
Reversible Fragile Medical Image Watermarking Scheme Resistant to
Malicious Tampering Attacks
Victor Fedoseev
1,2 a
and Anna Denisova
1,2 b
1
Samara National Research University, Samara, Russia
2
Image Processing Systems Institute, Branch of the Federal Scientific Research Centre “Crystallography and Photonics”
of Russian Academy of Sciences, Samara, Russia
Keywords: Fragile Digital Watermark, Medical Images, Quantization Index Modulation, Reversible Watermarking.
Abstract: Paper is aimed to eliminate a significant drawback of existing schemes for protecting medical images from
tampering using fragile watermarking: instability to “malicious tampering attacks”. In such attacks, an
intruder, while tampering image content, keeps unchanged an inconspicuous additional component that
contains a fragile watermark. In watermarking schemes based on least significant bit (LSB) embedding or
quantization index modulation (QIM), such a component is the remainder of dividing pixel values by some
number corresponding to embedding parameters. In this paper, we present a QIM-based fragile watermarking
method resistant to malicious tampering due to variation in quantization steps. This fact is justified
theoretically and confirmed experimentally. For use in real systems for processing and analyzing medical
images, a reverse watermarking scheme based on this method is proposed. The reversibility property is
achieved by the division of an image into a region of interest (ROI) and a region of noninterest (RONI) and
dual watermarking.
1 INTRODUCTION
Digital medical images (CT, X-ray, MRI and other)
stored as DICOM along with patient data are usually
transmitted via unsafe networks and can be
vulnerable to falsification and tampering (Memon,
2020). This could lead to misdiagnosis and have
serious consequences. Hence, medical image
protection from tampering is a crucial problem
requiring modern solutions. Since the mid-2000s a
significant number of watermarking methods have
been developed for tampering detection and
localization in medical images (Giakoumaki, 2006),
Coatrieux, 2006), (Memon, 2008).
It is important to note that an essential feature of
the use of watermarking methods for medical data is
the inadmissibility of introducing distortions into
image fragments significant for diagnostics. This
limitation explains the fact that most of the existing
watermarking schemes use image segmentation into
the region of interest (ROI) – a part used for medical
diagnostics – and the remaining region of noninterest
a
https://orcid.org/0000-0003-1750-1920
b
https://orcid.org/0000-0002-2297-758X
(RONI). We can specify the following classes of
watermarking schemes for ROI protection against
tampering:
1) Fragile reversible watermarking in ROI or
whole image (Al-Qershi, 2011), (Liu, 2019).
2) Fragile watermarking in ROI along with robust
watermarking in RONI. The robust watermark may
contain data to recover the introduced ROI error
(Mousavi, 2014), (Khor, 2017), (Memon, 2020).
3) Robust watermarking in RONI, where the
watermark should contain some ROI data (its hash
and/or hash of its parts) to detect tampering (Swaraja,
2018), (Alshanbari, 2021), (Balasamy, 2021).
All three classes have their pros and cons, as well
as efficient implementations described in the
literature. However, unfortunately, a significant
vulnerability, which is a characteristic of classes 1-2
(which involve ROI watermarking), remains outside
the scope of known research.
Our paper discusses this vulnerability in detail and
proposes its own watermarking algorithm, and a
specific scheme related to class 2, which is free from
Fedoseev, V. and Denisova, A.
Reversible Fragile Medical Image Watermarking Scheme Resistant to Malicious Tampering Attacks.
DOI: 10.5220/0011067200003209
In Proceedings of the 2nd International Conference on Image Processing and Vision Engineering (IMPROVE 2022), pages 57-65
ISBN: 978-989-758-563-0; ISSN: 2795-4943
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
57

this vulnerability. The rest of the paper includes three
sections. Section 2 introduces us to the current state
of research on this topic. Then Section 3 describes the
proposed scheme. Finally, Section 4 provides some
experimental results and gives a brief discussion.
2 RELATED WORK
First of all, let us take a closer look at a typical class
2 scheme. It involves dividing the image into ROI and
RONI and further embedding digital watermarks of
different content and purpose into each of them. In
ROI, a fragile watermark for tampering localization
is embedded. As a rule, this watermark does not carry
any meaningful information and can be generated
using a pseudo-random generator based on a secret
key. Being fragile, this watermark is designed to
break when the image changes and the positions of
incorrectly extracted watermark bits allow us to
estimate the local area of changes. Thus, the recipient
of the image extracts the fragile watermark and
compares it with the reference watermark data
generated using the secret key known to him. The
extraction procedure is usually computationally
efficient since fragile watermarking uses simple
algorithms in the spatial domain (or less often, a
simple spatial data transformation is performed
before embedding). If the extracted watermark is
completely correct, then the image is considered
suitable for further diagnostics. Otherwise, a
distortion map is built to identify the nature of the
distortion and investigate its causes.
Fragile watermarking usually does not cause
significant distortion, but for medical images, it is
advisable to exclude even the slightest possibility of
misdiagnosis. Therefore, the error introduced into the
ROI as a result of fragile watermarking is embedded
in the RONI area as a separate watermark. This
watermark is embedded using a robust method to
protect this information from distortion, which can
also be caused by random factors, such as noise in the
data transmission channel. Thus, if the received
image was found suitable for diagnosis as a result of
checking the correctness of the extracted fragile
watermark, the extraction of the ROI error from the
robust watermark is performed. Then the ROI area is
corrected, and the image is transferred to medical
specialists. It is also worth noting that, in addition to
the ROI error, the robust watermark may include
patient data, other metadata, and data for image
recovery after malicious distortion. Watermark
robustness is provided by using DWT (Al-Qershi,
2011), DWT-SVD (Priyanka, 2017), (Alshanbari,
2021), block-DCT (Parah, 2017) or any other
transform domain. In addition, error-correcting codes
may also be used.
An important practical issue in the
implementation of the described scheme is how to
segment the image into ROI and RONI. In some
studies focusing on a particular type of medical data
(e.g., ultrasound data), the ROI and RONI areas are
considered deterministic and do not change for
different images (Khor, 2017), (Alshanbari, 2021). A
number of papers propose automatic ROI extraction
algorithms based on image analysis or machine
learning technologies, such as edge detection, active
contours and others. Examples of such algorithms can
be found in (Memon, 2008), (Memon, 2020),
(Balasamy, 2021). Other papers (Al-Qershi, 2011),
(Eswaraiah, 2015), (Priyanka, 2017), (Golea, 2019)
indicate that ROI/RONI segmentation should be
carried out by a physician before the embedding
procedure. Finally, some authors do not address this
issue at all (Liu, 2019). In our study, we also do not
consider it necessary to choose any specific
segmentation method, believing that a specific
solution should be chosen in practice from the options
described above based on the specifics of the
particular medical images.
In this paper, we want to draw attention to an
important vulnerability of the currently existing
algorithms of the considered class. It is related to the
fact that for fragile watermarking, researchers use
solutions based on least significant bit (LSB)
watermarking or quantization index modulation
(QIM). For example, papers (Memon, 2008),
(Memon, 2009), (Memon, 2020) present dual
watermarking schemes where fragile watermarking is
based on LSB embedding into ROI (region of
interest). (Eswaraiah, 2014) proposes an LSB-based
fragile watermarking technique. In (Priyanka, 2017)
two LSBs of ROI are replaced at the protection stage
by some bits. (Liu, 2019) uses a QIM-based
reversible watermarking. More examples of LSB and
QIM based watermarking for tamper localization can
be found in (PhadiKar, 2012), (Shehab, 2018), (Su,
2020) and other papers.
The vulnerability mentioned above is that LSB
and QIM may be a subject of “malicious tampering
attacks”. In such attacks, an intruder, while tampering
image content, keeps unchanged an inconspicuous
additional component that contains a fragile
watermark. In watermarking schemes based on LSB
and QIM watermarking, such a component is a matrix
of remainders of dividing pixel values by some
number depending on the quantization step value
IMPROVE 2022 - 2nd International Conference on Image Processing and Vision Engineering
58

used at watermark embedding. If data is embedded in
the first LSB, this value equals 2.
Unfortunately, in the literature on fragile
watermarking for medical image protection, this
vulnerability is not considered at all, despite its
obviousness and vivid consequences. This was the
reason for conducting the present study. In our paper,
we propose a new QIM based fragile watermarking
method resistant to the malicious tampering attack,
and specify a medical image protection scheme based
on dual watermarking in ROI and RONI.
3 PROPOSED WATERMARKING
SCHEME
In this section, we define a new fragile watermarking
algorithm based on scalar QIM watermarking and a
complete medical protection scheme that uses this
algorithm. In addition to fragile watermarking, this
scheme contains RONI watermarking as any other
class 2 implementation (see Introduction).
The main feature of our fragile watermarking
approach is that it uses a range of quantization steps
when embedding watermark bits into ROI pixels. The
value of the quantization step for each particular pixel
is generated using a pseudorandom number generator
using a secret key unknown to an intruder. The
number of possible quantization step values is limited
due to the requirement of watermark imperceptibility.
Nevertheless, it is very hard for the intruder to save
the residue of pixel brightness on several quantization
steps and at the same time meaningfully modify an
image region.
3.1 Main Features
Let 𝑆
be the ROI area and 𝑆
be the RONI area.
The sum of 𝑆
and 𝑆
is equal to 𝑁
𝑁
, where
𝑁
is a height and 𝑁
is a width of the image. We
denote a number of bits per pixel (pixel depth) as 𝐷.
For DICOM images, pixel depth can take values from
a set 𝐷∈
8,10,12,14,16
, depending on image type.
For example, 𝐷16 is usual for computer
tomography and 𝐷12 is used for digital
radiography (Mildenberger, 2002).
The fractions of pixels belonging to ROI and
RONI are
𝑘
𝑆
𝑁
𝑁
,𝑘
𝑆
𝑁
𝑁
,
𝑘
𝑘
1.
(1)
Thus, ROI capacity can be calculated as 𝐼
𝑆
𝐷. Similarly, RONI capacity 𝐼
𝑆
𝐷.
As mentioned below, we do not specify how to
separate ROI and RONI. However, we supply that
both ROI and RONI are defined on an 𝑟𝑟 block
grid. In practice, it is reasonable to use 𝑟8.
The same grid of pixel blocks is used to localize
tampering. If at least one pixel in an 𝑟𝑟 block is
found as tampered then we decide the whole block is
tampered. To solve the authentication problem, we
embed 𝑐 pseudorandom watermark bits into 𝑐 pixels
of each block. The bigger value of 𝑐 is used the lower
probability of skipping a tampered block is achieved.
The distorted block may not be identified if the
extracted watermark bits occasionally match to the
embedded sequence. This situation is possible with
the probability 1/2
. On the other hand, the bigger 𝑐
corresponds to the bigger distortions in the
watermarked image.
3.2 Embedding and Extraction
Formulae
The embedding and extraction formulae for a pixel
𝑛
,𝑛
are written as follows:
𝐶
𝑛
,𝑛
𝐶
𝑛
,𝑛
2∆
,
⋅2∆
,
𝑊
𝑛
,𝑛
⋅∆
,
𝐶
𝑛
,𝑛
mod ∆
,
;
(2
)
𝑊
𝑛
,𝑛
𝐶
𝑛
,𝑛
∆
,
mod 2
.
(3
)
where 𝐶
𝑛
,𝑛
is the original image pixel,
𝑊
𝑛
,𝑛
is the bit of watermark, ∆
,
is the
quantization step varying from 1 to ∆
, 𝑎 mod b
calculates the remainder from division of 𝑎 on b,
⌊
𝑎
⌋
is the closest integer value less than 𝑎, 𝐶
𝑛
,𝑛
is
the watermarked image pixel, 𝑊
𝑛
,𝑛
is the
extracted watermark bit.
Equation (2) describes a supervised scalar
quantization of matrix 𝐶
𝑛
,𝑛
with quantization
step 2∆
,
, which varies depending on the pixel
coordinates
𝑛
,𝑛
according to the secret key. As a
result, the distortion of each particular pixel is equal
to 0 or ∆
,
. Watermark extraction is performed
according formula (3).
Reversible Fragile Medical Image Watermarking Scheme Resistant to Malicious Tampering Attacks
59

3.3 Resistance to Malicious Tampering
Attacks: Theoretical Analysis
The main goal of tampering attacks on medical
images is to obstruct making a correct diagnosis.
Common methods include image slicing, image
retouching, copy-move etc. In research papers (see,
for example, (Kaur, 2016)), tampering attacks are
usually modeled using common image processing
operations like average or median filtering, noise
addition, JPEG compression and others. However,
they model a blind intruder who does not know the
image protection scheme and does not make any
efforts to preserve a fragile watermark that may be
embedded into the image.
Since most tamper protection schemes for
medical images are based on fragile LSB or QIM
watermarking as shown in Introduction, an intruder
can try to implement a malicious tampering scenario:
both change the image contents and preserve the
watermark. For this purpose, he needs to allocate an
imperceptible signal component containing a
watermark, to make changes into the visible
component and then to re-add the allocated
component containing the watermark. In classical
LSB or QIM schemes, this component is the
remainder of a division each pixel value by 2∆, where
∆ has the same meaning as in (2)-(3) but does not
change for different pixel positions. We will call as
the simple malicious tampering attack this kind of
attack where ∆ is supposed to be guessed by an
intruder and equal to the real value used for image
protection (if it is a constant value).
This attack has common features with a vector
quantization (VQ) attack described in (Holliman,
2000) and later used in many papers on tamper
detection (Su, 2020). In VQ, entire image blocks are
replaced using samples from protected images in
order to save the watermark.
Since in (2)-(3) we see ∆
,
instead of constant
∆, theoretically, this attack should be ineffective for
our method. To adopt the attack, the intruder has to
keep unchanged C
n
,n
mod 2∆
,
for all
possible values of ∆
,
from 1 to ∆
. One way to
do that is to find least common multiple of the
numbers from 2 to 2∆
: 𝐿𝐶𝑀2,...,2∆
and
then use it instead of the constant 2∆. We call this
version of attack as the advanced malicious
tampering attack.
Table 1 shows the 𝐿𝐶𝑀 values for each particular
∆
and corresponding bit lengths to store them.
Based on the values given in Table 1, we can estimate
the value of ∆
, which is sufficient to protect the
image from the advanced attack: corresponding 𝐿𝐶𝑀
should be comparable with 2
. More precisely, we
can recognize the attack as not applicable in practice
if 𝐿𝐶𝑀
…
2
. This empirical rule leads to the
estimations of safe ∆
values shown in Table 2.
Table 1: Adequate dividers to perform a malicious attack
on the proposed watermarking method.
∆
LCM
2,…,2∆
∆
LCM
2,…,2∆
1 2 7 840
2 4 8 1680
3 12 9 5040
4 24 10 5040
5 120 11 55440
6 120 12 55440
Table 2: Adequate ∆
values for different 𝐷.
𝐷 ∆
Free bits
available for
an intrude
r
Distortions in
watermarked
p
ixels
85 1 0,5
10 7 0 0,7
12 8 1
0,8
16 11 0 0,11
3.4 Reversibility of ROI
Table 2 demonstrates that we may use relatively sall
∆
to prevent the described attacks and guarantee
watermark invisibility. Nevertheless, even small
changes in ROI should be removed before medical
diagnostics. To restore the original image, we use the
second part of our scheme: RONI watermarking,
where the difference between original ROI and ROI
of the watermarked image is used as the second
watermark. For each pixel, this difference equals zero
or ∆
,
(and we unambiguously define the sign of
nonzero difference). Thus, to restore the original pixel
value, we need only one bit meaning that the pixel
value is changed. As a result, the volume of the
restoration watermark equals
𝐼
𝑘
𝑁
𝑁
∙
bits.
(4
)
The ratio of RONI capacity to 𝐼
is
𝐼
𝐼
𝑘
𝑁
𝑁
𝐷
𝑘
𝑁
𝑁
∙
𝑐
𝑟
𝑟
𝑐
1
𝑘
1𝐷.
(5
)
Let us analyze this product. The first multiplier is
not less than one. Table 3 presents typical values of
the second multiplier. Finally, 𝐷∈
8,10,12,14,16
.
Thereby it is evident that the capacity of RONI is
enough to store the second watermark for ROI
IMPROVE 2022 - 2nd International Conference on Image Processing and Vision Engineering
60
restoration. For example, if 𝑟2, 𝑐1, 𝑘
1/4 then the watermark can be stored 12 times in one
LSB plane of RONI.
Table 3: Typical values of the second multiplier in (4).
𝑘
1/𝑘
1
1/10 9
1/5 4
1/4 3
1/3 2
1/2 1
3.5 RONI Watermarking Method
To determine the second watermarking method for
RONI, we need to analyze possible attacks on RONI.
Intuitively, we may suppose that we need a robust
watermarking method. However, what is the aim of
attacking RONI? If an intruder attacked ROI and we
identified and localized tampering by means of ROI
watermarking then ROI restoring becomes
unnecessary. Otherwise, if tampering is not detected,
then the attacker does not need to make changes in
RONI to keep tampering unknown. Thus, RONI
tampering in combination with ROI tampering has no
sense.
In the case of RONI tampering without distorting
ROI, the attacker's goal is to leave the ROI noisy and
simply complicate the doctor’s work without
“pushing” him to misdiagnose with meaningful
changes. But it is obvious that the potential danger of
such an attack is not so significant.
Thus, we come to the conclusion that we do not
need a robust RONI watermarking and can use even
LSB watermarking with a shuffle. In practice, we set
a number of bit planes 𝑃 used for RONI
watermarking equal to 2 for 𝐷8, 3 for 𝐷∈
10,12
and 4 for 𝐷∈
14,16
.
3.6 Pixel Selection for ROI
Watermarking
Although the changes in ROI caused by watermark
embedding are reversible, this does not entail the
acceptability of significant changes in the ROI. Such
distortions can be seen visually and misinterpreted by
participants in the data transfer process. Moreover,
significant distortions may help an attacker to reveal
the quantization steps for particular pixels. Therefore,
the ROI should not contain obvious artifacts. Further,
we consider the question how to select watermarked
pixel positions to reduce ROI distortions.
The first approach to select 𝑐 pixel positions is
random selection using a secret key. This approach is
very simple. However, it is not the best choice in
terms of visual quality because it does not take into
account original pixel values. If the pixel has low
value and corresponding ∆
,
is high then the pixel
has a high distortion relative to other pixels.
To reduce such distortions, we propose a second
approach. Its key point is to define positions for
embedding as pixels with the smallest ∆
,
among
all pixels in a block 𝑟𝑟. It is possible to achieve
the uniqueness of determining such points in each
block when we generate the whole matrix ∆
,
.
This approach requires big enough values of 𝑐 and 𝑟
to prevent a possible artificial decrease in ∆
.
4 EXPERIMENTAL RESEARCH
In this section, we describe the results of three
experiments. The first two ones investigate tampered
area localization quality in two tampering scenarios,
while the third one researches visual quality after ROI
watermark embedding. The RONI watermarking
procedure is quite clear so we did not investigate it
numerically.
As test data, we used four DICOM images from a
dataset presented in (Rutherford, 2021). Table 4
specifies the key characteristics of these images. The
first two letters in the image name stand for image
modality: CR is Computed Radiography, DX is
Digital X-ray and CT is Computed Tomography.
Table 5 shows ROI parameters for these images
(𝑦
,𝑥
are the coordinates of the left-upper corner of
the ROI and ℎ,𝑤 denote height and width of the
ROI).
Table 4: Test image parameters.
Name Image size D Body
Part
CR
_
PHI-001-1.dc
m
1760×2140 10 Chest
DX_PHI-002-4.dc
m
2022×2022 14 Chest
CR
_
PHI-006-1.dc
m
1760×1760 12 Uterus
CT
_
PHI-014-2.dc
m
1211×888 16 Bladde
r
Table 5: ROI parameters.
Name
𝑦
,𝑥
,ℎ,𝑤
CR
_
PHI-001-1.dc
m
[200,200,1023,1023]
DX
_
PHI-002-4.dc
m
[400,400,1023,1023]
CR_PHI-006-1.dc
m
[300,300,1023,1023]
CT_PHI-014-2.dc
m
[150,150,1023,511]
Reversible Fragile Medical Image Watermarking Scheme Resistant to Malicious Tampering Attacks
61

To estimate the quality of tampered area
localization, we use a true positive rate (TPR)
measure defined as follows:
𝑇𝑃𝑅
𝑄
𝑄
,
(6)
where 𝑄
is the number of blocks correctly
determined as tampered, 𝑄
is the total number of
changed blocks. To estimate the visual quality of
images after embedding, we compute mean square
error (MSE).
4.1 Localization of the Simple
Tampering
In our first experiment, we model the attack described
in Section 2.3. We suppose that an intruder modifies
a specific number of pixels in each block. The
modification consists in replacing 𝐶
𝑛
,𝑛
with 𝑥
which has the same remainder from the division on
2∆:
𝑥
mod 2∆
𝐶
𝑛
,𝑛
mod 2∆
.
(7
)
In this experiment, ∆ is fixed for the whole image
and acts as a parameter varying from 1 to ∆
. Thus,
we consider a scenario in which the intruder tries to
save the remainder of a division by 2∆ and does not
know the valid quantization step values used at the
embedding procedure and the positions of protected
pixels.
Figure 1: Tamper localization quality for CR_PHI-001-
1.dcm, 𝑀𝑅0.5.
We tested our method for 𝑀𝑅
0.5,0.75
(number of modified pixels divided by the total
number of pixels), 𝑟
4,8
and 𝐸
0.25,0.5,0.75,1
, where 𝐸𝑐𝑟
⁄
. The average
results for different images and different 𝑀𝑅 values
are shown in Figures 1-4. These figures demonstrate
that more than 90% of tampered blocks are detected
if we embed watermark bits into half pixels of each
block or more. The worst result (60-90% of correctly
identified blocks) corresponds to the case of 𝐸
0.25 for CR_PHI-001-1.dcm. As a result, we
recommend to use 𝐸 greater than 0.5.
Figure 2: Tamper localization quality for DX_PHI-002-
4.dcm, 𝑀𝑅0.75.
Figure 3: Tamper localization quality for CR_PHI-006-
1.dcm, 𝑀𝑅0.5.
Figure 4: Tamper localization quality for CT_PHI-014-
2.dcm, 𝑀𝑅0.75.
We should also stress that the quality of the
resulting mask of unauthorized tampering can be
additionally improved by post processing. In this
procedure, we applied morphological closing with a
square structural element of size 3𝑟 3𝑟. Our
experiments showed that average 𝑇𝑃𝑅 value
obtained in the worst case (𝐸 0.25, 𝐶𝑅0.5 for
IMPROVE 2022 - 2nd International Conference on Image Processing and Vision Engineering
62
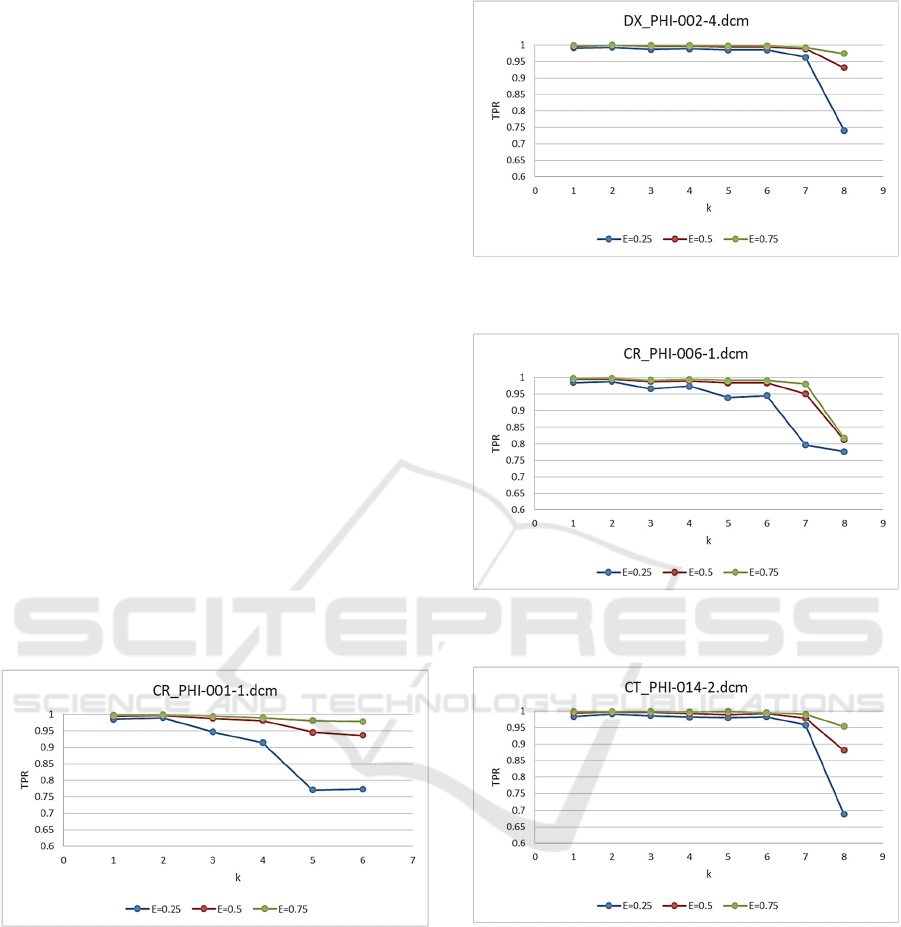
image CR_PHI-001-1.dcm) rose to 0.98. To sum up,
the proposed method in combination with post
processing provides 𝑇𝑃𝑅0.98.
4.2 Localization of the Advanced
Tampering
In our second experiment, we modeled a more
advanced tampering attack when an intruder
substitutes a pixel 𝐶
𝑛
,𝑛
mod δ
with 𝑥 such
as
𝑥
mod δ
𝐶
𝑛
,𝑛
mod δ
,
(8
)
where 𝛿LCM2,4…,2k and k varies from 1 to
∆
. Some of k values were not considered because
the resulting LCM was too big and changes exceeded
the dynamic range of the image.
For this experiment, we decided to use post
processing for all δ values. The other parameters of
the method are: 𝑀𝑅
0.5,0.75
, 𝑟
4,8
and
𝐸
0.25,0.5,0.75
. Figures 5-8 show the results for
our four DICOM images. They demonstrate that our
watermark remains resistant to the second attack.
𝑇𝑃𝑅 starts to degrade only for
𝑘
more than 7.
However, in this case the changes made by the
intruder became visible because the LCM2,4…,2k
value become too big (more than 840) and an
authorized user can detect the changes visually.
Figure 5: Tamper localization quality for CR_PHI-001-
1.dcm, 𝑀𝑅0.5, for different k, after post processing.
4.3 Visual Quality Examination
In our third experiment, we assessed visual
degradation of images after watermarking. In
Section 2.6, we presented two approaches to select
positions for embedding. The first one is random,
while the second one embeds watermark bits in pixels
with the smallest ∆
,
values in the block.
Figure 6: Tamper localization quality for DX_PHI-002-
4.dcm, 𝑀𝑅0.75, for different k, after post processing.
Figure 7: Tamper localization quality for CR_PHI-006-
1.dcm, 𝑀𝑅0.5, for different k, after post processing.
Figure 8: Tamper localization quality for CT_PHI-014-
2.dcm, 𝑀𝑅0.75, for different 𝑘, after post processing.
The embedding method was tested under the
following parameters: 𝑀𝑅0.5, 𝑟
4,8
and 𝐸
0.25,0.5,0.75
. MSE values obtained for both
approaches are shown in Tables 4 and 5. The tables
show that the second approach produces less MSE
error than the first one. Specifically, the second
approach reduces the RMSE value in 1.81 times in
average.
Reversible Fragile Medical Image Watermarking Scheme Resistant to Malicious Tampering Attacks
63
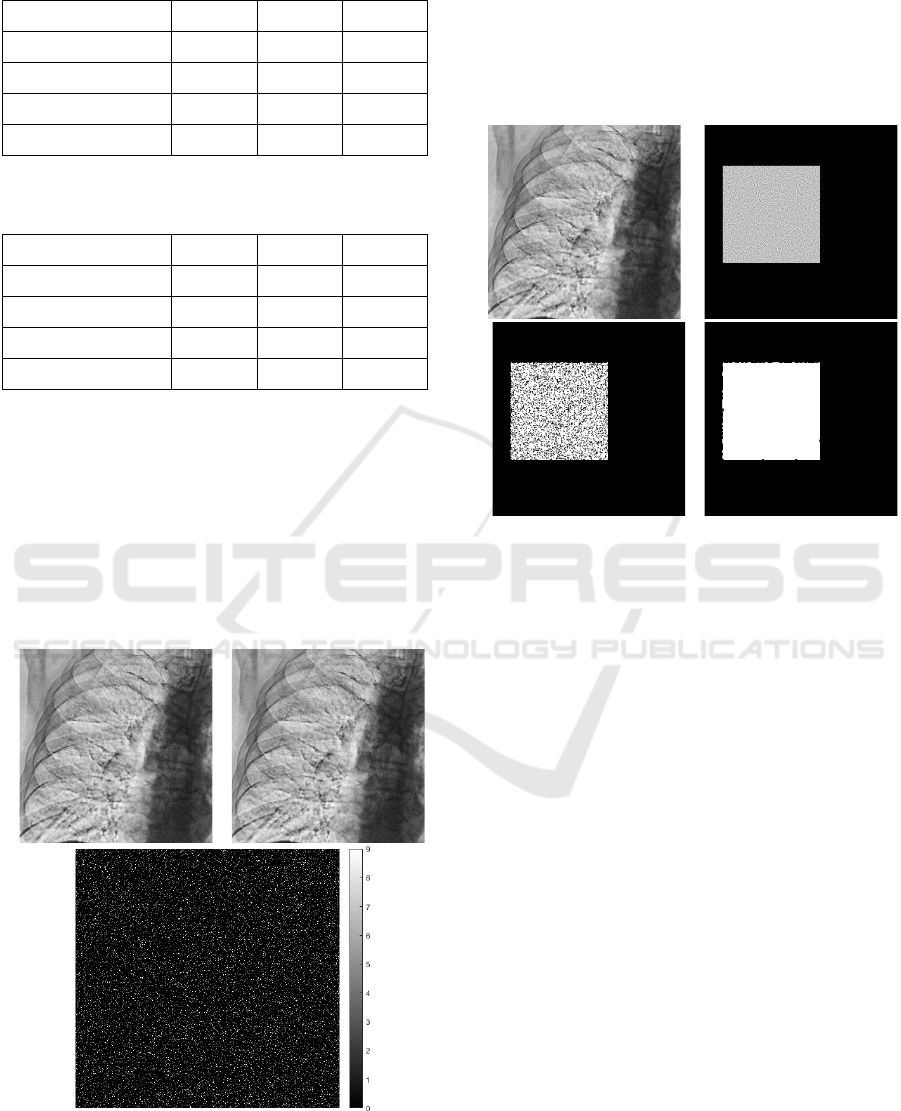
Table 6: MSE of watermarked images (first pixel selection
approach).
Image E=0.25 E=0.5 E=0.75
CR_PHI-001-1.dcm 2.97 4.20 5.14
CR_PHI-006-1.dcm 3.39 4.80 5.87
CT_PHI-014-2.dcm 4.38 6.21 7.61
DX_PHI-002-4.dcm 3.68 5.21 6.38
Table 7: MSE of watermarked images (second pixel
selection approach).
Image E=0.25 E=0.5 E=0.75
CR_PHI-001-1.dcm 1.25 2.60 4.11
CR_PHI-006-1.dcm 1.36 2.86 4.64
CT_PHI-014-2.dcm 1.64 3.65 6.04
DX_PHI-002-4.dcm 1.45 3.12 5.10
As the experiment showed, due to the wide
dynamic range of the images, the embedded
watermark is imperceptible. Examples of a source
image, a corresponding watermarked image and their
difference shown in Figure 9 illustrate that watermark
traces are very hard to locate visually. Moreover, we
should not forget (according to Section 2.5) that the
watermarking method is reversible, and the
watermark can be removed from the image after its
detection.
a) b)
c)
Figure 9: Watermark embedding effect for DX_PHI-002-
4.dcm: (a) source image, (b) watermarked image, (c)
absolute value of their difference.
Figure 10 illustrates an example of tampering
localization for the same image. Although the
tampered area is imperceptible by human eye, our
algorithm gives a good approximation of this area.
Moreover, a post-processing morphological closing
procedure let us improve this approximation (we used
a 9×9 window in this example).
a) b)
c) d)
Figure 10: Tampering localization for DX_PHI-002-4.dcm:
a) tampered image, b) correct map of tampered values, c)
map of tampered values estimated by our algorithm, d)
estimated map after post-processing.
5 CONCLUSION
In this paper, we have addressed the issue of the
vulnerability of the known fragile watermarking
methods for medical images to malicious tampering.
To fix this issue, we have proposed a new QIM-based
fragile digital watermarking method. This method
embeds a digital watermark into ROI. The method is
based on random generation of the quantization steps
for each pixel of the ROI using a secret key. The
variation of quantization steps protects the image
from malicious tampering when an intruder tries to
keep unchanged the invisible image component
containing the watermark. To make the scheme
reversible, the embedding error is stored in RONI.
The experimental results approved the efficiency
of the proposed approach to malicious tampering and
demonstrated visual imperceptibility of the
watermark.
IMPROVE 2022 - 2nd International Conference on Image Processing and Vision Engineering
64

ACKNOWLEDGEMENTS
The reported study was funded by RFBR, project
number 19-29-09045.
REFERENCES
Al-Qershi, O. M., & Khoo, B. E. (2011). Authentication
and Data Hiding Using a Hybrid ROI-Based
Watermarking Scheme for DICOM Images. Journal of
Digital Imaging, 24(1), 114–125.
Alshanbari, H. S. (2021). Medical image watermarking for
ownership & tamper detection. Multimedia Tools and
Applications, 80(11), 16549–16564.
Balasamy, K., & Suganyadevi, S. (2021). A fuzzy based
ROI selection for encryption and watermarking in
medical image using DWT and SVD. Multimedia Tools
and Applications, 80(5), 7167–7186.
Coatrieux, G., Lecornu, L., Sankur, B., & Roux, Ch. (2006).
A Review of Image Watermarking Applications in
Healthcare. 2006 International Conference of the IEEE
Engineering in Medicine and Biology Society, 4691–
4694.
Eswaraiah, R., & Reddy, E. S. (2014). A Fragile ROI-Based
Medical Image Watermarking Technique with Tamper
Detection and Recovery. 2014 Fourth International
Conference on Communication Systems and Network
Technologies, 896–899.
Eswaraiah, R., & Sreenivasa Reddy, E. (2015). Robust
medical image watermarking technique for accurate
detection of tampers inside region of interest and
recovering original region of interest. IET Image
Processing, 9(8), 615–625.
Giakoumaki, A., Pavlopoulos, S., & Koutsouris, D. (2006).
Multiple Image Watermarking Applied to Health
Information Management. IEEE Transactions on
Information Technology in Biomedicine, 10(4), 722–
732.
Golea, N. E. H., & Melkemi, K. (2019). ROI-based fragile
watermarking for medical image tamper detection.
International Journal of High Performance Computing
and Networking, 13, 199.
Holliman, M., & Memon, N. (2000). Counterfeiting attacks
on oblivious block-wise independent invisible
watermarking schemes. IEEE Transactions on Image
Processing, 9(3), 432–441.
Kaur, A., & Rani, J. (2016). Digital Image Forgery and
Techniques of Forgery Detection: A brief review.
International Journal of Technical Research & Science,
1(4), 18–24.
Khor, H. L., Liew, S.-C., & Zain, J. Mohd. (2017). Region
of Interest-Based Tamper Detection and Lossless
Recovery Watermarking Scheme (ROI-DR) on
Ultrasound Medical Images. Journal of Digital
Imaging, 30(3), 328–349.
Liu, X., Lou, J., Fang, H., Chen, Y., Ouyang, P., Wang, Y.,
Zou, B., & Wang, L. (2019). A Novel Robust
Reversible Watermarking Scheme for Protecting
Authenticity and Integrity of Medical Images. IEEE
Access, 7, 76580–76598.
Memon, N. A., & Gilani, S. A. M. (2008). NROI
watermarking of medical images for content
authentication. 2008 IEEE International Multitopic
Conference, 106–110.
Memon, N. A., Gilani, S. A. M., & Qayoom, S. (2009).
Multiple watermarking of medical images for content
authentication and recovery. 2009 IEEE 13th
International Multitopic Conference, 1–6.
Memon, N. A., & Alzahrani, A. (2020). Prediction-Based
Reversible Watermarking of CT Scan Images for
Content Authentication and Copyright Protection.
IEEE Access, 8, 75448–75462.
Mildenberger, P., Eichelberg, M., Martin, E. (2002).
Introduction to the DICOM standard. European
radiology, 12(4), 920-927.
Mousavi, S. M., Naghsh, A., & Abu-Bakar, S. A. R. (2014).
Watermarking Techniques used in Medical Images: a
Survey. J Digit Imaging, 27, 714-729.
Parah, S. A., Sheikh, J. A., Ahad, F., Loan, N. A., & Bhat,
G. M. (2017). Information hiding in medical images: A
robust medical image watermarking system for E-
healthcare. Multimedia Tools and Applications, 76(8),
10599–10633.
Phadikar, A., Maity, S. P., & Mandal, M. (2012). Novel
wavelet-based QIM data hiding technique for tamper
detection and correction of digital images. Journal of
Visual Communication and Image Representation,
23(3), 454–466.
Priyanka, & Maheshkar, S. (2017). Region-based hybrid
medical image watermarking for secure telemedicine
applications. Multimedia Tools and Applications,
76(3), 3617–3647.
Rutherford, M., Mun, S. K., Levine, B., Bennett, W., Smith,
K., Farmer, P., Jarosz, Q., Wagner, U., Freyman, J.,
Blake, G., Tarbox, L., Farahani, K., Prior, F. (2021). A
DICOM dataset for evaluation of medical image de-
identification. Scientific Data, 8(1), 1-8.
Shehab, A., Elhoseny, M., Muhammad, K., Sangaiah, A.
K., Yang, P., Huang, H., & Hou, G. (2018). Secure and
Robust Fragile Watermarking Scheme for Medical
Images. IEEE Access, 6, 10269–10278.
Su, G.-D., Chang, C.-C., & Lin, C.-C. (2020). Effective
Self-Recovery and Tampering Localization Fragile
Watermarking for Medical Images. IEEE Access, 8,
160840–160857.
Swaraja K. (2018). Medical image region based
watermarking for secured telemedicine. Multimedia
Tools and Applications, 77(21), 28249–28280.
Reversible Fragile Medical Image Watermarking Scheme Resistant to Malicious Tampering Attacks
65
