
Medical Treatment with a Remote Care Technological Solution
Diego Marca-Mariaca, Oscar Medina-Poemape and Willy Ugarte
a
Universidad Peruana de Ciencias Aplicadas (UPC), Lima, Peru
Keywords:
Remote Care, Mobile Application, Cloud Computing.
Abstract:
The care service for the treatment of diseases is an activity that is performed in person, which uses the usual
flow of appointment reservation and waiting time to access care, so that the diagnosis was provided and
subsequently the appropriate treatment. Here, we present the development of a technological architecture
that will allow you to manage user information to optimize the service in which you can reduce appointment
booking time, attention time and even compliance with treatments remotely. Validation of the work proposal
was carried out through a mobile solution in the test scenario that functioned as a pilot to demonstrate the
feasibility of outpatient care service and to keep remote follow-ups to patients treated against the pathology of
overweight. The results show the feasibility of our proposal.
1 INTRODUCTION
In Peru, the application of therapy in the public sector
is applied to people who are generally adult patients
between 40 and 70 years old, who opt for this method
of treatment
1
.
However, the current care model for therapy is car-
ried out in the traditional way, that is, in person so that
allows the diagnosis and identification of the appro-
priate treatment for the patient can be completed.
This process requires the face-to-face meeting of
the specialist doctor and the patient for the follow-up
of the treatment, since the material used in the pa-
tient’s data can remain on average eight days (Lee
et al., 2008; Hou et al., 2015).
Given this, for the patient this process implies
non-compliance with the treatments prescribed, since
it requires a significant amount time lost in accessing
the service due to the following factors.
First, according to the national institute of statis-
tics and informatics (INEI) published in February
2020, shows the average wait time to set an appoint-
ment can be up to two and a half days regardless if it
is public or private.
The same study also indicates that the average
waiting time for the patient to be seen is approxi-
mately 51 minutes at the national level.
In addition, the average commute time to reach
the health center is calculated to be approximately 31
a
https://orcid.org/0000-0002-7510-618X
1
Essalud (in Spanish) - 2016
minutes due to various factors such as the location be-
tween users and vehicular traffic
2
.
The benefits of the therapy required significant of
monitoring and control to improve the physical and
mental well-being of the patients.
Monitoring patients through telemedicine makes
possible to obtain patterns or make future predictions
for patient treatment.
Our contributions are as follows:
• We develop a mobile solution that provides care
service for treatment of diseases.
• We propose a solution to encourage patients to
comply with the treatments, so that the benefits
of applying this therapy will be performed.
These treatments do not require invasive methods,
and these benefits will empower the patient im-
prove their physical and mental well-being.
• We expect to provide the medical care service re-
motely to patients efficiently.
This work is organized as follows. Section 2 presents
the study of the related works. Section 3 describes the
technological proposal and the case study completed.
Finally, experimental results are presented to validate
the feasibility of our proposal.
2
INEI (in Spanish) - 2020
Marca-Mariaca, D., Medina-Poemape, O. and Ugarte, W.
Medical Treatment with a Remote Care Technological Solution.
DOI: 10.5220/0011041300003188
In Proceedings of the 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2022), pages 213-219
ISBN: 978-989-758-566-1; ISSN: 2184-4984
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
213

2 RELATED WORKS
In (Chen et al., 2018), the authors present an intelli-
gent system, called Healthcare System App, for the
health care of university students in Taiwan by estab-
lishing an interactive diet in which users can record
the contents of their diet, nutrients and their exercise
routines anytime, anywhere.
The main result that was identified in the study
was that the application helped students to achieve the
proposed objectives:
• 75% reached the breakfast goal.
• 90% reached the lunch goal.
• 90% reached the exercise goal.
Unlike them, we have established a treatment that in-
teracts with the specialist doctor through the mobile
solution platform.
The contribution of (Luhanga et al., 2018) was to
present an application that includes the influences and
interaction of social support with attachments to phys-
ical activities, identifying certain requirements and
specifications that users require for its use.
The main results of this study were that 63.04%
of the challenges were completed and that the appli-
cation had a rating of 3.04 out of 5 (Luhanga et al.,
2018). Unlike them, we have implemented an evalua-
tion module in the style of a form.
In (Kronborg et al., 2018), the authors analyze pa-
tient data in the Telehomecare trial using home mea-
surements through prediction models based on logis-
tic regression.
The main result that was identified in the study
was that the optimal combination of predictors (using
three physiological predictors and exacerbations) ex-
cluding the incidence of exacerbation in patients and
populations.
The contribution of (Almeida et al., 2010) is to
implement an alternative application that allows the
monitoring of patients with amyotrophic lateral scle-
rosis using Telehome monitoring devices that ensures
the transmission of data and request for medical as-
sistance.
The work configuration evidenced the number of
hours of use per day, the percentage of spontaneous
respiration, backup respiratory rate, average respira-
tory rates and the percentage of pressures that were
reached contributed to an increase in the respiratory
activation sensitivity, where the patient felt comfort-
able with a normal respiratory rate.
In contrast, we implemented a tracking system
through weekly evaluations where the patient records
user data to track its evolution.
In most of the work, the characteristic is that
through the use of different technological tools they
can maintain continuous monitoring of patients for
the benefit of health.
3 METHOD
In this section we present the main concepts and ar-
chitecture for our proposal.
3.1 Preliminary Concepts
3.1.1 Technological Architecture
This enterprise architecture model presents a more
complete perspective of how you will develop and de-
ploy your application components.
This has four layers, which are business, logic,
data and physics that act as a basis for the efficient
performance of the information systems that support
the service and solution provided users.
The architecture design presents a series of steps
to be considered to determine the structure and orga-
nization of the information systems
These include the components, functions, nodes,
operating systems, data instances and physical de-
vices such as servers computers, mobile equipment,
among others that must be defined (Syynimaa, 2019;
Lugma
˜
na-Hidalgo and Garrido, 2019).
The main components of our proposal are as fol-
lows:
1. Business Architecture: The business architec-
ture is defined as the layer that presents the busi-
ness strategy through a set of requirements speci-
fied in mapping the processes.
To complete, it is important to analyze the pro-
cesses that make up the current state and identify
deficiencies that can be improved so that stake-
holders achieve their business objectives (Ma-
suda, 2021; Niemi and Pekkola, 2020).
2. Data Architecture: This layer manages the phys-
ical and logical information, which will present
information through views.
It is responsible for storing the information in in-
stances which must be consulted by the business
stakeholders (Masuda, 2021; Niemi and Pekkola,
2020).
3. Logical Architecture: The architecture layer
shows the technical aspects for the solution cre-
ated, where the functions developed for the appli-
cation that are based on business processes and
requirements are used.
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
214

It is important to emphasize that this layer is con-
tained in the technological layer because physi-
cal executions are required for operation (Masuda,
2021; Niemi and Pekkola, 2020).
4. Physical Architecture: In this layer, the lowest-
level components of the solution are presented.
The support the elementary resources for the con-
tinuation of the business such as directories, apps,
databases, emails, etc.
Therefore, this layer is essential for the correct
execution of the implemented solution, guaran-
teeing the correct flow of communication and al-
low for the continuity of the strategic objectives of
the business (Masuda, 2021; Niemi and Pekkola,
2020).
3.1.2 Cloud Service
It is a tool that through its design allows easy access to
applications or resources over the internet without the
need to pay for hardware with dedicated components.
The adoption of services is naturally at the request
of the client or company user.
In this global context, people make use of these
services consciously even if they do not have deep un-
derstandings of the of technologies.
Thus, the management of these cloud services are
provided by experts in the field of Cloud Computing
who provide information backup, application hosting,
among others.
Likewise, the services provided to meet customer
needs are called Infrastructure as a Service (IaaS) and
Platform as a Service (PaaS)
3
.
1. Infrastructure as a Service (Iaas): Cloud ser-
vice that is oriented for IT system administrators
who require IT resources from providers so as
not to pay for local infrastructure installations and
maintenance (e.g., Amazon Web Services, Google
Compute Engine, and Microsoft Azure
3
).
2. Platform as a Service (Paas): Cloud service that
are targeted to application developers, provide ca-
pabilities such as database, operating system, and
a programming language to meet the needs of de-
velopment environments
3
.
3.2 Mobile Solution
This proposal consists on implementing a mobile so-
lution that will provide medical care service for peo-
ple who require treatment of diseases.
3
What is a cloud service? - Citrix - 2020
A series of phases has been identified that will al-
low us to understand the proper flow of our work.
The phases of the mobile solution are detailed be-
low:
1. Phase 1 (Analysis): The problem was analyzed
and, secondly to complement the data, surveys
were carried out to contextualize the usual tasks
required of the users, so that the service could be
optimized remotely, including the reservation of
the appointment, history of symptoms, means of
health monitoring, waiting time for care and time
during care.
Thus, the analysis of the app stores of Apple and
Android, to locate any apps related to the tasks
required in the environment.
In addition, in order to identify tangibles in our
proposal, we had the need to find programming
environments to be used and the Cloud service
that through its characteristics would allow the de-
velopment. of the proposal (e.g., Android Studio
and Microsoft Azure).
2. Phase 2 (Technological Architecture and De-
velopment): This process is presented in Fig 1
and shows the logic application layer found in the
application design, including the part of the sys-
tem with which the user interacts shown.
These interfaces make use of controllers to com-
municate with the back-end and the processing
logic to make the application work.
The data layer is where we store our components
as CRUD operations this includes links to the Mi-
crosoft MySQL database service.
In summary, both the patient interface and the spe-
cialist interface through the use of mobile data or
Wi-Fi network to connect to the API hosted in Mi-
crosoft Azure where the business logic layer and
the Data layer are located, which is finally linked
with MySQL.
3. Phase 3 (Evaluation Process): This process re-
quires to start with the functional tests that in our
case we validate all the flows that the mobile so-
lution incurs.
Then we have the identification of the case study,
considering the recommendations of the clinic
and the influx of patients to collect the sample
group.
After, we have the validation where the volunteers
were instructed their execution of the mobile so-
lution was supervised.
A product satisfaction survey to capture opportu-
nities in how to improve the mobile solution will
be analyzed.
Medical Treatment with a Remote Care Technological Solution
215
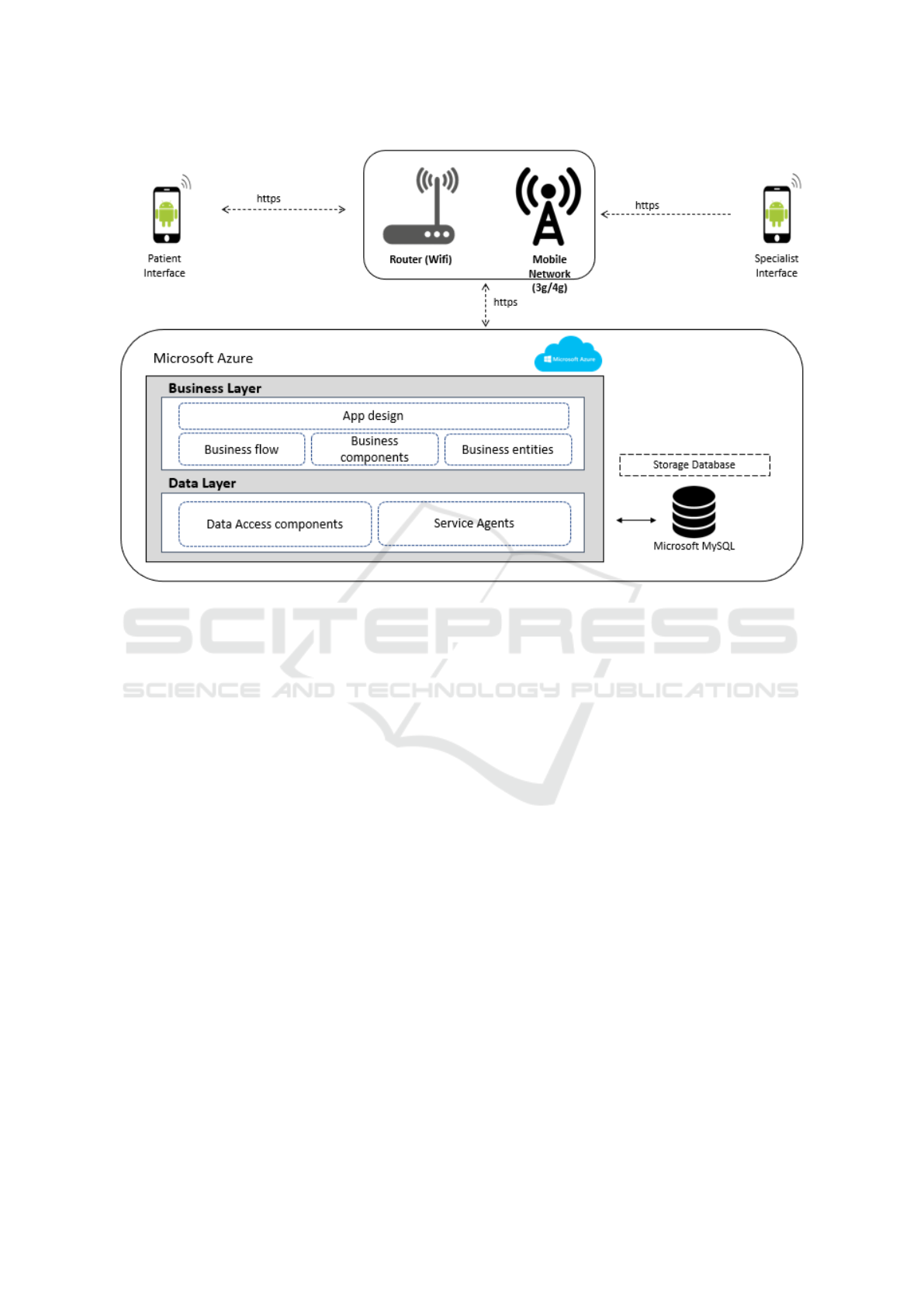
Figure 1: Deployment Architecture Model.
As a final step, the indicators would be evaluated.
4 EXPERIMENTS
The experimentation of this work had three valida-
tion sources which compare between the average re-
sults shown by outpatient care process in the public
and private places, the results of the compliance of
the treatment remotely and the satisfaction of the user
using the mobile application.
4.1 Experimental Protocol
The solution was developed using the .NET and
Kotlin programming language, which made it possi-
ble to obtain the expected backend and frontend func-
tionalities.
In addition, it requires the CloudinaryAPI, which
enables the solution to manage the upload of images
in the cloud.
The APK of our proposal is publicly available at
https://bit.ly/2HckOU5.
4.2 Test Scenario
The validation of the proposed model was carried out
in a medical center downtown district of Lima, Peru,
with 15 patients and one specialist representing 10%
of the patients for the month during the COVID-19
pandemic.
In this validation, the volunteers used the mo-
bile solution to record the appointments and request
a treatment, allowing a specialist to display applica-
tions and address them through their mobile devices.
The patients underwent a process where they
recorded essential information; height, age, weight
and a photo of their ear, so that the specialist can in-
struct the therapy points and maintain control of the
patient’s treatment evolution.
4.3 Results
Table 1 (columns 2 and 5) shows how greatly reduced
the time to choose the proper attention of the first 3
items, where the results of the MINSA (Public Hospi-
tal) months before COVID 19 pandemic started, com-
pared to our proposal where the average time to book
the appointment, waiting time and the time to arrive
at the establishment were reduced by 86.36%, 91.8%
and 100% respectively.
It should be noted that this public information
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
216
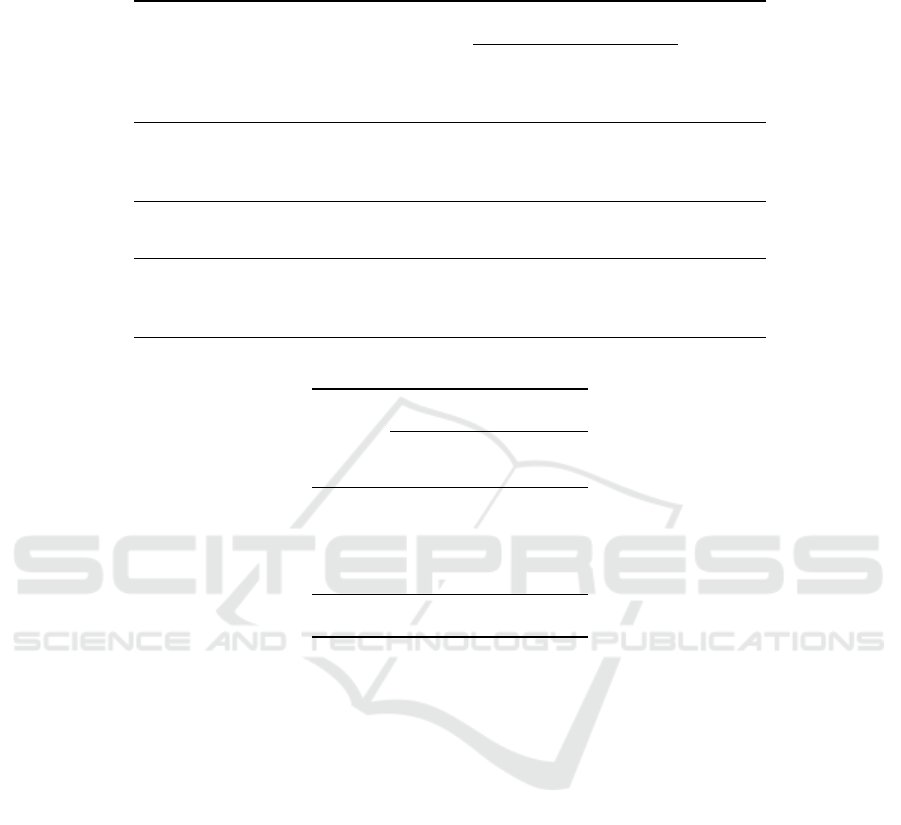
Table 1: Main results.
(a) Comparison of current situation with our solution.
Public Entity
Service
Private
Entity
(minutes)
Before
Pandemic
(minutes)
After
Pandemic
(minutes)
Our
Solution
(minutes)
Average time
to reserve the
appointment
22 5 5 3
Average wait
time for care
49 24 8 4
Average time
to reach the
establishment
31 50 70 -
(b) Results of the Remote Process.
BMI Average
Age
State
Before
Treatment
After
Treatment
Young 27.94 27.62
Adult 24.86 24.71
Elderly 26.83 26.42
Average 26.69 26.41
does not consider the information during the COVID-
19 pandemic, because the official report was not avail-
able at the time of the study.
In Table 1 (columns 3 and 4), where the data given
by the private establishment before the pandemic is
compared with our proposed solution, it is possible to
reduce the treatment wait time in that order between
40%, 83.3% and 100% respectively.
Additionally in the same establishment during the
pandemic, the reservation time of the appointment,
waiting to receive attention and commuting to the es-
tablishment was reduced by 40%, 50% and 100% re-
spectively.
In Figure 2, there is the result of the treatment for
the overweight where there is evidence of a decrease
in the Body Mass Index (BMI) after the sessions ac-
cording to the person’s life cycle, where the young
person (14 to 29 years old) reduced by 1.17%, the
adult (30 to 34 years) in 0.64% and the elderly (45 to
60 years) in 1.55%.
Other result of the treatment for the overweight is
a decrease in the Body Mass Index (BMI) after the
sessions, where the BMI for young people (14 to 29
years old) reduced by 1.17%, for the adults (30 to 34
years) in 0.64% and for the elderly (45 to 60 years) in
1.55%.
4.4 Discussion
As we can see all the results given by Fig 1, we es-
timate a quantitative improvement, that reduces the
time of care in a public or private establishment that
provides treatments.
In addition, according to the results given by
Fig 1b and 2, the volunteer patients when following
the specialist’s instructions through the mobile solu-
tion were able to stimulate the atrial cavity according
to the recommended points.
And according to their age groups they managed
to decrease the body mass index.
After this, in our mobile solution obtained good
to satisfactory references in the survey completed by
volunteers where 54% corresponding to the Fig 2
were found satisfied with the mobile solution.
Fig 2 shows that 67% of the people found the mo-
bile solution process very efficient.
Medical Treatment with a Remote Care Technological Solution
217
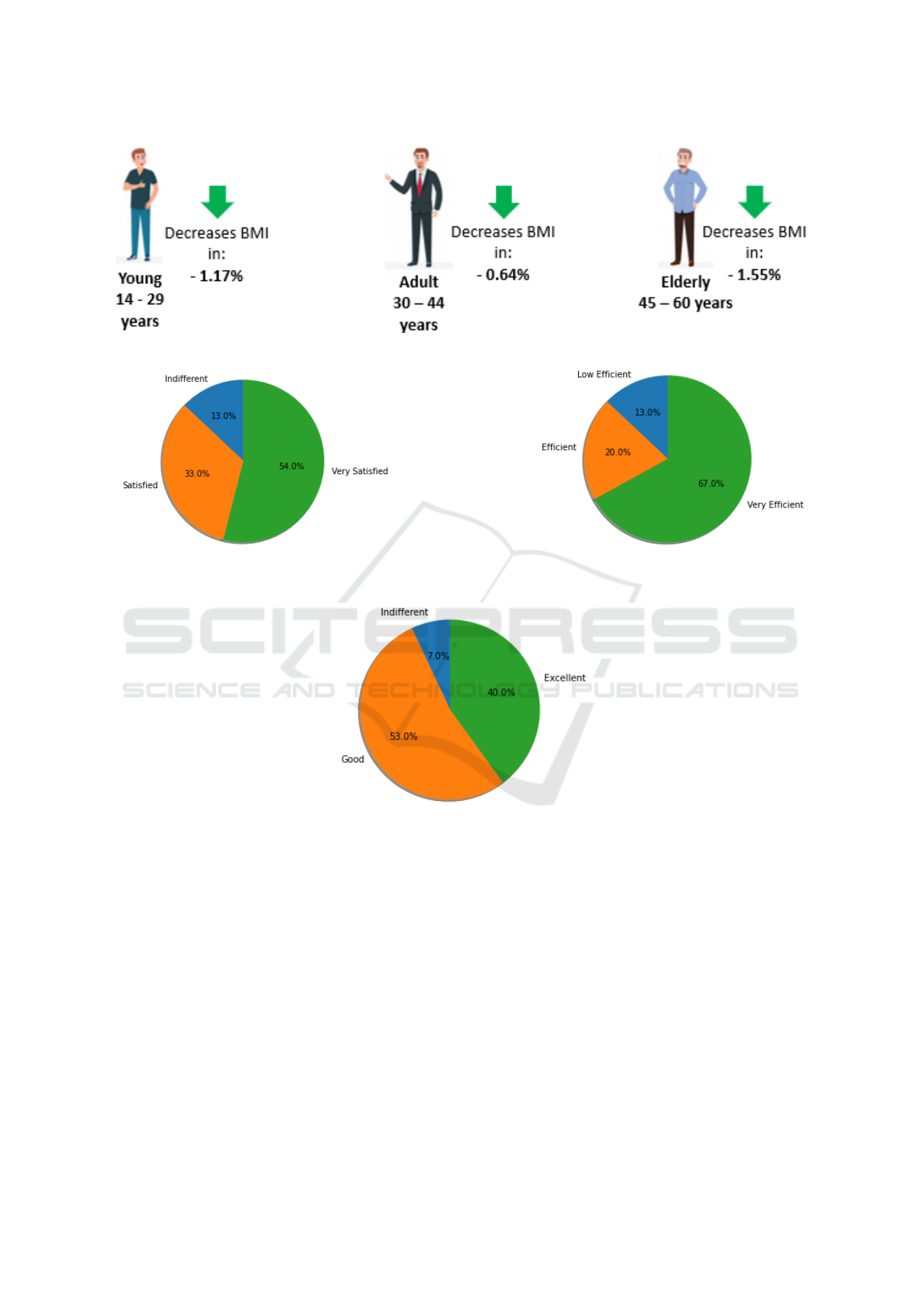
(a) Results of the Remote Process.
(b) Satisfaction for the Mobile Solution Function-
alities.
(c) Efficiency of Mobile Solution Process.
(d) User Experience w.r.t. the Mobile Solution.
Figure 2: Comparison of results for different criteria.
In Fig 2, 40% found the user experience with the
solution excellent.
5 CONCLUSION
In conclusion, our mobile solution based on our tech-
nological architecture improves the patient experi-
ence to maintain control and monitoring the treat-
ments.
On one hand, the deployment of this solution en-
ables to optimize remote care by registering appoint-
ments and going to specialized centers to access care.
On the other hand, the data collected from our vol-
unteers treated against being overweight through our
mobile solution showed that patients were able to de-
crease their BMI during the first week of the session,
therefore, our proposal is able to provide follow-up
and control towards patients requiring remote therapy
care.
Our results show that the implementation of tech-
nologies such as Machine Learning and image recog-
nition, would greatly improve the automation the spe-
cialist’s instructions identifying the diseases and leads
to a better diagnosis.
Furthermore, using Genetic information to seek
for historical data about a patients (Arroyo-Mari
˜
nos
et al., 2021) or monitoring symptoms with a simi-
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
218

lar technological solution for other diseases (Jorge-
L
´
evano et al., 2021).
REFERENCES
Almeida, J., Pinto, A., Pereira, J., Pinto, S., and de carvalho,
M. (2010). Implementation of a wireless device for
real-time telemedical assistance of home-ventilated
amyotrophic lateral sclerosis patients: A feasibility
study. Telemedicine journal and e-health : the official
journal of the American Telemedicine Association, 16.
Arroyo-Mari
˜
nos, J. C., Mejia-Valle, K. M., and Ugarte, W.
(2021). Technological model for the protection of ge-
netic information using blockchain technology in the
private health sector. In ICT4AWE.
Chen, S., Chiang, D., Chen, T., Lin, H., Chung, Y., and Lai,
F. (2018). An implementation of interactive healthy
eating index and healthcare system on mobile plat-
form in college student samples. IEEE Access, 6.
Hou, P.-W., Hsu, H.-C., Lin, Y.-W., Tang, N.-Y., Cheng, C.-
Y., and Hsieh, C.-L. (2015). The history, mechanism,
and clinical application of auricular therapy in tradi-
tional chinese medicine. Evidence-Based Compl. and
Alt. Medicine, 2015.
Jorge-L
´
evano, K., Cuya-Chumbile, V., and Ugarte, W.
(2021). Technological solution to optimize the
alzheimer’s disease monitoring process, in metropoli-
tan lima, using the internet of things. In ICT4AWE.
Kronborg, T., Mark, L., Cichosz, S. L., Lilholt, P. H., and
Hejlesen, O. K. (2018). Population exacerbation inci-
dence contains predictive information of acute exacer-
bations in patients with chronic obstructive pulmonary
disease in telecare. IJMI.
Lee, M. S., Shin, B.-C., Suen, L. K. P., Park, T.-Y., and
Ernst, E. (2008). Auricular acupuncture for insomnia:
a systematic review. Int. Jour. of Clinical Practice,
62(11).
Lugma
˜
na-Hidalgo, F. and Garrido, J. L. (2019). Implement-
ing a business/technology architecture alignment-
oriented process applied to the social-sanitary sector.
In IOV.
Luhanga, E. T., Hippocrate, A. A. E., Suwa, H., Arakawa,
Y., and Yasumoto, K. (2018). Identifying and evalu-
ating user requirements for smartphone group fitness
applications. IEEE Access, 6.
Masuda, Y. (2021). Digital enterprise architecture for global
organizations. In Architecting the Digital Transforma-
tion, Intel. Syst. Ref. Lib. Springer.
Niemi, E. I. and Pekkola, S. (2020). The benefits of en-
terprise architecture in organizational transformation.
Bus. Inf. Syst. Eng., 62(6).
Syynimaa, N. (2019). Technology architecture as a driver
for business cooperation: Case study - public sector
cooperation in finland. In ICEIS.
Medical Treatment with a Remote Care Technological Solution
219
