
Biomarker Study of Cholangiocarcinoma
Qinyi Cai
Medical Laboratory Technology, Chengdu University of TCM, Chengdu, 611137, China
Keywords:
Cholangiocarcinoma, Diagnostic Method, Biomarker.
Abstract: Cholangiocarcinoma is a malignant tumor originating from the epithelial cells of the bile duct mucosa in the
biliary tract. The incidence of cholangiocarcinoma is increasing day by day. The current diagnostic
technology cannot meet the needs of early diagnosis and the prognosis is poor, resulting in high mortality.
Therefore, cholangiocarcinoma is known as the "king of cancer". How to effectively diagnose
cholangiocarcinoma as soon as possible is of great significance for prolonging the life of patients with
cholangiocarcinoma. Based on the diagnosis and treatment of cholangiocarcinoma, this paper summarizes
the existing research results and clinical methods, reviews the current research status of biomarkers for
cholangiocarcinoma, and looks into the future development of biomarkers.
1 INTRODUCTION
Cholangiocarcinoma is a kind of malignant tumor
originating from epithelial cells, which can be
divided into intrahepatic cholangiocarcinoma and
extrahepatic cholangiocarcinoma according to the
site of the disease. Extrahepatic cholangiocarcinoma
can be divided into hilar cholangiocarcinoma and
distal cholangiocarcinoma. Cholangiocarcinoma
patient inchoate does not have special symptom
commonly, abdominal unwell ache, icteric is this
disease the most common symptom, as the
development of the illness, may appear temperature
rises, nausea and vomiting, weak and weak, serious
when the patient is immersed in coma.
Carbohydrate antigen 19-9 (CAI9-9) and
carcinoembryonic antigen (CEA) is the most widely
studied of CCA molecular markers, but its
diagnostic value is not high. The current diagnostic
methods for cholangiocarcinoma include imaging
examination, endoscopy, histological examination
and pathological examination, and serum marker
examination, but these examinations cannot meet the
diagnostic needs. There is still no fully effective
biomarker for early detection of
cholangiocarcinoma. For these reasons,
cholangiocarcinoma is usually diagnosed at
advanced stage. And the survival rate of patients
with advanced bile duct carcinoma is less than 5%.
Now, the treatment methods for
cholangiocarcinoma mainly include surgical
resection of tumor focus, liver transplantation and
adjuvant therapy (radiotherapy and chemotherapy).
Currently, targeted therapy and immunotherapy in
cancer treatment cannot be effectively promoted due
to the research dilemma of biomarkers for bile duct
cancer. Based on the current research status of
cholangiocarcinoma, we clearly know that the
discovery of biomarkers that can be used for
screening diagnosis is of great significance for the
treatment of cholangiocarcinoma. Effective
biomarkers can undoubtedly save the lives of more
patients with cholangiocarcinoma.
2 EPIDEMIOLOGY
Cholangiocarcinoma accounts for about 3% of all
digestive tract tumors, with a peak age of 70 years
and slightly more men than women. ICC and eCC
have different epidemiological characteristics. The
incidence and mortality of CCA are on the rise in
western countries. The incidence and mortality of
ICC showed significant gender and ethnic
differences. The incidence of ICC is 15 times higher
in men than in women. The incidence of yellow
people is 20 times higher than that of white and
black people. The three subtypes of CCA also have
different epidemiological trends. Over the past few
decades, the age-standardized incidence of iCC has
steadily increased in most parts of the world, while
the age-standardized incidence of eCC has declined.
288
Cai, Q.
Biomarker Study of Cholangiocarcinoma.
DOI: 10.5220/0011201800003443
In Proceedings of the 4th International Conference on Biomedical Engineering and Bioinformatics (ICBEB 2022), pages 288-294
ISBN: 978-989-758-595-1
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
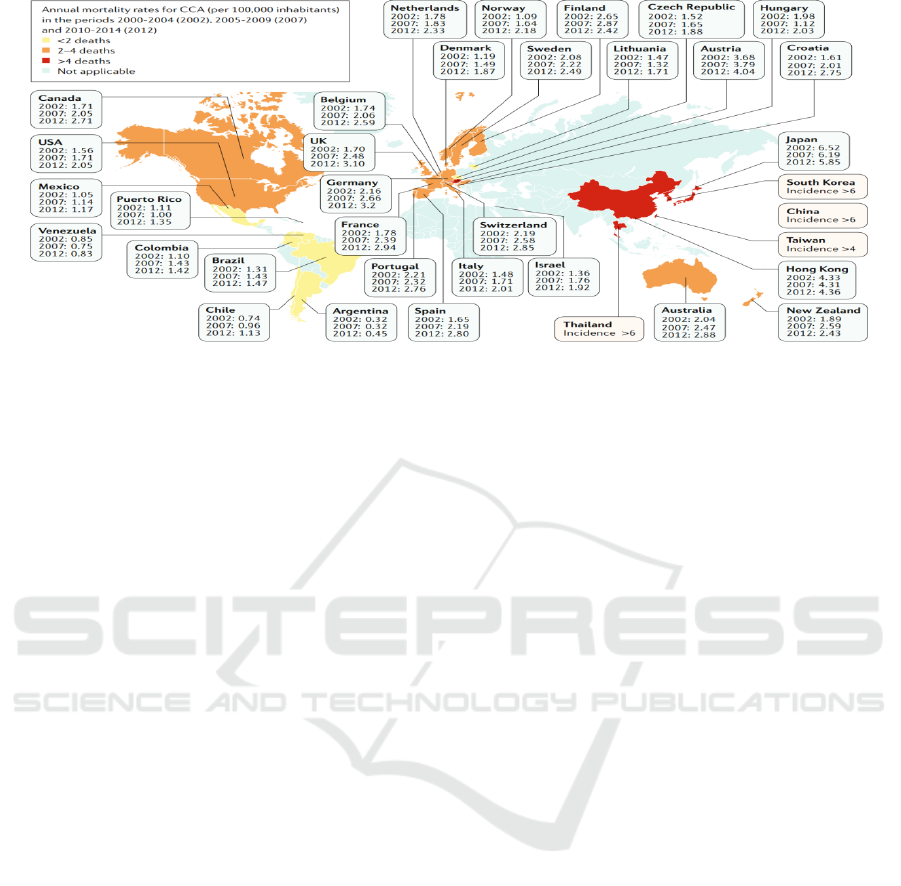
Figure 1: Mortality of cholangiocarcinoma worldwide.
3 SCREENING AND DIAGNOSIS
3.1 Imaging Examination Methods
At present, the commonly used imaging examination
methods for the diagnosis of extrahepatic
cholangiocarcinoma include ultrasound (US),
computed tomography (CT), magnetic resonance
imaging (MRI or MRCP), percutaneous transhepatic
puncture cholangiography (PTC), endoscopic
retrograde cholangiography (ERCP).
3.1.1 Abdominal B-Type Ultrasound
Abdominal B-mode ultrasonography is the first
choice in the diagnosis of cholangiocarcinoma
because it is noninvasive, simple and economical.
However, the accuracy of abdominal ultrasound in
the diagnosis of cholangiocarcinoma varies greatly.
Hennedige et al. showed that the sensitivity and
specificity of B-ultrasound in the diagnosis of
extrahepatic cholangiocarcinoma were 89% and
80% ~ 95% respectively, which are mostly used as
routine screening for cholangiocarcinoma.
3.1.2 CT Examination
CT is one of the traditional methods for the
examination of bile duct diseases, which can show
the location, scope and invasion of surrounding
organs more comprehensively. The accuracy of
multi-slice spiral CT (MDCT) in the diagnosis of
extrahepatic cholangiocarcinoma can reach 78.6% ~
92.3%, and the sensitivity and specificity of the
diagnosis of cholangiocarcinoma can reach 84%.
3.1.3 MRI
MRI examination is currently the gold standard for
non-invasive examination of hepatobiliary system
diseases. It is a safe and effective non-invasive
imaging technique. A number of studies have shown
that MRCP has a high sensitivity for extrahepatic
cholangiocarcinoma and can identify the lesion site.
3.1.4 ERCP and PTC
ERCP and PTC, as direct cholangiography methods,
have good spatial resolution and can accurately
understand the location and scope of the tumor.
ERCP has an accuracy of 75% in diagnosing
cholangiocarcinoma with duct obstruction. Yu et al.
showed that preoperative PTCD combined with bile
reperfusion can improve the resection rate and safety
of patients with hilar cholangiocarcinoma.
3.1.5 Other Imaging Examinations
Positron emission computed tomography (PET) is a
noninvasive imaging method, which has obvious
advantages in early detection of malignant lesions
and monitoring of recurrence and metastasis. Park et
al. showed that whether distant lymph node
metastasis was detected by preoperative PET/CT
was positively correlated with the recurrence rate of
patients with cholangiocarcinoma one year after
surgery. Confocal laser microendoscopy (CLE) was
initially used for the diagnosis of gastrointestinal
diseases, and its subtype pCLE was used for the
examination of diseases of the pancreatic bile duct
system due to its good flexibility. Giovannini et al.
confirmed the feasibility of pCLE for the diagnosis
Biomarker Study of Cholangiocarcinoma
289

of bile duct obstruction with a sensitivity and
specificity of 83% and 75%, respectively.
3.2 Endoscopy
3.2.1 Endoscopic Ultrasonography (EUS)
EUS currently plays an important role in diagnosing
cholangiocarcinoma. Mohamadnejad et al. found
that EUS was relatively more sensitive to the
diagnosis of cholangiocarcinoma, with a detection
rate up to 94%.
3.2.2 Duodenoscopic Intrabile Duct
Ultrasound (IDUS)
IDUS has more advantages than EUS in the
diagnosis of cholangiocarcinoma, which can be used
to determine the location of cholangiocarcinoma and
evaluate the possibility of its resection. Compared
with ERCP, IDUS has obvious advantages in
sensitivity and accuracy.
3.3 Serum Tumor Markers
3.3.1 A Separate Test
Ca19-9 is the most studied diagnostic and prognostic
indicator of cholangiocarcinoma, and its level is
related to the development stage of the disease.
Coelho et al. showed that CA19-9 level ≥103U/L
can be used as a predictor of survival and metastasis
in patients with cholangiocarcinoma. Hu et al.
showed that serum CA19-9 could be used as an
independent risk factor for resectable hilar
cholangiocarcinoma. It is believed that CEA can
also be used to guide clinical diagnosis of
cholangiocarcinoma. Tang et al. proposed that the
diagnostic sensitivity of CEA in extrahepatic
cholangiocarcinoma was affected by the tumor
location, with a high sensitivity to the middle
cholangiocarcinoma, while the sensitivity to the
distal cholangiocarcinoma was only 15.4%. CEA
cannot be used in the diagnosis of
cholangiocarcinoma alone, but is usually used as an
indicator to observe the clinical effect and
postoperative follow-up.
3.3.2 The Joint Detection
In view of the limitations of single application of
CA19-9, CA125 and CEA, clinicians advocate the
combination of multiple tumor markers to reduce the
rate of missed diagnosis. Combined detection of ≥2
tumor markers can improve the sensitivity and
specificity of diagnosis. Franco et al. found that the
combined detection of CEA, CA19-9, cytokeratin 19
fragment and matrix metalloproteinase-7 can be
used for preliminary screening of
cholangiocarcinoma.
3.3.3 microRNAs
In recent years, miRNAs have received extensive
attention due to their biostability.
Wang et al. found that serum Mir-26a
concentration in patients with cholangiocarcinoma
was significantly higher than that in healthy controls
(P < 0.01), which was associated with clinical stage,
distant metastasis, differentiation state and low
survival rate of cholangiocarcinoma, and was an
independent prognostic indicator of
cholangiocarcinoma, and provided a new therapeutic
target for cholangiocarcinoma.
Deng et al. also showed that serum Mir-29A
level is associated with the progression of
cholangiocarcinoma, which is an independent
prognostic factor for patients with
cholangiocarcinoma and can be used as a new
biomarker to evaluate the prognosis of patients with
cholangiocarcinoma.
Cheng et al. found that with the decrease of
serum Mir-106A concentration, the risk of lymph
node metastasis increased, and its expression level
could serve as a strong prognostic indicator for
patients with cholangiocarcinoma.
3.3.4 Other Tumor Markers
Specific modification of n-glycosylation of
glycoprotein is recognized as a key component in
cancer progression. Wang et al. found that
hematoqing n-glycosylation can be used as a new
tumor marker for diagnosis of extrahepatic
cholangiocarcinoma. Its diagnostic value was higher
than that of CA19-9. Okada et al. found that S-p53-
ABS can be used for diagnosis of extrahepatic
cholangiocarcinoma. In addition, studies showed
that MUC5AC in blood serum could be used as a
surrogate indicator for the diagnosis of
cholangiocarcinoma.
Histopathological Examination
3.4.1 Cytological Examination
ERCP can be used for bile duct biopsy, brush
examination and exfoliated cell examination by
endoscopy to obtain pathological data. Korc et al.
showed that the specificity of brush cytology was
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
290

close to 100%, and the sensitivity was 30%-57%.
Endoscopic ultrasound fine needle aspiration (EUS-
FNA) is another method for obtaining extrahepatic
bile duct cancer cells.
3.4.2 Biopsy Histology
Histological diagnosis is highly specific. Chen et al.
showed that the sensitivity and specificity of
extrahepatic bile duct biopsy were 53.85% and
100.00%, respectively. In summary, there are many
studies on the diagnosis of extrahepatic
cholangiocarcinoma in recent years. However, the
diagnosis and treatment of extrahepatic
cholangiocarcinoma is still a complex problem at the
present stage. How to improve its diagnosis and
treatment will be the focus of future research.
4 BIOMARKER
CLASSIFICATION OF
CHOLANGIOCARCINOMA
4.1 Circulating Nucleic Acids
MiRNA is a kind of tiny non-coding RNA that plays
an important role in regulating protein expression.
MiRNA has been confirmed to be involved in the
development and metastasis of many human
cancers. Because mirnas are common in the early
stage of some cancers, they are often used as
diagnostic indicators of some cancers. Studies have
shown that the contents of mirnas (Mir-21, Mir-34c,
Mir-200b and Mir-221) in serum of iCCA patients
are 2.18-3.79 times higher than those in non-tumor
cells. In addition, serum Mir-483-p and Mir-222,
Mir-26a and Mir-150 have certain diagnostic value
for CCA.
Chen et al. found that mir-21, Mir-141 and Mir-
200b were highly expressed in malignant bile duct
cancer cells, and the sensitivity of cancer cells to
chemotherapy drug gemcitabine was increased by
inhibiting the expression of Mir-21, and the
potential tumor suppressor target gene PTEN of
Mir-21 was screened out through experiments. In
the study of Mir-21, Selaru et al. found that TMP3
protein is a tumor suppressor gene that promotes
apoptosis of cancer cells and inhibits invasion and
metastasis of cancer cells, and also found the
relationship between Mir-21 and TMP3 protein:
inhibition of cancer cell growth means inhibition of
Mir-21 and enhancement of negative regulatory
relationship of TMP3 protein. You Hao et al.
obtained a tumor suppressor gene, Maspin, and
found that maspin was related to tumor size and
invasion degree in cholangiocarcinoma, and its
expression could be increased by inhibiting Mir-21.
Zeng et al. found that the overexpression of Mir-124
inhibits the migration and invasion of cancer cells in
intrahepatic cholangiocarcinoma.
Long non-coding RNA (lncRNA) and circRNA
(circRNA). Xu et al. found that inhibition of
SPRY4-IT1 expression could weaken the
proliferation, metastasis and invasion ability of
HuCCT1 and RBE cells in cholangiocarcinoma.
Wang et al. found that overexpression of
lncRNADANCR could promote proliferation,
metastasis and invasion of bile duct cancer cells.
XingLC et al. found through experimental studies
that low expression of hsa-circ-0001649 can
enhance the ability of cancer cell proliferation,
metastasis and invasion. Lu and Fang found that the
expression of CIRC-SmarCA5 was negatively
correlated with TNM staging of cholangiocarcinoma
and abnormal status of CA199.
CfDNA is a section of DNA that can be released
into the blood by physiological or pathological
mechanisms. In malignant tumors, cfDNA is mainly
derived from apoptotic and necrotic tumor cells,
which are characterized by genetic and epigenetic
abnormalities, such as point mutation, loss of
heterozygosis (LOH), microsatellite instability
(MSI) and DNA methylation, etc.
Dicer, one of the RNase iii endoribonuccinases,
plays an important role in regulating the methylation
of CpG islands in mammalian cancer cells. Cheng et
al. found through experiments that Dicer promoted
DNA methylation of SFRP1 promoter, thus leading
to proliferation and invasion of bile duct cancer
cells. Liu et al. conducted a comprehensive analysis
of tissue samples from 152 patients with
cholangiocarcinoma, and found that GATA5 inhibits
the proliferation and metastasis of
cholangiocarcinoma by inactivating Wnt/β -catenin
signal transduction.
4.2 Other Markers
4.2.1 In Serum
IL-6 is a 184-amino acid pleiotropic cytokine that
promotes acute inflammatory response. Serum
levels of L-6 cannot be measured under normal
circumstances, but serum IL-6 is significantly
elevated in hepatocellular carcinoma and
cholangiocarcinoma. The positive judgment value of
IL-6 as a serum marker was 83.3% for
Biomarker Study of Cholangiocarcinoma
291

cholangiocarcinoma and 81.3% for hepatocellular
carcinoma. The sensitivity and specificity of IL-6
increased in cholangiocarcinoma was 100% and
91.4%. The serum IL-6 value of patients with
cholangiocarcinoma was positively correlated with
tumor load, and the mean and median value of il-6
activity were significantly higher than those of other
tumors. IL-6 is one of the ideal tumor markers for
the diagnosis of cholangiocarcinoma.
Frampton et al. found that IL-6 can regulate the
activity of ERK1/2 / RSK1 / C/EBP pathway,
catalyzing the expression of PGRN, and further
promoting cell proliferation. Long-term up-
regulation of PGRN can promote cell malignancy.
IL-6 can also enhance the methylation level of
tumor suppressor factor by modulating DNMT-1
(DNMT-1) and promote cell proliferation. IL-6
induced low cell cycle modulation of egg white P21
(WAF1 / CIP1) by activating p38MAPK, and up-
regulated anti-apoptotic egg white Mcl 1 by
increasing stat-3 activity.
Carcinoembryonic antigen (CEA) is present in
the serum, bile and bile duct epithelium of patients
with cholangiocarcinoma. The bile CEA of patients
with cholangiocarcinoma [(50.2±5.8)ng/ml] was
significantly higher than that of patients with benign
biliary stenosis [(1±3.9)ng/ml], suggesting that the
determination of CEA in serum and bile is helpful
for the early diagnosis of cholangiocarcinoma, the
evaluation of residual tumor and the prognosis of
cholangiocarcinoma .
Ca19-9, CA50, CA242 and other glycochain
group tumor markers were highly sensitive to hilar
cholangiocarcinoma. Patel et al. analyzed serum
CA19-9 of patients with benign and malignant
biliary tract diseases and found that when serum
CA19-9>100μ/ mL, the sensitivity of
cholangiocarcinoma was 53%, while that of patients
with benign liver disease and benign biliary tract
stenosis was 24% and 8%, respectively. The serum
CA19-9 concentration in patients with tumor
resection was significantly lower than that in
patients without tumor resection. Therefore, CA19-9
may be an effective tumor marker for the diagnosis
of cholangiocarcinoma and the monitoring of
efficacy. The sensitivity and specificity of CA50 in
the diagnosis of cholangiocarcinoma were 94.5%
and 33.3% respectively. Brockmann et al. analyzed
the concentrations of CA19-9, CEA, CA72-4,
CA125 and AFP in gallbladder bile of patients with
pancreatic biliary system malignant tumor, and
found that the concentration of CA19-9 was very
high. The sensitivity of CA19-9 in
cholangiocarcinoma was 100%, and the sensitivity
and specificity of CEA in mastoid carcinoma was
100%. Ca19-9 differs between primary carcinoma
and lymph node metastasis. Therefore, CA19-9,
CEA and CA72-4 are valuable in the early diagnosis
and prognosis of cholangiocarcinoma.
Cyfra21-1 is released into the blood by
malignant epithelial cells and is a molecular
biomarker for a variety of malignancies, including
non-small cell lung cancer and gastric cancer.
Similarly, elevated levels of CyFRA21-1 were found
in serum samples from patients with primary liver
tumors, including CCA. Huanget al found that the
diagnostic effect of CYFRA21-1 was superior to
CEA and CA19-9 in iCCA.
EXT1 is one of the five genes encoding the exon
globulin family, and its mutation is believed to be
the cause of hereditary diseases. Studies have found
that the level of EXT1 in the blood of CCA patients
is significantly higher than that of healthy subjects.
Mmp-7 is an endopeptidase in the MMP family,
which can degrade extracellular matrix proteins. In
CCA tumor tissues, it is closely related to tumor
invasiveness and poor prognosis. Mmp-7 in serum
of CCA patients can also be used as a molecular
biomarker for the diagnosis of CCA.
Heat shock protein 70(HSP70) is a stress
response protein, and excessive production can
enhance the resistance of cancer cells to apoptosis-
inducing factors such as tumor necrosis factor α.
One study showed that plasma HSP70 antibody
titers were highest in patients with CCA compared
with cholangitis and healthy controls.
Angpt-2 (ANGPT-2) sophora lectin (SJA) is the
antagonistic ligand of tyrosine kinase Tie2 in the
Angpt/Tie2 system. Since ANGPT-2 is strongly
expressed in the vascular system of many tumors, it
is speculated that it promotes tumor development
together with other cytokines. Serum ANGPT-2
levels were higher in patients with CCA than in
patients with primary sclerosing cholangitis (PSC)
and in patients with bile duct stones. Therefore,
serum ANGPT-2 is feasible as a molecular
biomarker for the diagnosis of CCA.
4.2.2 In the Bile
MUC4, a mucin protein in bile specimens, is
considered as a potential diagnostic marker for
cholangiocarcinoma. Matull et al. did not use
western blots to analyze MUC4 of the biliary tract,
and the results showed high specificity in
differentiating biliary tract cancer from other
malignant tumors, PSC and other benign biliary tract
diseases. In addition, it has also been reported that
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
292

SSP411 protein is a potential molecular biomarker
for the diagnosis of CCA.
4.2.3 In the Urine
Molecular biomarkers related to the diagnosis of
CCA in urine mainly include urinary protein and
miRNA. Urine contains proteins and peptides
derived from ultrafiltration of plasma, and urine
protein bodies are highly sensitive to changes in
both renal and other non-renal diseases. Urine
proteomic analysis (UPA) of the urine peptide-
labeled model showed high sensitivity and
specificity for the diagnosis of CCA.
5 DISCUSSION AND
CONCLUSION
Cholangiocarcinoma is characterized by high
incidence and difficult improvement of long-term
postoperative survival rate, which makes it a major
problem in clinical treatment. Therefore, it is
extremely important to find and diagnose the disease
as early as possible to save the lives of patients.
Based on this, this paper summarized the existing
findings through the review of relevant international
studies, hoping to be helpful for the study of
biomarkers for cholangiocarcinoma. In this review,
the current treatment and diagnosis methods are
summarized. It is not difficult to see from the
current research results that there are still many
blank fields in the research of cholangiocarcinoma.
Although many biomarkers have been found to have
diagnostic value in cholangiocarcinoma, the further
mechanism and other studies are not clear. Through
the efforts of scientists, the clinical treatment of
cholangiocarcinoma has changed significantly in the
past few years, improving the survival rate,
especially in advanced patients, but the survival rate
is still very low, so how to improve the rate of early
diagnosis is still the goal of research. At present,
biomarkers have become a powerful tool for
diagnosis, prognosis and prediction of treatment
response, and the development of biomarkers plays
an important role in improving the prognosis of
these patients. However, biomarker guided liver
tumor treatment is currently a closed clinical
practice, and current technical methods still cannot
fully meet its early diagnosis needs, we still lack
accurate non-invasive biomarkers to diagnose and
evaluate the prognosis of patients with
cholangiocarcinoma. There is still a long way to go
to study biomarkers for cholangiocarcinoma.
REFERENCES
Banales JM, Marin JJG, Lamarca A, Rodrigues PM, Khan
SA, Roberts LR, Cardinale V, Carpino G, Andersen
JB, Braconi C, Calvisi DF, Perugorria MJ, Fabris L,
Boulter L, Macias RIR, Gaudio E, Alvaro D,
Gradilone SA, Strazzabosco M, Marzioni M,
Coulouarn C, Fouassier L, Raggi C, Invernizzi P,
Mertens JC, Moncsek A, Rizvi S, Heimbach J,
Koerkamp BG, Bruix J, Forner A, Bridgewater J,
Valle JW, Gores GJ. Cholangiocarcinoma 2020: the
next horizon in mechanisms and management. Nat
Rev Gastroenterol Hepatol. 2020 Sep;17(9):557-588.
doi: 10.1038/s41575-020-0310-z. Epub 2020 Jun 30.
PMID: 32606456; PMCID: PMC7447603.
Brockmann J, Emparan C,Hernandez CA etal. Gallbladder
bile tumor marker guantification for detection of
pancreatobiliary malignancies[J]. Anticancer Res,
2000, 20(6):4941-4947.
Coelho R, Silva M, Rodrigues-Pinto E, etal.CA 19-9 as
amarker of survival and a predictor of metastization in
cholan-giocarcinoma[J].GE Port J Gastroenterol,
2017, 24 (3): 114-121.
Cheng Q, Feng F, Zhu L, etal.Circulating miR-106a is a
novel prognostic and lymph node Metastasis indicator
for cholangiocarcinoma[J]. Sci Rep, 2015, 5 (4): 1-10.
Chen L, Yan H X, Yang W, et al. The role of microRNA
expression patern in human intrahepatic
cholangiocarcinoma [J]. J Hepatol, 2009, 50(2):358-
369.
Cheng W, Qi Y, Tian L, et al. Dicer promotes
tumorigenesis by translocating to nucleus to promote
SFRP1 promoter methylation in cholangiocarcinoma
cells. Cell death Dis, 2017, 8(2): e2628.
Deng YB, Chen YX. Increased expression of miR-29a
andits prognostic significance in patients with
cholangiocarci-noma [J]. Oncol Res Treat, 2017, 40
(3): 128-132.
Franco L, Giovanni LR, Renato T, etal. Measurement
ofserum carcinoembryonic antigen, carbohydrate
antigen 19-9, cytokeratin-19 fragment and matrix
metalloproteinase-7 for detecting cholangiocarcinoma:
a preliminary case-con-trol study[J]. Anticancer Res,
2014, 34 (11): 6663-6668.
Giovannini M, Bories E, Monges G, etal.Results of a
phaseI -II study on intraductal confocal microscopy
(IDCM) in patients with common bile duct (CBD)
stenosis[J].Surg Endosc, 2011, 25 (7): 2247-2253.
Goydos JS, Brumfield AM, FrezzaE etal. Marked
elevation of serum inter leukin-6 in patients with
cholangiocarcinoma validation of utility as a clinical
marker [J]. Ann Surg, 1998,227(3): 398-404.
Hu HJ, Hui M, Ta YQ, etal. Clinical value of preoperative
serum CA 19-9 and CA 125 levels in predicting the
re-sectability of hilar cholangiocarcinoma [J].
Springerplus, 2016, 5 (1): 551
Huang L, Chen W, Liang P, et al. Serum CYFRA 21-1 in
biliary tract cancers: a reliable biomarker for
gallbladder carcinoma and intrahepatic
Biomarker Study of Cholangiocarcinoma
293

cholangiocarcinoma. Dig Dis Sci 2015, 60(5): 1273-
1283
Hennedige TP, Neo WT, Venkatesh SK.Imaging of
malignan-cies of the biliary tract-an update[J].Cancer
Imaging, 2014, 14 (1): 14.
Isomoto H, KobayashiS. W erneburg NW. eta1.
Interleukin6 upregulates myeloid cell leukemia 1
expression through a STAT3 pathway in
cholangiocarcinoma cells. Hepatology, 2005, 42: 1329
1338.
LuQ, FangT. Circular RNA SMARCA5 correlates with
favorable clinical tumor features and prognosis, and
increases chemotherapy sensitivity in intrahepatic
cholangiocarcinoma [J]. J Clin Lab Anal, 2020, 34(4):
e23138.
Liu P, Zhou TF, Qiu BA, et al. Methylation-Mediated
Silencing of GATA5 Gene Suppresses
Cholangiocarcinoma Cell Proliferation and Metastasis.
Transl Oncol, 2018, 11(3): 585-592.
Madhusudhan KS, Gamanagatti S, Gupta AK.Imaging and
interventions in hilar cholangiocarcinoma: a review[J].
WorldJ Radiol, 2015, 7 (2): 28-44.
Mohamadnejad M, De Witt JM, Sherman S, etal.Role of
EUS for preoperative evaluation of
cholangiocarcinoma: a large single-center experience
[J]. Gastrointest Endosc, 2011, 73 (1): 71-78.
Matull WR, Andreola F, Loh A, et al. MUC4 and
MUC5AC are highly specific tumour-associated
mucins in biliary tract cancer. Br J Cancer 2008,
98(10): 1675-1681
Metzger J, Negm AA, Plentz RR, et al. Urine proteomic
analysis differentiates cholangiocarcinoma from
primary sclerosing cholangitis and other benign biliary
disorders. Gut, 2013,62(1): 122-130
Nakeeb A,Lipsett PA,Lillemoe K etal.Biliary
carcinoembryonic antigen levels are marker for
cholangiocareinoma [J].Am J Surg, 1996, 171(1): 147-
152.
Okada R, Shimada H, Otsuka Y, etal.Serum p53 antibody
as a potential tumor marker in extrahepatic
cholangiocarci- noma[J].Surg Today, 2017, 47 (12):
1492-1499.
Onda S, Ogura T, Kurisu Y, etal.EUS-guided FNA for
biliary disease as first-line modality to obtain
histological evidence[J]. Therap Adv Gastroenterol,
2016, 9 (3): 302-312.
Park TG, Yu YD, Park BJ, etal. Implication of lymph
nodemetastasis detected on 18 F-FDG PET/CT for
surgical plan-ning in patients with peripheral
intrahepatic cholangiocar-cinoma [J].Clin Nucl Med,
2014, 39 (1): 1-7.
Patel AH, Harnosis DM, Klee G etal. The utility of CA19-
9 in the diagnoses of cholangiocarcinoma in patients
without primary sclerosing cholangitis [J]. Am J
Gastroenterol, 2000, 95(1): 204-207.
Rucksaken R, Pairojkul C, Pinlaor P, et al. Plasma
autoantibodies against heat shock protein 70, enolase
and ribonuclease/angiogenin inhibitor as potential
biomarkers for cholangiocarcinoma. PLoS One, 2014,
9(7): el03259
Selaru F M, Olaru A V, Kan T, et al. MicroRNA-21 is
overexpressed in human cholangiocarcinoma and
regulates programmed cell death 4 and tissue inhibitor
of metal oproteinase 3, [J]. Hepatology, 2009, 49(5):
1595-1601.
Voigtlander T, David S, Thamm K, et al. Angiopoietin-2
and biliary diseases: elevated serum, but not bile
levels are associated with cholangiocarcinoma. PLoS
One, 2014, 9(5): e97046
Wang LJ, Zhang KL, Zhang N, etal.Serum miR-26a as
adiagnostic and prognostic biomarker in
cholangiocarcinoma[J]. Oncotarget, 2015, 6 (21):
18631-18640.
WangN, ZhangC, WangW, et al. Long noncoding RNA
DANCR regulates proliferation and migration by
epigenetically silencing FBP1 in tumorigenesis of
cholangiocarcinoma[J]. Cell Death Dis, 2019,
10(8):585.
XuY, YaoY, JiangX, et al. SP1-induced upregulation of
lncRNA SPRY4-IT1 exerts oncogenic properties by
scaffolding EZH2/LSD1/DNMT1 and sponging miR-
101-3p in cholangiocarcinoma[J]. J Exp Clin Cancer
Res, 2018, 37(1):81.
XingLC, ZhangLM, FengYL, et al. Downregulation of
circular RNA hsa_circ_0001649 indicates poor
prognosis for retinoblastoma and regulates cell
proliferation and apoptosis via AKT/mTOR signaling
pathway[J]. Biomed Pharmacother, 2018, 105:326-
333.
Xuan J, Li J, Zhou Z, etal. The diagnostic performance of
serum MUC5AC for cholangiocarcinoma: a
systematic review and meta-analysis[J]. Medicine,
2016, 95 (24): e3513.
Yu FX, Ji SQ, Su LF, etal.Effectiveness and safety of pre-
operative percutaneous transhepatic cholangiodrainage
with bile re-infusion in patients with hilar
cholangiocarcinoma: a retrospective controlled study
[J]. Am J Med Sci, 2013, 346 (5): 353-357.
You Hao, Huang Qiang, Liu Chen, etc.miRNA-21
targeting acts on maspin and its effects on cell
proliferation, apoptosis in cholangiocarcinoma [J]
Practical Preventive Medicine, 2011, 18 (7): 1187-
1190.
ZengB, LiZ H, ChenRF, et al. Epigenetic regulation of
miR- 124 by hepatitis C virus core protein promotes
migration and invasion of intrahepatic
cholangiocarcinoma cells by targeting SMYD3[J].
FEBS Lett, 2012, 586(19): 3271-3278.
ICBEB 2022 - The International Conference on Biomedical Engineering and Bioinformatics
294
