, by the bedside monitoring network, on secure
wireless communication channels. Although, the val-
idation of the proposed framework effectiveness is
fundamental, and requires the design of the software
modules needed.
The system called ADSA (Automatic Detection
of risk Situations and Alert) (Ahouandjinou et al.,
2016) is based on a hybrid architecture for a visual
patient monitoring system using a multi-camera sys-
tem and collaborative medical sensors network was
developed. Although this proposal proved to enable
personalization of treatment and management options
targeted particularly to the specific circumstances and
needs of the individual, it requires the use of cameras
to support the decision process which is not possible
considered the financial constraints faced by the hos-
pital used as a case of study.
In (Gupta et al., 2016) the IoT-based health moni-
toring system can provide support in Intensive Care
Units(ICU) using an INTEL GALILEO 2ND. This
system contains a live graph of the patients heart rate
and the temperature is being monitored. However, the
system could have been developed in a mobile appli-
cation for facilitating the access of the users.
In (Chiuchisan et al., 2014) propose the architec-
ture of a health care system for Intensive Care Unit
(ICU) through of bedside monitors to monitor and
record multiple physiological parameters of patients;
Microsoft XBOX Kinect to monitor the movement of
the patients; and sensor board for monitoring of envi-
ronmental parameters such as temperature, humidity,
atmospheric pressure. The system is part of a more
complex system in development and will be improved
by adding new types of sensors like pressure, body
weight.
In (Pickering et al., 2018) using the Continuous
Time Markov Chain (CTMC) in the develop a bot-
tleneck analysis method to identify opportunities for
improvement in the rounding process in an Inten-
sive Care Units at Mayo Clinic. The workflow re-
design needs further investigation as the ideal balance
between patient care activities and education is still
largely unknown and is likely to vary depending on
the circumstances.
In (Mahmud et al., 2018) present a Fog-based IoT-
Healthcare solution structure and explore the integra-
tion of Cloud-Fog services in inter-operable Health-
care solutions extended upon the traditional Cloud-
based structure. The mobility of the user and edge-
centric affinity of the applications should be handled
together by the Fog cluster for better performance.
3 SYSTEM DESIGN
In this section, we present the design of the proposed
system taking into account the users requirements to
better asset their needs. Based on this requirements
a top-level architecture is proposed. In addition, the
back end server components are described as well as
the application and node design.
3.1 User Requirements
From a user perspective, collecting and sharing health
information of patients must satisfy at least the fol-
lowing properties:
• Data accuracy: A margin of error should be es-
tablished for the data measuring. In this particular
case, health measures must be very precise since
the slightest difference can have a serious or un-
wanted impact.
WINSYS 2022 - 19th International Conference on Wireless Networks and Mobile Systems
102
• Availability: The system is used by different users
who have different access roles and requirements,
and therefore, must be available to all users any-
time, anywhere.
• Performance: The system should offer a satisfac-
tory performance to end users. The response time
in all procedures should be as low as possible.
• Data privacy: The privacy of health data must
be protected for all users, especially those under
critical monitoring. The system should provide a
proven mechanism to ensure privacy.
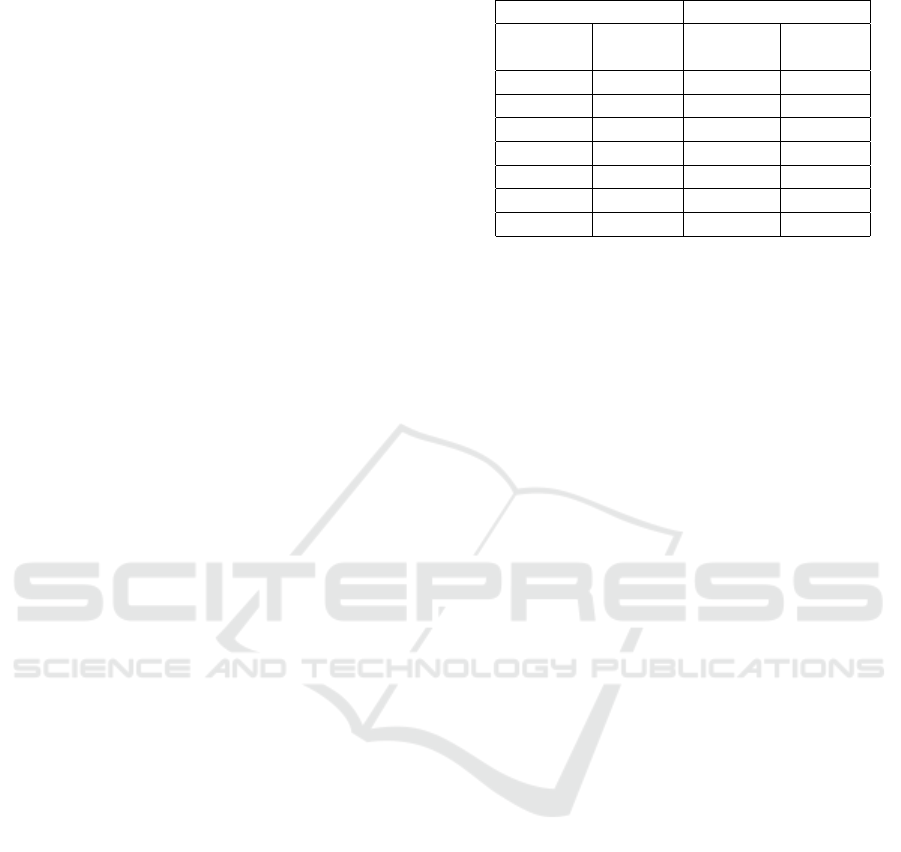
3.2 System Architecture
Figure 1 presents the top-level architecture of the pro-
posed ICU automation system. The architecture con-
sists of a Sink Node that is connected to the back-end
server using the Local Area Network (LAN). The ex-
isting infrastructure provides a WiFi physical layer to
connect the smart devices or phones to the local net-
work. The intranet is also connected to this WiFi net-
work. Thus, these devices provide the primary human
machine interface for the nurses, doctors and other
staff. The server has its own database and application
servers and MySQL is used as the Data Base Manage-
ment System (DBMS) engine while Apache provides
the application server functionality. The application is
Web-enabled, which requires only a standard browser
at the client side.
The first module is composed of the sensors de-
ployed on the beds. These sensors are connected to
a gateway designed with an Arduino UNO and an
Ethernet Shield, connected directly to the hospital’s
internal network where the data is transmitted and
stored in the MySQL database. In addition, each pa-
tient has a monitor connected directly to the hospital
network, which provides their vital signs and stores
this information in a proprietary database. The sec-
ond module consists of a PHP-based server based and
a MySQL server. The server contains several scripts
to perform search, add or update information in the
database when a request is received from the mobile
application. The third module is a mobile application
that allows physicians to visualize patient data.
3.3 Sink Node
The sink node consists of an accelerometer sensor and
a wireless transceiver, connected to an Arduino Nano,
on the other side each node is connected to BeneView
T8 vital signs monitor. The motion sensor MMA7361
is used to detect a fall from the bed. This sensor al-
lows us to measure the acceleration of 3 axes (x, y,
Table 1: Connections between Arduino and transceivers.
Transmitter Receiver
nrf24101 Arduino nrf24101 Arduino
nano UNO
VCC 3.3V VCC 3.3V
GND GND GND GND
CSN 10 CSN 8
CE 9 CE 7
MOSI 11 MOSI 11
SCK 13 SCK 13
MISO 12 MISO 12
z), and it was calibrated correctly at the time of use.
Then we connected it to the nano Arduino, together
with a nrf24101 transceiver that allows the connec-
tion between the nodes and the sink node (Table 1).
The Arduino nano is programmed so that when the
severity of an axis changes abruptly, the Arduino will
register that the person is falling and send a signal to
the sink node to notify the emergency.
The sink node was built over an Arduino UNO, to
which an ethernet shield was added to be able to com-
municate with the server. When the Arduino UNO re-
ceives the signal that the patient fell, he connects with
the server and sends him a request with the number
of the bed to generate an alarm in the database which
the cell phone will notify the doctors. This module
should be improved with equipment with higher ca-
pacity and durability, which can support long periods,
such as a Beaglebone or a Raspberry.
3.4 Transactional Server
The transactional server consists of several PHP
scripts to perform the requests generated by the users
of the mobile application. These scripts receive a re-
quest from the application to search information from
the database and return the requested query in a spe-
cific format, which is transferred through JSON mes-
sages because of their simplicity and the speed to
transfer the data. To prevent the leakage of sensi-
tive information or problems such as SQL injection,
the data received in each request was sent separately
and parameterized, and no script contains queries that
could reveal data about database structures. More-
over, as an extra security measure, the patient’s in-
formation and vital signs are not stored in the device
running the mobile application.
3.5 Database Server
The management of MySQL database was carried out
by means of PHPMyAdmin software tool. With this
tool, we were able to maintain an up-to-date copy of
IoT-based Health Monitoring System for Intensive Care Units
103
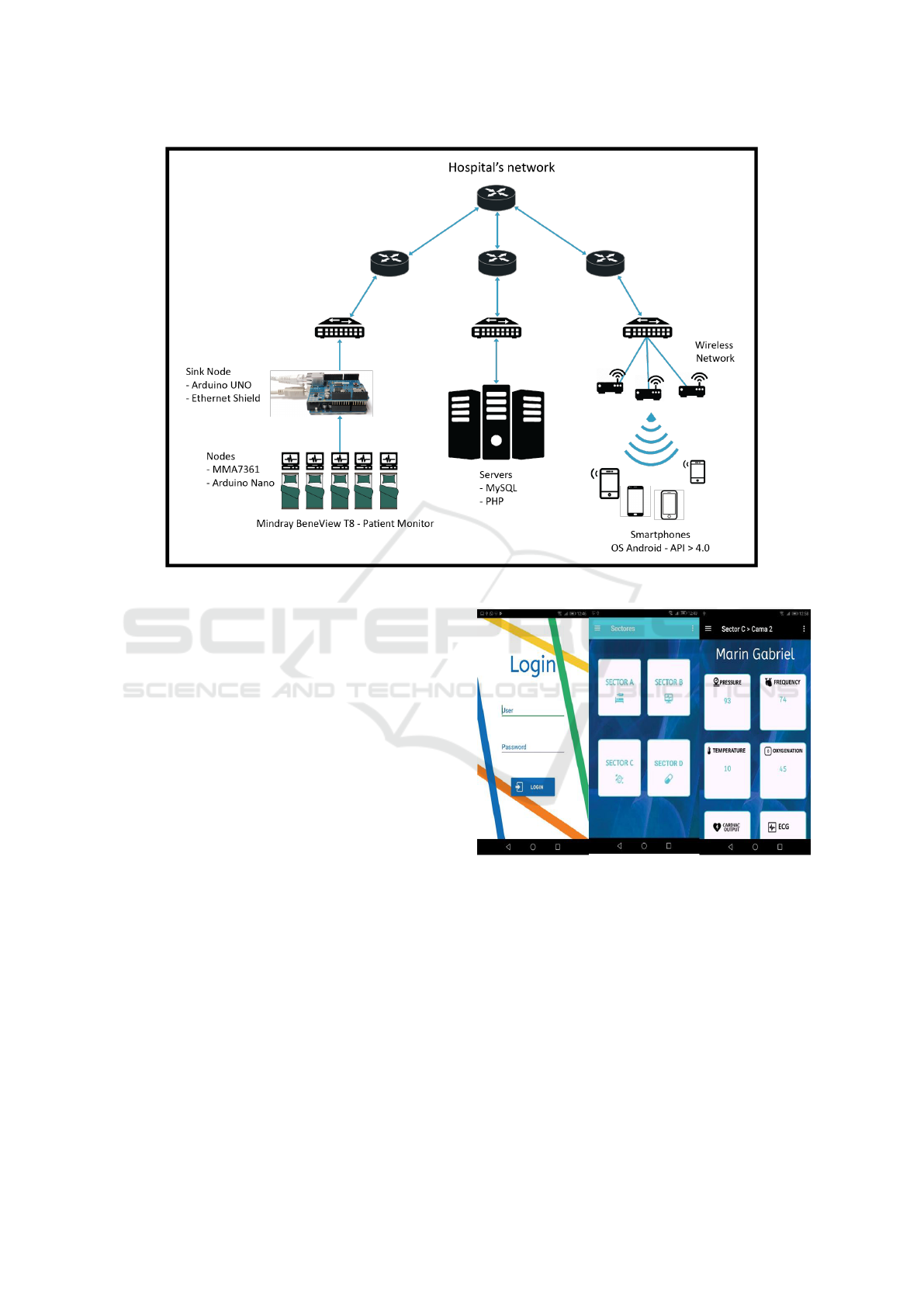
Figure 1: Top-level system architecture of the UCI system.
the database structure and its contents from a hospi-
tal vendor’s proprietary equipment. Thus, we will not
affect the integrity of the actual data of the patients in
the intensive care unit. The patient’s name, location,
blood pressure, heart rate, temperature and oxygena-
tion are some of the information stored as the patient
data. This data can also be consulted through the mo-
bile application.
3.6 Mobile Application
The mobile application was developed using Android
Studio for phones with Android operating system be-
cause it is a prevalent mobile operating system in
Ecuador. This IDE has available libraries that allow
direct interaction with mobile functions and offers a
suitable graphical environment for view design.
The application generates POST requirements to
communicate with the PHP server. Figure 2 illustrates
different views that the mobile application has. The
first is used to allow the user can connect to the sys-
tem using their identification number and password.
The second view shows the four sectors of the ICU
area and by selecting any of these, the numbered beds
in the sector is shown. For each bed, the app shows
the patient’s name when there is a patient using the
bed otherwise it shows ”NO DATA”. By choosing the
patient, a parameter view is presented, where the val-
ues of the patient’s vital signs in real time.
Figure 2: Mobile Application Interfaces.
To facilitate the data analysis, the user can choose
any of the parameters and a real-time graph of this
parameter is shown. In addition, the user can choose
to forecast the trend of the parameter, which is done
using the 3rd order moving average of the parameter.
To obtain this data, the system generates requests to
the server every 0.5 seconds sending the correspond-
ing information of the selected parameters, bed and
section.
The mobile application has a persistent service
that keeps the medical staff aware of the patient’s sta-
tus. This service sends a request every 3 seconds and
thus be able to issue timely emergency alerts.
WINSYS 2022 - 19th International Conference on Wireless Networks and Mobile Systems
104

When an event is identified, a vibrating and sound
alert notification is generated. Such notifications may
not be silenced unless the user voluntarily logs out or
the emergency is resolved.
For the generation of alarms, a hierarchical clas-
sification is implemented according to users’ role as
follows:
• Physician on shift: instant alert generation.
• Sector supervisor: 5 minutes after the emergency
alert is generated.
• Area supervisor: 10 minutes after the emergency
alert is generated.
To keep control of notifications, the user’s role
is saved in the internal memory of the mobile phone
while his session is active.
4 RESULTS ANALYSIS
Once the system was fully developed, we perform
several tests to validate the functionality of each com-
ponent. The tool used for testing was Android Profile,
which is part of the Android Studio software package
() [7]. This tool allows the developer to determine the
usage of CPU, memory, power and data. Each test
was performed fifteen times and the results were av-
eraged. The first test consisted of measuring the total
time between the generation of an emergency in the
database and the notification in the mobile application
to determine the average time to generate emergency
notifications.
Each sample time period began with the activa-
tion of the emergency trigger and ended with the re-
ceived pop-up notification. For better precision, a dig-
ital trigger was used to start the tests. Also, the trigger
system and the alarm were installed on different net-
works and separated by a distance of 9.1 miles.
During the initialization period, the average re-
sponse took around 5.5 seconds with standard devia-
tion of 1.5s. With the system in steady state, the mean
response time was 3 seconds with a standard devia-
tion of 0.5s, as shown in Fig 3
The second test was used to measure mobile data
consumption and to estimate the maximum band-
width consumption during a 20-second period while
keeping the real-time parameters window open, as it
is the most resource-consuming window of the appli-
cation due to the constant checking of the different
vital signs of the patient.
Fig. 4 shows the data rate used for transmission
while performing the parameter analysis in real-time
since it is the most demanding activity of the mobile
Figure 3: Tests of the time interval between the patient’s fall
and the notification of the alert.
Figure 4: Data Rate for the functionality of parameter anal-
ysis in real-time.
application. Each test was run for a duration of 20
seconds, and the average data rate was 2.11 Kbps.
The third test allows us to measure the bandwidth
consumption of the notification generation service to
determine the minimum bandwidth consumption of
the mobile application when it is in the background.
This test consists of having the alarm system running
in background mode considering a time 20-seconds
interval. In this case, the average data rate was 0.51
Kbps, as shown in Fig. 5
The purpose of the paper was to analyze the
amount of resources required on the mobile phone to
run the application in a controlled environment. How-
ever, it is important to remark that the used sensor was
a low cost sensor, which means that it is device with
a time-consuming maintenance. In addition, the ac-
celerometer starts to overheat after a few hours, which
might affect the response time and the accuracy. This
should be taken into account when implementing a
sustainable solution for a real environment.
IoT-based Health Monitoring System for Intensive Care Units
105
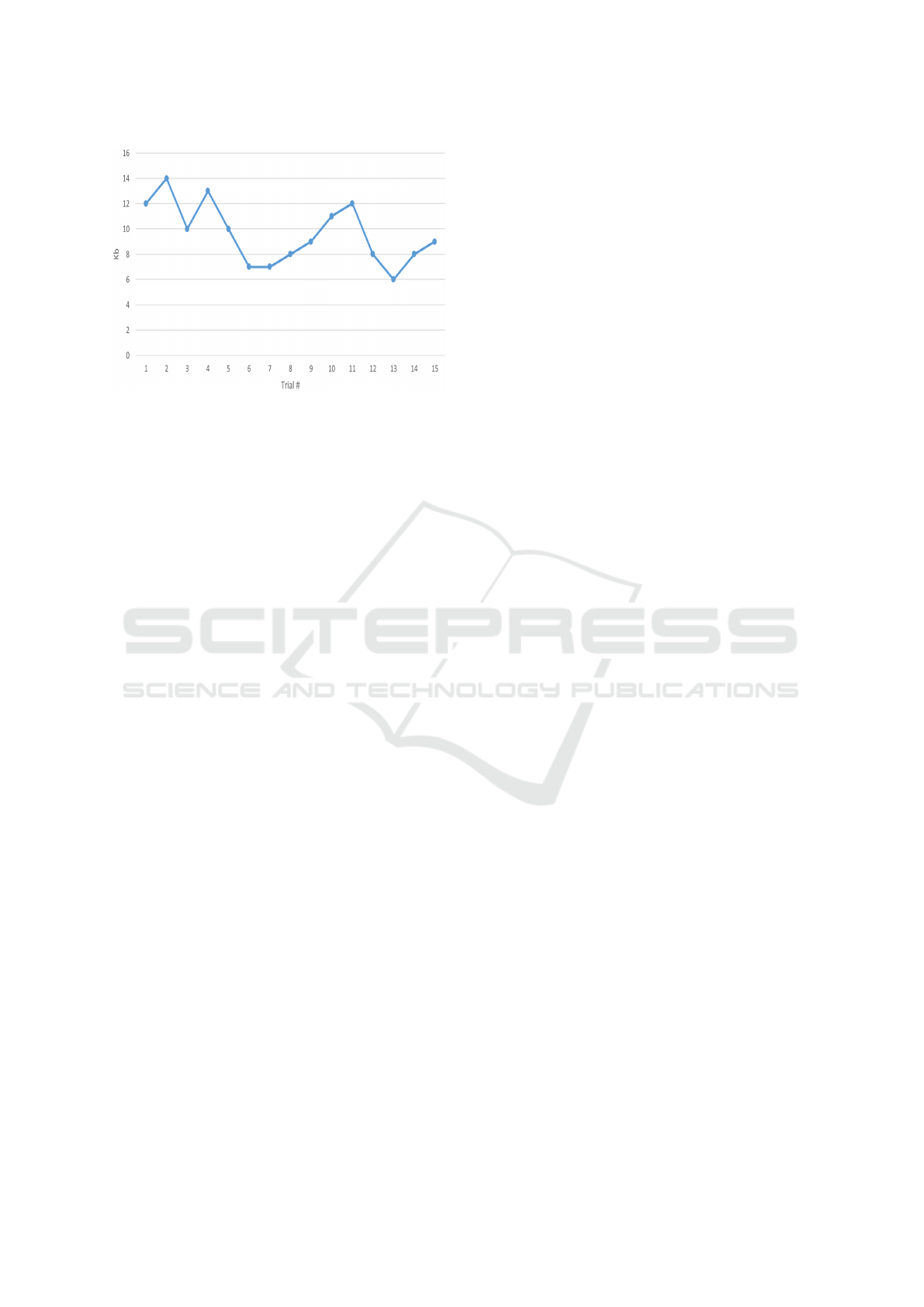
Figure 5: Data Rate required for notification generation ser-
vice.
5 CONCLUSIONS
In this paper, we presented an innovative system that
enables the medical staff to check and analyze the vi-
tal signs of ICU’s patients from distance, having a
constant control of them. Pop-up notifications alert
the response team if one or more patients have a sig-
nificant change of vital signs. This allows the med-
ical team to react quickly and apply the appropri-
ate treatment. The database access table helps the
hospital management team to control and protect pa-
tient data. This also helps the system provide a hi-
erarchically controlled alert. The resources required
for mobile application allows it to be run in low-mid
range and higher phones. The application design fa-
cilitates the training period its users, which helps the
users’ work environment. As future work, we plan
to make the system more functional, allowing to es-
tablish relationships between several parameters and
obtain more accurate information about the patient’s
condition. Patients’ data from the system could be an-
alyzed with the machine learning algorithm to predict
their status and reduce the generation of emergency
notifications to the cases where the presence of the
main doctor is really necessary.
REFERENCES
Ahouandjinou, A., Assogba, K., and Motamed, C. (2016).
Smart and pervasive ICU based-IoT for improving
intensive health care. In 2016 International Con-
ference on Bio-engineering for Smart Technologies
(BioSMART), pages 1–4. IEEE.
Chiuchisan, I., Costin, H. N., and Geman, O. (2014).
Adopting the internet of things technologies in health
care systems. In EPE 2014 - Proceedings of the 2014
International Conference and Exposition on Electri-
cal and Power Engineering, pages 532–535. Institute
of Electrical and Electronics Engineers Inc.
Dr. Ovidiu Vermesan, SINTEF, N., Friess, D. P., and EU, B.
(2017). Internet of Things: Converging Technologies
for Smart Environments and Integrated Ecosystems.
Gupta, P., Agrawal, D., Chhabra, J., and Dhir, P. K. (2016).
IoT based smart healthcare kit. In 2016 International
Conference on Computational Techniques in Infor-
mation and Communication Technologies, ICCTICT
2016 - Proceedings, pages 237–242. IEEE.
Lamberti, F. and Montrucchio, B. (2003). Ubiquitous real-
time monitoring of critical-care patients in intensive
care units. In Proceedings of the IEEE/EMBS Region
8 International Conference on Information Technol-
ogy Applications in Biomedicine, ITAB, volume 2003-
Janua, pages 318–321.
Mahmud, R., Koch, F. L., and Buyya, R. (2018). Cloud-Fog
Interoperability in IoT-enabled Healthcare Solutions.
In Proceedings of the 19th International Conference
on Distributed Computing and Networking - ICDCN
’18, pages 1–10, New York, New York, USA. ACM
Press.
Ministerio de Salud, E. (2018). Rendici
´
on de cuentas 2018.
National Health Service. Intensive care - NHS.
Pickering, B., Li, J., Dong, Y., Gajic, O., and Lee, H. K.
(2018). Bottleneck Analysis to Improve Multidisci-
plinary Rounding Process in Intensive Care Units at
Mayo Clinic. IEEE Robotics and Automation Letters,
3(3):2678–2685.
Thibaud, M., Chi, H., Zhou, W., and Piramuthu, S. (2018).
Internet of Things (IoT) in high-risk Environment,
Health and Safety (EHS) industries: A comprehensive
review. Decision Support Systems, 108:79–95.
WINSYS 2022 - 19th International Conference on Wireless Networks and Mobile Systems
106
