
Exploring Privacy: Mental Models of Potential Users of AAL
Technology
Caterina Maidhof
a
, Martina Ziefle
b
and Julia Offermann
c
Chair of Communication Science, Human-Computer Interaction Center, RWTH Aachen University, Campus-Boulevard 57,
Aachen, Germany
Keywords: Perception of Privacy, Older Adults, AAL Technology, Lifelogging, Mental Models, Cognitive Maps, 3CM
Method.
Abstract: Ambient Assisted Living (AAL) technologies have a high potential to combat healthcare challenges while
supporting older adults to live independently at their own home. Despite the general positive uptake of such
technology, perceptions of barriers of acceptance persist, a major one regards privacy. With an explorative
qualitative approach, the current study aimed at investigating participants` cognitive representations of a
scenario in which AAL is installed in the own home as a support at an older age. Special focus was on eliciting
participants` implications for privacy in this scenario and to understand the individual requirements of using
AAL technology at home. Opinions of 12 participants (age range: 23-81 years) from Germany and
Switzerland were assessed through semi-structured interviews. The paper presents descriptive results and
emerging themes of the mapping approach. The results show the usefulness of the method to understand
thought processes of potential users regarding privacy preferences and technology usage. Findings might be
useful to inform technical designers as well as lawmakers to consider these usage requirements during
technology or law development.
1 INTRODUCTION
Ambient Assisted Living (AAL) technologies are
intended to be a constant part of the day-to-day life of
older adults in need of care (Blackman et al., 2016;
Muñoz et al., 2011). Such technological solutions
have a high potential to effectively combat healthcare
challenges and support people living at home in older
age (Peek et al., 2014) – improving quality of life for
them as well as their caregivers (Pollack, 2005).
Various sensors, actuators, smart interfaces, and
artificial intelligence are integrated into homes and
lives of the elderly to provide support for functional
capabilities of “activities of daily living” as well as
sensing and preventing risky situations such as falls
(Blackman et al., 2016; Calvaresi et al., 2017). In the
context of AAL, many sensors, either wearable or
ambient installed, are used for lifelogging. The latter
term refers to digitally tracking and documenting
everyday live by recording physiological and
a
https://orcid.org/0000-0002-0573-4498
b
https://orcid.org/0000-0002-6105-4729
c
https://orcid.org/0000-0003-1870-2775
behavioural data in real time which is stored for a
subsequent knowledge extraction (Selke, 2016). To
adequately log people`s lives, data recording is
always on and usually shared with stakeholders such
as care personnel or medical practitioners to
adequately design independent-living strategies
(Selke, 2016).
1.1 AAL Technologies, Acceptance and
Privacy
Generally, many of these specific applications are
perceived positively by a broad range of users and are
thought to be helpful and beneficial, providing an
increased feeling of safety and greater independence
(e.g., Garg et al., 2014; Gövercin et al., 2016;
Lorenzen-Huber et al., 2011; Wild et al., 2008).
Potential barriers and concerns raised by different
user groups are the lack of personal contact, perceived
control, continuous monitoring, fear of data misuse as
well as invasion of privacy (e.g., Beringer et al., 2011;
Maidhof, C., Ziefle, M. and Offermann, J.
Exploring Privacy: Mental Models of Potential Users of AAL Technology.
DOI: 10.5220/0011046200003188
In Proceedings of the 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2022), pages 93-104
ISBN: 978-989-758-566-1; ISSN: 2184-4984
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
93

Demiris et al., 2004; Kirchbuchner et al., 2015; van
Heek et al., 2018). An increased need for care
(Offermann-van Heek et al., 2019; van Heek et al.,
2017) as well as care experience can have an
influence on technology acceptance. Care
experienced people seem to rely more on emotional
aspects compared to inexperienced potential users
(Offermann-van Heek & Ziefle, 2019). General
findings from Offermann-van Heek and Ziefle
(2019) suggest that data access and privacy are the
most relevant factors when deciding on AAL
technology usage for both, caretakers and caregivers.
Indeed, privacy concerns are a main barrier to
acceptance of AAL (Peek et al., 2014; Yusif et al.,
2016) and they largely come about when the actual
level of privacy does not match the desired amount
(Altman, 1976). The “ideal” amount of privacy and
the balance between sharing and protecting individual
data mainly depend on the context and personal
attitudes (Altman, 1976; Bergström, 2015;
Nissenbaum, 2010). This reflects findings that
privacy concerns in the context of AAL are tradeable
in adequate circumstances. Ulrich et al. (2020) show
that older adults are willing to trade privacy for safety
due to their need for autonomy, suggesting that users`
willingness to reduce privacy is altered especially
when they feel in control of the situation. Similarly,
privacy concerns are reduced if the devices provide
positive contributions to health and wellbeing, are
easy to use, and do not cause stigmatization (Ulrich et
al., 2020). Findings from a longitudinal study of
Himmel and Ziefle (2016) reveal that technology
acceptance depends on the location of the devices in
the user´s home. Technology in more private rooms
such as the bath and bedroom are less accepted
compared to the kitchen, living room or the home
office.
Taking the previously reviewed literature into
account it becomes evident that privacy is a
multidimensional construct and its evaluation in the
AAL context of whether it is a concern, a desired
state, or even a tradeable unit depends on multiple
contextual as well as personal factors. Based on
previous definitions of privacy Burgoon (1982)
makes a distinction of four dimensions of privacy that
account for the complex circumstances in the context
of AAL (Schomakers & Ziefle, 2019). Namely, in the
AAL context dimensions of social privacy (control
over social contacts, interaction, and
communication), of physical privacy (degree of
physical inaccessibility) as well as of psychological
privacy (degree of inaccessibility to thoughts,
feelings, and intimate information), and of
informational privacy (control over personal
information) might play a pivotal role.
One way to study the multifaced construct of
privacy is through the assessment of mental models.
This has already been done, for instance, to assess
laypersons general conceptualization of privacy
(Oates et al., 2018), older adults` understanding of
privacy in digital and non-digital contexts (Ray et al.,
2019, 2021) as well as older adults` privacy
expectations in adaptive assistive technologies
(Hamidi et al., 2020).
In the context of ageing and living with AAL,
however, mental conceptualizations of privacy still
require further investigations.
1.2 Mental Representations of Privacy
and Cognitive Maps
Mental models are cognitive representations of the
external reality that guide people to interact with the
world around them (Craik, 1943; Johnson-Laird,
1983). Based on personal life experiences,
perceptions, and understandings of the world
individuals create a cognitive structure that shapes the
basis of reasoning and decision making. Cognitive
maps have an influence on what information
individuals focus on and how they perceive it, thus,
ascribing them a leading role when it comes to
integrating and interpreting new information (Kaplan
& Kaplan, 1982). According to Collins and Gentner,
(1987) to explain unfamiliar domains people make
use of familiar mental models similar to the unknown.
As studies show (e.g., Rickheit & Sichelschmidt,
1999), phenomena that are not directly perceivable in
the external reality are explained in the same way as
unfamiliar domains. Kaplan and Kaplan (1981) view
cognitive maps as mental models that are schematics
of individuals’ cognitive representation of a specific
situation or problem. Kearny and Kaplan (1997)
argue that the most important, significant, and
concerning contents of a cognitive map are those
quickly coming to mind.
Even though, to date there is no consensus on the
definition of a mental model (e.g., see Thagard, 2010)
and still confusion about the nature of cognitive maps
(e.g., see Kitchin, 1994), various methods exist to
elicit and study people´s internal cognitive
representations of the world. Among the latter, there
is the open-ended 3CM (conceptual content cognitive
map) method, a corroborated method proposed by
Kearney and Kaplan (1997) for assessing peoples`
cognitive structures and processes. It has already been
used in the field of healthcare to understand personal
perceptions and concerns of people diagnosed with
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
94

lung cancer (Lehto & Therrien, 2010) and to
understand nurses` perceptions of children’s pain
(Van Hulle Vincent, 2007). The method is suited to
measure people`s viewpoints on complex domains
(Kearney & Kaplan, 1997) and as such, the
interaction and support with AAL technologies can be
seen. Particularly suited for small-scale samples and
for in depth-exploration the open-ended version of the
method will be employed in this study to gain
information about individuals’ perspectives of a
personal healthcare scenario with assistive
technology.
Besides exploratively testing through semi-
structured interviews the effectiveness of the
described method within the given AAL and care
context, the aim of the study is to deeply understand
thought processes regarding the role of personal
privacy while being supported and cared for by AAL
technology in older age. The goal is to get insights on
opinions of a diverse sample consisting of people
from two different European countries, being of all
ages, with and without (professional) care experience
and various levels of technical understandings. In line
with previous theoretical explanations and given a
scenario where people are confronted with using
AAL technology in their own home for the first time,
they would immediately think of and possibly reveal
core contents of their existing mental representation
regarding this scenario.
2 METHOD AND MATERIALS
This chapter outlines the empirical approach of the
study. First, the characteristics of the semi-structured
interviews and its successive data analysis are
explained. Subsequently, the interview guidelines
and procedure are described in detail including the
AAL scenario. Lastly, participants of the study are
presented.
2.1 Semi-structured Interviews and
Data Analysis
The interview was divided into two main parts. The
first part consisted of questions regarding privacy in
daily life and feelings of privacy violation. The
second part started with the introduction of the AAL
scenario. Based on the Conceptual Content Cognitive
Map (3CM) method described by Kearney and
Kaplan (1997) participants were guided to create their
mental representation of this scenario.
The interviews were audiotaped and transcribed
verbatim. The theoretical foundation of the analysis
was the thematic qualitative text analysis as outlined
by Kuckartz (2014). The study was carried out in both
German and Italian. The selected quotes were
translated into English for this publication.
2.2 The Interview Procedure
Participants were welcomed to the interview with a
general introduction into the topic of privacy and
AAL technologies.
The first part of the interview consisted of four
main questions regarding the meaning of privacy,
privacy behaviour, and feelings of privacy violation.
The second part of the interview started with the
introduction into the AAL scenario and was followed
by the task of creating a mental map. Therefore,
participants were asked to imagine themselves in this
scenario and were told that their answers of the
upcoming three questions were written down in boxes
to create a visualization of their thoughts – each box
corresponded to another mental object in this
scenario. These three questions addressed
participants` first impression of the scenario,
connections they could draw to privacy and their ideal
imagination of this technology in line with their
privacy preferences. Each topic was discussed
extensively and only when participants clearly
signalled that the visualization map was complete for
them, the interviewer proceeded. Like this, maps
varied in complexity meaning that the number of
objects within the maps varied depending on
participants` personal understanding of the scenario.
As for the subsequent task participants were asked to
sort the answer boxes into meaningful groups of
statements. Then, participants had to code each group
or box according to the degree of importance, i.e.,
how important they would consider each of their
statements in terms of privacy in this scenario. The
interviewer then picked the statement that was rated
as most important and questioned if it was
interchangeable. If so, participants were encouraged
to name what they considered as an adequate
exchange.
The interview finished with an informal talk about
participants` demographics and their experiences in
care as well as regarding technology.
2.2.1 The AAL Scenario
Participants were encouraged to picture themselves as
an eighty-year-old healthy but frail person living
alone at their own home. Participants had to imagine
that AAL technology was installed in their homes to
support them and to counteract frailty due to ageing.
Exploring Privacy: Mental Models of Potential Users of AAL Technology
95

The type and functionality of this technology was not
important, but participants were informed that the
technology would have various social and functional
features. Among the latter the following were
mentioned: medical care support (e.g., measuring
temperature, blood pressure), household assistance
(e.g., turning light on and off, vacuum cleaning),
monitoring (e.g., gait monitoring), memory aid (e.g.,
daily reminders for medicine or important events) and
a social companion (e.g., motivates and provides
games for physical and cognitive exercise, facilitates
communication with family and friends). Hence, this
technology consisted of a very extensive non-human
support for both, the person in need of assistance as
well as the caregivers involved.
2.3 Participants
The qualitative interview study was carried out in
June and July 2021 with twelve participants who were
interviewed with semi-standardized questions
through videophone. The interviews lasted
approximately one hour and were conducted with
participants from Germany and from Switzerland
(Swiss-Italian region) who were recruited from the
personal network of the authors and volunteered to
take part in the study. The aim was to cover young,
middle-aged, and senior females and males differing
in their level of technical understanding and their care
experiences.
The interviews (N=12 participants, ranging in age
between 23 and 82 years M=52.67; SD=22.49) were
conducted and analysed. Half of them were females
(50% males). Nationality was not divided as equal as
gender, with interviewing five Swiss, all of them
Italian native speakers and seven Germans, all of
them German native speakers. As their highest
educational level, seven out of all participants stated
to hold an academic degree, among them one
participant holding a doctorate, whereas four
completed vocational training and one person holding
an A-level certificate. Slightly more than half of
participants (i.e., seven participants) stated having
(professional or informal) care experience, three
among them reported working in the medical or care
sector. High levels of technical literacy were
attributed to four participants whereas three were
classified as having low technical literacy. The
remaining five participants ranged in between. No
participant reported hands-on experience and
knowledge of AAL technologies.
All participants agreed to take part in this
empirical study after they were transparently
informed about the use of the collected data as well
as the purpose and aim of this qualitative research. No
compensation was given for participation.
4 RESULTS
In the following, results of the second part of the
interviews will be reported. Findings from this part
might be most relevant in understanding how people
conceptualize privacy in an AAL scenario.
4.1 Descriptive Results
In total, maps of eleven participants were examined
(P2-P12). While every mental map was equally
informative the maps differed in complexity, i.e., the
number of objects included in the map (see Table 1).
Interestingly, P3 the most care experienced
participant (59 years, MA. Nursing and health
sciences, 22 objects) conceptualized the most
complex map with the highest number of objects
included (Figure 1) followed by the youngest,
technically highly skilled participant (23 years, 21
objects). Among the participants who created the
least complex map were the two oldest participants
(both aged 81, low-medium technical literacy, P12
informal care experience, both 7 objects). Participants
with more complex maps (P2, P3, P4, P5, P6, P9,
P10) were able to group their objects into two to six
categories, whereas this was not possible for the less
complex maps of P7, P8, P11, and P12.
Seven participants were able to select one most
important object of the map. Among these chosen
objects were
“Safety” (P2), “The problem of camera
technology”
(P3) “Data Protection” (P5), “unobtrusive
technology”
(P6), “Independence” (P7), “Usefulness”
(P8), and
“Simple Use” (P9). The most important
object of the map was interchangeable, except for two
participants (P5, P8). Participants wished to replace
their most important object with
“increased quality of
life” (P2), “social contacts” (P3), “even more helpful
technology”
(P6), “being cared for by skilled and nice
professional caregivers”
(P7), and “being cared for by the
own two children”
(P9).
Table 1: Descriptive statistics regarding the number of
objects within the maps.
Descri
p
tive Statistics Partici
p
ants
Mean 14,36
Median 12
Mode (bimodal) 7 P7, P11, P12
Mode (bimodal) 12 P8, P9, P10
Max 22 P3
Min 7 P7, P11, P12
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
96
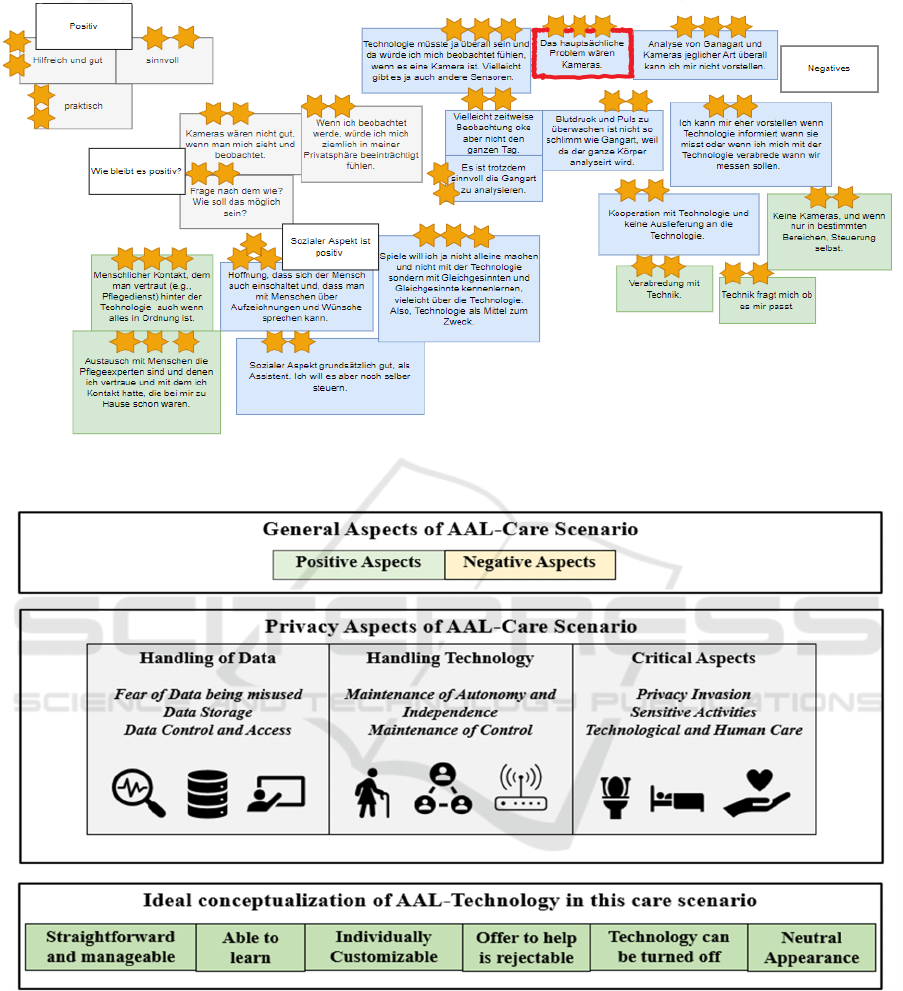
Figure 1: Exemplary schematic visualization of P3`s mental map (in German language). The yellow stars represent the coding
for importance (3 stars = very important). The box framed in red corresponds to the most important object.
Figure 2: Illustration of categories.
4.2 Qualitative Findings
Results from the thematic analysis of the single maps
revealed three major categories, “General Aspects of
the AAL Scenario”, “Privacy Aspects of the AAL
Scenario” and “Ideal Conceptualization of AAL
Technology”.
These three broad classifications were further
divided into several major and minor subcategories.
Allocations are illustrated in Figure 2 and details are
described in the following.
4.2.1 General Aspects of the AAL Scenario
Positive Aspects. Overall, participants mentioned
more general positive than negative thoughts on the
AAL scenario. Indeed, all participants but one (P4)
Exploring Privacy: Mental Models of Potential Users of AAL Technology
97

had a positive first impression, meaning that the first
word they mentioned had a positive connotation.
In general, the AAL technology in this scenario was
considered as
“helpful for oneself” (P3) and “for
relatives”
(P4) as well as “useful” (P8) and “important
for life” (P12).
In addition, some participants even shared more
excitement when asked about their general
impression:
“For me it is fascinating if I fall down, and the system
calls an emergency service.” (P5)
“I am enthusiastic, […] it lights my thoughts. Without
the technology no one knows about my health, and I can
only guess if I am not well. Just thinking that with this
technology there is someone, is a great relief.”
(P10)
Negative Aspects. As what can be identified as
general negative aspects or concerns regarding the
AAL technology, only a few were mentioned.
Participants feared that interaction with AAL devices
would make them particularly aware of their frailty or
in the extreme case be the cause of further health
decline and frailness.
“Every day you are reminded of your frailty, you are
always reminded that you can´t do certain things
anymore and you have the feeling that you are
dependent on this thing. […].”
(P2)
“I am afraid that I am no longer challenged. Basically,
it is like diminishing self-esteem from the outside”
(P4)
4.2.2 Privacy Aspects of the AAL Scenario
Handling of Data. Participants frequently raised the
issue how data is handled in this scenario and
discussed it in various lights. Thoughts concerning
this topic can be divided into three subcategories that
are Fear of Data being misused, Data Storage and
Data Control and Access.
Fear of Data being misused. Participants were
aware that the AAL technology records most of their
everyday activities and health information which
makes the resulting data highly sensitive. Participants
feared fatal consequences if this data would get in
wrong hands.
“A film is a data, a photo is a data, a state of health can
also be another piece of information and I wouldn´t
want many others to know that I have a certain illness.
I mean inappropriate dissemination of data. You have
to understand who is on the other side, […] if one looks
for a specific purpose regarding health okey, but if one
looks to make fun of me then it becomes almost a
crime.” (P10)
Data Storage. How data is stored was only a
matter for participants with high technical
understanding. Indeed, to express preferences, one
might need to know how and where data can be stored
as well as what implication the storage location has
for data security. P5 for instance preferred data to be
stored locally rather than in a cloud.
Data Control and Access. Participants agreed that
the fewer people have access and control of the data,
the better. However, some preferred giving access to
a small circle of trusted people others favoured a care
service. Participants shared the reasons for these
preferences. P6 argued for granting access to a small
circle and gives an example of an
“uptight granny” who
does not want to show the data to anyone even though
it might be helpful. Therefore, she says, that it is
nonetheless important that a small circle of trusted
people has access to the real data because otherwise–
as she put it,
“you might end up cheating yourself.” (P6).
Others, such as P7, would prefer to give access mostly
to a care service to avoid being a burden for family
members and informal caregivers.
“Regarding data access and monitoring, I think it
should be a care service. If something extreme happens,
relatives can always be taken on board. [...] Smaller
issues might arise frequently, and a care service reacts
quickly and maybe comes over. I don´t want the
relatives to worry a lot and then be obliged to keep
checking.” (P7)
Handling Technology. Participants pictured ways
they would interact with such integrated AAL
devices. They discussed to what extent the degree of
autonomy and independence changes and potentially
diminishes in such a scenario. In addition, they
explored latitudes and limits of technology in terms
of keeping or giving up control over oneself. These
thoughts can be summarized into two categories,
namely Maintenance of Autonomy and
Independence and Maintenance of Control.
Maintenance of Autonomy and Independence.
As a first impression, participants felt that such AAL
technology would take away a lot of independence
and control from them and would not consider their
remaining cognitive and physical abilities required in
daily life. One participant having this opinion (P8)
stated that decisions on giving up autonomy and
independence highly depend on,
“the will to extend my
life” (P8) considering beliefs and values on life and
destiny one has at that point in time. Others
concentrated on the meaning of independence and
autonomy discovering that there might be two sides
of the same coin.
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
98

“On one hand something is taken over but then you
keep your independence longer […]. On one hand
deactivated, on the other hand, increased autonomy. It
is perhaps a paradox” (P4)
“I would feel being taken care of as well as being
independent […] I don´t always need someone to come
by all the time but I can actually handle it myself and if
there is something wrong, the system takes care of it, so
I am coping with everyday life” (P2)
Maintenance of Control. Participants thoughts on
handling the technological devices were driven by the
fear of losing control over technology and with that
losing control over oneself. According to participants,
AAL technology should therefore operate based on
individual needs and avoid evoking feelings of being
controlled.
“Technology must serve me when I need it. The
machine must be at my service, and it is not I who must
be at the service of the machine.” (P10)
“When you are so old that you no longer know how to
operate this device you even feel more controlled by the
device. […]. Then, it would be important that the device
is hidden so that you don´t notice it or that the device
helps you to operate it to give you the feeling that it
doesn´t control you.” (P6)
The notion of control in this context was also
viewed as control over information about oneself and
with that control over the own image.
“Imagine if you say that you were doing well last week
and your friend replies: ´No I don´t believe you, I know
your data´. You decide what you tell your friend or how
you felt, and how you generally feel about yourself. You
decide what to tell and what don´t” (P6)
Critical Aspects. Three critical categories were
identified that can be put under the umbrella of
privacy in this AAL scenario. Namely, Privacy
Invasion, Sensitive Activities and Technological and
Human Care.
Privacy Invasion. During the process of creating
the mental map, participants gave concrete examples
regarding critical situations where privacy might be
threatened. Interestingly, some of the participants
considered this threat as rather unproblematic.
“It doesn´t bother me in my situation […] Maybe for the
younger ones it is a disturbance, but I don´t mind those
things, I go around and do things as I am and there is
nothing to hide -I have nothing to hide” (P12)
On the contrary, others mentioned situations
where interference of technology is not desired and
considered as a disturbance of privacy. Among them
P2 and P4 shared examples:
“An example: I am reading something, and I am
concentrating and now technology informs me it is my
turn to take my pills or whatever and I am disturbed. I
think that is an invasion of my privacy.” (P4)
“The more the measurement is noticeable […] thinking
of a moment when I have guests over who could also
see it, then I would feel that my privacy had been hurt.”
(P2)
Sensitive Activities. Activities that are repeatedly
cited as particularly sensitive and critical to monitor
are activities in the bath- and bedroom. In the
bathroom, especially toileting and showering were
concerning. Oftentimes, participants even either
rejected the use of technology in these intimate
moments or accepted it unwillingly.
“I would like it if there were areas without technology
for example in the bathroom or in the bedroom.” (P6)
“What I don´t feel comfortable with is, for example,
when I go to the toilet, knowing that I am being
watched, or other intimate acts that I don´t like to do in
public. […] As long as I understand this cognitively, I
can accept it, even if reluctantly. But I think it becomes
difficult when the mind can no longer grasp it. Then it
becomes a burden.” (P4)
Technological and Human Care. Despite all the
positive aspects mentioned about the AAL
technology in this scenario, participants talked about
their hope that human care and human contact is still
provided or at least complemented with technology.
“The technology is there but maybe one day a human
being will come by. That is what I hope. […] Even if
everything is okey every two days, once a week, you can
talk to a person about these things that were recorded
or about your wishes, that would be good. It doesn’t
matter if all the values are good, you still want to talk
to someone when you are alone” (P3)
“There is no longer a person who helps you and stays
with you all day long and therefore favours an
exchange of social information and physical contact
that a person who is alone may need. This is missing in
this scenario here.” (P8)
4.2.3 Ideal Conceptualization of AAL
Technology
Participants shared their ideal conception of the
technology in this scenario in line with privacy
preferences. This means that participants were asked
how they wanted the technology in this scenario
ideally to be designed in terms of functionalities,
Exploring Privacy: Mental Models of Potential Users of AAL Technology
99
appearance, and interaction. Findings are
summarized in Table 2.
Table 2: Ideal conceptualizations of AAL technology.
Ideal
Conceptualization
of Technology
Description
Straightforward and
manageable
Technology should be simple,
and it should be easy to learn
how to interact with it.
Able to learn Technology should have the
ability to learn about the users,
their habits, and (health)
conditions.
Individually
Customizable
Technology should adapt to the
user´s rhythm of life and each
function should be
customizable and work as the
user wishes.
Offer to help is
rejectable
Users should have the freedom
to refuse help from technology.
Technology can be
turned off
Users should be able to switch
the technolo
gy
off an
y
time.
Neutral Appearance Technology should be hardly
seen, be very subtle and discreet
or at least look like a design
object rather than a health
device.
5 DISCUSSION
The paper presented cognitive maps of potential users
of AAL technology and the resultant findings
regarding their opinions on living with such assistive
devices. This qualitative approach aimed at
understanding thought processes regarding privacy
when in need of care due to age-related frailness and
being supported by AAL technology.
5.1 General Findings and Privacy
Criteria
Overall, and in line with existing literature (e.g., see
Garg et al., 2014; Gövercin et al., 2016; Lorenzen-
Huber et al., 2011; Wild et al., 2008) participants had
a positive impression of themselves using AAL
technology at home in older age and mentioned more
positive than negative aspects.
Participants` opinions of the AAL scenario were
elicited with a cognitive mapping method (3CM).
Maps varied in complexity which is also reasonable
according to Kearney and Kaplan (1997) and maps of
experts tend to have stronger and more objects. In this
study, the sample consisted of non-experts of the
AAL domain, but several participants had
professional care experience and/or a high general
technical understanding. Participants with the least
complex maps were the two oldest participants (both
81 years) both with limited technical understanding
and no professional care experience. One explanation
might be that older adults generally have less
experience with technology compared to younger
adults and therefore have less developed mental
models of how to use them (Ziefle & Bay, 2004).
Opposed to that, the most care experienced,
technically skilled adult (59 years, MA. Nursing and
health sciences) created the most complex map. The
second most complex map was conceptualized by the
youngest technically highly skilled participant. Even
though both participants were not experts in the AAL
domain they had important knowledge in related and
relevant domains of care or technology respectively.
In line with theoretical argumentations (Collins &
Gentner, 1987; Rickheit & Sichelschmidt, 1999), this
knowledge has probably helped in the creation of
their compound mental maps. Previous findings have
already suggested that care experience plays a role in
AAL acceptance (Offermann-van Heek et al., 2019;
Offermann-van Heek & Ziefle, 2019). Related to this,
this study provides hints that care experiences are
strongly reflected in the mental model of an AAL
scenario which focuses on privacy implications.
Findings on privacy in this study can roughly be
allocated to Burgoon`s four dimensions of privacy
(Burgoon, 1982).
Naturally, the category Handling of Data
including its identified subcategories can be assigned
to the dimension of informational privacy (control
over personal information). Data contains intimate
details and therefore the dimension of psychological
privacy might also be relevant for this category.
Findings fit in the picture on AAL acceptance of
previous studies (e.g., Kirchbuchner et al., 2015;
Offermann-van Heek & Ziefle, 2019) confirming data
access and the fear of data misuse as relevant aspects.
The category Handling of Technology including
its subcategories regarding autonomy, independence,
and control might be most closely related to
psychological privacy (degree of inaccessibility to
thoughts, feelings, and intimate information) as well
as social privacy (control over social contacts,
interaction, and communication). Previous studies
show the importance of autonomy and independence
for older adults when interacting with technology
(e.g., Lorenzen-Huber et al., 2011; Ulrich et al.,
2020). Within the subcategory Maintenance of
Autonomy and Independence, several participants
concluded that AAL technology enhanced and
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
100

supported independence and autonomy even though
it invaded a large part of the intimate everyday life.
Previous studies have called it a trade-off between
autonomy and privacy (e.g., Lorenzen-Huber et al.,
2011). In this study, one participant labelled it as a
paradox which might be a less functional description
but it emphasizes the complexity and multificacety of
such an AAL scenario. Control and the feeling of
being in control when using AAL is another core
aspect when interacting with AAL (e.g., Schomakers
& Ziefle, 2019; Ulrich et al., 2020) and has been
summarized in this study in the subcategory
Maintainance of Control. Participants mentioned
their desire to keep control over their data as well as
to keep control over devices including being able to
reject technological offers and being able to turn
devices off completely, as results from ideal
conceptulaizations show.
The category Critical Aspects might somehow
be related to all privacy dimensions. The subcategory
Sensitive Activities might be particularly bounded to
the psychological as well as the physical dimension
of privacy. The latter because the sensitive activities
mentioned are typically done in the bath and bedroom
and some participants even referred to the location.
This is consistent with findings from Himmel and
Ziefle (2016). The importance to complement AAL
with human care and contact is emphasized in the
subcategory Technological and Human Care. The
fact that technology should not replace human care
has already been mentioned previously (e.g.,
Lorenzen-Huber et al., 2011). Indeed, participants
want actual humans to discuss their wellbeing and at
the same time participants consider human physical
contact as important contribution to their wellbeing.
The subcategory Privacy Invasion and several ideal
conceptualizations (i.e., “Able to learn”,
“Individually Customizable”) show that privacy
within an AAL scenario is a very personal matter.
Similarly, concerns especially regarding privacy are
best countered with customizable solutions and
individual support which partly includes human care.
5.2 Method Evaluation
The study procedure was based on the open-ended
3CM method. Participants quickly grasped the
cognitive mapping approach and provided objects to
be written on the cards in the form of entire sentences
or single words. The main constructs assessed were
“general perceptions of AAL in older age”, “privacy
perceptions when interacting with AAL” and “ideal
conceptualization of AAL”. According to Kearney
and Kaplan (1997), construct validity can be
examined by the following three major theoretical
expectations: (1) if participants are able to distinguish
between the objects they own and the ones they do
not (i.e., the extent to which participants are certain
that a specific object belongs in their mental
representation), (2) if hierarchical relationships are
shown through the creation of 5 ± 2 created
categories, and (3) if participants express satisfaction
with the measurement process.
These three criteria for construct validity apply to
most of the sample´s maps. Nonetheless, reliable and
quantifiable practices to test for these criteria during
data collection were limited. Firstly, concerning
ownership of the objects, no specific measures were
taken to test for it. However, participants` were given
time to think about further additions to the map
without being pressured. Without being prompted by
the interviewer, participants were also able to express
when their map was completed. Secondly, theoretical
expectations regarding hierarchical relationships
apply to six out of eleven maps. Indeed, six
participants were able to create minimum two and
maximum six categories and some participants even
provided headlines for each category. Lastly, most
participants expressed satisfaction and enthusiasm
during the mapping exercise. This was shown from
participants` persistent search for additional objects
and their positive comments on this mapping task
during the informal talk after the interview.
Overall, within the scope of available resources
and objectives of the study, reasonable efforts and
measures were taken to ensure construct validity as
best as possible. Furthermore, the high degree of
consistency with existing findings on privacy
perceptions and acceptance of AAL suggest that the
method is appropriate for the assessment of the given
context.
5.3 Practical Implications
The field of AAL connects many disciplines such as
legal, technological, and social disciplines, and
benefits from close inter- and transdisciplinary
collaboration and communication. As such the
reported findings from a social science perspective
might have implications for engineers and designers
as well as lawmakers working on aspects of AAL.
Especially when it comes to the perception of an
“Ideal” Conceptualization of Technology, the
insights of potential users of such AAL devices in
terms of expectations and requirements towards an
accepted technology in line with privacy preferences
might be informative for other disciplines and
Exploring Privacy: Mental Models of Potential Users of AAL Technology
101

professional groups. From the results, several key
principles can be outlined:
Usability. AAL users want to feel in control of
technology, being able to turn it off and to manage it
easily, even with little technological knowledge. This
means, the usability of the AAL interface is key.
Interaction with the interface should be simple and
explainable in a few steps. If users know how to
navigate the device, their feeling of control will be
enhanced.
Framing and Information Style. Even though
AAL might support crucial tasks of daily life,
technological support should never be provided in an
authoritarian and domineering way. Ideally, users
should barely be aware of the technological support
they receive. This might be accomplished with
technological features that enable customization and
personalization of AAL devices. Acceptance and
integration of AAL in daily life becomes more natural
for users if devices can quickly adapt to personal
rhythms and preferences of each user. Preferences
can range from technological functioning, interaction
modality and data sharing to the actual design and
visibility of AAL.
AAL should Match Individual (Design)
Preferences at Home. Indeed, AAL does not only
need to fit to users` life rhythms but also to their own
home and the way users feel at home. The own four
walls are a place of refuge, creativity, and wellbeing
and not a healthcare facility. Despite its purpose of
care and health monitoring, AAL and particularly its
hardware should be designed to reflect standards of
home interior.
Perception of Control should Be Considered by
Legal Framing. Furthermore, this study bears
another implication especially regarding legal
aspects. Again, the notion of control plays a crucial
role. In fact, participants, as potential users, stated to
prefer being in control of technology but at the same
time, they emphasized the importance of being in
control of the data captured by the devices. They want
to know and decide with whom, how, and when data
is logged and shared. At the same time, potential data
misuse and hacking are a great concern. As users
might decide on data access and storage based on
their personal preferences, the legal framework
should enable a broad range of data elaboration
methods while ensuring rights of users and allow for
strict prosecuting in cases of misuse.
Those key features should be considered in future
professional education not only for care personnel but
also for technical designers and persons that are in
charge of providing legal frameworks. The more such
user aspects are considered from the very beginning
of technological development, the higher will be the
potential of acceptance of AAL technologies. This
especially applies to the type of technology under
study. In particular, camera technologies and sensors
as essential parts of AAL technology might be
important when it comes to perceptions of privacy.
Thus, based on current research (Wilkowska et al.,
2021), future studies should focus on the specificity
of privacy perceptions of visual technologies at home.
5.4 Limitations and Future Research
The applied qualitative procedure was an explorative
study to evaluate the methodological approach,
including the 3CM Method, and its suitability to
examine privacy perceptions within an AAL context.
It proofed useful in getting the participants to think
and reflect thoroughly about the given AAL scenario
and the implications for privacy. Nonetheless, the
validity of the method has limitations as outlined
previously.
Related to the representativeness of the method
might be the fact that the present qualitative
assessment was scenario-based and did not evaluate
actual technology and real-life experience and
knowledge of the given domain.
Furthermore, as the study was explorative, the
AAL scenario used for the creation of mental maps
was very generic. Indeed, the technology described
had many functions and left a lot of space to the
imaginary. To attain more elaborate cognitive maps
the technology presented should be more specific and
its functioning should be explained more explicitly.
Ideally, participants should have the opportunity to
test the actual technology for a determinate period
prior to the assessment of their mental representations
regarding it.
The semi-structured interviews all lasted roughly
one hour, and the mental mapping procedure was
created in the second half. The long duration might
have been challenging especially for older
participants who sometimes showed difficulties in
concentrating until the end of the interview. Future
studies attempting to study mental conceptualizations
might solely focus on the creation of the mental map
without any further questions.
The present study was conducted in two
neighbouring countries in Europe, namely Germany
and Switzerland (Italian-speaking region). No
remarkable differences between answers of
participants could be identified due to nationality. For
future studies, the approach of this study should be
applied in other non-European countries to compare
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
102

mental conceptualizations of privacy within AAL in
different cultures and certain healthcare systems.
ACKNOWLEDGEMENTS
Authors thank all participants for their enthusiasm,
patience, and openness to share their opinions during
the interview sessions. We also thank Sophia Otten
and Alexander Hick for research support. This work
resulted from the project VisuAAL “Privacy-Aware
and Acceptable Video-Based Technologies and
Services for Active and Assisted Living” and was
funded by the European Union’s Horizon 2020
research and innovation programme under the Marie
Skłodowska-Curie grant agreement No 861091.
REFERENCES
Altman, I. (1976). Privacy A Conceptual Analysis.
Environment and Behavior, 8(1), 7–29.
Bergström, A. (2015). Online privacy concerns: A broad
approach to understanding the concerns of different
groups for different uses. Computers in Human
Behavior, 53, 419–426. https://doi.org/10.1016/
j.chb.2015.07.025
Beringer, R., Sixsmith, A., Campo, M., Brown, J., &
McCloskey, R. (2011). The “acceptance” of ambient
assisted living: developing an alternate methodology to
this limited research lens. Proceedings of the
International Conference on Smart Homes and Health
Telematics, Toward Useful Services for Elderly and
People With Disabilities., 161–167.
https://doi.org/10.1007/978-3-642-21535-3_21
Blackman, S., Matlo, C., Bobrovitskiy, C., Waldoch, A.,
Fang, M. L., Jackson, P., Mihailidis, A., Nygård, L.,
Astell, A., & Sixsmith, A. (2016). Ambient Assisted
Living Technologies for Aging Well: A Scoping
Review. Journal of Intelligent Systems, 25(1), 55–69.
https://doi.org/10.1515/jisys-2014-0136
Burgoon, J. K. (1982). Privacy and Communication. Annals
of the International Communication Association, 6(1),
206–249.
https://doi.org/10.1080/23808985.1982.11678499
Calvaresi, D., Cesarini, D., Sernani, P., Marinoni, M.,
Dragoni, A. F., & Sturm, A. (2017). Exploring the
ambient assisted living domain: a systematic review.
Journal of Ambient Intelligence and Humanized
Computing, 8(2), 239–257. https://doi.org/10.1007/
s12652-016-0374-3
Collins, A., & Gentner, D. (1987). How people construct
mental models. In D. Holland & N. Quinn (Eds.),
Cultural models in language and thought. (pp. 243–
268). Cambridge University Press.
Craik, K. J. W. (1943). The nature of explanation.
Cambridge University Press.
Demiris, G., Rantz, M. J., Aud, M. A., Marek, K. D., Tyrer,
H. W., Skubic, M., & Hussam, A. A. (2004). Older
adults’ attitudes towards and perceptions of “smart
home” technologies: A pilot study. Medical Informatics
and the Internet in Medicine, 29(2), 87–94.
https://doi.org/10.1080/14639230410001684387
Garg, V., Camp, L. J., Lorenzen-Huber, L., Shankar, K., &
Connelly, K. (2014). Privacy concerns in assisted living
technologies. Annales Des Telecommunications/Annals
of Telecommunications, 69(1–2), 75–88.
https://doi.org/10.1007/s12243-013-0397-0
Gövercin, M., Meyer, S., Schellenbach, M., Steinhagen-
Thiessen, E., Weiss, B., & Haesner, M. (2016).
SmartSenior@home: Acceptance of an integrated
ambient assisted living system. Results of a clinical
field trial in 35 households. Informatics for Health and
Social Care, 41(4), 430–447. https://doi.org/10.3109/
17538157.2015.1064425
Hamidi, F., Poneres, K., Massey, A., & Hurst, A. (2020).
Using a participatory activities toolkit to elicit privacy
expectations of adaptive assistive technologies.
Proceedings of the 17th International Web for All
Conference, W4A 2020, April. https://doi.org/10.1145/
3371300.3383336
Himmel, S., & Ziefle, M. (2016). Smart Home Medical
Technologies: Users’ Requirements for Conditional
Acceptance. I-Com, 15(1), 39–50. https://doi.org/
10.1515/icom-2016-0007
Johnson-Laird, P. N. (1983). Mental Models. Cambridge
University Press.
Kaplan, S., & Kaplan, R. (1982). Cognition and
Environment: Functioning in an uncertain world.
Ulrich Books.
Kearney, A. R., & Kaplan, S. (1997). Toward a
methodology for the measurement of knowledge
structures of ordinary people: The conceptual content
cognitive map (3CM). In Environment and Behavior
(Vol. 29, Issue 5, pp. 579–617).
https://doi.org/10.1177/0013916597295001
Kirchbuchner, F., Grosse-Puppendahl, T., Hastall, M. R.,
Distler, M., & Kuijper, A. (2015). Ambient Intelligence
from Senior Citizens’ Perspectives: Understanding
Privacy Concerns, Technology Acceptance, and
Expectations. AMBIENT INTELLIGENCE, AMI 2015,
9425, 48–59.
Kitchin, R. M. (1994). Cognitive maps: What are they and
why study them? Journal of Environmental
Psychology, 14(1), 1–19. https://doi.org/10.1016/S027
2-4944(05)80194-X
Kuckartz, U. (2014). Qualitative Text Analysis A Guide to
Methods, Practice Using Software (K. Metzler (ed.)).
SAGE Publications.
Lehto, R., & Therrien, B. (2010). Death concerns among
individuals newly diagnosed with lung cancer. Death
Studies, 34(10), 931–946. https://doi.org/10.1080/
07481181003765477
Lorenzen-Huber, L., Boutain, M., Camp, L. J., Shankar, K.,
& Connelly, K. H. (2011). Privacy, Technology, and
Aging: A Proposed Framework. Ageing International,
Exploring Privacy: Mental Models of Potential Users of AAL Technology
103

36(2), 232–252. https://doi.org/10.1007/s12126-010-
9083-y
Muñoz, A., Augusto, J. C., Villa, A., & Botía, J. A. (2011).
Design and evaluation of an ambient assisted living
system based on an argumentative multi-agent system.
Personal and Ubiquitous Computing, 15(4), 377–387.
https://doi.org/10.1007/s00779-010-0361-1
Nissenbaum, H. (2010). Privacy in Context: Technology,
Policy, and the Integrity of Social Life. Stanford
University Press.
Oates, M., Ahmadullah, Y., Marsh, A., Swoopes, C.,
Zhang, S., Balebako, R., & Cranor, L. F. (2018).
Turtles, Locks, and Bathrooms: Understanding Mental
Models of Privacy Through Illustration. Proceedings
on Privacy Enhancing Technologies, 2018(4), 5–32.
https://doi.org/10.1515/popets-2018-0029
Offermann-van Heek, J., Schomakers, E.-M., & Ziefle, M.
(2019). Bare necessities? How the need for care
modulates the acceptance of ambient assisted living
technologies. INTERNATIONAL JOURNAL OF
MEDICAL INFORMATICS, 127, 147–156.
Offermann-van Heek, J., & Ziefle, M. (2019). Nothing else
matters! Trade-offs between perceived benefits and
barriers of AAL technology usage. Frontiers in Public
Health, 7(JUN), 1–16. https://doi.org/10.3389/
fpubh.2019.00134
Peek, S. T. M., Wouters, E. J. M., van Hoof, J., Luijkx, K.
G., Boeije, H. R., & Vrijhoef, H. J. M. (2014). Factors
influencing acceptance of technology for aging in
place: A systematic review. International Journal of
Medical Informatics, 83(4), 235–248.
https://doi.org/10.1016/j.ijmedinf.2014.01.004
Pollack, M. E. (2005). Intelligent technology for an aging
population: The use of AI to assist elders with cognitive
impairment. AI Magazine, 26(2), 9–9.
Ray, H., Wolf, F., Kuber, R., & Aviv, A. J. (2019). “Woe is
me:” Examining older adults’ perceptions of privacy.
Conference on Human Factors in Computing Systems -
Proceedings, 1–6. https://doi.org/10.1145/3290607.33
12770
Ray, H., Wolf, F., Kuber, R., & Aviv, A. J. (2021). “Warn
Them” or “Just Block Them”?: Investigating Privacy
Concerns Among Older and Working Age Adults.
Proceedings on Privacy Enhancing Technologies,
2021(2), 27–47. https://doi.org/10.2478/popets-2021-
0016
Rickheit, G., & Sichelschmidt, L. (1999). Mental models:
some answers, some questions, some suggestions. In G.
Rickheit & C. Habel (Eds.), Mental models in discourse
processing and reasoning. (pp. 9–40). Elsevier.
Schomakers, E. M., & Ziefle, M. (2019). Privacy
perceptions in ambient assisted living. ICT4AWE 2019
- Proceedings of the 5th International Conference on
Information and Communication Technologies for
Ageing Well and e-Health, Ict4awe, 205–212.
https://doi.org/10.5220/0007719802050212
Selke, S. (2016).
Lifelogging: Digital self-tracking and
Lifelogging-between disruptive technology and cultural
transformation. (S. Selke (ed.)). Springer.
Thagard, P. (2010). How brains make mental models. In L.
Magnani, W. Carnielli, & C. Pizzi (Eds.), Model-based
reasoning in science and technology: Abduction, logic,
and computational discovery. Springer, Germany.
Ulrich, F., Ehrari, H., & Andersen, H. B. (2020). Concerns
and trade-offs in information technology acceptance:
the balance between the requirement for privacy and the
desire for safety. Communications of the Association
for Information Systems, 47, 227–247.
https://doi.org/10.17705/1CAIS.04711
van Heek, J., Himmel, S., & Ziefle, M. (2018). Caregivers’
perspectives on ambient assisted living technologies in
professional care contexts. Proceedings of the 4th
International Conference on Information and
Communication Technologies for Ageing Well and E-
Health., 37–48. https://doi.org/10.5220/0006691400
370048
van Heek, J., Himmel, S., & Ziefle, M. (2017). Helpful but
spooky? Acceptance of AAL-systems contrasting user
groups with focus on disabilities and care needs.
ICT4AWE 2017 - Proceedings of the 3rd International
Conference on Information and Communication
Technologies for Ageing Well and e-Health, April, 78–
90. https://doi.org/10.5220/0006325400780090
Van Hulle Vincent, C. (2007). Nurses’ Perceptions of
Children’s Pain: A Pilot Study of Cognitive
Representations. Journal of Pain and Symptom
Management, 33(3), 290–301. https://doi.org/10.1016/
j.jpainsymman.2006.08.008
Wild, K., Boise, L., Lundell, J., & Foucek, A. (2008).
Unobtrusive in-home monitoring of cognitive and
physical health: Reactions and perceptions of older
adults. Journal of Applied Gerontology, 27(2), 181–
200. https://doi.org/10.1177/0733464807311435
Wilkowska, W., Offermann-van Heek, J., Florez-Revuelta,
F., & Ziefle, M. (2021). Video Cameras for Lifelogging
at Home: Preferred Visualization Modes, Acceptance,
and Privacy Perceptions among German and Turkish
Participants. International Journal of Human-
Computer Interaction, 00(00), 1–19.
https://doi.org/10.1080/10447318.2021.1888487
Yusif, S., Soar, J., & Hafeez-Baig, A. (2016). Older people,
assistive technologies, and the barriers to adoption: A
systematic review. International Journal of Medical
Informatics, 94, 112–116. https://doi.org/10.1016/
j.ijmedinf.2016.07.004
Ziefle, M., & Bay, S. (2004). Mental models of a cellular
phone menu. Comparing older and younger novice
users. Lecture Notes in Computer Science (Including
Subseries Lecture Notes in Artificial Intelligence and
Lecture Notes in Bioinformatics), 3160, 25–37.
https://doi.org/10.1007/978-3-540-28637-0_3
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
104
