
An Online Randomised Controlled Trial of the Positive Confiding to
Improve Emotional Wellbeing in Nurses during the COVID-19
Pandemic: A Protocol Study
Cui Lu
1,2,3 a
, Yi Tang
4,5 b
and Tianyong Chen
1,2,* c
1
Institute of Psychology, Chinese Academy of Sciences, Beijing, China
2
Department of Psychology, University of Chinese Academy of Sciences, Beijing, China
3
Emergency Department, TEDA Hospital, Tianjin, China
4
Department of Neurology, Xuan Wu Hospital, Beijing, China
5
National Center for Neurological Disorders, Capital Medical University, Beijing, China
Keywords: Online Intervention, Depression, Confiding, Well-Being, Emotion.
Abstract: In the time of COVID-19 pandemic, nurses suffering from stress and depression. Meanwhile, previous
studies indicated that the psychological well-being of medical staff benefited from confiding. However,
hitherto there is no experimental evidence supporting the implementation of confiding for nurses to
optimize their emotional outcome. Based on previous studies and the background of positive psychological,
we creates the “positive confiding intervention”, which means asking participants to consider the social
support or positive meaning gaining from expericence of confiding occupational hassles weekly. An online
two group randomised controlled trial design will be used in this study. We will use random grouping
method. A control group and a “positive confiding intervention” group will comprise 100 eligible
participants in total. The expected result is that the “positive confiding intervention” will significantly
improve nurses’ positive affect, interpersonal emotion regulation, perceived social support and cognitive
reappraisal, as well as decrease negative affect and depression.
1 INTRODUCTION
1
Amount of studies revealed that nurses face
extraordinary stresses in the medical environment
which can lead to choronic burnout (Cohen-Katz
2004, Happell 2013, Dall'Ora, 2020) and damage
nurses’ emotional wellbeing (Huang 2018, Boyle
2018, Boyle,2021), especially in the time of the
COVID-19 pandemic (Sanliturk 2021, Murat 2020).
Several systematic reviews reported that, in time of
the COVID-19 pandemic, quite a few of healthcare
workers’ suffering from stress, anxiety, depression
and sleep disturbance (Salari 2020a, Salari 2020b,
Sahebi 2021, Maqbali 2021, Marvaldi 2021).
Especially, it was reported that, during the time of the
COVID-19 epidemic, the prevalence of sleep
disturbance, anxiety and depression respectively
were 43%, 37% and 35% (Maqbali 2021). Therefore,
a
https://orcid.org/0000-0001-8943-2202
b
https://orcid.org/0000-0002-8052-065X
c
https://orcid.org/0000-0001-8948-4969
improving nurses’ emotional wellbeing will be an
important intervention goal, which would also benefit
patients’ caring (Di Muzio 2019, Giorgi 2018).
As a wide reach and low cost intervention with
high ecological validity, confiding to others maybe
an effective strategy for improving nurses’ emotional
wellbeing. It was found that, 79.3% medical staff
would confide their troubles to others (Liu 2020), and
comparing to confiding troubles to others, never
confiding troubles to others was associated with
medical staff’s self-reported anxiety (OR=2.2) and
depression (OR=2.0) under the COVID-19 epidemic
(Liu 2020). This result is consistent with a study
based on a big sample of 123,794 adults, which
revealed that the most protective factors for
depression are frequency of confiding in others
(adjusted OR=0.85) (Choi 2020). Previous studies
has indicated that, confiding is conducive to people’s
psychological well-being (Choi 2020, Slepian 2018,
Eldridge 2020, Pennebaker 1997), and medical staff
also benefits from confiding (Liu 2020). However,
hitherto there is no experimental evidence supporting
Lu, C., Tang, Y. and Chen, T.
An Online Randomised Controlled Trial of the Positive Confiding to Improve Emotional Wellbeing in Nurses during the COVID-19 Pandemic: A Protocol Study.
DOI: 10.5220/0011212200003438
In Proceedings of the 1st International Conference on Health Big Data and Intelligent Healthcare (ICHIH 2022), pages 37-42
ISBN: 978-989-758-596-8
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
37

the implementation of confiding for nurses to
optimize their emotional outcome.
Confiding means disclose one’s own personal
experience including emotions, attitudes or opinions,
to others. The need of confiding is universal. Humans
have the urge to to confide, and will release stress by
confiding (Eldridge 2020, Kant 1963, Smith 2002).
Confiding has remained an important component of
many forms of psychotherapy (Kelly 1996). A
previous study showed that, as for women, their
reasons for not confiding were unsupportive social
interactions and lack of social support, and they
tended to confide to their family and friends instead
of health workers, (Figueiredo 2010). In real life,
decisions of whether to confide hassles to others are
personal, and individuals pick and choose both what
information they share and with whom they share it.
There are several frameworks contextualizing
decisions of disclosure (or confiding), such as the
Communication Privacy Management Theory, the
Disclosure Processes Model, the Health Disclosure
Decision-Making Model and the Revelation Risk
Model. These frameworks above reflect the
agreement that the decision of whether to confide
private information depend on the advantages and
disadvantages (Afifi 2020). Many factors influence
the effects of confiding on well-being, including “the
type of relationship, the valence of the stressor, the
response to the disclosure, and the meaning
generated from the disclosure” (Slepian 2018, Afifi
2020). In literature (Eldridge 2020, Pennebaker 1997,
Lu 2019, Howell 2009), several positive meanings of
confiding were mentioned: 1) confiding helps to
form and develop interpersonal relationships; 2)
people can benefit from confiding by co-regulating
emotional experiences; 3) confiding can help people
co-construct meanings, as well as affirm, challenge
and develop their identity; 4) future social support
can be positively shaped; 5) By confiding, people
may could receive others’ concrete aid; 6) Confiding
may help people get more message about others’
feels about similar things, and people can compare
and learn others’ emotion regulation strategy.
In short, the main benefit of confiding is helping
confider receive social support. According to Kahn
and Antonucci (Kahn 1980), “there are three types of
social support or support exchanges: aid, affect, and
affirmation”. Aid means tangible assistance,
including providing money or sick care, information
and advice. Affect means emotional support,
including perceived love, care, fondness or affection
of others. Finally, affirmation is the intangible
communication to another convoy member that
members share or respect the same values, goals, and
aspirations. Additionally, many studies indicated
that, perceived support is more helpful than received
support (Santini 2015). So, it is important that people
would perceive the social support they can benefit
from confiding, which is an active and positive
behavioral model. As a recent study reported that,
confiding predicts higher well-being through framing
confiding as a source of social support (Slepian
2018).
From the perspective of Interpersonal Emotion
Regulation, Rimé (2007) argues that emotional
episodes are virtually always followed by long-term
congnitive and social effects, and particularly
individul emtional experiences elicit important social
behaviors by which the actor informs his or her
socical partner of what happened and shares with
them related thoughts and feelings. It was expounded
that (Rimé 2007), people who share positive
emotions may make their positive effect and social
bonds improve. For negative emotional experience,
people would tolerate the reexperience involved in
social sharing because of the final benefit it provides
them (Rimé 2007). It was concluded that there are
three classes of regulation needs, including
sociaffective needs, congnitive needs and action
needs (Rimé 2007). It was reported that the reasons
for sharing negative emotion was socioaffective
motives, including receiving support, validation and
comfort (Rimé 2007). As an integrative review
argues that interpersonal emotion regulation may
decrease depression through improving perceived
social support (Marroquín 2011).
Above all, similar to positive psychology’s use of
research on the “Three Good Things Intervention”
and the “Meaning-Oriented Interventions” (Parks
2004), we created the “positive confiding
intervention”, which means asking partcipants to
consider the social support or positive meaning
gaining from expericence of confiding occupational
hassles and record the positive meanings gaining
from the most satisfied confiding experiences
weekly. In light of the Handbook of Positive
Psychological Interventions, by participating online
positive psychological interventions may make
people be more willing to manage of their own heath,
because online interventions provide methods to
enlighten their behaviour, thinking, and interpersonal
interaction (Parks 2004). Therefore, we are going to
conduct the “positive confiding intervention” by
online techniques.
ICHIH 2022 - International Conference on Health Big Data and Intelligent Healthcare
38
2 STUDY PURPOSES
This study aims to test the efficacy of our created
“positive confiding intervention” to improve nurses’
emotional wellbeing, including improving nurses’
positive affect, interpersonal emotion regulation,
perceived social support and cognitive reappraisal,
as well as decrease negative affect and depression.
3 METHODS/DESIGN
3.1 Design and Participants
The study has received ethical approval from the
Ethics Committee of the Institute of Psychology,
Chinese Academy of Sciences. A two group
randomised controlled trial design will be used in
this study. The G*Power 3.1 (Faul 2007) was used
to estimate the required number of participants (see
Table 1). As seen in Table 1, the required overall
number of participants is 45, which can guarantee
enough sample size for detecting an effect.
Table 1 Sample size estimated by G*Power 3.1.
Input paramete
r
s Output
p
aramete
r
s
Effect size
d
0.5
α err
p
rob 0.05
Power (1-β err prob) 0.95
Number of
g
rou
p
s 2
Noncentrality parameter
λ
3.35
t value 1.68
d
f 44
Total sam
p
le size 45
p
owe
r
0.95
We decide to improve the number of participants
to 100 participants (see Table 2). Nurses aged 18-55
years old, working in domestic public hospitals in
China, won't leave this job during the study period.
Table 2 Inclusion/exclusion criteria.
Inclusion criteria Exclusion criteria
Nures aged between
18 and 60 years ol
d
Cannot grantee completing
this stud
y
Working in domestic
public hospitals in
China
Participating in other
similar psychological
studies
Won't leave this job
during the study
p
erio
d
Taking a long vacation
during the study period
Do not need to take care of
patients during working
time
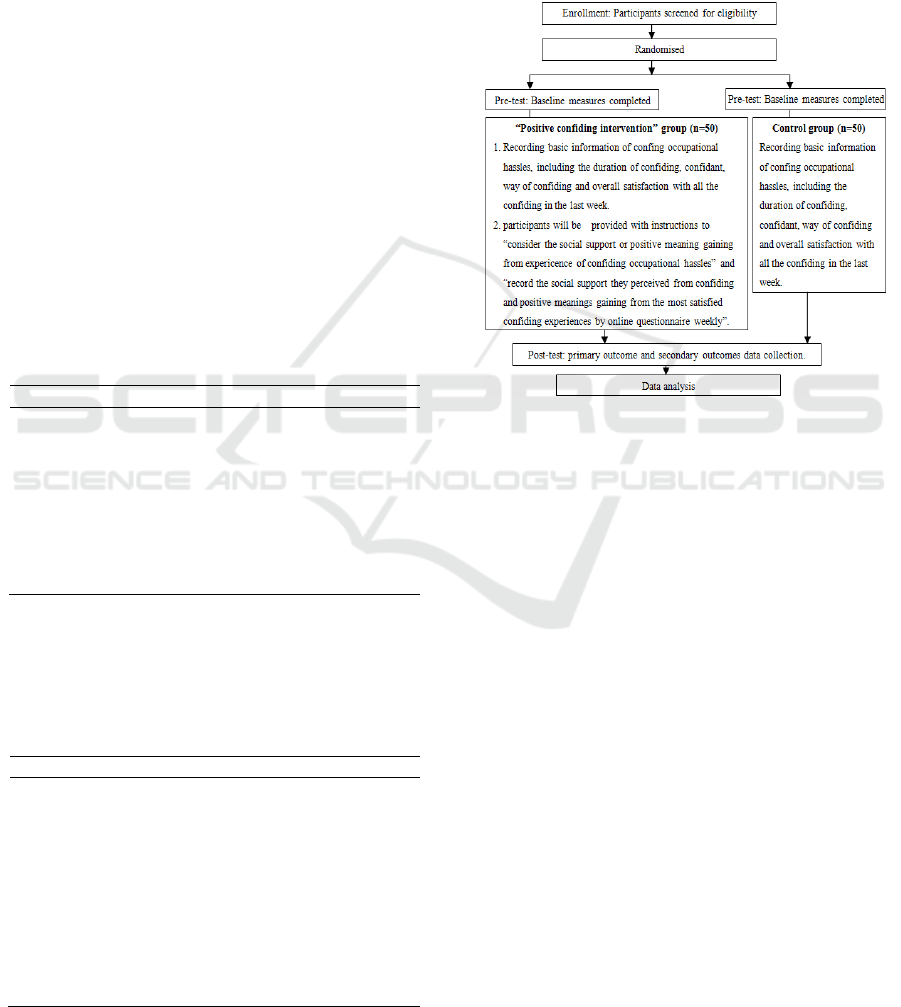
3.2 Randomisation and Allocation
After completing all the baseline measures, all the
participants will be randomly grouped, which means
all the objects will participate in the “positive
confiding intervention” group or control group
randomly (see Figure 1). We will use a computer
program to generate an allocation sequence, which
will be used for random allocation.
Figure 1: Flow chart of trial procedure.
In the “positive confiding intervention” group,
participants will be provided with instructions to
“consider the social support or positive meaning
gaining from expericence of confiding occupational
hassles” and record the social support they perceived
from confiding, and record positive meanings
gaining from the most satisfied confiding
experiences by online questionnaire weekly. In the
online questionnaire, participants will be asked to
think about how much social support[28] or positive
meaning they have perceived, including: 1) concrete
help for solving problems, advice for solving
problems and information helping promote
understanding; 2) emotional support including
enhancing eomtional connection, helping improve
positive emotion or decreasing negative emotion, 3)
feeling validated or supported, promote understand
or endorse of self and increase affirmation of
professional value. In the online questionnaire for
control group, only the basic information of
confiding occupational hassles will be involved,
including the duration of confiding, confidant, ways
of confiding and overall satisfaction with all the
confiding in the last week, the same as in the
“positive confiding intervention” group.
An Online Randomised Controlled Trial of the Positive Confiding to Improve Emotional Wellbeing in Nurses during the COVID-19
Pandemic: A Protocol Study
39
4 DATA COLLECTION AND
OUTCOME MEASURES
4.1 Background Information
Demographic data, socioeconomic status,
occupational status and health condition will be
collected before intervention. Demographic data
includes age, gender, marital status, and nuber of
childern. Socioeconomic status includes education
background and if there is difficulty in paying bills,
saving money, having enough pocket money every
month. Occupational status includes working years
as a nurse, professional title and whether participate
work in shift work. Health condition includes
perceived overall health condition, perceived overall
sleep quality in the past one month.
4.2 The Primary Outcome Measures
The Patient Health Questionnaire (PHQ) is used to
assesse depression, consists 9 items and rated with
four-point degrees according to symptom in the past
two weeks (Kroenke 2004).
The simple positive and negative affect scale
(PANAS-S) is a 12-item likert-style (4-point) rating
scale that assesses affect by situation or persistent
affect. For each item, a four-point degrees of the
scale was used to assess the frequency arise in the
past week (0=never; 1= once in a while; 2=
sometimes; 3= often; 4=always). Thereinto, 8 items
are express positive affect, and 4 items express
negative affect. Higher scores means more positive
or negative affect (Kahneman 2004).
Nurses Work Stressors Scale (NWSS) is a is a
35-item likert-style (4-point) rating scale that
assesses nurses’ source of occupational stress.
Higher scores means more work stress (Li 2000).
4.3 The Secondary Outcome Measures
The Interpersonal emotion regulation Questionaire
(IERQ) consists 20 items, which use a 5-point likert-
style rating scale to assesse how people regulate
their emotions by using others (Hofmann 2016). For
each item, a five-point degrees of the scale was used.
The Multidimensional Scale of Perceived Social
Support (MSPSS) consists 12 items, which measures
how many social support people can feel. For each
item, a 7-point degrees of the scale was used.
(Dambi 2018).
The emotion regulation questionnaire (ERQ) is
used to assesse cognitive reappraisal and expressive
suppression, which consists 10 items. For each item,
a 7-point degrees of the scale was used. (Gross
2003).
The Table 3 shows all the measures used in this
study, and the time-points of measurement have
been presented too.
5 DATA ANALYSES
5.1 Primary Analyses
We will use descriptive statistics to summarize the
characteristics of all the participants, and analyse the
primary and secondary outcome measures by using t
test with a between subject factor of intervention
condition and a within-subject. Besides, we will use
effect sizes (Cohen’s d) (Cohen 1988) to illustrate
differences in all the measured results between the
before and after the intervention.
Table 3 Timeline for data collection.
Measure-
ment
time-
point
Measures
PHQ-9 PANAS IERQ
MSP
SS
NW
SS
Basline
× × × × ×
1 weeks
×
2 weeks
× ×
3 weeks
×
4 weeks
× ×
5 weeks
×
6 weeks
× ×
7 weeks
×
8 weeks
× × × × ×
6 CONCLUSIONS
Accumulating evidence indicated that nurses
confronted a lot of stress, anxiety, depression
(Salari
2020a, Salari 2020b, Sahebi 2021, Maqbali 2021,
Marvaldi 2021)
. As an important component of many
forms of psychotherapy (Kelly 1996), confiding is
also highly common among laypersons. However,
hitherto there is no experimental evidence
supporting the implementation of confiding for
nurses to optimize their emotional outcome.
Empirical research has highlighted the harm of
repress the need of confiding, as well as a lot of
benefits of confiding. However, some harm of
ICHIH 2022 - International Conference on Health Big Data and Intelligent Healthcare
40

confiding also has been put forward (Kelly 1996,
Slepian 2018). To explore the effective model of
confiding, this study creates the “positive confiding
intervention” based on previous studies and will
conduct an online randomised controlled trial to
exam its effect for promoting emotional wellbeing
by comparing the “positive confiding intervention”
with control group. The expected result is that the
“positive confiding intervention” will significantly
improve nurses’ positive affect, interpersonal
emotion regulation, perceived social support and
cognitive reappraisal, as well as decrease negative
affect and depression. will significantly improve
nurses’ positive affect, decrease negative affect and
depression, and the mediating variables of these
effect will be interpersonal emotion regulation,
perceived social support and cognitive reappraisal.
This study will build on suggestions from
previous studies that confiding tends to promote
mental well-being. Our study firstly developed the
“positive confiding intervention” as an effective
confiding for nurses to improve emotional wellbeing
innovatively, which is a wide rich and low cost
intervention with high ecological validity. By
examing the effect of this “positive confiding
intervention” on nurses, this study would further
discuss the precise mechanism through how this
“positive confiding intervention” promots nurses’s
emotional wellbeing. This study will contribute to
build an effective psychotherapy method applying to
nurses. In addition, this study will encourage people
to positively confiding, which will also contribute to
the study of social support from the perpective of
positvely constructing social support.
FUNDING
The National Key Research and Development
Program of China supports this study
(2017YFC1310102).
REFERENCES
Afifi, W.A., Afifi, T.D. (2020). The relative impacts of
disclosure and secrecy: the role of (perceived) target
response. Current Opinion in Psychology. 2020,31:94-
98.
Boyle, D.A., Bush, N.J. (2018). Reflections on the
Emotional Hazards of Pediatric Oncology Nursing:
Four Decades of Perspectives and Potential. Journal of
Pediatric Nursing, 40,63-73.
Boyle, D.A., Steinheiser, M.M. (2021). Emotional
Hazards of Nurses' Work: A Macro Perspective for
Change and a Micro Framework for Intervention
Planning. Journal of Infusion Nursing, 2(44),78-93.
Cohen-Katz, J., Wiley, S.D., Capuano, T., et al. (2004).
The Effects of Mindfulness-Based Stress Reduction on
Nurse Stress and Burnout: A Quantitative and
Qualitative Study. Holistic Nursing Practice.
18(6),302-308.
Choi, K.W., Stein, M.B., Nishimi, K.M., et al. (2020). An
Exposure-Wide and Mendelian Randomization
Approach to Identifying Modifiable Factors for the
Prevention of Depression. Am J Psychiatry.
177(10),944-954.
Dall'Ora, C., Ball, J., Reinius, M., et al. (2020). Burnout in
nursing: a theoretical review. Human Resources for
Health. 18(1),41.
Di Muzio, M., Dionisi. S., Di Simone, E. et al (2019). Can
nurses' shift work jeopardize the patient safety? A
systematic review. Eur Rev Med Pharmacol Sci.
23(10),4507-4519.
Dambi, J.M., Corten, L., Chiwaridzo, M. (2018). A
systematic review of the psychometric properties of
the cross-cultural translations and adaptations of the
Multidimensional Perceived Social Support Scale
(MSPSS). Health Qual Life Outcomes.16(1):80.
Eldridge, J., John, M., Gleeson, K. (2020). Confiding in
others: exploring the experiences of young people who
have been in care. Adoption & Fostering. 44(2),156-
172.
Figueiredo, M.I., Fries, E., Ingram, K.M. (2010). The role
of disclosure patterns and unsupportive social
interactions in the well-being of breast cancer patients.
Psycho-Oncology. 13(2),96-105.
Faul, F., Erdfelder, E., Lang, A.G. (2007). G*Power 3: a
flexible statistical power analysis program for the
social, behavioral, and biomedical sciences. Behav
Res Methods. 39(2),175–191.
Giorgi, F., Mattei, A., Notarnicola, I., et al. (2018). Can
sleep quality and burnout affect the job performance of
shift-work nurses? A hospital cross-sectional study. J
Adv Nurs. 74(3),698-708.
Gross, J.J., John, O,P. (2003). Individual differences in
two emotion regulation processes: implications for
affect, relationships, and well-being. Journal of
Personality and Social Psychology. 85(2),348-362.
Cohen, J. 1988. Statistical power analysis for the
behavioral sciences. Lawrence Erlbaum Associates.
New Jersey.
Happell, B., Dwyer, T., Reid-Searl, K., et al. (2013).
Nurses and stress: recognizing causes and seeking
solutions. Journal of Nursing Management. 21(4),638-
647.
Huang, CL., Wu, MP., Ho, CH., et al. (2018). Risks of
treated anxiety, depression, and insomnia among
nurses: A nationwide longitudinal cohort study. PloS
one.13(9), e0204224.
Howell, E.A., Mora, P.A., DiBonaventura, M.D. (2009).
Modifiable factors associated with changes in
An Online Randomised Controlled Trial of the Positive Confiding to Improve Emotional Wellbeing in Nurses during the COVID-19
Pandemic: A Protocol Study
41

postpartum depressive symptoms. Arch Women’s
Ment Health. 12, 113-120.
Hofmann, S.G., Carpenter, J.K., Curtiss, J. (2016).
Interpersonal Emotion Regulation Questionnaire
(IERQ): Scale Development and Psychometric
Characteristics. Cognit Ther Res.40(3),341-356.
Kelly, A.E., Mckillop, K.J. (1996). Consequences of
revealing personal secrets. Psychological Bulletin.
120(3),450-465.
Kant, I., 1963. Lectures on Ethics. Indianapolis, Hackett.
Kroenke, K., Spitzer, R.L., Williams, J.B. (2004). The
PHQ-9: validity of a brief depression severity
measure. J Gen Intern Med.16, 606-13.
Kahneman, D., Krueger, A.B., Schkade, D.A. (2004). A
Survey Method for Characterizing Daily Life
Experience: The Day Reconstruction Method. Science.
306, 1776-1780.
Kahn. R.L., Antonucci, T.C. 1980. Convoys over the life
course: attachment, roles, and social support. Life-
span development and behavior. 3.
Liu, Y., Chen, H., Zhang, N., et al. (2020). Anxiety and
depression symptoms of medical staff under COVID-
19 epidemic in China. J Affect Disord. 278,144-148.
Lu, Y., Pan, T., Deng, S. (2019). What Drives Patients
Affected by Depression to Share in Online Depression
Communities? A Social Capital Perspective.
Healthcare (Basel).7(4),133.
Li, X.M., Liu, Y.J. (2000). Job Stressors and Burnout
among Staff Nurses. Chinese Journal of Nursing.
35(11),645-649.
Maqbali, M.A., Sinani, M.A., Al-Lenjawi, B. (2021).
Prevalence of stress, depression, anxiety and sleep
disturbance among nurses during the COVID-19
pandemic: A systematic review and meta-analysis.
Journal of Psychosomatic Research. 141,110343.
Marvaldi. M., Mallet. J., Dubertret, C., et al. (2021).
Anxiety, depression, trauma-related, and sleep
disorders among healthcare workers during the
COVID-19 pandemic: A systematic review and meta-
analysis. Neurosci Biobehav Rev. 126,252-264.
Murat, M., Köse. S., Savaşer, S. (2020). Determination of
stress, depression and burnout levels of front-line
nurses during the COVID-19 pandemic. Int J Ment
Health Nurs. 30(2),533-543.
Marroquín, B. (2011). Interpersonal emotion regulation as
a mechanism of social support in depression. Clinical
Psychology Review. 31(8), 1276-1290.
Pennebaker, J.W., 1997.Opening Up: The healing power
of emotional expression. New York, Guilford Press.
Parks, A.C., Schueller, S.M. 2004. The Wiley Blackwell
Handbook of Positive Psychological Interventions.
John Wiley & Sons.
Rimé, B. 2007. Interpersonal emotion regulation.
Handbook of Emotion Regulation. The Guilford Press.
London.
Sanliturk, D. (2021). Perceived and sources of
occupational stress in intensive care nurses during the
covid-19 pandemic. Intensive and Critical Care
Nursing. 67,103-107.
Salari, N., Khazaie, H., Hosseinian-Far, A., et al. (2020a).
The prevalence of stress, anxiety and depression
within front-line healthcare workers caring for
COVID-19 patients: a systematic review and meta-
regression. Hum Resour Health.18(1),100.
Salari, N., Khazaie, H., Hosseinian-Far, A., et al. (2020b).
The prevalence of sleep disturbances among
physicians and nurses facing the COVID-19 patients: a
systematic review and meta-analysis. Global
Health.16(1),92.
Sahebi, A., Nejati, B., Moayedi, S., et al. (2021). The
prevalence of anxiety and depression among
healthcare workers during the COVID-19 pandemic:
An umbrella review of meta-analyses. Progress in
Neuro-Psychopharmacology and Biological
Psychiatry. 107,110247.
Slepian, M.L, Moulton-Tetlock E (2018). Confiding
Secrets and Well-Being. Social Psychological and
Personality Science, 10(4),194855061876506.
Smith, A. 2002. The Theory of Moral Sentiments. New
York, Cambridge University Press.
Santini, Z.I., Koyanagi, A., Tyrovolas, S., et al. (2015).
The association between social relationships and
depression: A systematic review. Journal of Affective
Disorders.175,53-65.
ICHIH 2022 - International Conference on Health Big Data and Intelligent Healthcare
42
