
Gender Differences in ICT Acceptance for Health Purposes, Online
Health Information Seeking, and Health Behaviour among Estonian
Older Adults during the Covid-19 Crisis
Marianne Paimre
1,2 a
and Kairi Osula
1
1
School of Digital Technologies, Tallinn University, Narva Street 25, Tallinn, Estonia
2
Tallinn Health Care College, Kännu 67, Tallinn, Estonia
Keywords: Gender Differences, Older Adults, Acceptance of ICT, Health Information Behaviour, Health, Covid-19
Pandemic, Estonia.
Abstract: ICT tools play an important role in accessing health information today. Although health ratings have improved
in Estonia, the inequalities in women's and men's health continue to persist. As consumption of relevant
information creates favourable preconditions for better health behaviour, it is paramount to study gender
differences regarding online health information seeking and its relations to health behaviour. This article
focuses on gender differences in ICT acceptance for health purposes, online health information seeking, and
health behaviour choices among Estonian older adults. A survey involving 204 men and 297 women aged 50
and over living in Estonia was conducted in the summer of 2020. Cross-tabulation and chi-square tests were
used to analyse the retrieved data. The results indicate that women prioritised remote communication with a
medical doctor more during the Covid-19 crisis while men were more eager to use digital applications for
health purposes. The latter also reported better access to computers and smart devices allowing them to
conduct online health information searches more conveniently. Men also stood out for their readiness to be
vaccinated against Covid-19. Thus, their interest in digital health information should be given due
consideration when developing various health services and apps along with national health communication
strategies.
1 INTRODUCTION
Information and Communication Technologies
(ICTs) provide older people with opportunities to
access useful health information and enable distant
communication with medical professionals (Ageing,
2021; Haase et al, 2021; Nedeljko et al, 2021).
This is
especially important now during the Covid-19 crisis
when older adults are known to be most vulnerable to
the disease and distance communication has been
widely recommended by the authorities everywhere
(Choi et al, 2021; Kor et al, 2021; Moore and
Hancock, 2020). Thus, it is no wonder that internet
use among older people in Estonia has increased
during the Covid-19 crisis. For example, if in 2019
69% of the 55-75-year-olds used the internet every
week, then in 2021 the corresponding figure was
a
https://orcid.org/0000-0002-7079-6513
74%. Among men, the growth in internet use has been
greater (Eurostat, 2022).
In Estonia, life expectancy and health ratings
have improved steadily, however the inequalities in
women's and men's health continue to persist (Naiste,
2022). Although men’s health and their readiness to
see a doctor have improved during the last decade,
they are still more indifferent about their health
(Abuladze et al, 2017). As non-communicable health
problems, often related to poor health behaviour
choices, are largely preventable, the consumption of
relevant health information and better health
awareness could to some extent be conducive to the
extended life expectancy of men (Eriksson-Backa et
al, 2018, Ek, 2015). Therefore, this study focuses on
gender differences in acceptance of ICT tools for
health purposes, online health information behaviour
and health behaviour among Estonian older adults
during the Covid-19 pandemic when everyone was
134
Paimre, M. and Osula, K.
Gender Differences in ICT Acceptance for Health Purposes, Online Health Information Seeking, and Health Behaviour among Estonian Older Adults dur ing the Covid-19 Crisis.
DOI: 10.5220/0011089400003188
In Proceedings of the 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2022), pages 134-143
ISBN: 978-989-758-566-1; ISSN: 2184-4984
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

advised to manage their daily affairs and
communicate with others remotely in order to prevent
the virus.
On the one hand, Estonia is a country often
acclaimed for its digital success (e.g., solutions like
digital signatures, electronic tax returns, e-Business
Register, X-road, and Industry 4.0 (e-Estonia) (Kattel
and Mergel, 2019). On the other hand, it compares
rather unfavourably with the rest of the EU as to poor
health, gender inequality in healthy life years and life
expectancy, but also in connection with the digital
divide between generations (European, 2019). For
example, the healthy life years of Estonian men at
birth (53,9) is the second-lowest figure in the EU
(64,2) (Eurostat, 2022a). The corresponding figure
for women is also not high, i.e., 57,7, compared to the
EU average of 65,1 (Ibid). This clearly calls for a
more detailed examination of the gender differences
in online health information behaviour among
Estonian older adults.
The remaining part of the paper proceeds as
follows: the second section presents the findings of
earlier studies on gender differences in ICT usage and
in use of computers and smart devices for health
purposes, and the links between ICT acceptance,
online health information seeking, and health
behaviour among older people followed by the
hypotheses of the study. Subsequently, the applied
methodology will be introduced together with the
principal outcomes of the study. The paper ends with
a discussion of the findings and conclusions drawn
from them.
2 LITERATURE REVIEW
2.1 ICT Adoption among Older People
Studies often indicate that the groups who have been
less familiar with new technology mainly comprise
older people and women (Goswami and Dutta, 2016;
Ihm and Hsieh 2015; Peacock and Künemund, 2007).
However, older people’s digital skills vary greatly
along with their use of computers and smart devices
(Menéndez Alvarez-Dardet et al, 2020). As Anderson
and Perrin (2017) from the Pew Research Centre note,
those who are younger, more affluent, and more
highly educated report owning and using various
technologies at rates similar to adults under the age of
65.
It could be surmised that during the Covid-19
crisis almost everyone started using either a computer
or smart devices. However, research show that the
digital divide among the older people has deepened
even more during the pandemic (ELSA, 2021). For
example, the English Longitudinal Study of Ageing
(ELSA) Covid-19 Substudy (Wave 1), conducted in
the summer of 2020 show that while just under a
quarter (24%) of over-75s in England have increased
their internet usage since the pandemic hit, this is
mainly driven by the existing users going online more
often. Most older online users stated that their use has
remained unchanged, with nearly one in ten actually
using it less (ELSA, 2021).
2.2 Gender Differences in ICT Use
among Older Adults
With respect to gender, it is more difficult to draw
conclusions about the acceptance and use of ICT.
According to some studies men tend to use digital
devices more than their female counterparts
(Goswami and Dutta, 2016; Durndell et al, 2000).
Lately Shi et al (2021) explored the current status of
e-health literacy among Chinese older adults and
analysed the related influencing factors and found
that gender is an important factor in health
information literacy at the individual level. Marston
and her colleagues’ (2016) study on technology use
and adoption (digital device/internet use, ownership,
length, and frequency as well as social networking)
among people aged 65 or older in Australia shows
that most participants owned a computer with men
being its main user (Marston et al 2016). Sieverding
and Koch (2009) established that there was no
significant difference between gender in assessments
of digital skills, however, women judged their
computer competence to be lower than did men.
However, the gap in Europe has not been very
large in the last years. According to Eurostat, in 2020,
an average of 87% of men and 85% of women aged
16-75 used the internet in Europe (Eurostat, 2022). In
Estonia, statistics show that while in the past (e.g., in
2005) men were more avid internet-users, then by
2019 the gap had disappeared: 89% of men and 88%
of women aged 16-74 used the internet. In 2020, the
proportion of men and women using the internet was
already on par (88%) (Statistics, 2021).
Menéndez Alvarez-Dardet et al. (2020) have
highlighted that the differences between older males
and females do not seem to be unequivocal, instead
they are related to other sociodemographic indicators,
such as educational level. As Anderson and Perrin
(2017) note, those older people who are more
affluent, and more highly educated report owning and
using various technologies at rates similar to younger
people. However, those seniors who are less affluent
or with lower levels of educational attainment
Gender Differences in ICT Acceptance for Health Purposes, Online Health Information Seeking, and Health Behaviour among Estonian
Older Adults during the Covid-19 Crisis
135

continue to have a distant relationship with digital
technology (Ibid).
A wide range of digital health-related
applications for older people has been developed in
advanced countries, however they have been found to
be less attractive to them as compared to younger
people (Choi, et al, 2021; Broekhus et al, 2019;
Gordon and Hornbrook, 2018). The readiness of older
people to use them often depends on the ease of use
of their apps and services and perceived efficiency
(Enwald et al, 2016; Heart and Kalderon, 2013).
Another problem is their lukewarm interest in online
health information (Ihm, Jennifer and Chul-Joo Lee,
2021; Moore and Hancock, 2020).
2.3 OHISB among Older People
Online health information seeking behaviour
(OHISB) can be construed as in general means how
individuals seek information about their health, risks,
illnesses, and health-protective behaviours (Lambert
and Loiselle, 2007; Mills and Todorova, 2016) in the
online environment referring also to a series
interaction diminishing uncertainty with respect to
health status (Tardy & Hale, 1998).
Studies suggest that women are more likely to
seek health information online (Hallyburton and
Evarts, 2014). In the study of Eriksson-Backa et al
(2018), gender was significantly related to both
interest in information about health or illness (chi-
square=8.345, p≤.05) and seeking activity (chi-
square=13.202, p≤.001). 80% of the female
respondents compared to 65% of the male
respondents claimed to be fairly or very interested in
health information, and 71% of the women but only
50% of the men sought information fairly or very
often. Study of Enwald et al (2016) on OHISB among
Finnish older people indicate that women were more
likely to have shared information with others related
to physical activity.
According to Ek (2015), men often lack
motivation for health information seeking. He found
that Finnish women are more interested in health
information, and they are much more active health-
related information seekers as compared to men.
Women also pay more attention to potential
worldwide pandemics and are more attentive to how
the daily goods they purchase affect their health
(Ibid.). Another study indicates that, there are
subgroups including younger, more active, and
family-oriented males that may be reached with
online health information (Weber et al, 2020).
Bidmon and Terlutter (2015) wanted to know
why women use the internet more often for health-
related information searches than men. They were
also interested in gender differences in their research
subjects’ current use of the internet for
communicating with their general practitioner (GP)
and in their future intention to do so (virtual patient-
physician relationship). Their results indicate that
women use the internet for health-related information
searches to a higher degree for social motives and
enjoyment and they judge their information retrieval
outcomes more profoundly than men. Women also
reported higher health and nutrition awareness as well
as a higher personal disposition of being well-
informed as a patient. They concluded that women
have a stronger social motive for and experience
greater enjoyment in health-related information
searches, explained by social role interpretations,
suggesting these needs should be met when offering
health-related information on the internet. The
authors also established that men were more open to
engaging in a remote relationship with the GP;
therefore, they could be the primary target group for
additional online services offered by GPs.
In view of the above, it would be instrumental to
learn which older people use digital technology and
which do not, to what extent it is used for health
purposes and to what extent it affects health
behaviours (e.g., vaccination readiness). Little
research has been done in the era of internet and ICT
dominance, e.g., during the Covid-19 pandemic when
everything seems to have moved online (Pourrazavi
et al, 2022; Tan et al, 2022; Choi et al, 2021; Zhao et
al, 2020) most of which do not focus on gender
differences. It is necessary to investigate the situation
in Estonia as no major studies on the health
information behaviour of older people have recently
been conducted here. As Estonia is a renowned digital
country, the authors of the article expect the patterns
of health information behaviour of older adults to be
slightly different here than elsewhere in the world. In
this study, in light of the ongoing pandemic, the
authors were interested also in older adults’ readiness
to vaccinate themselves against Covid-19 and how
this correlates with their online health information
behaviour.
The overall aim of the article is to analyse gender
differences in acceptance of digital technology for
health purposes (access to computers and smart
devices, willingness to use digital health applications
and services, and to communicate with medical
doctors remotely), online health information
behaviour (OHISB) (frequency of seeking online
health information, preferences for information
sources, problems in finding and assessing the
retrieved information), and its relations to health
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
136

behaviour choices including vaccination readiness for
Covid-19.
The article makes the following hypotheses:
1. 50+ men are more interested in technical
solutions, and remote communication with a
general practitioner (GP) than women.
2. Men have higher computer self-efficacy
ratings.
3. Men are less likely to seek information on
health and diseases.
4. Women exhibit better health behaviour,
including vaccination readiness against
Covid-19.
3 METHODOLOGIES
The data for this study originates from a larger survey
conducted among Estonian older adults by the market
research company Norstat in 2020. Half of the
participants were questioned online and the other half
over the phone between 20 July and 3 August. The
survey had a representative sample in terms of
gender, age, and nationality. As the prevalence of
internet use drops among Estonian people already in
their 50s, this study centres on adults aged 50 and
older. The sample included 501 respondents: 204
(40,7%) men and 297 (59,3%) women from age 50
onwards.
3.1 Participants
The sample included 204 (40,7 %) men and 297 (59,3
%) women
. The oldest participant was 94, the
youngest ones 50 years old. The median age was 65.
The representative group of 55 to 64 comprised 154
people, whereas 130 respondents made up the 65 to
74 age group and 51 belonged to the 75+ group. 75+
were included because the official statistics in Estonia
do not report on this age group’s internet use. 71,7%
of the respondents were Estonians and almost half of
them (52,9%) were pensioners. 54,5% of the
respondents had an average income per family
member in the range of 351-750 euros.
The questionnaire comprised 15 substantive
multiple-choice questions as well as questions
regarding the socio-demographic profile of the
respondents (gender, age, nationality, education
level, employed/unemployed) and monthly income.
10 questions have been used in this article, which
provided more information on ICT acceptance,
OHISB, health behaviour, and health. For each
question, it was possible to choose between different
answer options. For some, the respondent could
choose between yes/no (e.g., do you have access to a
computer or a smart device?). For others (e.g., which
sources of information do you prefer?) there was a list
from which the respondent could choose multiple
answers. For assessment of their digital competence
and health, a Likert-type scale was used, with a choice
of 5 options (very good/good/fair /poor/ I do not wish
to answer this question). For frequencies (e.g., how
often do you need information on illnesses or health
in general), the respondent could choose between 4
options (once a week or more often/ 2 to 3 times a
month/ 2 to 3 times per 3 months/ 2 to 3 times a year
or less often).
The questions included: a) ICT acceptance (for
health purposes): 1) Do you have access to a personal
computer or similar digital device which can be used
for conducting online searches? 2) During the
COVID-19 lockdown, how important was it for you
to have access to a doctor from a distance (e.g.,
exchanging e-mails, texting, video consultations)? 3)
Would you have any use for digital health solutions
or services? For instance, the kind that allows you to
consult with medical personnel, monitor your blood
pressure or sleep patterns, check your heart rate,
remind you to take a pill or keep you company?
b) Self-reported digital competence: 4) How
would you rate your computer skills? 5) When
searching for online information on health concerns
or illnesses have you experienced the following
problems.
c) OHISB. 6) When did you last conduct an
online search on health, illnesses, or disease
prevention?) 7) You come across health information
by accident (e.g., while reading another article you
also spot health news) or by conducting a relevant
search (e.g., you submit the specific query)?
Health behaviour. 8) Do you engage in any of the
following activities? 9) Would like to get vaccinated
if the opportunity arose?
Self-reported health: 10) How do you rate your
general health status?
Socioeconomic indicators included gender, age,
nationality, level of education, employment, and
monthly income.
3.2 Data Analysis
Cross-tabulation and chi-square tests were used to
analyse the retrieved data.
Gender Differences in ICT Acceptance for Health Purposes, Online Health Information Seeking, and Health Behaviour among Estonian
Older Adults during the Covid-19 Crisis
137

4 RESULTS
This section provides an overview of the gender
differences identified in the following categories: ICT
acceptance for health purposes, self-reported
computer skills, OHISB, health behaviour, and self-
reported health.
4.1 ICT Acceptance for Health
Purposes
As could be expected, more men (86,3%) than
women (74,1%) reported access to a computer or a
smart device (p<,05; χ2(1) = 10,87) (see Table 1).
They also expressed greater interest in various digital
health gadgets and services, e.g., electronic sleep
trackers and aids, blood pressure or pulse monitors
and robot communication: 39,5% of men aged 50+
and over were interested in such devices compared to
28,7% of women of the same age. The difference was
statistically significant (p<,05; χ2(3) = 9,64).
However, more women (53,9%) than men
(36,5%) deemed it important to have access to a
doctor from a distance (exchanging e-mails, texting,
video consultations) during the COVID-19
lockdown. The difference was statistically significant
(p<,01; χ2(2) = 13,87).
There was no statistical difference between men
and women regarding different levels of education or
age groups. With respect to different nationalities,
non-Estonian women considered it slightly more
important (61,9%) to have the opportunity to
communicate with a doctor (remotely) than Estonian
women (51,1%). The difference was statistically
significant (p <,05; χ2 (2) = 7,29).
4.2 Self-reported Computers Skills
There was no statistical difference between genders
in computer skills ratings (p>,05; χ2 (3) = 5,95). In
general, almost half of the respondents chose the
response that they would not have any problems
finding and interpreting information. A significant
difference between men and women emerged only in
the category “I don’t know what to make of the
information retrieved (e.g., should I believe the
article/story or not)”. Here, 41,8% of women and
31,3% of men chose this category. The difference was
statistically significant (p <,05; χ2 (1) = 4,68).
4.3 OHISB
4.3.1 Frequency of Online Health
Information Searches
42,5% had searched for information on health, illness
or disease prevention at least once in the last 30 days,
and a little over a fifth (22%) in the last 7 days. 12,1%
answered that they had never searched the internet for
information on health or diseases. There was no
statistically significant difference between men and
women regarding the last time they searched the
internet. Both the chi square test and the distribution
of answers in the table produced the same result.
When analysing the answers of men from
different educational backgrounds, it was found that
61,5% of men with higher education had looked for
information within the preceding month. In other
groups with lower educational levels fewer men had
looked for information during the preceding month,
their percentage points ranged from 33,0% to 46,9%.
The difference was statistically significant (p <,05; χ2
(9) = 21,13). In the case of women, there was no
statistically significant difference by educational
level.
As regards ethnicity, the difference was not
significant. However, the age variable accounted for
a statistically significant difference in the answers of
women: during the previous month, women aged 55-
64 had searched for more information than older
(64+) females (68,1%). The difference was
statistically significant (p <,05; χ2 (9) = 18,30).
There were no significant gender differences in
the information being found by accident or searched
for specifically. There were slightly more men who
initiated a particular search themselves as opposed to
finding the relevant pages by chance, but the
difference was not statistically significant.
4.3.2 Preference for Health Information
Sources
To the question – what are the main online sources
you obtain health information from? – the option
“arbitrary sources of information that Google
displays first” was chosen in 47,2% of the cases. The
option “designated e-health portals and websites on
illnesses” was mentioned in 39,9% of the responses,
“online publications in the professional press, news
portals and their health sections and health
magazines” in 31,3% of the cases, and Wikipedia
amounted to one fifth (20,2%). The remaining
variants were chosen less frequently, for example
research databases and open access sites
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
138

disseminating research outputs (15,4%), internet
forums and discussion groups where people share
their experiences with medical professionals and
illnesses (14,4%), social media platforms (Facebook,
Twitter, YouTube, etc) (13,9%), official websites of
international organisations, government offices and
public agencies (e.g. WHO, Estonian National
Institute for Health Development, Estonian Health
Board) (11,9%), alternative medicine websites
(alternatiivravi.ee, tervisekliinik.ee) (5,3%),
movies/videos (5,3%), alternative media (e.g.
Telegram) (3,3%) and blogs (2,5%). The choices of
men and women were statistically significantly
different only for the two option: a) “special health
and disease portals and websites”, where 46,8% of
women and only 31.3% of men chose this category (p
<,01; χ2 (1) =9,88), and b) “online publications of
professional journalism, news portals and their health
sections and health magazines” which was selected
by 35,9% of women and only a quarter (25%) of men.
The difference was statistically significant (p <,01; χ2
(1) = 5,43).
4.4 Choices in Health Behaviour
The majority of respondents (69,5%) monitor their
diet, try to eat healthy (e.g., plenty of fruits and
vegetables). 76,1% of women and 59,8% of men
opted for this answer. The difference was statistically
significant (p <,001; χ2 (1) = 15,13). 60,9% said they
walk or go cycling on a regular basis. 31,7% swim,
work out in a gym, exercise, or do other sports at
home. 62,3% claimed to be physically active in other
ways (e.g., gardening). 30,3% reported sitting a lot.
23,2% ate fatty foods, semi-finished products, or
sweets. 9,6% reported smoking and 4,1% frequently
consumed alcohol.
There were many more fatty food lovers among
men with basic education (77,8%), while the
corresponding figure for men with higher levels of
education ranged from 12% to 31%. The difference
was statistically significant (p <,001; χ2 (3) = 22,79).
The comparison of different levels of education
among men and women revealed that a healthy diet
gave statistically significantly different results among
women: the lower the level of education, the fewer
healthy eaters were among them, e.g., they accounted
for 44,4% of women with basic education and 67,5%
of women with higher education. The difference was
statistically significant (p <,05; χ2 (3) = 8,94).
In addition to diet, the difference between men
and women was also evident in the consumption of
alcohol where 7,4% of men chose the answer
“consume alcohol often”. In the case of women, the
corresponding figure was only 1,7%. The difference
was statistically significant (p <,01; χ2 (1) = 10,14).
The difference was also statistically significant for
smoking (p <,01; χ2 (1) = 8,53). 6,4% of women and
14,2% of men chose this answer. The responses of
men and women by comparison did not differ in all
other categories.
There was a statistically significant difference
between men as regards their time spent sitting, men
with higher and secondary education sat significantly
more than others (on average 35% of men). The
difference was statistically significant (p <,05; χ2 (3)
= 9,05). There were no differences between the
subgroups of other men or women in terms of
educational attainment.
The results also surprisingly indicated that men
appeared to be more enthusiastic about getting
vaccinated against Covid-19. 60,8% of men agreed to
be vaccinated and the corresponding figure for
women was 48.5%. The difference was statistically
significant (p<.05, χ2(2)=7.54).
4.5 Self-reported Health
61,9% of the respondents considered their health to
be quite good, 4,8% downright excellent. Almost a
third (30,8%) rated it as poor and 2,5% as very bad.
Gender differences were not statistically significant
here.
Looking at different age groups of men and
women, younger women rated their health better
compared to other groups (78,6% rated it as excellent
or fairly good). The older the women were, the less
they rated their health as good or excellent. For
example, among 75+ women 53,6% of the
respondents reported such ratings. Assessment of
one’s health status in different age groups was
statistically significant only for women (p <,01; χ2 (9)
= 21,91). Among men, assessment of health status did
not differ (p> ,05; χ2 (9) = 13,24).
5 DISCUSSIONS
The first hypothesis – 50+ men living in Estonia are
more interested in technical solutions, remote
communication with GP – was partially confirmed.
Men reported better access to ICT devices (computers
and smart devices) and were more willing to use
digital apps and services for health purposes. Thus, in
this respect the results of this study differed from the
outcomes of Ek (2015). However, the current study
also revealed that women found it more important to
communicate with a GP remotely during the Covid-
Gender Differences in ICT Acceptance for Health Purposes, Online Health Information Seeking, and Health Behaviour among Estonian
Older Adults during the Covid-19 Crisis
139
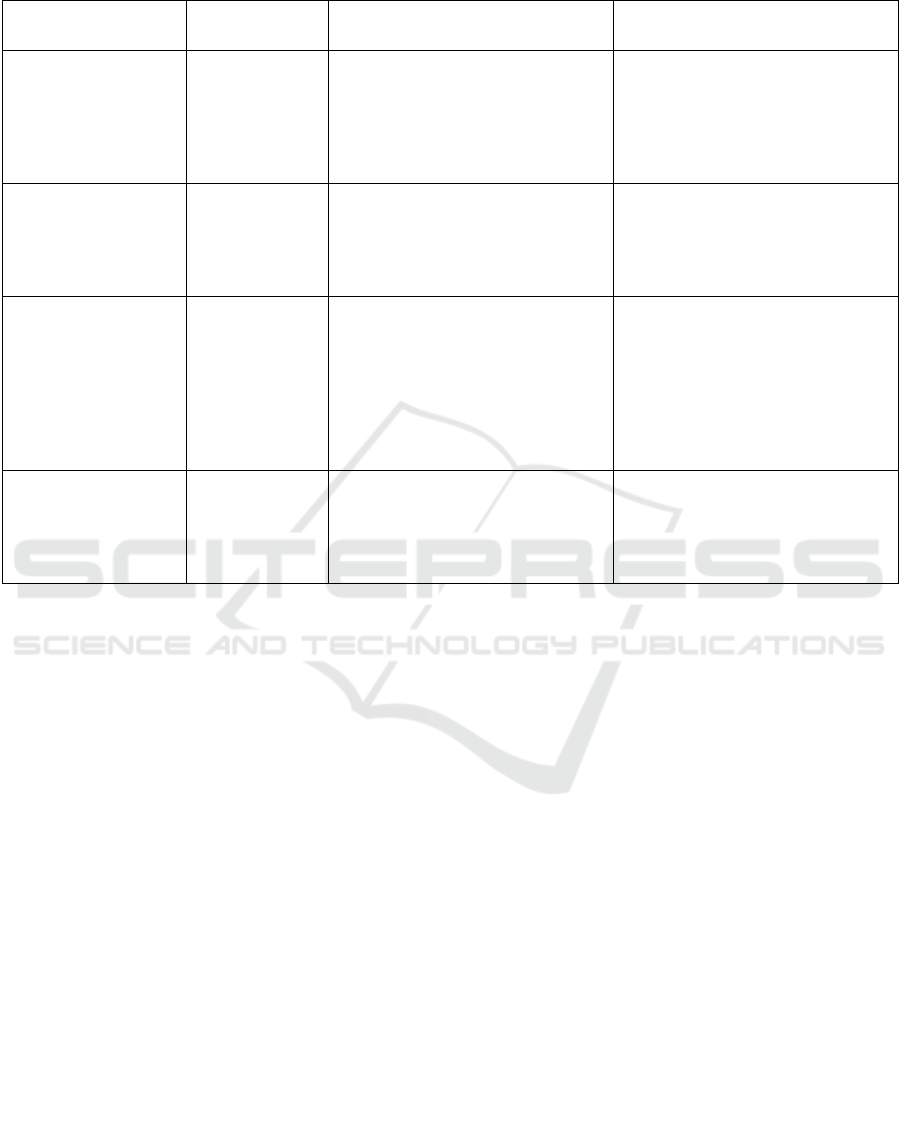
Table 1: Hyphotheses and the results.
Hypothesis
Have hypotheses
been confirmed?
Men Women
50+ men are more
interested in technical
solutions, and remote
communication with a
general practitioner
(GP) than women.
Partly
Men (86,3%) reported better access
to ICT devices.
Men were more willing to use digital
apps and services for health
purposes.
74,1% of women had access to a
computer, or a smart device. Women
found it more important to
communicate with a GP remotely
during the Covid-19 crisis.
Men have higher
computer self-efficacy
ratings.
No
In general, there was no statistical
difference between genders in
computer skills ratings.
However, more women (41,8%)
than men (31,2%) chose the category
“I don’t know what to make of the
information retrieved (e.g., should I
believe the article/story or not)”.
Men are less likely to
seek information on
health and diseases.
No
There was no significant difference
between genders in the frequency of
information seeking.
Although women chose certain
sources of health information (e.g.,
special health and disease portals
and websites and online outlets of
professional journalism) more often
there were no major differences
between gender in terms of source
preference.
Women exhibit better
health behaviour,
including vaccination
readiness against
Covid-19.
Partly
Men appeared to be more
enthusiastic about getting vaccinated
against Covid-19.
The hypothesis was true in respect to
alcohol and tobacco use.
19 crisis. Thus, it can be said that women's and men's
interest in using ICT tools for health purposes is
slightly different which became also evident in a
study conducted by Bidmon and Terlutter (2015).
This may be explained by the fact that men are fond
of technology, but their desire to go to the doctor and
communicate with him/her is lower.
The second hypothesis that men show higher
computer self-efficacy ratings proved to be false as
there was no statistical difference between genders in
computer skills ratings. However, more women than
men expressed doubts about their ability to interpret
the information retrieved.
The third hypothesis that men are less likely to
seek information on health and diseases was also
false. There was no significant difference between
genders in the frequency of information seeking. In
this respect, this result differs from, for example,
some studies conducted in the Nordic countries
(Eriksson-Backa et al, 2018; Ek, 2015).
Although women chose certain sources of health
information (e.g., special health and disease portals
and websites and online outlets of professional
journalism) more often there were no major
differences between gender in terms of source
preference. However, it is worrying that random
search results displayed by Google first were popular
among men and women alike, suggesting modest
levels of critical evaluation of the sources.
The fourth hypothesis – women exhibit better
health behaviour, including vaccination readiness
against Covid-19 – was true in terms of alcohol and
tobacco use. However, men appeared to be more
enthusiastic about getting vaccinated against Covid-
19, which was quite surprising. This result is partly in
line with Estonian vaccination statistics (Estonian,
2022) according to which 65+ men have been
vaccinated more than women. One could ask what
sparks men’s interest in vaccination at an older age.
This most probably may be put down to their poorer
health.
A sedentary lifestyle seems to be a problem
among older adults, especially among those who use
computers and smart devices.
This study revealed that slightly different trends
have emerged in Estonia compared to the previous
studies (e.g., Eriksson-Backa et al, 2018; Ek, 2015;
Hallyburton and Evarts, 2014), which could be
explained by the peculiarities of Estonia as a top
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
140

performer in the digitalisation of its administration
and public services.
Due to the limited scope of the questionnaire and
the subsequent study, this survey did not attempt to
establish which attributes, in addition to the socio-
demographic characteristics, influence personal
interest in electronic health information and health
behaviour (e.g., psychological characteristics of the
respondent, past experience with technology and
information retrieval, trust in physicians, etc.). All
these aspects warrant further investigation.
6 CONCLUSIONS
Gender differences in health information behaviour
were not particularly pronounced among 50+ people
living in Estonia. However, men reported better
access to computers and smart devices and a higher
willingness to use ICT for health purposes. Women,
on the other hand, were more interested in remote
communication with a medical doctor during the
pandemic. Men, as expected, smoke and consume
more alcohol, while women eat more fatty foods.
The premise that men tend to be ignorant about
their health was misguided. Perhaps the peculiarity of
Estonia as a smart/digital country also accounts for
the fact that men are increasingly more interested in
health information retrieved via digital channels.
It follows from the above that in the realm of
health communication and/or promotion, it is well
worth the effort to try to reach 50+ men through
digital channels.
ACKNOWLEDGEMENTS
This survey was supported by the "Ülikoolide
arengufondid" grant TF3320 “Conducting a survey
related to my doctoral dissertation on the health
information behaviour of Estonian older adults (50+)
in the online environment”.
The presentation at the 8
th
International
Conference on Information and Communication
Technologies for Ageing Well and e-Health is
supported by the European Union from the European
Regional Development Fund.
REFERENCES
Abuladze, L., Kunder, N., Lang, K., & Vaask, S. (2017).
Associations between self-rated health and health
behaviour among older adults in Estonia: a cross-
sectional analysis. BMJ open, 7(6), e013257.
https://bmjopen.bmj.com/content/7/6/e013257
Ageing in the Digital Era. (2021). UNECE Policy Brief on
Ageing No. 26 July. https://unece.org/sites/default/
files/2021-07/PB26-ECE-WG.1-38.pdf
Anderson, M., Perrin, A. (2017). Tech Adoption Climbs
Among Older Adults. Pew Research Centre.
https://www.pewresearch.org/internet/2017/05/17/tech
nology-use-among-seniors/.
Bidmon, S., Terlutter, R. (2015). Gender Differences in
Searching for Health Information on the Internet and
the Virtual Patient-Physician Relationship in Germany:
Exploratory Results on How Men and Women Differ
and Why. Journal of medical Internet research, 17(6):
e156. https://doi.org/10.2196/jmir.4127
Broekhuis, M., Velsen, L.V., Stal, S.T., Weldink, J., &
Tabak, M. (2019). Why My Grandfather Finds
Difficulty in using Ehealth: Differences in Usability
Evaluations between Older Age Groups. In
Proceedings of the 5th International Conference on
Information and Communication Technologies for
Ageing Well and e-Health, (ICT4AWE): 48–57.
Heraklion, Crete, Greece. DOI:10.5220/00076808004
80057.
Choi, N.G, DiNitto, D. M, Marti. C.N, Choi, B.Y. (2021).
Telehealth Use Among Older Adults During COVID-
19: Associations with Sociodemographic and Health
Characteristics, Technology Device Ownership, and
Technology Learning. Journal of Applied Gerontology,
5. doi: 10.1177/07334648211047347.
Durndell, A., Haag, Z., Asenova, D.,Laithwaite, H. (2000).
Computer Self Efficacy and Gender: a cross cultural
study of Scotland and Romania. Personality and
Individual Differences, 28: 1037-1044.
DOI:10.1016/S0191-8869(99)00155-5
Ek, S. (2015). Gender differences in health information
behaviour: a Finnish population-based survey. Health
Promotion International, (3)30, 736–745,
https://doi.org/10.1093/heapro/dat063.
ELSA. (2021). English Longitudinal Study of Ageing.
Covid-19 Substudy (Wave 1). Digital inclusion and
older people – how have things changed in a Covid-19
world? https://www.pslhub.org/learn/commissioning-
service-provision-and-innovation-in-health-and-care/
digital-health-and-care-service-provision/digital-inclus
ion-and-older-people-%E2%80%93-how-have-things-
changed-in-a-covid-19-world-march-2021-r4342/
Enwald, H., Kangas, M., Keränen, N., Immonen, M.,
Similä, H., Jämsä, T., Korpelainen, R. (2017). Health
information behaviour, attitudes towards health
information and motivating factors for encouraging
physical activity among older people: differences by
sex and age. Information Research, 22(1): 22-1.
http://informationr.net/ir/22-1/isic/isic1623.html
Eriksson-Backa, K., Enwald, H., Hirvonen, N., & Huvila, I.
(2018). Health information seeking, beliefs about
abilities, and health behaviour among Finnish seniors.
Journal of Librarianship and Information Science,
Gender Differences in ICT Acceptance for Health Purposes, Online Health Information Seeking, and Health Behaviour among Estonian
Older Adults during the Covid-19 Crisis
141

50(3): 284-295. https://journals.sagepub.com/doi/
abs/10.1177/0961000618769971
Estonian Covid-19 open-data portal. (2022). Retrieved
7.1.2022. https://opendata.digilugu.ee/docs/?fbclid=Iw
AR1ZP9jARzOh80wHvumaYFJ6FNRPBK1lp_7Py2
NBX_lvZEi3GIUMTJxCCzw#/et/readme
European Social Survey. (2019). Round 9 (2018/2019).
https://www.europeansocialsurvey.org/data/download.
html?r=9
Eurostat. (2022). Individuals – frequency of internet use.
Retrieved 24.1.2022 from: http://appsso.eurostat.ec.
europa.eu/nui/show.do?dataset=isoc_ci_ifp_fu&lang=
en
Eurostat. (2022a). Healthy life years at birth by sex.
Retrieved 25.1.2022 from https://ec.europa.eu/eurostat/
databrowser/view/tps00150/default/table?lang=en&fb
clid=IwAR3_p1sJIGlaw90IFJW4gaZptN-
mvzZOhWAeEa3nipo-9gMh68ogKTIkW98
Gordon, N.P., Hornbrook, M.C. (2018). Older adults’
readiness to engage with eHealth patient education and
self-care resources: a cross-sectional survey. BMC
Health Serv Res 18: 220 https://doi.org/10.1186/
s12913-018-2986-0
Goswami, A., Dutta, S. (2016). Gender Differences in
Technology Usage—A Literature Review. Open
Journal of Business and Management, 4: 51-59.
http://dx.doi.org/10.4236/ojbm.2016.41006.
Haase, K., Cosco, T., Kervin, L., Riadi, I., O'Connell, M.
(2021). Older Adults’ Experiences with Using
Technology for Socialization During the COVID-19
Pandemic: Cross-sectional Survey Study. JMIR Aging,
4(2), e28010. URL: https://aging.jmir.org/
2021/2/e28010,
Hallyburton, A., Evarts, L.A. (2014). Gender and Online
Health Information Seeking: A Five Survey Meta-
Analysis. Journal of Consumer Health on the Internet,
18(2): 128–142.
Heart, T., Kalderon, E. (2013). Older adults: are they ready
to adopt health-related ICT? Int J Med Inform. 82(11):
e209-31. doi: 10.1016/j.ijmedinf.2011.03.002.
Ihm, J., Hsieh, Y.P. (2015). The implications of
information and communication technology use for the
social well-being of older adults. Information,
Communication & Society 18(10): 1123-1138.
https://doi.org/10.1080/1369118X.2015.1019912.
Ihm, J., Lee, C.-J. (2021). Toward More Effective Public
Health Interventions during the COVID-19 Pandemic:
Suggesting Audience Segmentation Based on Social
and Media Resources. Health Communication, 36(1):
98-108. DOI:10.1080/10410236.2020.1847450.
Kattel, R., Mergel, I. (2018). Estonia’s Digital
Transformation. Mission Mystique and the Hiding
Hand. Working Paper Series: IIPP WP 2018-09.
DOI:10.1093/oso/9780198843719.003.0008.
Kor, P.P.K., Leung, A.Y.M., Parial, L.L., Wong, E.M.L.,
Dadaczynski, K., Okan,O., Amoah, P.A., Wang, S.S.,
Deng, R., Cheung, T.C.C., Molassiotis, A. (2021). Are
People with Chronic Diseases Satisfied with the Online
Health Information Related to COVID-19 During the
Pandemic? J Nurs Scholarsh, 53(1): 75-86. doi:
10.1111/jnu.12616. Epub 2020 Dec 14. PMID:
33316121.
Lambert, S., Loiselle, C. (2007). Health information
seeking behavior. Qualitative Health Research, 17:
1006–1019. DOI: 10.1177/1049732307305199.
Marston, H. R., Kroll, M., Fink, D., Rosario, H., Gschwind,
Y.-J. (2016). Technology use, adoption and behavior in
older adults: Results from the iStoppFalls project.
Educational Gerontology 42, 6: 371-387.
https://doi.org/10.1080/03601277.2015.1125178.
Menéndez Alvarez-Dardet, S., Lorence Lara, B., Perez-
Padilla, J. (2020). Older adults and ICT adoption:
Analysis of the use and attitudes toward computers in
elderly Spanish people. Computers in Human
Behaviour, 110. https://doi.org/10.1016/j.chb.2020.10
6377.
Mills, A., Todorova, N. (2016). An integrated perspective
on factors influencing online health-information
seeking behaviours. ACIS 2016 Proceedings, 83.
https://aisel.aisnet.org/acis2016/83.
Moore RC, Hancock JT. (2020). Older Adults, Social
Technologies, and the Coronavirus Pandemic:
Challenges, Strengths, and Strategies for Support.
Social Media + Society. doi:10.1177/205630512094
8162
Naiste ja meeste võrdõiguslikkus [Equality between women
and men]. (2022). Sotsiaalministeerium. Retrieved
24.1.2022 from: https://gender.sm.ee/teemad/tervis/
Nedeljko, M., Bogataj, D., Kaučič, B.M. (2021). The use of
ICT in older adults strengthens their social network and
reduces social isolation: Literature Review and
Research Agenda. IFAC PapersOnLine, 645–650.
Peacock, Sylvia E., Künemund, H. (2007). Senior citizens
and Internet technology. European Journal of Ageing
4(4):191-200. DOI: 10.1007/s10433-007-0067-z.
Pourrazavi S, Kouzekanani K, Asghari Jafarabadi M,
Bazargan-Hejazi S, Hashemiparast M, Allahverdipour
H. (2022). Correlates of Older Adults' E-Health
Information-Seeking Behaviors. Gerontology. Jan
14:1-8. doi: 10.1159/000521251. Epub ahead of print.
PMID: 35034012.
Shi Y, Ma D, Zhang J, Chen B. (2021). In the digital age: a
systematic literature review of the e-health literacy and
influencing factors among Chinese older adults. Z
Gesundh Wiss, 4(1): 9. doi: 10.1007/s10389-021-
01604-z. Epub ahead of print. PMID: 34104627;
PMCID: PMC8175232.
Statistics Estonia. (2021). Statistika andmebaas:
Sotsiaalelu. 16-74-aastased internetikasutajad elukoha
ja kasutuseesmärgi järgi. (Statistical database: Social
life. Internet users aged 16-74 by residence and purpose
of use.) Accessed January 5, 2022. http://pub.stat.ee/px-
web.
Sieverding, M., Koch, S. (2009). Self-Evaluation of
computer competence: How gender matters. Computers
& Education, 52: 696-701. 10.1016/j.compedu.20
08.11.016.
Tan, Y.R, Tan, M.P., Khor, M.M, Hoh, H.,B., Saedon, N.,
Hasmukharay, K., Tan, K.M., Chin, A.V.,
Kamaruzzaman, S.B., Ong, T., Davey, G., Khor, H.M.
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
142

(2022). Acceptance of virtual consultations among
older adults and caregivers in Malaysia: a pilot study
during the COVID-19 pandemic. Postgrad Med., 6(1):
6. doi: 10.1080/00325481.2021.2004792. Epub ahead
of print. PMID: 34758702.
Tardy, R.W., Hale, C.L. (1998). Getting “plugged in: A
network analysis of health ‐ information seeking
among “ stay ‐ at ‐ home moms. Communication
Monographs, 65(4): 336-357. DOI: 10.1080/0363775
9809376457
Weber, W., Reinhardt, A., Rossmann, C. (2020). Lifestyle
Segmentation to Explain the Online Health
Information–Seeking Behavior of Older Adults:
Representative Telephone Survey. Journal of Medical
Internet Research 22(6)):e15099. doi:10.2196/15099.
Zhao, X., Fan, J., Basnyat, I., Hu, B. (2020). Online Health
Information Seeking Using "#COVID-19 Patient
Seeking Help" on Weibo in Wuhan, China: Descriptive
Study. Journal of Medical Internet Research, 22(10):
e22910. https://doi.org/10.2196/22910.
Gender Differences in ICT Acceptance for Health Purposes, Online Health Information Seeking, and Health Behaviour among Estonian
Older Adults during the Covid-19 Crisis
143
