
An Ethical Framework for Big Data and Smart Healthcare
Victor Chang
1a
, Rahman Olamide Eniola
2b
, Ben Shaw-Ching Liu
3c
and Mitra Arami
4a
1
Department of Operations and Information Management, Aston Business School, Aston University, Birmingham, U.K.
2
Cybersecurity, Information Systems and AI Research Group, School of Computing, Engineering and Digital Technologies,
Teesside University, U.K.
3
Department of Marketing, Lender School of Business Center, Quinnipiac University Hamden, CT 06518, U.S.A.
4
Pardis Limited, London and EM Normandie Business School, France
Keywords: Ethics for AI and Data Science, Ethical Framework, Ethics for Smart Healthcare.
Abstract: There has been significant growth in big data technology in healthcare in recent years. However, the potential
of big data analytics is affected by various ethical and security concerns, which have hampered the application
of big data analytics in healthcare. Recently, numerous studies have been conducted on the emerging big data
ethical issues in healthcare. While most of the journal reflects on privacy and security questions, it did not
examine; objectively the possible discriminatory impact of big data analytics has no. This mixed-method
project aims to highlight various ethical problems in big data analytics while also providing an in-depth insight
into the biased results derivable from big data analytics and the effects of such outcomes.
1 INTRODUCTION
Higher healthcare investment in a nation can provide
better health prospects that can enhance human
capital and increase productivity, thus contributing to
economic performance (Raghupathi and Raghupathi,
2020; Cutillo et al., 2020). However, the exponential
growth in the world's population presents a critical
threat to current medical and healthcare systems (Zhu
et al., 2019). The change in population demographics,
the increase in the number of aged people, and the
drastic increase in the cost of in-hospital services all
lead to realizing the value of effective healthcare
systems (Demirkan, 2013). The professional-to-
patient ratio is another factor that led to the rise in
demand for an efficient healthcare system (Borodin et
al., 2016).
With the explosive growth of disruptive
technologies in recent years, the speed and quantity
of digital data collected have expanded steadily and
rapidly (Chang, Shi and Zhang, 2019).
Correspondingly, the evolution of information
technology and the introduction of digitized computer
a
https://orcid.org/0000-0002-8012-5852
b
https://orcid.org/0000-0001-9799-861X
c
https://orcid.org/0000-0002-2950-9607
c
https://orcid.org/0000-0001-6855-9888
systems has resulted in the transition of conventional
hard copy medical data to Electronic Health Records
(EHR) and Electronic Medical Records (EMR)
systems (Rehman, Naz and Razzak, 2021). These
systems resulted in exponential data expansion
(Razzak, Imran and Xu, 2020), which has contributed
to the growth of big data analytics, especially in
healthcare.
According to a 2021 Grand View Research, Inc.
study, the worldwide healthcare analytics market was
valued at USD 23.6 billion in 2020, projected to rise
at a Compound Annual Growth Rate (CAGR) of 23.8
percent from 2021 to 2028 (‘Healthcare Analytics
Market Size Industry Report: 2021-2028’, 2021). See
Figure1.
This massive increase fulfills the growing need
for improved healthcare, aided by innovative
technology.
Administrative claim reports, hospital registries,
electronic records of health, biometric data, patient
data, the internet, medical imaging, biomarkers,
prospective cohort studies, and clinical trials are
possible medical big data sources in healthcare
(Hermon and Williams, 2014; Luo et al., 2016).
Chang, V., Eniola, R., Liu, B. and Arami, M.
An Ethical Framework for Big Data and Smart Healthcare.
DOI: 10.5220/0011030900003206
In Proceedings of the 4th International Conference on Finance, Economics, Management and IT Business (FEMIB 2022), pages 65-74
ISBN: 978-989-758-567-8; ISSN: 2184-5891
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
65

Figure 1: Healthcare Analytics market in the USA, by end
user, 2018 – 2028 (USD Million).
These sources; are aggregated to produce fast and
cost-effective prescriptive, descriptive, and
diagnostic insights for the healthcare stakeholders.
While strategically analyzing data for insightful
analysis is crucial, the existence of different data
types accessible from numerous sources makes big
data management extremely difficult (Nair, 2020).
Despite the aforementioned benefits of big data
technology, it is worth remembering that big data
analytics has its drawbacks due to its intertwinement
with people's sensitive personal information, daily
behavioral patterns, and potential prospects. The most
pressing concerns of big data analytics are privacy
(Francis, 2014), confidentiality and informed consent
(Ioannidis, 2013), epistemic hurdles (Floridi, 2012),
and the analysis of monitoring in a growing
datafication of the society (Ball et al., 2016). Indeed,
the assurance of privacy and safety of subjects
through the application of big-data analytics are of
significant importance and high priority. The study by
IBM (IBM, 2019) in Figure 2 shows that the health
sector has suffered an average overall cost of data
breaches considerably higher than other sectors such
as hospitality, media, and research. Healthcare data
should be securely kept, and big data analytics
performed ethically (Mittelstadt, 2019).
Figure 2: Trend of Industry Average Data Cost (IBM,
2019).
The possibility of potential discrimination is
among the most alarming yet understudied issues of
big data technology. There is no universally accepted
definition of discrimination. The term generally refers
to acts, practices, or policies that impose a relative
disadvantage or treat a person or specific group of
people differently, especially in a worse way than
treating other people because of their skin color,
gender, sexuality, language, or other factors (Reinsch
and Goltz, 2016).
The research (Obermeyer et al., 2019) that
revealed pervasive racism in decision-making
systems utilized by US clinics is an excellent
demonstration of discrimination in healthcare
analytics. Participants who self-identified as black
were rated lower risk scores than equally ill white
people in the study. Consequently, black individuals
were less likely to be referred for more personalized
medical care (Obermeyer et al., 2019).
The emergence of these instances describes why
discrimination in big data analytics has become an
emerging topic in a variety of fields, from data
science and artificial intelligence to psychology,
culminating in a dispersed and fractured
interdisciplinary corpus that tends to make
thoroughly accessing the foundation of the problem
difficult (Favaretto et al., 2019).
This study summarized big data and its use in
healthcare, addressing current ethical and security
issues relevant to big data application in healthcare.
Moreover, we suggest several alternative solutions to
compromise between the application and the ethical
obligation.
2 LITERATURE REVIEW
Big data and big data analytics are arguably the pillars
of other disruptive technologies, providing the
necessary business insights for patients, experts, and
government (Wong, Zhou, and Zhang, 2019). Big
data analytics is the method of storing, processing,
and analyzing vast collections of data to find trends
and other valuable knowledge (Heyman et al., 2004).
These massive and complex big data collections are
manipulated and managed using various
computational methods such as machine learning and
artificial intelligence (Ward and Barker, 2013). The
advent of advanced technology has provided
conditions and procedures for voluminous databases
to be compiled and processed, resulting in informed
decision-making in addressing health problems (Raja
et al., 2020).
FEMIB 2022 - 4th International Conference on Finance, Economics, Management and IT Business
66

Big data has emerged as a promising option with
the potential to revolutionize the healthcare system by
lowering costs and optimizing treatment process,
delivery, and management (Patil and Seshadri, 2014).
The application of big data comes with some ethical
issues that demand careful consideration (Camilleri,
2020). Suresh and Guttag (2019) explain how bias
problems occur, how they apply to specific
applications, and how they inspire various solutions.
They also present a framework for understanding
analytical bias at a higher level of abstraction to
facilitate constructive dialogue and solution
development.
Notwithstanding the amount of data generated in
healthcare, the underlying challenge remains in the
integration, of structured and unstructured health
data. According to Dridi et al. (2020), approximately
80% of clinical data is unstructured: and widely
underutilized, once generated. Different clinical data
formats, such as scanned canned medical documents,
prescriptions, patient registries, and clinician notes,
result in poor standardization of healthcare data,
making it more difficult to handle by EHR systems
and more prone to bias from data preprocessing (Cave
et al., 2019; Dridi et al., 2020).
Patient privacy invasion is an emerging problem
in big data analytics. Patients' behavior and sentiment
data can be obtained from various online sources. For
example, an online drug retailer may have recorded
the purchase of a particular medication, a ride-hailing
app may have recorded a visit to a clinic or lab, or a
social media app may have recorded patients'
interactions with a medical web page. Furthermore,
patients' data can also be extracted unethically via
health-care-specific applications and wearable
devices.
Also, we studied several publications to grasp
better the potential discriminatory effects and popular
drivers of discrimination or inequality in big data
analytics on subjects. Different writers arrived at
different conclusions. Big data analytics may result in
unintentional discrimination (Žliobaitė, 2017;
Sonawane and Irabashetti, 2015). Žliobaitė (2017)
established that discrimination is indirect, not by the
analyst's intention but because of the structure and
noise of experimental data. Such algorithms may
systematically disfavor persons belonging to
particular groups or categories, rather than depending
purely on individual merits.
Conversely, other academic studies emphasized
intentional discrimination (e.g., Kuempel, 2016;
Sonawane and Irabashetti, 2015). According to
Kuempel (2016), data brokers frequently combine
raw components of personal data in a discriminatory
way, leaving customers exposed to exploitative and
distasteful marketing techniques. The effect of
utilizing such a biased dataset with sensitive
information is that such individuals or groups of
people would lead to direct discrimination.
Suresh and Guttag (2019) explain how bias
problems occur, how they apply to specific
applications, and how they inspire various solutions.
They also present a framework for understanding
analytical bias at a higher level of abstraction to
facilitate constructive dialogue and solution
development.
3 RESEARCH QUESTIONS AND
BIG DATA ANALYTICS
ARCHITECTURE
The first step of the research was to identify relevant
research questions. The main research question is,
"given the many applications and benefits of big data
and big data analytics in healthcare, do the ethical
risks overshadow the benefits?"
To answer this main question, we need to find
answers to the following sub-questions:
1. What are the applications of big data in
healthcare?
2. What are the current ethical issues of healthcare
big data analytics?
3. What is the cause of discrimination in big data
analytics?
The big data analytics framework utilized in this
project is a blend of many steps that explains the big
data Analytics procedure (shown in Figure 3 above).
The first phase in the framework is data preparation,
which involves the ETL, i.e., Extraction,
Transformation, and Loading of the data. Extraction
is the process of determining the data type to be
utilized and collecting it from different data sources,
such as existing databases and repositories, APIs, and
the cloud. Data transformation is the next step in
which data is transformed, aggregated, and loaded
into the Power Business Intelligence (BI) dashboard.
Figure 3: Power BI architecture.
An Ethical Framework for Big Data and Smart Healthcare
67
The transformation step is to ensure the: (1) handling
of inconsistencies and missing values in the data; (2)
elimination of duplicate data; (3) removal of useless
data; and (4) sorting of data into the appropriate type.
Figure 3 below illustrates the overview of the Power
BI analytics procedure.
The visualization step involves taking the
processed outputs and transforming them into
meaningful insights by viewing the results in
diagrams, KPIs, or other easy-to-understand formats.
It is crucial to ensure that results can be interpreted by
those with no previous experience or expertise.
Unlike other tools, Power BI allows the integration of
different programming languages. Applying Python
and R functionalities while using the DAX and M-
language formulas is the advantage of Power BI. It
gives a better result due to the combined strengths of
different programming languages.
4 APPLICATION AND BENEFITS
OF BIG DATA ANALYTICS
4.1 Preventive Medicine
Preventive medicine is arguably the most innovative
application of big data analysis which employs
cutting-edge data analytics methods: for disease
detection and classification, association analytics,
and clustering, with the promise of efficiently
discovering valuable patterns by analyzing large
amounts of unstructured, heterogeneous, non-
standard data (Razzak et al., 2020). Appropriate
disease prevention involves identifying and treating
at-risk patients. To increase therapeutic adherence,
several preventative strategies are employed.
Pertinent data, such as body temperature, pulse, and
blood pressure, are electronically collected, enabling
automated risk prediction. Consonantly, the increased
usage has contributed significantly to the
appropriateness of big data analytics in healthcare
(Rehman et al., 2021). The aggregate of these data is
analyzed to assist patients with diets, reminders of
preventative care, personalized medical care, follow-
up on prior consultations and medicines, and
counseling (Razzak et al., 2020).
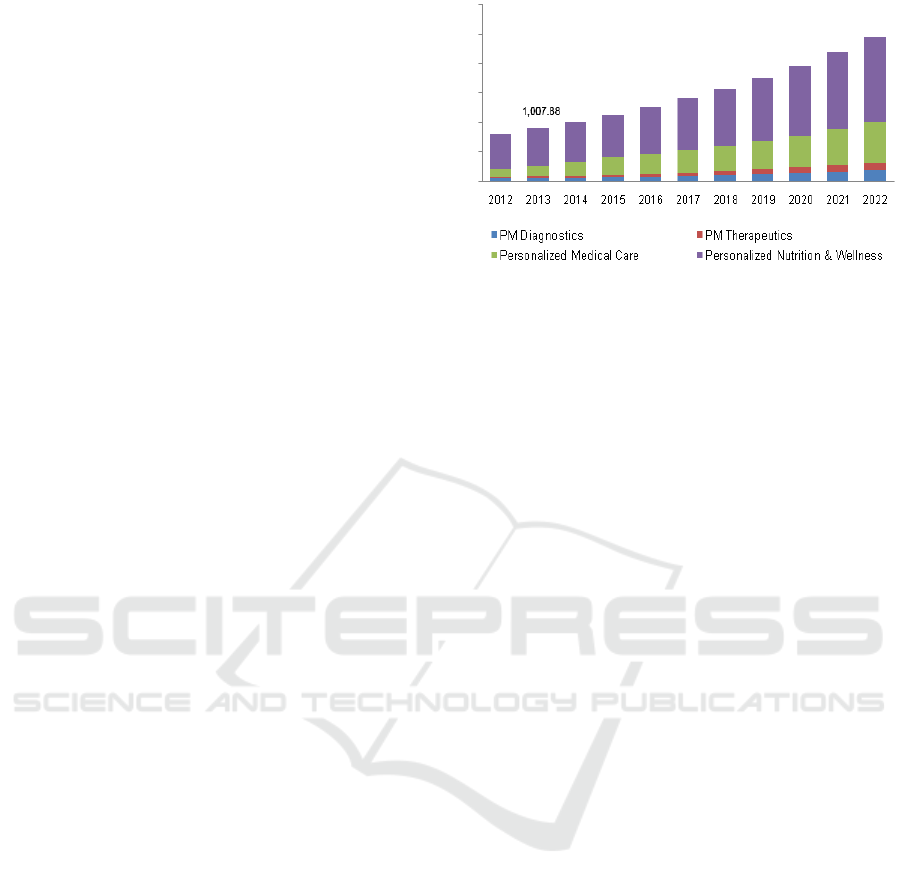
Due to the considerably broad customer base,
relatively few regulatory obligations and ease of
access to wearable devices and medical apps,
personalized medical care has significantly increased
its market size, as shown in Figure 4.
Figure 4: Trend of Personalized Medicine (2012 -2022).
4.2 Evidence-based Healthcare
Traditional healthcare is changing from expedient
and discretionary decision-making to evidence-based
medical practices (Piai and Claps, 2013).
Evidence care is a healthcare practice where we
base the patients' conditions on scientific proof.
Through consolidating data from various outlets, big
data offers evidence-based treatment. The data trends
and patterns would provide sufficient support for
diagnosis and treatment (Piai and Claps, 2013).
4.3 Enhancement of Public Health
Monitoring
The analysis of healthcare data with ground-breaking
methods aids in the epidemic trends analysis, disease
outbreaks monitoring, and the spread of disease. This
approach improves public health monitoring,
education, and reaction time. An excellent example is
the Covid 19 pandemic surveillance system in the
United Kingdom which offers a daily update of a
postcode district-based location with infection rates
in that district, generates a risk score, and
communicates it to the user. Furthermore, the app
allows users to check into a specific place, recording
their presence at that particular time and date. The app
also stores an individual's check-ins with the name
and IDs of such locations, which work with the test
and trace teams to inform users on association with a
particular area at a given time. For example, suppose
someone visits a local bar and is tested positive with
Coronavirus. In that case, the app alerts everyone who
has also checked in the same place to self-isolate or
quarantine.
FEMIB 2022 - 4th International Conference on Finance, Economics, Management and IT Business
68
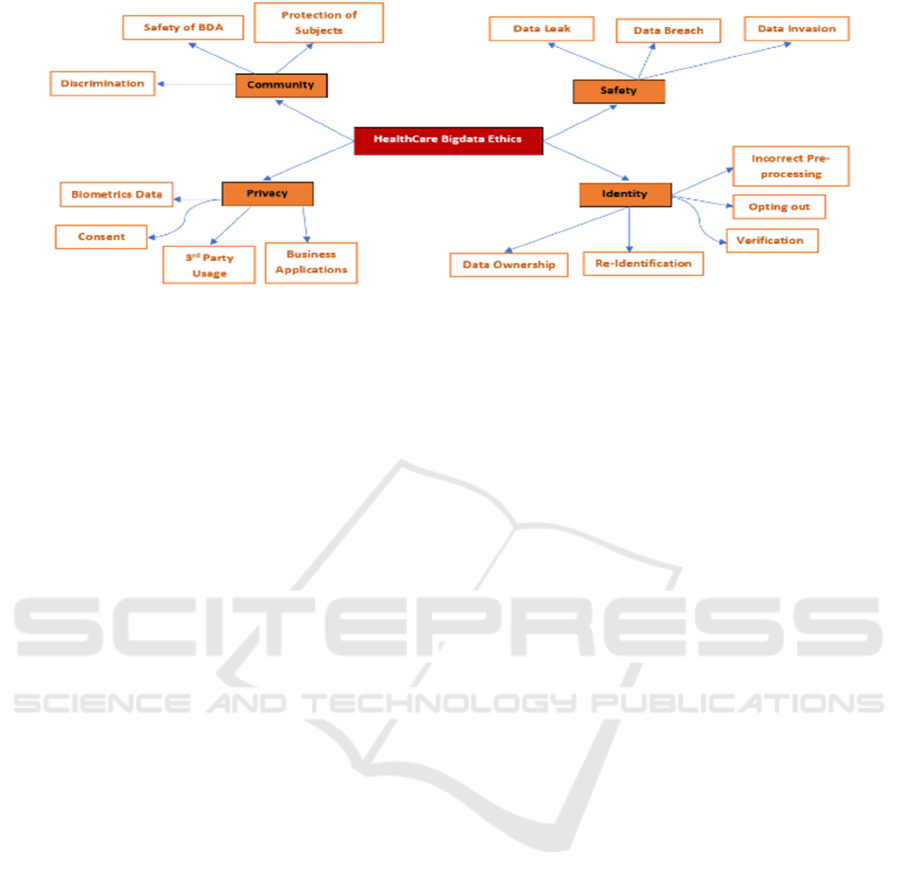
Figure 5: Emerging Ethical Issues in Healthcare Big data.
4.4 Improves Interaction between
Healthcare Providers and Patients
Big data technology also improves collaboration
between healthcare providers and patients. For
example, on social media, people with common
health conditions and healthcare professionals with
similar specialties across the world can share
information on the treatment and cure of some
illnesses, thereby promoting interaction within health
systems.
5 METHODOLOGY
5.1 Systematic Literature Review
The complete literature review of the paper deals with
'big data in healthcare' based papers and studies
published in scholarly journals focuses on the
following objectives:
• Understanding the concept of big data for
healthcare.
• Recognizing tools and techniques for big data
analytics in healthcare.
• Underlining the future benefits and uses of big
data in healthcare.
• Reviewing emerging ethical concerns of big
data systems in healthcare.
We obtained most of the pertinent papers used for this
study from Research Gate, IEEE, and Google Scholar
research sources, which we used to explore for the set
of specific articles related to the proposed research.
We used an inclusion basis to choose big data and
healthcare papers to find relevant papers to answer
research questions based on predefined keywords.
Our aim is to support developing an emerging ethical
framework for Healthcare big data, as shown in Figu
5.2 The Diabetes Dataset (UCL
Repository)
Since millions of healthcare data points are created
and shared daily, a central data repository that
aggregates the entire dataset in one location is needed
(Luo et al., 2016). We also need powerful tools to
extract information rapidly and analyze the selected
data effectively. While Power BI will give healthcare
organizations visibility into their data and help them
gather many insights, other more effective analytics
tools should also be considered. Furthermore, even
though the data has been de-identified, there are other
ethical issues and concerns that we will discuss in the
subsequent section of the article (Durcevic, 2020).
5.3 Research Surveys
In this project, we used primary data collected by the
authors' team from randomly selected respondents
and a pre-processed dataset originally obtained from
Health Information National Trends Survey HINTS 4
Cycles 1 (NCI, 2012).
5.3.1 Primary Research Survey
We used Sogo Survey to conduct the primary
research questionnaire to extract respondents'
concerns with big data analytics and ensure that the
required data is retrievable intelligently.
Unlike the traditional approach, an online survey
makes retrieval and analysis of the relevant
information more accessible. Power BI visualization
is appropriate because it can display complex data in
an interactive and user-friendly manner. To move this
forward, 53 people filled the survey, and we will
address the results in the following segment.
An Ethical Framework for Big Data and Smart Healthcare
69
5.3.2 Secondary Research Survey
We used the pre-processed first cycle HINTS 4
survey, conducted on 3959 responders between
October 2011 and February 2012, with a response rate
of 36.7 percent. Five questions, labeled A-E, were
listed, and are discussed further below.
A. Concerns of unauthorized access to their
health records as they are transferred
electronically between healthcare facilities.
B. Concerned about unauthorized access to
their records as they are faxed between
healthcare professionals.
C. Satisfied that protections were in place to
shield their patient records from unwanted
access.
D. Satisfied that they had a voice in collecting,
using, and exchanging their medical records.
E. Hidden details from a healthcare provider
out of respect for the patient's safety?
We used the following concepts in this work.
6 ANALYSIS AND FINDINGS
6.1 Ethical Problems of Big Data
Analytics in Smart Healthcare
As mentioned earlier, this project discusses some
emerging ethical concerns of big data in healthcare,
including discrimination, data breaching and privacy
issues as delineated in the following. We also discuss
further how some ethical issues could lead to
potential discrimination.
6.1.1 Discrimination
Big data analytics can potentially exacerbate pre-
existing demographic gaps in healthcare by
presenting biased results from the algorithm used
(Cahan et al., 2019; Cutillo et al., 2020). The data
used to train these algorithms contributes more to
such generalization or stereotypes against a group.
Racial biases embedded in typically biased training
datasets are more likely to yield racially
discriminatory predictive models (Cutillo et al.,
2020). For example, the predictive models derived
from the Framingham Heart Study and precision
medicine protocols centered on European ancestry
(Paulus et al., 2018). The causes of discriminatory
bias in a dataset could occur at different phases of an
analytical pipeline (Suresh and Guttag, 2019).
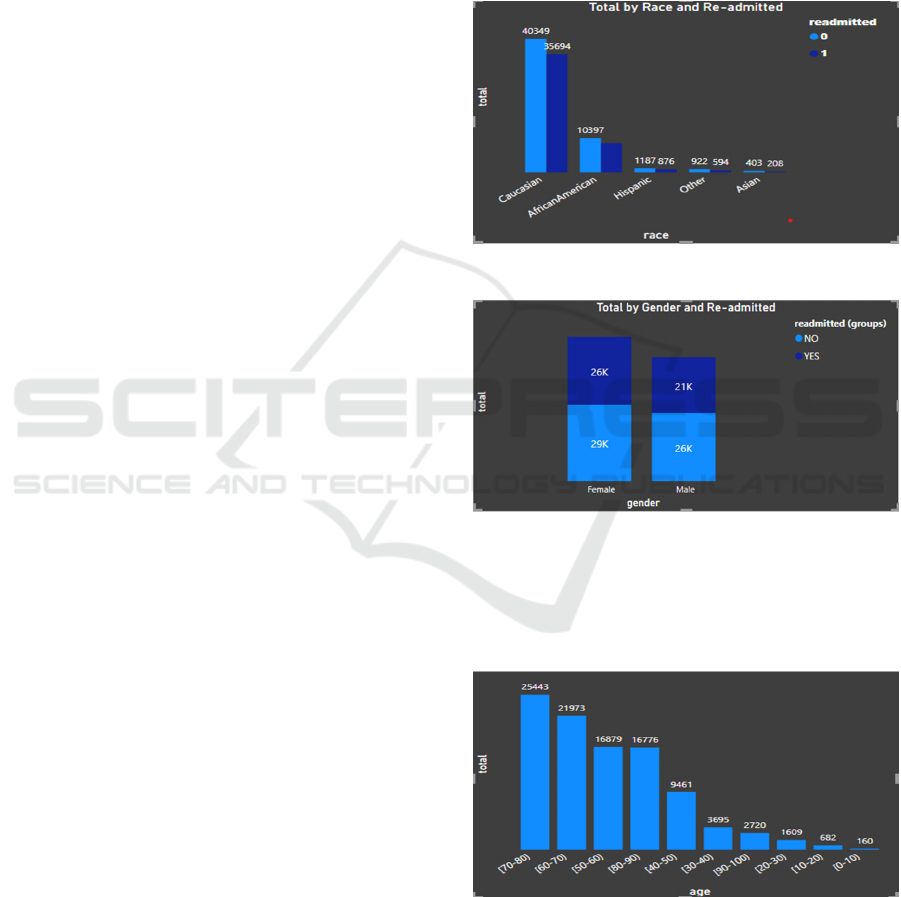
As observed in Figures 6 & 7 below, the Diabetes
readmission dataset used in this project is highly
imbalanced. The dataset has an overrepresentation of
the Caucasian race, leading to a false generalization.
Additionally, there is an aggregation bias in the
dataset as it is hard to know which group (race) is
others. While the gender feature is well represented,
the LGBT populations can feel unfairly aggregated
with the two genders.
Figure 6: Number of Readmissions by Race.
Figure 7: Number of readmissions by Gender.
On the other hand, we cannot say there is an
underrepresentation based on age because it is rare for
people below 20 years to be diabetic (as shown in
Figure 8 below).
Figure 8: Number of Readmissions by Age.
The model analysis with Power BI Key Influencer
(shown in Figures 9 & 10 below) identified
evaluation bias. It revealed that Asians, Hispanics,
FEMIB 2022 - 4th International Conference on Finance, Economics, Management and IT Business
70

African Americans, and people weighing between 0
and 25kg are unlikely to be readmitted.
Figure 9: What factors Influences Readmission to be No.
However, Caucasians and people weighing more
than 200kg are more likely to be readmitted due to
Diabetes. This finding could lead to a misleading
generalization of readmitting Caucasian patients
weighing more than 200kg even though they are fine.
Figure 10: What factors Influences Readmission to be Yes.
Conversely, it might also lead to refusal of
admission for patients who do not identify as White
or do not weigh up to 200kg.
The aforementioned analytical outcome might
lead to social exclusion, marginalization, and
stigmatization. Because some persons may be picked
out and excluded or included due to the bias, the
revelation and application of this study may result in
stigma and discrimination. The possible implication
could be prioritizing hospital spaces for some patients
or refusing to readmit other patients due to their racial
identity. The possible implication could also be
prioritizing hospital spaces for some patients or
refusing to readmit other patients due to their body
weight. This finding is consistent with Obermeyer et
al.'s (2019) research, identifying how big data
analytics could be discriminatory, affecting patients'
treatment plans.
6.1.2 Data Breach
Breach of protected health information (PHI) security
substantially impacts individuals and healthcare
institutions (Agaku et al., 2014). The annual cost of
stolen or compromised PHI in the US healthcare
sector is estimated to be up to $7 billion. According
to research conducted by IBM Security (2019),
healthcare data is the most cost of all sectors, with
continuous growth in the number of breaches. Figure
11 illustrates that healthcare has the highest average
cost of a data breach, almost twice the global average.
Figure 11: Average cost of data breach by industry.
Big data Ethical challenges are not isolated issues
as data breaches could result in the disclosure of
personal health information and financial or medical
identity theft. In some cases, it can result in severe
health consequences on patients (Agaku et al., 2014).
Furthermore, a data breach may result in disclosing
hitherto undetectable behavioral or psychographic
tendencies (Winter, 2018). Data from seemingly
insignificant daily routines is gradually being pooled
and utilized to uncover behaviors or patterns,
clustering or associating individuals into separate
groups, resulting in unfair generalizations against
such groups. Unauthorized access to private
information or activities, such as medical data, could
be used to discriminate against persons seeking
immigration eligibility, medical treatment, education,
banking, and jobs (Winter, 2018).
6.1.3 Privacy
Privacy is a fundamental human right that allows one
to choose between exposing or not to expose
themselves to others and the rest of the world (Chang,
Shi and Zhang, 2019). From the primary survey
results shown in Figures 12 & 13, most people agree
that big data analytics technologies are functional in
healthcare. However, respondents are concerned
An Ethical Framework for Big Data and Smart Healthcare
71
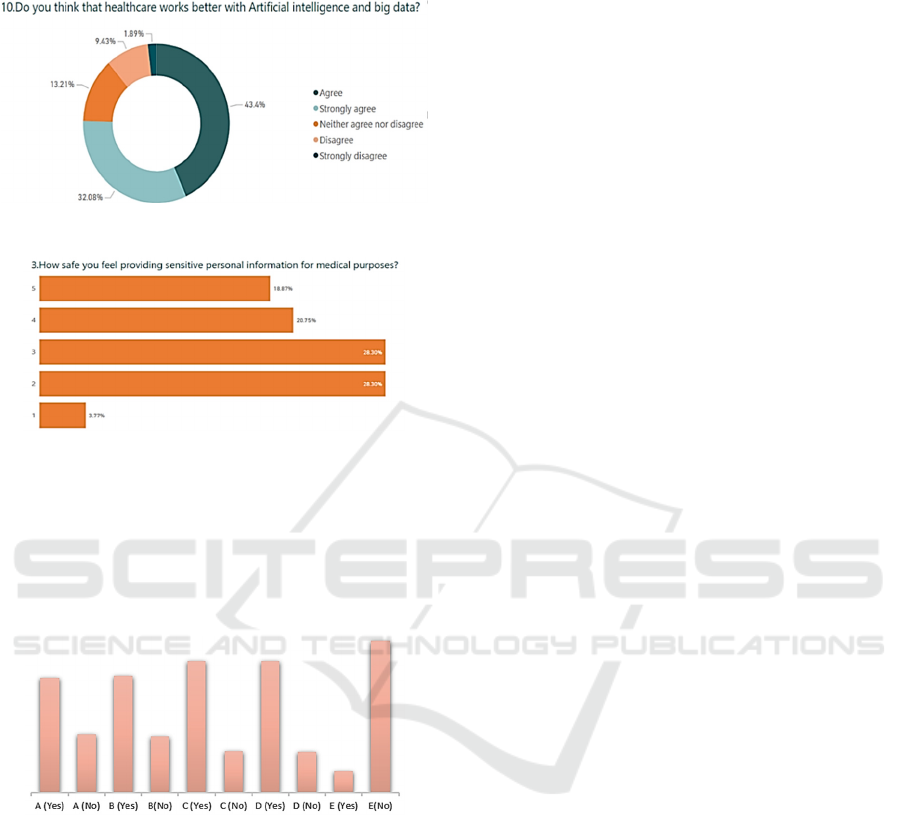
about the sensitivity of healthcare data, which may
jeopardize their privacy.
Figure 12: Big data and AI in Healthcare.
Figure 13: Sensitive Data.
The HINT (NCI, 2020) survey results (shown in
Figure 14 below) indicate that, while the majority of
respondents are concerned about unauthorized access
to their health records, they have confidence that
medical providers and institutions would value their
voice and therefore keep their data secure.
Figure 14: HINT Survey Results.
Personal data can be retrieved at different stages
of analytics (Dev Mishra and Beer Singh, 2017).
Since modern healthcare services demand patients to
provide private and sensitive information to access
medical services, clients lose control over the
confidentiality of their data when they hand over
personal information to third parties and rely on the
organization to safeguard its security. Such
dependence increases the risk of information leakage
if the trusted entity does not implement proper
security measures to secure client data (Mariani,
Mohammed, and Mohammed, 2015). Protection of
patients should be prioritized by avoiding any type of
surveillance or unauthorized identification.
7 EVALUATION AND
DISCUSSION OF FINDINGS
7.1 Conclusion and Implications
Removing private information to increase patients'
anonymity is a powerful method of protecting patient
data. The difficulty faced is determining the
removable feature with high sensitivity from the data.
While, in cases such as the coronavirus pandemic,
the use of sensitive patient data such as location may
improve governments' and research institutions'
ability to combat the threat more quickly by a
surveillance system that provides location data used
to curb the current crisis. The diabetes data, on the
other hand, has features that could give
discriminatory and stereotypical generalizations.
Data scientists must be mindful that utilizing these
large amounts of data comes at the expense of human
liberty and social autonomy. Lessening the risks of
using these data must be monitored by established
legislative measures, such as the General Data
Protection Regulation (GDPR). The Human-
Centered Design approach must be the intent and
goals of data usage, including its processing, analysis,
warehousing, and dataset sharing.
The following are the main conclusions observed
from these principles and criteria for operational use
of data-driven healthcare analytics:
7.1.1 Data Sensitivity Is Relative
The description and decision of feature sensitivity
vary from project to project, and it also depends on
the social value and regulations. For example, the
outcome from diabetes data analytics is
discriminatory and stereotypical. Can we say that
Caucasian white women weighing more than 200 kg
are more likely to be diabetic than other ethnic
groups?
7.1.2 Discrimination Is Just as Severe
Understanding the significance of data privacy and
security is crucial. Most data science ethics journals
are concerned with privacy and security and their
implications. Notwithstanding, there are
discriminatory and racist submissions arising from
big data analytics, which also have grave
consequences. Furthermore, to ensure a fair model,
we must measure analytics discriminatory tendencies
against respective advantages.
FEMIB 2022 - 4th International Conference on Finance, Economics, Management and IT Business
72

7.1.3 Human-Centered Design (HCD) Must
Be Ethically Compliant
Each phase in the Machine Learning and big data
analytics design process should consider the data
citizens impacted by models, methods, and
algorithms developed by data scientists. Biases in
defective datasets, algorithms, and human users are
numerous and discussed in depth. We must not ignore
that, owing to the vulnerability of data subjects and
groups, the risk of discrimination is more severe.
Furthermore, data scientists are also data citizens,
asides from developing big data insights, they are also
affected by such techniques. As a result, maintaining
ethically acceptable data processing and analytics is a
win-win scenario for all parties involved.
ACKNOWLEDGEMENT
This work is partly supported by VC Research
(VCR0000158) for Prof Chang.
REFERENCES
Agaku, I. T., Adisa, A.O., Ayo-Yusuf, O.A., and Connolly,
G.N. (2014) 'Concern about security and privacy, and
perceived control over collection and use of health
information are related to withholding of health
information from healthcare providers', journal of the
American Medical Informatics Association, 21(2), pp.
374–378.
Alzahrani, A. G. M., Alenezi, A., Mershed, A., Atlam, H.,
Mousa, F., and Wills, G. (2020) 'A framework for data
sharing between healthcare providers using
blockchain'.
Ball, K., Di Domenico, M. L. and Nunan, D. (2016) ‘Big
Data Surveillance and the Body-subject’, Body and
Society, 22(2), pp. 58–81. doi:
10.1177/1357034X15624973.
Borodin, A. V., Lebedev, N.F., Vasilyev, A., Zavyalova,
Y.V., and Korzun, D.G (2016) 'An experimental study
of personalized mobile assistance service in healthcare
emergency situations', Pdfs.Semanticscholar.Org, (c),
pp. 178–183. Available at:
https://pdfs.semanticscholar.org/64e7/c0da0b9f7fd403
831f6e1a8ade2688f216cc.pdf.
Cahan, E. M., Hernandez-Boussard, T., Thadaney-Israni, S.
and Rubin, D.L. (2019) ‘Putting the data before the
algorithm in big data addressing personalized
healthcare’, npj Digital Medicine, 2(1).
Camilleri, M. A. (2020) ‘The use of data-driven
technologies for customer-centric marketing’,
International Journal of Big Data Management, 1(1),
50-63.
Cave, A., Kurz, X., and Arlett, P. (2019) 'Real-World Data
for Regulatory Decision Making: Challenges and
Possible Solutions for Europe', Clinical pharmacology
and therapeutics', 106(1), 36–39.
https://doi.org/10.1002/cpt.1426
Chang, V., Shi, Y. and Zhang, Y. (2019) ‘The
Contemporary Ethical and Privacy Issues of Smart
Medical Fields’, International Journal of Strategic
Engineering, 2(2), pp. 35–43. doi:
10.4018/ijose.2019070104.
Cutillo, C. M., Sharma, K.R., Foschini, L., Kundu, S.,
Mackintosh, M. Mandl, K.D., Beck, T., Collier, E.,
Colvis, C., Gersing, K. Gordon, V., Jensen, R.,
Shabestari, B. (2020) ‘Machine intelligence in
healthcare—perspectives on trustworthiness,
explainability, usability, and transparency’, npj Digital
Medicine, 3(1), pp. 1–5.
Demirkan, H. (2013) ‘A Smart Healthcare Systems
Framework’ in IT Professional, vol. 15, no. 05, pp. 38 -
45, 2013. doi: 10.1109/MITP.2013.35. url:
https://doi.ieeecomputersociety.org/10.1109/MITP.20
13.35.
Dev Mishra, A. and Beer Singh, Y. (2017) ‘Big data
analytics for security and privacy challenges’,
Proceeding - IEEE International Conference on
Computing, Communication and Automation, ICCCA
2016, pp. 50–53. doi: 10.1109/CCAA.2016.7813688.
Dridi, A., Sassi, S.B., Chbeir, R., and Faïz, S. (2020) 'A
Flexible Semantic Integration Framework for Fully-
integrated EHR based on FHIR Standard' ICAART.
Durcevic, S. (2020) ‘18 Examples Of Big Data Analytics In
Healthcare That Can Save People’, Datapine’.
Available at: https://www.datapine.com/blog/big-data-
examples-in-healthcare/.
European Union Agency for Fundamental Rights (FRA)
(2018) ‘Big Data: Discrimination in data-supported
decision making’, FRA Focus, p. 14. Available at:
https://fra.europa.eu/sites/default/files/fra_uploads/fra-
2018-focus-big-data_en.pdf.
Favaretto, M., De Clercq, E. and Elger, B. S. (2019) ‘Big
Data and discrimination: perils, promises and solutions.
A systematic review’, Journal of Big Data, 6(1). doi:
10.1186/s40537-019-0177-4.
Floridi, L. (2012) ‘Big data and their epistemological
challenge’, Philosophy and Technology, 25(4), pp.
435–437. doi: 10.1007/s13347-012-0093-4.
Francis, J. G. (2014) ‘Introduction: Technology and New
Challenges for Privacy,” Journal of Social Philosophy
45(3): 291-303, University of Utah College of Law
Research Paper No. 107. Available at:
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2
564314.
Grandview Research Inc., (2021) ‘Healthcare Healthcare
Analytics Market Size, Share & Trends Analysis
Report,’ Available at https://www.grandview
research.com/industry-analysis/healthcare-analytics-
market, last accessed on 12/8/2021.
Healthcare Industry Insights (no date) ‘Healthcare
Analytics Market Is Estimated To Be Valued At $53’.
An Ethical Framework for Big Data and Smart Healthcare
73

Available at: https://sites.google.com/site/healthcare
industryinsights/healthcare-medical-analytics-market.
Hermon, R. and Williams, P. (2014) ‘Big data in healthcare:
What is it used for?’, Proceedings of the 3rd Australian
eHealth Informatics and Security Conference, pp. 40–
49. doi: 10.4225/75/57982b9431b48.
Heyman, D. L., and Rodier, G. (2004) 'Global Surveillance,
National Surveillance, and SARS. Emerging Infectious
Diseases.', PubMed, 10(2), pp. 173–175.
doi.org/10.3201/eid1002.031038
IBM (2019) ‘Cost of a data breach report’, IBM Security,
p. 76. Available at: https://www.ibm.com/
downloads/cas/ZBZLY7KL.
Ioannidis J. P. (2013). 'Informed consent, big data, and the
oxymoron of research that is not research', The
American journal of bioethics: AJOB, 13(4), 40–42.
Journal, H. (2019) ‘Healthcare Data Breach Statistics’,
Www.Hipaajournal.Com, pp. 1–13. Available at:
https://www.hipaajournal.com/healthcare-data-breach-
statistics/.
Kuempel, A. (2016) ‘The invisible middlemen: A critique
and call for reform of the data broker industry’,
Northwestern Journal of International Law and
Business, 36(1), pp. 207–234.
Luo, J. Wu, M., Gopukumar, D., & Zhao, Y. (2016) ‘Big
Data Application in Biomedical Research and Health
Care: A Literature Review’, Biomedical Informatics
Insights, 8, p. BII.S31559. doi: 10.4137/bii.s31559.
Mariani, D.M.R., Mohammed, S. and Mohammed, S.,
(2015) ‘Cybersecurity challenges and compliance
issues within the us healthcare sector’, International
Journal of Business and Social Research, 5(02).
Mittelstadt, B. (2019) ‘AI Ethics – Too principled to fail?’,
arXiv, pp. 1–15. doi: 10.2139/ssrn.3391293.
Nair, S. R. (2020). ‘A review on ethical concerns in big data
management’, International Journal of Big Data
Management, 1(1), 8-25.
NCI (National Cancer Institute) (2020) ‘HINTS 5 cycle 4
public codebook’, Hints. Available at:
https://hints.cancer.gov/data/download-data.aspx.
NIH (2021) ‘Health Information National Trends Survey
(HINTS)’, National Cancer Institute, p. Survey.
Available at: https://hints.cancer.gov/%0Ahttp://
hints.cancer.gov/docs/HINTS 2007 Annotated Mail
Instrument.pdf.
Obermeyer, Z., Powers B., Vogeli C., Mullainathan S.
(2019) ‘Dissecting racial bias in an algorithm used to
manage the health of populations’, Science, 366(6464),
pp. 447–453. doi: 10.1126/science.aax2342.
Patil, H. K. and Seshadri, R. (2014) ‘Big data security and
privacy issues in healthcare’, Proceedings - 2014 IEEE
International Congress on Big Data, Big Data Congress
2014, pp. 762–765. doi: 10.1109/BigData.Congress.
2014.112.
Paulus, J. K., Wessler, B. S., Lundquist, C. M., & Kent, D.
M. (2018) ‘Effects of Race Are Rarely Included in
Clinical Prediction Models for Cardiovascular
Disease’, Journal of General Internal Medicine, 33(9),
pp. 1429–1430. doi: 10.1007/s11606-018-4475-x.
Piai, S. and Claps, M. (2013) ‘Bigger data for better
healthcare’, IDC Health Insights, pp.1-24.
Raghupathi, V. and Raghupathi, W. (2020) ‘Healthcare
Expenditure and Economic Performance: Insights From
the United States Data’, Frontiers in Public Health,
8(May), pp. 1–15. doi: 10.3389/fpubh.2020.00156.
Raja, R., Ali, S., Mukherjee, I., Sarkar, B.K. (2020) ‘A
Systematic Review of Healthcare Big Data’, Scientific
Programming, 2020. doi: 10.1155/2020/5471849.
Razzak, MI, Imran, M. & Xu, G. (2020) 'Big data analytics
for preventive medicine', Neural Comput & Applic 32,
4417–4451. doi.org/10.1007/s00521-019-04095-y
Rehman, A., Naz, S. and Razzak, I. (2021) ‘Leveraging big
data analytics in healthcare enhancement: trends,
challenges and opportunities’, Multimedia Systems.
doi: 10.1007/s00530-020-00736-8.
Reinsch, R. W. and Goltz, S. (2016) ‘Big Data: Can the
Attempt To Be More Discriminating Be More
Discriminatory Instead?’, St. Louis University Law
Journal, 61(1), pp. 35–82.
Selby-Bigge, L. A. (ed.) (1975). ‘Enquiries Concerning
Human Understanding and Concerning the Principles
of Morals’. Oxford University Press.
Sonawane, V. P. and Irabashetti, P. (2015) ‘Method for
preventing direct and indirect discrimination in data
mining’, Proceedings - 1st International Conference on
Computing, Communication, Control and Automation,
ICCUBEA 2015, 25(7), pp. 353–357.
Suresh, H. and Guttag, J. V. (2019) ‘A framework for
understanding unintended consequences of machine
learning’, arXiv preprint arXiv:1901.10002, 2.
Ward, J. S. and Barker, A. (2013) ‘Undefined By Data: A
Survey of Big Data Definitions’. Available at:
http://arxiv.org/abs/1309.5821.
Winter, J. S. (2018) ‘Introduction to the Special Issue:
Digital Inequalities and Discrimination in the Big Data
Era’, Journal of Information Policy, 8, 1–4.
https://doi.org/10.5325/jinfopoli.8.2018.0001.
Wong, Z. S. Y., Zhou, J. and Zhang, Q. (2019) ‘Artificial
Intelligence for infectious disease Big Data Analytics’,
Infection, Disease and Health, 24(1), pp. 44–48. doi:
10.1016/j.idh.2018.10.002.
Zhu, H, Wu, C.K., Koo, C.H., Tsang, Y.T., Liu, Y., Chi,
H.R. and Tsang, K-F. (2019), 'Smart Healthcare in the
Era of Internet-of-Things', IEEE Consumer Electronics
Magazine, vol. 8, no. 5, 8822574, pp. 26-30.
https://doi.org/10.1109/MCE.2019.2923929
Žliobaitė, I. (2017) ‘Measuring discrimination in
algorithmic decision making’, Data Mining and
Knowledge Discovery, 31(4), pp. 1060–1089.
FEMIB 2022 - 4th International Conference on Finance, Economics, Management and IT Business
74
