
Detection of Urinary Biomarkers for Early Diagnosis of Pancreatic
Cancer by Data Analysis
Chi Le
1,† a
, Yucheng Liu
2,† b
, Fangyi Tian
3,† c
and Yang Xu
4,† d
1
ZJU-UoE Institute, Zhejiang University, Hangzhou, Zhejiang, China
2
College of Animal Sciences & Technology, Huazhong Agricultural University, Wuhan, Hubei, China
3
Basic Medical School, Capital Medical University, Beijing, China
4
College of Life Sciences, Nanjing Agricultural University, Taizhou, Jiangsu, China
†
These authors contributted equally
Keywords: Pancreatic Cancer, Diagnosis, Urinary Biomarkers.
Abstract: In this sample-structured document, neither the cross-linking of float elements and bibliography nor
metadata/copyright information is available. The sample document is provided in “Draft” mode and to view
it in the final layout format, applying the required template is essential with some standard steps.
According to data released by the American Cancer Society in 2019, the mortality rate caused by pancreatic
cancer ranks fourth among malignant tumors. By 2030, the incidence of Pancreatic ductal adenocarcinoma
(PDAC) will continue to increase and may become the second leading cause of death among all tumor
diseases. If the tumor could be detected and resectted at an early stage, the survival rate of PDAC patients
will be greatly improved. However, symptoms rarely show until the cancer reaches its advanced stage and
most of the available treatments are palliative. Therefore, most patients have reached the advanced stage of
cancer when they are diagnosed and thus having poor prognoses. Therefore, we are interested in the early
detection, prediction and diagnosis of pancreatic cancer, and we will discusse which factors are related to
pancreatic cancer in the following parts.
We collected a total of 590 samples in which 7 attributes, age, CA 19–9 (Carbohydrate antigen199),
creatinine, LYVE1 (Lymphatic Vessel Endothelial Hyaluronic Acid Receptor 1), REG1B (regenerating islet-
derived 1 beta), TFF1 (Recombinant Trefoil Factor 1) and REG1A (Recombinant Human Regenerating Islet-
Derived Protein 1-alpha) were selected as our independent variables. The dependent variable Y is diagnosis
which indicates whether a participant has pancreatic cancer. Logistic regression and lasso regression were
used to construct a model for the prediction of pancreatic cancer. All analyses above were performed using R
software, version 4.1.1.
We finally found that the distributions of Blood plasma levels of CA 19–9 monoclonal antibody, creatine,
LYVE1, REG1B, TFF1 and REG1A are all positive skewed and asymmetrical. In addition, people's illness is
significantly related to age, creatine, LYVE1, REG1B, TFF1 and REG1A. However, the level of CA 19-9
monoclonal antibody in the human body is not so significantly correlated with the corresponding human
disease. After selecting appropriate methods and analyzing a large amount of data, according to the regression
results, etc., we can conclude that the incidence of PDAC disease is significantly related to age and gender.
Based on this, in the follow-up research, it has provided the possibility for early prediction and disease
prevention and control of PDAC based on age and gender, and also provided new ideas for the pharmaceutical,
treatment and daily care of the disease.
a
https://orcid.org/0000-0003-4414-3073
b
https://orcid.org/0000-0002-3095-9904
c
https://orcid.org/0000-0003-0536-6127
d
https://orcid.org/0000-0001-9482-5887
56
Le, C., Liu, Y., Tian, F. and Xu, Y.
Detection of Urinary Biomarkers for Early Diagnosis of Pancreatic Cancer by Data Analysis.
DOI: 10.5220/0011228500003438
In Proceedings of the 1st International Conference on Health Big Data and Intelligent Healthcare (ICHIH 2022), pages 56-61
ISBN: 978-989-758-596-8
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

1 INTRODUCTION
The pancreas is an organ located in the abdomen and
it plays an important role in converting the food we eat
into energy for body's activities. Pancreatic cancer is
one of the most common digestive tract malignancies.
It begins in the tissue of pancreas and is an extremely
deadly type of cancer, which is ranked as fourth
leading cause of cancer-related mortality in western
countries (Zeng et al., 2019). 90% of pancreatic
malignancies are pancreatic ductal adenocarcinoma
(PDAC) (He et al., 2014). Symptoms rarely shows
until the cancer reaches its advanced stage and most of
the available treatments are palliative (Adamska,
Domenichini and Falasca, 2017). With over 80% of
cases diagnosed at advanced stages, PDAC patients
have a median survival of 5-6 months, and the overall
5-year survival rate is less than 10% because patients
are diagnosed too late (Arnold et al., 2019). However,
if we can detect and resect the tumor at an early stage
of PDAC, the survival rate of cancer patients can be
greatly improved.
Therefore, we are interested in the early detection,
prediction, and diagnosis of PDAC, and trying to find
out what factors are related to pancreatic cancer. Also,
the development of non-invasive diagnosis to detect
early PDAC becomes an urgent need. Non-invasive
diagnostic technology can avoid or reduce pancreatic
biopsy to identify PDAC fibrosis early, and can
perform dynamic monitoring, which has important
clinical application value. Nevertheless, there is no
reliable, non-invasive screening test to detect PDAC
accurately and those methods are expensive (Brezgyte
et al., 2021). By contrast, detecting biomarkers for the
diagnosis of PDAC is minimally invasive and
relatively cheap.
Serum CA19-9, the only biomarker in clinical
practice currently, is less specific and sensitive for
screening purposes and is mainly used to monitoring
treatment response (Ballehaninna and Chamberlain,
2012). Previous studies have found that urine, an
alternative biological fluid has many advantages, such
as accumulation of biomarkers at higher concentra-
tions so that the biomarkers are easy to be detected.
Certain urinary metabolites can indicate malignancy
of various organs, possibly reflecting the metabolic
effects of cancer (Dinges, et al., 2019). Creatinine is a
product of muscle metabolism and is primarily cleared
by the kidneys (Delanaye, Cavalier and Pottel, 2017).
Therefore, biostatistical methods such as model
analysis can be used to identify more effective and
stable biomarkers and provide a reference basis for
early-stage PDAC detection and diagnosis, clinical
practice, related treatment and so on.
In the existing literature, a regression model
PancRISK have been developed using three protein
biomarkers to detect pancreatic cancer and classify
PDAC patients. Researchers of this experiment
creatively replaced REG1A with REG1B, showing
the ability of our urinary panel to distinguish control
individuals and patients with benign hepatobiliary
diseases from early stage PDAC patients with
specificity and sensitivity >85%. On the basis of these
studies, our team explored the previous research to
make some bold assumptions and continued to use
PancRISK with other methods to analyze data basing
on the original database to evaluate whether PDAC is
related to age, gender and other factors.
2 METHODS
2.1 Data Source
The data was selected from the Kaggle platform.
Kaggle is an open online platform, mainly for
developers, data scientists and anyone in need to
provide a platform for holding machine learning
competitions, hosting databases, and writing and
sharing code. The data comes from the data set in a
paper published by Silvana Debernardi and
colleagues in the journal PLOS Medicine on
December 10, 2020. The paper and the complete data
set are open access.
590 clinical specimens were obtained from
different centers: Barts Pancreas Tissue Bank,
University College London, University of Liverpool,
Spanish National Cancer Research Center, Cambridge
University Hospital, and University of Belgrade.
590 urine specimens were assayed and there were
three groups: 183 individuals who had no pancreatic
diseases in control group (group 1), 208 patients who
had benign hepotobiliary diseases in benign group
(group 2) and 199 PDAC patients before treatments
(group 3). 50.7% specimens were obtained from
female individuals.
Among these three types of samples, benign
samples included 119 CP cases, 54 gallbladder
diseases, 20 cystic lesions of the pancreas, and 15
cases with abdominal pain and gastrointestinal
symptoms suggestive of pancreatic origin.
In group 3, PDAC patients had 6 stages: 102 I-II
(IA, IB, IIA) and 97 III-IV (IIIB, III, IV)
Besides, there were 67 patients in urine specimens
with common urological tract malignancies: 18
patients with prostate cancers (PC) (median age 69
years, range 52–83), 29 patients with renal cell
carcinoma (RCC) (median age 67 years, range 20–
Detection of Urinary Biomarkers for Early Diagnosis of Pancreatic Cancer by Data Analysis
57

85), and 20 patients with bladder transitional cell
cancer (TCC) (median age 65 years, range 44–81).
The restriction is that the number of I–IIA PDAC
samples is low (n=27). In addition, the study used
samples collected from control individuals as
replacements for the lack of specimens from
individuals with hereditary predisposition to PDAC.
350 matched plasma specimens for samples (92
control, 108 benign, and 150 PDAC).
Our dataset Urinary biomarkers for pancreatic
cancer was downloaded from Kaggle, which was
uploaded in 2020.
2.2 Variable Measuring
The required urine and plasma samples were
collected from multiple centers after the respective
institutional review board approvals, and the potential
impact of bacterial growth on urine biomarkers was
tested with 20 mg/ml boric acid. Finally, the samples
were maintained at a low temperature of -80°C.
Commercially sourced ELISA kits were used for
assaying the biomarkers: lymphatic vessel
endothelial hyaluronan receptor 1 (LYVE1), trefoil
factor 1 (TFF1), regenerating family member 1 beta
(REG1B) and plasma CA19-9. Each measurement
was run in duplicate, and further repeats were
performed when there was a discrepancy. The
FLUOstar Omega Microplate Reader was used to
determine optical density. The Roche platform
(Cobas 601E [ECLIA] technology) at The Doctors
Laboratory in London was used to measure plasma
CA19-9. Urine creatinine was determined at the
Clinical Biochemistry Laboratory of the University of
Westminster using an ILab Aries analyser from
Instrumentation Laboratory.
All the research staff who performed the
experiments did not know about the sample diagnosis.
All protein concentration data were natural-log-
transformed and mean-centred.
2.3 Data Analysis
The values obtained from open access were analyzed
by exploratory data analysis firstly. At the beginning,
there were 14 original attributes and we finally
selected 7attributes age, CA 19–9, creatinine,
LYVE1, REG1B, TFF1 and REG1A as our
independent variables. The other 7 attributes are
confounders. The dependent variable Y is diagnosis
which indicates whether a participant has pancreatic
cancer. To meet the requirements of logistic
regression, all the category variables were coded by 0
and 1. After that, we chose to use random forest
algorithm to interpolate all the not available data in
the dataset. To explore the relationship between
independent variable and response, boxplots were
chosen to demonstrate the independent variables
visually (Fig 1.). It should be noted that all the
independent variables except the creatinine are
greater in the pancreatic cancer group significantly.
The χ2 test is used to test the correlation between sex
and diagnosis. The t-test is employed for the purpose
of testing the correlation between all independent
variables and dependent variables. To further explore
influence of interactions between the independent
variables, P-value was calculated.
In logistic regression, the logit function of p is used
to modeling the log odds of response variable as a
suitable transformation. In our study, we found that
some variables were highly correlated with others, in
which case their interactions are possible to differently
effect the response compared to single independent
variable. According to the result of correlation
analysis, we kept all the significantly-correlated
interactions of two variables. Lasso analysis were
performed to further select useful variables and
interactions. Next, we performed best subset selection
to identify the best model that contains a given number
of independent variables. We finally selected the
model based on best subset selection and the Akaike
Information Criterion (AIC) value, and then evaluated
the model with confusion matrix.
3 RESULTS
During the process of exploratory data analysis
(EDA), we first chose age, plasma CA 19-9,
creatinine, LYVE1, REG1A, REG1B and TFF1 as
independent variables and diagnosis as our dependent
variables. After viewing characteristics of all
variables (Table 1.), we found that the distributions of
most of them were skewed, which means that they
were asymmetrical. Take plasma CA 19_9 as an
example, the maximum of its blood plasma level is
31000, but more than 88% participants are smaller
than 1,000. The boxplots also verified this point (Fig
1.). In the comparison of plasma CA 19_9, there are
much more outliers in PDAC group than the PDAC-
free group, which indicates it might be a significant
measurement for PDAC. Also, in variables age,
LYVE1, REG1A, REG1B and TFF1, the minimums,
maximums, medians, first quartile, and third quartile
of PDAC patients group seem to be greater.
ICHIH 2022 - International Conference on Health Big Data and Intelligent Healthcare
58
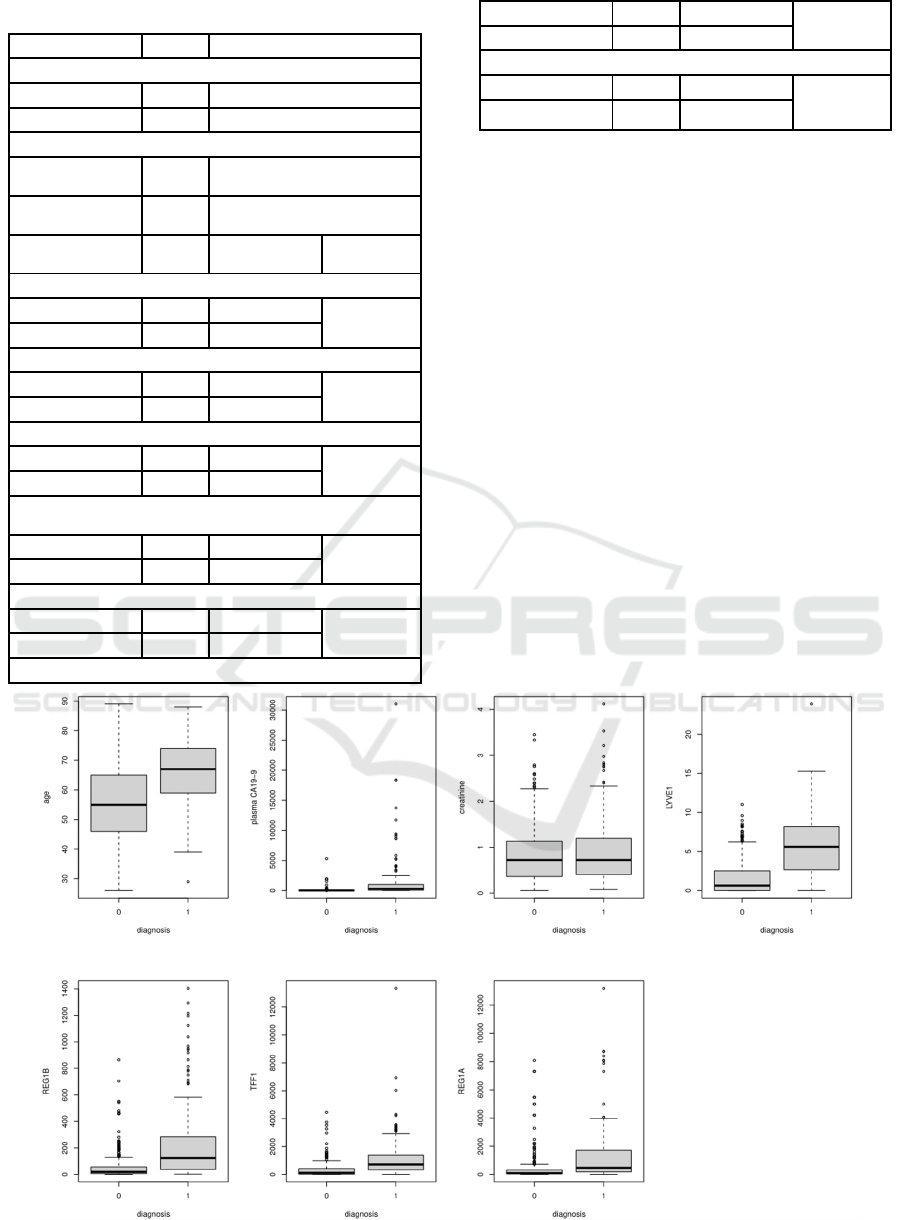
Table 1: Characteristics of Variables (N=590).
Characteristics
N
Percent(%)
Sex
Male 301 51.0
Female 289 49.0
Diagnosis
Pancreatic-
cance
r
-free
391 66.3
Pancreatic
cance
r
199 33.7
Continuous
variable
N
Percent(%) Range
Age
>=50 446 75.6
26-89
<50 144 24.4
Plasma CA19_9
>=1000 69 11.7
0-31000.0
<1000 521 88.3
Creatine
>=2 39 0.1
0-4.1
<2 551 99.9
Lymphatic vessel endothelial hyaluronan receptor 1
(LYVE1)
>=10 32 0.1
0-23.9
<10 558 99.9
Regenerating family member 1 beta (REG1B)
>=700 18 0.1
0-1403.9
<700 572 99.9
Trefoil factor 1 (TFF1)
>=1000 95 16.1
0-13344.3
<1000 495 83.9
Regenerating family member 1 alpha (REG1A)
>=1000 97 16.4
0-13200.0
<1000 493 83.6
What’s more, both male and female participants
are nearly 50%. More than three quarters of the
participants are older than 50 years old. For the
diagnosis of pancreatic cancer, about one-third of the
participants are patients.
In the regression part, we decided to select the model
with 5 predictors: Logit (diagnosis) = 0.65 +
0.0077Age + 0.057LYVE1 + 0.00033REG1B +
0.00011REG1A - 0.000074 (creatinine: REG1A).
The colon means the interactions between two
variables. The confusion matrix showed the accuracy
of prediction made by the model (Table 2). According
to the confusion matrix, the accuracy is 0.85 which
represents the proportion of correctly identified
samples. The sensitivity is 0.73 which represents the
proportion of actual positive samples identified
correctly. The precision is 0.82, which represents the
proportion of predict positive samples identified
correctly. The specificity is 0.91, which represents the
proportion of actual negative samples identified
correctly. These four factors indicate that our model
fits well with the practical condition.
Figure 1: The Boxplots of Associations Between Independent Variables X and Dependent Variable Y Diagnosis.
Detection of Urinary Biomarkers for Early Diagnosis of Pancreatic Cancer by Data Analysis
59

The boxplots were used to demonstrate all the independent
variables X visually and verify the positive skewed trend.
Table 2: Confusion matrix of the model.
Reference
predict 0 1
0 105 17
1 10 45
After fitting the best lambda, we create a
confusion matrix to evaluate the accuracy of our
modeling. Our data are divided into two parts in
which the training part contains 70 percent of the data
and the test part contains 30 percent. The reference
means the true value and the prediction represents the
value that the model predicted.
4 DISCUSSION
Pancreatic cancer is a highly malignant tumor of the
digestive system, and the molecular mechanism of its
occurrence and progression is still uncertain. In this
article, we are interested in the early detection,
prediction and diagnosis of pancreatic cancer. We
have analyzed and discussed again based on the data
of previous researchers, trying to explore which
factors are related to pancreatic cancer, but it still has
certain limitation.
We detect five urinary biomarkers in this study.
Lymphatic vessel endothelial hyaluronan receptor 1
(LYVE1) is a receptor that binds to both soluble and
immobilised hyaluronan. LYVE1 plays an important
role in lymphatic hyaluronan transport and tumor
metastasis. Regenerating family member 1 beta
(REG1B) belongs to a family of glycoproteins and
may promote regeneration of pancreatic islets.
Regenerating family member 1 alpha (REG1A) is a
protein which is highly similar to REG1B (Frappart
and Hofmann, 2020). Trefoil factor 1 (TFF1) is a 6.5
kDa secreted protein that belongs to a family of
gastrointestinal secretory peptides. It is expressed
predominantly in normal gastric mucosa and involved
in the regeneration and repair of urinary tract. TFF1
plays an important role in the development of cancer.
Creatinine is a protein which is a product of muscle
metabolism and is primarily cleared by the kidneys.
There are still many factors that are not included
in the database that can still affect the incidence and
prediction of PDAC to a large extent. Firstly, HER2
may play an important role in the occurrence and
development of pancreatic ductal adenocarcinoma in
elderly patients. The overexpression rate of HER2
may be related to gender, but its mechanism needs
further study (Ballehaninna and Chamberlain, 2012).
Secondly, we still have a lot to learn from in research
methods. In known studies, including drawing
survival curves based on the Kaplan-Meier method,
comparing survival time differences using Log-rank
test, multivariate Cox regression analysis to assess the
risk factors affecting patient survival, etc., can be
used to obtain better results. good result. In future
research, we will continue to work hard to bring better
research and results.
5 CONCLUSION
In our work, it can be concluded that age, LYVE1,
REG1A, REG1B, and the interaction between
creatinine and REG1A are the key predictors for the
diagnosis of pancreatic cancer. Their performances
are successfully validated by confusion matrix.
Furthermore, we plan to search for more clinical
datasets to verify our model and apply our logistic
regression approach to more available datasets of
cardiovascular diseases and other types of cancer.
REFERENCES
Adamska, A., Domenichini, A., & Falasca, M. (2017).
Pancreatic Ductal Adenocarcinoma: Current and
Evolving Therapies. International journal of molecular
sciences, 18(7), 1338.
https://doi.org/10.3390/ijms18071338
Arnold, M., Rutherford, M. J., Bardot, A., Ferlay, J.,
Andersson, T. M., Myklebust, T. Å., Tervonen, H.,
Thursfield, V., Ransom, D., Shack, L., Woods, R. R.,
Turner, D., Leonfellner, S., Ryan, S., Saint-Jacques, N.,
De, P., McClure, C., Ramanakumar, A. V., Stuart-
Panko, H., Engholm, G., … Bray, F. (2019). Progress
in cancer survival, mortality, and incidence in seven
high-income countries 1995-2014 (ICBP
SURVMARK-2): a population-based study. The
Lancet. Oncology, 20(11), 1493–
1505.https://doi.org/10.1016/S1470-2045(19)30456-5
Ballehaninna, U. K., & Chamberlain, R. S. (2012). The
clinical utility of serum CA 19-9 in the diagnosis,
prognosis and management of pancreatic
adenocarcinoma: An evidence based appraisal. Journal
of gastrointestinal oncology, 3(2), 105–119.
https://doi.org/10.3978/j.issn.2078-6891.2011.021
Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre,
L. A., & Jemal, A. (2018). Global cancer statistics
2018: GLOBOCAN estimates of incidence and
mortality worldwide for 36 cancers in 185
countries. CA: a cancer journal for clinicians, 68(6),
394–424. https://doi.org/10.3322/caac.21492
ICHIH 2022 - International Conference on Health Big Data and Intelligent Healthcare
60

Brezgyte, G., Shah, V., Jach, D., & Crnogorac-Jurcevic, T.
(2021). Non-Invasive Biomarkers for Earlier Detection
of Pancreatic Cancer-A Comprehensive Review.
Cancers, 13(11), 2722.
https://doi.org/10.3390/cancers13112722
Delanaye, P., Cavalier, E., & Pottel, H. (2017). Serum
Creatinine: Not So Simple!. Nephron, 136(4), 302–
308. https://doi.org/10.1159/000469669
Dinges, S.S., Hohm, A., Vandergrift, L.A. et al. Cancer
metabolomic markers in urine: evidence, techniques
and recommendations. Nat Rev Urol 16, 339–362
(2019). https://doi.org/10.1038/s41585-019-0185-3
Frappart, P. O., & Hofmann, T. G. (2020). Pancreatic
Ductal Adenocarcinoma (PDAC) Organoids: The
Shining Light at the End of the Tunnel for Drug
Response Prediction and Personalized
Medicine. Cancers, 12(10),
2750.https://doi.org/10.3390/cancers12102750
He, X. Y., & Yuan, Y. Z. (2014). Advances in pancreatic
cancer research: moving towards early detection. World
journal of gastroenterology, 20(32), 11241–11248.
https://doi.org/10.3748/wjg.v20.i32.11241
Makawita, S., Dimitromanolakis, A., Soosaipillai, A.,
Soleas, I., Chan, A., Gallinger, S., Haun, R. S., Blasutig,
I. M., & Diamandis, E. P. (2013). Validation of four
candidate pancreatic cancer serological biomarkers that
improve the performance of CA19.9. BMC cancer, 13,
404. https://doi.org/10.1186/1471-2407-13-404
Newton, J. L., Allen, A., Westley, B. R., & May, F. E.
(2000). The human trefoil peptide, TFF1, is present in
different molecular forms that are intimately associated
with mucus in normal stomach. Gut, 46(3), 312–320.
https://doi.org/10.1136/gut.46.3.312
Siegel, R. L., Miller, K. D., & Jemal, A. (2018). Cancer
statistics, 2018. CA: a cancer journal for
clinicians, 68(1), 7–
30.https://doi.org/10.3322/caac.21442
Zeng, S., Pöttler, M., Lan, B., Grützmann, R., Pilarsky, C.,
& Yang, H. (2019). Chemoresistance in Pancreatic
Cancer. International journal of molecular
sciences, 20(18), 4504.
https://doi.org/10.3390/ijms20184504
Detection of Urinary Biomarkers for Early Diagnosis of Pancreatic Cancer by Data Analysis
61
