
A Controlled Virtual Reality Exposure Therapy Application for
Smartphones
∗
Joana Teixeira, Bruno Patr
˜
ao and Paulo Menezes
University of Coimbra, Department of Electrical and Computer Engineering, Institute of Systems and Robotics,
Rua S
´
ılvio Lima, Coimbra, Portugal
Keywords:
Virtual Reality, Exposure Therapies, Serious Games, Smartphone VR.
Abstract:
Exposure therapy (ET) is often used as a therapeutic process for the treatment of a psychological disorder.
Usually, this type of therapy is challenging to apply traditionally as the therapist must expose the patient
safely to the cause of the disorder. To help surpass this problem, a virtual reality (VR) application was de-
veloped to support exposure therapy. As these therapies are based on a gradual and repetitive process, with
this application, the patient can be exposed to the phobic element at different levels of anxiety intensity as
prescribed by the therapist. This application was designed to be used either during the therapeutic sessions or
at home. While using it in therapeutic sessions, it allows the therapist to include the analysis of physiological
signals, escape movements, or other reactions during the exposure. At home, as homework for the therapy
sessions, it will allow the patient to keep training what was learned during therapy. It is being developed as a
serious game for smartphones, and users will only need a cardboard-like VR headset.
1 INTRODUCTION
The evolution of VR-based technologies is allowing
the application of new medical procedures that oth-
erwise were complicated or completely impossible.
Mental health is one of the areas where this technol-
ogy is being applied and where this work is focusing
on. Every year, anxiety disorders affect nearly 18.1%
of adults and are still registered as one of the most
commons mental disorders (Saloni Dattani and Roser,
2021). Anxiety can become a daily obstacle for those
who suffer from it, as it introduces significant dis-
tress, with consequent impairment in the quality of
life. This is also a problem for the society since, as un-
treated mental health disorders become more severe,
social and economic costs tend to increase (Botella
et al., 2011).
Numerous authors have shown that VR experi-
ences can be compared to real ones as VR scenarios
can induce some sensations similar to the ones felt in
the physical world (Penn and Hout, 2018). VR is be-
ing increasingly used in behavioural therapies, in par-
ticular in exposure therapies that consist in exposing
the patient to anxiety triggers, so that learning, habit-
uation, desensitization, or other, will help overcome
∗
This work was supported by Fundac¸
˜
ao para a Ci
ˆ
encia e
a Tecnologia (FCT) through project UID/EEA/00048/2020
or, at least, help in the process of managing it in the
daily life. Long term studies show the effectiveness
of VR to ET in the treatment of phobias (Krzystanek
et al., 2021).
Exposure therapy has proved its efficacy in the last
20 years (Botella et al., 2011; Anderson and Mol-
loy, 2020). Nevertheless, the traditional application
of this treatment does not please everyone. Some pa-
tients fear the in-real-life confrontation with phobic
elements and some therapists also tend to believe that
in real-life exposure can be unethical by provoking
uncontrollable fear to their patients and, depending
on the disorder, by not being able to maintain the ses-
sions private and violating the patient-client bound-
aries (Miloff et al., 2019). Therapists also avoid in-
vivo exposure due to the time-consuming sessions and
the work around it, for instance, catching and keep-
ing a spider in the clinic for later reuse (Hinze et al.,
2021). When compared to traditional exposure ther-
apies, virtual reality counterparts tend to be accepted
by both parties, and seen as more ethical, and help-
ful (Botella et al., 2011). They are also considered
safer, and in most cases, as effective as in-vivo expo-
sures (Anderson and Molloy, 2020). Another advan-
tage of a VRET is the fact that it can be conducted in
an medical office, even if the elements to be explored
cannot be physically there (Miloff et al., 2019).
294
Teixeira, J., Patrão, B. and Menezes, P.
A Controlled Virtual Reality Exposure Therapy Application for Smartphones.
DOI: 10.5220/0010990300003124
In Proceedings of the 17th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP 2022) - Volume 1: GRAPP, pages
294-301
ISBN: 978-989-758-555-5; ISSN: 2184-4321
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

One notable disadvantage of VR systems is their
high prices. The development of this technology in
the past four years, has led to a cost reduction and
increased quality, and that makes this issue continu-
ally less significant. With the recent release of new
and more inexpensive virtual reality headsets, clinical
trials are more common and find high levels of user
satisfaction with VR (Anderson and Molloy, 2020).
Although cybersickness is still one of the major ob-
stacles, considerable improvements in the devices’
quality make this issue increasingly less significant.
Also in this respect, the careful design of applica-
tions (Patr
˜
ao et al., 2015), and the fact that most ex-
posure scenarios do not need fast displacements in the
VR space, may contribute to reduce the percentage of
users experiencing this type of discomfort.
It is commonly accepted that VR and ET are use-
ful with anxiety disorders, especially for disorders
such as zoophobia, aerophobia, acrophobia, among
others. However, psychologists who are specialized
in other disorders like eating disorders, ADHD and
OCD also believe VRET can be an alternative treat-
ment with success (Lindner et al., 2019). In the
case of OCD, VR is capable of provoking symptoms
such as anxiety in patients and compare the results to
healthy control. So, with the help of VR, therapists
can recognize OCD symptoms and diagnose this dis-
turb easier (Van Bennekom et al., 2021). Nowadays,
the main question is no longer if VRET is indeed as
effective as in-vivo ET, but how to engage the patient
to keep working on himself and not giving up for lack
of interest.
Since the concept of computer games has been
emerging as a powerful new economic, cultural, and
educational force (Botella et al., 2011), serious games
are also becoming more popular among people of all
ages.
Serious games, unlike traditional computer
games, are alternative educational, training, or ther-
apeutic tools that go beyond mere entertainment
(Lievense et al., 2021) and are an effective medium
for creating a non-threatening and engaging learn-
ing environment (Fitzgerald and Ratcliffe, 2020). It
has been proven that serious games can change be-
haviour (Botella et al., 2011) and reduce disorder-
related symptoms (Lau et al., 2017). It actively en-
gages the player and promotes change within a safe
virtual environment (Lievense et al., 2021), eliminat-
ing both the privacy issue and the out-of-control el-
ements that worried the therapists. Since it has an
entertaining form, the ethical conflict of provoking
fear in the patients is also toned down and is more
acceptable between professionals. This type of game
places its goal outside the game itself. According to
the self-determination theory, there are two types of
motivation that may influence the retention of a per-
son in one activity - extrinsic motivation and intrinsic
motivation (Lievense et al., 2021). From a gaming
perspective, extrinsic motivation leads to material re-
wards, or cheering messages for other players. For in-
stance, when the player receives fictional coins to pur-
chase bonuses or elements in the game. On the other
side, intrinsic motivation is based on personal interest,
the final reward is related to each individual (Fischer
et al., 2019). Serious games thrive on intrinsic mo-
tivation since the player must have personal goals to
succeed in the game. The different levels of the seri-
ous games are achieved with the acquisition of skills
or therapeutic progress (Botella et al., 2011). If the
players have a clear purpose and the goals and levels
of the game are clearly defined, then the game is well
accepted, and the engagement is enhanced (Fitzgerald
and Ratcliffe, 2020). The use of serious games and
gamification principles to promote treatment for men-
tal illness had high levels of feasibility and acceptabil-
ity among both users and providers (Fitzgerald and
Ratcliffe, 2020). The current problem is no longer the
effectiveness of VR and the application of exposure
therapy, but the user experience itself that can lead to
more positive or negative results (Tao et al., 2021).
The application of VR can follow quite different
approaches. Some aim to develop an application for
smartphones to be used at home without the presence
and/or without the consultation of a therapist. These
applications can sometimes be a serious game or a se-
lection of VR scenarios that the user needs to explore.
In this case, the progress achieved is measured by the
user or by the application itself. However, this can
make the situation worse by exposing the user to lev-
els of disturbing elements that he/she is not prepared
to face, thus incubating the fear even more.
The problem we perceived with the current home-
use application, is that it does not engage the user
to come home after a day of work to use it. This is
a big problem with exposure therapy, as it requires
constant exposure to the anxiety source to eventually
overcome the problem. Other commonly used ap-
proaches consist of the application of VR in-clinic
sessions with the constant presence of the therapist
that walks through all the stages with the patient, and
maintaining full control of the exposure level through
out the session.
1.1 Contributions of the Paper
This work presents the development of a immersive
application to promote learning and coping with anx-
iety, tuned for a specific clinical case. The ultimate
A Controlled Virtual Reality Exposure Therapy Application for Smartphones
295

goal is to facilitate the therapist work and help the
patient to reach a level of well-being by overcoming
constraining anxiety and/or phobias.
To this end, a serious game is proposed that allows
the user to have fun while learning how to manage his
anxiety in the presence of whatever triggers it. The
player levels up in the game as the therapeutic goals
are met and according to the therapist. This serious
game will aim at not only anxiety disorders but also
other disorders such as OCD and ADHD, making it
possible for the therapist to personalize it to the pa-
tient needs.
2 DESIGNING A FRIENDLY
SPACE FOR ET
The concept explored is the development of a serious
game to facilitate the application of ET for both the
patient and the therapist. The patient can comfortably
use the application at home by only needing a smart-
phone, and a VR headset for smartphones, such as
Google Cardboard.
The design of the VR environment can integrate
ET with different types of disorders elements. VR is
commonly associated with anxiety disorders. How-
ever, psychologists believe that VR can also help
other non-anxiety related disorders, and this serious
game aims to meet those expectations.
Due to its high popularity among all ages and
its versatility, the game ”Escape Room” is one ex-
ample of how this serious game can present itself.
The player needs to complete several tasks and gather
clues to escape the current room. By changing rou-
tines and adding new clues, the patient will be con-
stantly entertained and stimulated to maintain engage-
ment. It allows to prevent disinterest and conse-
quently keep the patient exposed, as if the patient
loses interest, the therapeutic progress will decrease.
However, as the concept of this game may, on itself,
trigger some disorders like claustrophobia, it can be
changed to other possible less anxiety-prone games
such as treasure hunting.
The escape-room scenario creates the perfect con-
text to contain multiple and different mini-games.
The disturbing elements are to be included in those,
allowing the patient to take a break between expo-
sures without leaving the VR environment and con-
sequently not losing any sense of presence. In the
case of arachnophobia, the anxiety disorder that will
serve as an example throughout the article has a pho-
bic element, the spider, so there are mini-games that
only show images of it, and others present themselves
with a virtual representation of the animal. Each mini-
game addresses a different anxiety level and has small
therapeutic goals. Since the patient must have a grad-
ual exposure to the phobic elements, with the mini-
games the patient can be exposed slowly from images
to videos to the actual virtual presence.
3 DESIGN AND
IMPLEMENTATION OF A
VIRTUAL COMFY SPACE FOR
ET
The mobile application developed has to address
some complex issue in terms of displacement and in-
teraction within the game. As for the home usage, the
patient will use it in a cardboard configuration, there-
fore no joysticks, gamepads, or other game controllers
should be considered. By consequence the only pos-
sibility is to use the head orientation itself to support
the interaction with the VR environment in its various
aspects, as will be discussed bellow.
This limited interaction form presented some chal-
lenges in the game’s development, such as playing
only moving the head and avoiding any fast move-
ments to prevent motion sickness. As reported by
(Anderson and Molloy, 2020), people who suffer
from mental health illnesses tend to be more prone
to cyber-sickness, so this was a subject that received
particular attention.
3.1 Interact with the VR Environment
To interact with the VR environment the patient can
search for specific points that will light up to let him
know that there is the possibility to interact with and
a small pointing sphere will change colour to the in-
verted colour of the object that it collides with. The
sphere simultaneously represents the point where the
player is looking at in the game, and is the interaction
element. In fact, its collision with the active elements
of the virtual world is exploited to enable the player to
select objects, move within the game space, or interact
with the mini-games. Whenever the sphere is placed
on top of an active element it immediately starts in-
flating showing the interactive control, and activating
the element after a while.
Some places are important to the game flow, such
as where a code can be inserted, or where the mini
games are playable. Because of this characteristic,
small blue moving circles are placed in those specific
locals to grab the attention of the player that it is im-
portant to move at some point to that location as can
be seen in Fig 1.
GRAPP 2022 - 17th International Conference on Computer Graphics Theory and Applications
296

Since interaction is limited, and motion sickness
is an issue, so travelling to different places in the
room consists of a fade-in, turning the screen slowly
black, and a fade-out in the correct position, turning
the screen slowly back to the initial state, maintain-
ing the rotation and the height the player was in. The
player can only move in the ground plane.
Figure 1: Teleport circle.
3.2 The Interaction with the
Mini-games
The serious game is sequential with an exposure lad-
der where some have a lower anxiety level and others
are more intense. In the higher difficulty, all imple-
mented anxiety sources are present. The game itself
also has some variations between plays, such as dif-
ferent images and random placement of the matches
in the case of a memory matching game card.
Since sometimes the patient can have more diffi-
culties in an exposure given by a specific mini-game,
the therapist can request the patient to play only that
mini-game without the need to play the full serious
game, and for that there is the possibility playing in-
dividual mini-games.
The interaction between each mini-game also
needed to be analysed to create a random yet sequen-
tial relation between them. Upon completing each
one, a digital code is provided to the player and acts
as a bridge between the mini-games. The codes are
presented differently, forming a final colour code to
unlock the last door and finish the escape room (Fig
2). The mini games also present hints once finished
like where the code is or to where it is to be inserted.
For instance, as can be seen in Fig 4, once the drawer
is opened a line of sparkle particles flow to the correct
keypad. If the code inserted is correct it will change
color to green, if not it changes color to red (Fig 3).
Figure 2: Color Code Keypad and Codes found.
The static mini-games such as memory card
matching and puzzles are played in a similar man-
ner. Spark particles appear where the player is staring
at and like moving, the interactive sphere increases
and when full the game develops. In the case of the
”find the differences game”, the spark particles do not
show and the sphere does not increase unless it is to
press the hint button. However it is still necessary to
wait two seconds looking ate the same spot to play.
This happens to avoid giving the difference location
away. On more dynamic mini-games, like the maze,
the phobic element follows the interactive sphere and
the game is played by controlling its location.
A Controlled Virtual Reality Exposure Therapy Application for Smartphones
297
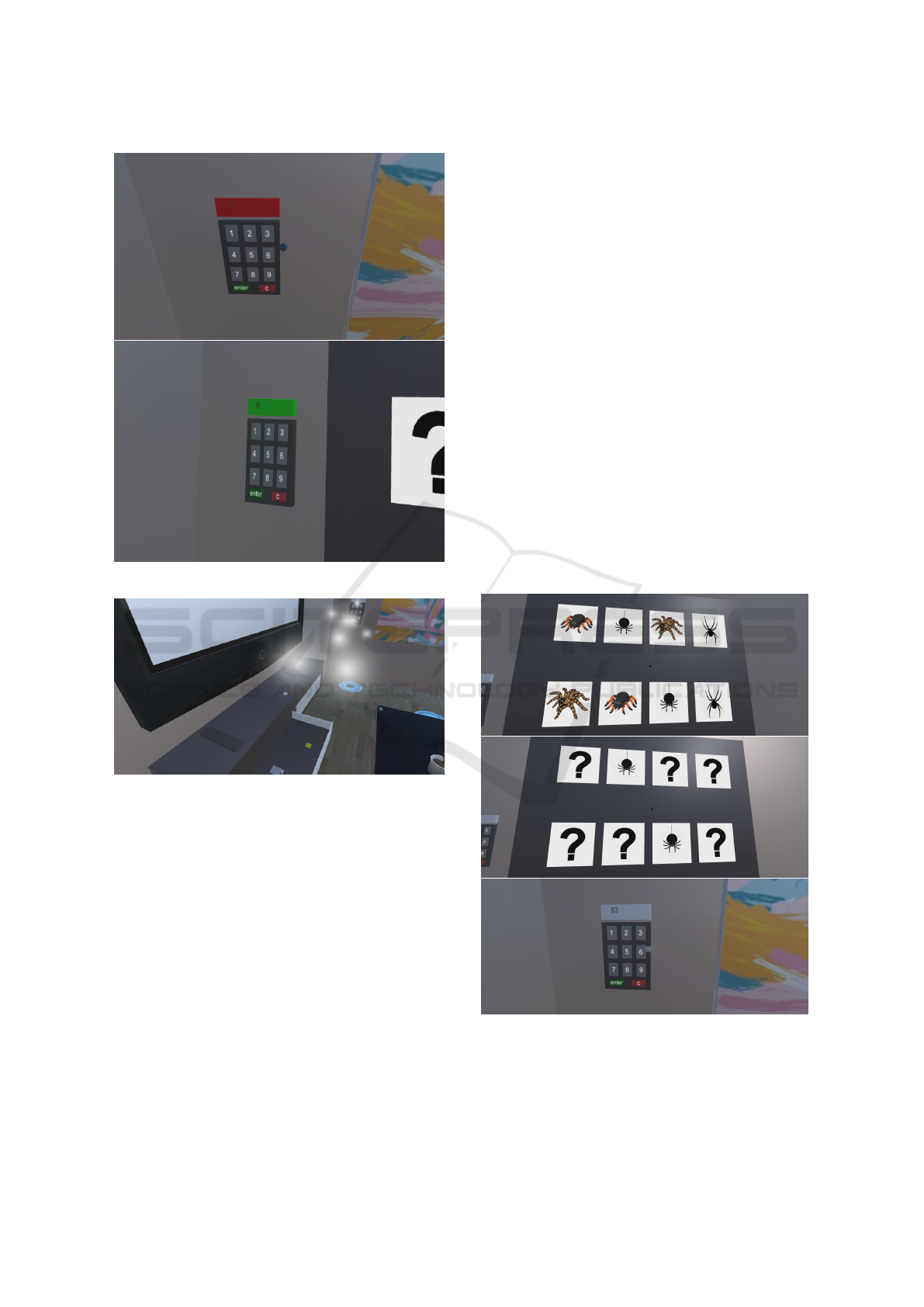
Figure 3: Correct and wrong color code inserted.
Figure 4: Hint after opening drawer.
4 BREAKING DOWN THE
EXPOSURE INTO MINI-GAMES
The mini-games serve to expose the patient to the dis-
order element. The time between each mini-game act
as a pause of exposure or even as a panic emergency
escape. The patient can leave the mini-game, take a
break wondering the virtual room and resume it when
calmer, preventing the break of the sense of presence.
The serious game starts with all the mini-games
hidden. When the patient inserts the codes onto the
keypad, the corresponding mini-game uncover itself.
Each one executes isolated, being coordinated by the
main script. This format enables the therapist to re-
quire the patient to play only one of the mini games
without it being necessary to play the escape room.
The chosen mini-games to develop in the concept
of ”Escape Room” and arachnophobia are:
• Memory Card Matching
• Find the Differences
• Slide Puzzle
• Rotating Puzzle
• Maze
In the ”Memory Card Matching” mini-game (Fig.
5), the user has constant contact with different im-
ages of its anxiety source. When playing, if the cards
turned do not make a pair, they turn themselves back.
As the game proceeds, the number of images exposed
increases, and the anxiety may make it harder to com-
plete. The mini-game leads to the necessity to memo-
rise a determined image’s position and details to cor-
respond with its duplicate. This mini-game also al-
lows the player to decide if he wants to see the inan-
imate disorder related element. In order to keep the
challenge level constant between game session, each
image position is randomized at the beginning of the
game. After completing all the matches, a code ap-
pears in the room. This code will lead to the next
mini-game.
Figure 5: Memory Matching Card Game.
The ”Find the Differences” mini-game (Fig. 6)
consists of two very similar images with slight differ-
ences between them which the user has to find and
mark.
GRAPP 2022 - 17th International Conference on Computer Graphics Theory and Applications
298

The game starts hidden behind a closet. After
acquiring the code from the memory matching card
game, the player can insert it onto the keypad, and the
mini-game appears. To play, the user selects a posi-
tion on either the images. After waiting two seconds,
if it corresponds to a difference, a red doughnut will
target the spot as found. If not, then nothing happens.
If needed, a hint feature will help the player com-
plete the mini-game. The hint consists of the pho-
bic element moving towards the difference’s position.
Depending on the level of exposure, this element can
be the phobic element. In the case of arachnophobia, a
spider shows the patient where one of the differences
is. All the animated phobic elements show a neutral
white sphere if the patient is playing the lowest inten-
sity.
Figure 6: Find the Differences Game.
The maze (Fig. 7), according to the selected dis-
turb, may have different aspects. For instance, to
OCD, the lines are not straight, and some lights turn
on and off while passing on a specific part of the
path. For ADHD, distractions such as random blink-
ing lights or sounds can easily make it harder for the
patient to concentrate on the task. If it is arachnopho-
bia or other small animal-related phobias, the phobic
element follows the position of the user’s head, and
the goal is to lead the animal to the end of the maze
without it touching the walls. The maze path shuf-
fles between predefined paths. Along the maze there
are several platforms. The phobic element must touch
every platform or the final color is not provided.
The last two mini-games are two different kinds of
puzzles: a rotating puzzle and a slide puzzle, but the
therapeutic goal is similar, making the patient gradu-
ally assemble the image related to the anxiety source.
Nine pieces of the same image constitute the rotating
puzzle, and the player needs to rotate each one, 90 de-
grees at a time, to build the final image and complete
the mini-game. The slide puzzle consists of 8 pieces
of the same image and a blank spot of the same size
as the other parts of the image. The player must move
the pieces within the available space until the final im-
age appears.
Figure 7: Maze Game.
5 THE THERAPIST ROLE ON A
CONNECTED APP
The presence of a therapist in this process is of high
importance. It does not need to be a constant pres-
ence, but one-off checkups. The progress made by
the patient needs to be analysed, and with those con-
clusions, the therapist decides which level of anxiety
intensity the patient plays at home. The therapist has
access to the patient progress by a data base. When
the patient logs in, a code provided by the therapist
is inserted and that data is saved and can be accessed
later by the therapist.
Figure 8: Login and game options.
A Controlled Virtual Reality Exposure Therapy Application for Smartphones
299
The patient must play at least once every session
for the therapist to evaluate the progress. The physio-
logical signals such as the heart rate and galvanic skin
response will also target that evaluation.
During the development of the presented work,
meetings with psychologists clarified the patients
point of view and how to help and not overexpose
them to the anxiety source. The therapist must be
able to evaluate the situation step by step so the ex-
posure remains controlled. So, to facilitate and help
keep track of the patient progress, he has access to
the scores of each mini-game and the total time of
play of each patient. It is then possible to know how
many times throughout the time-off sessions the pa-
tient played and the difficulty they faced.
6 PRELIMINAR VALIDATION
6.1 Game / Usability Analysis
The game was tested by 10 individuals. At the end
of each test, the individuals filled a User Experi-
ence Questionnaire (UEQ), a Flow Short Scale Ques-
tionnaire and an open answer questionnaire to obtain
some information about the individuals.
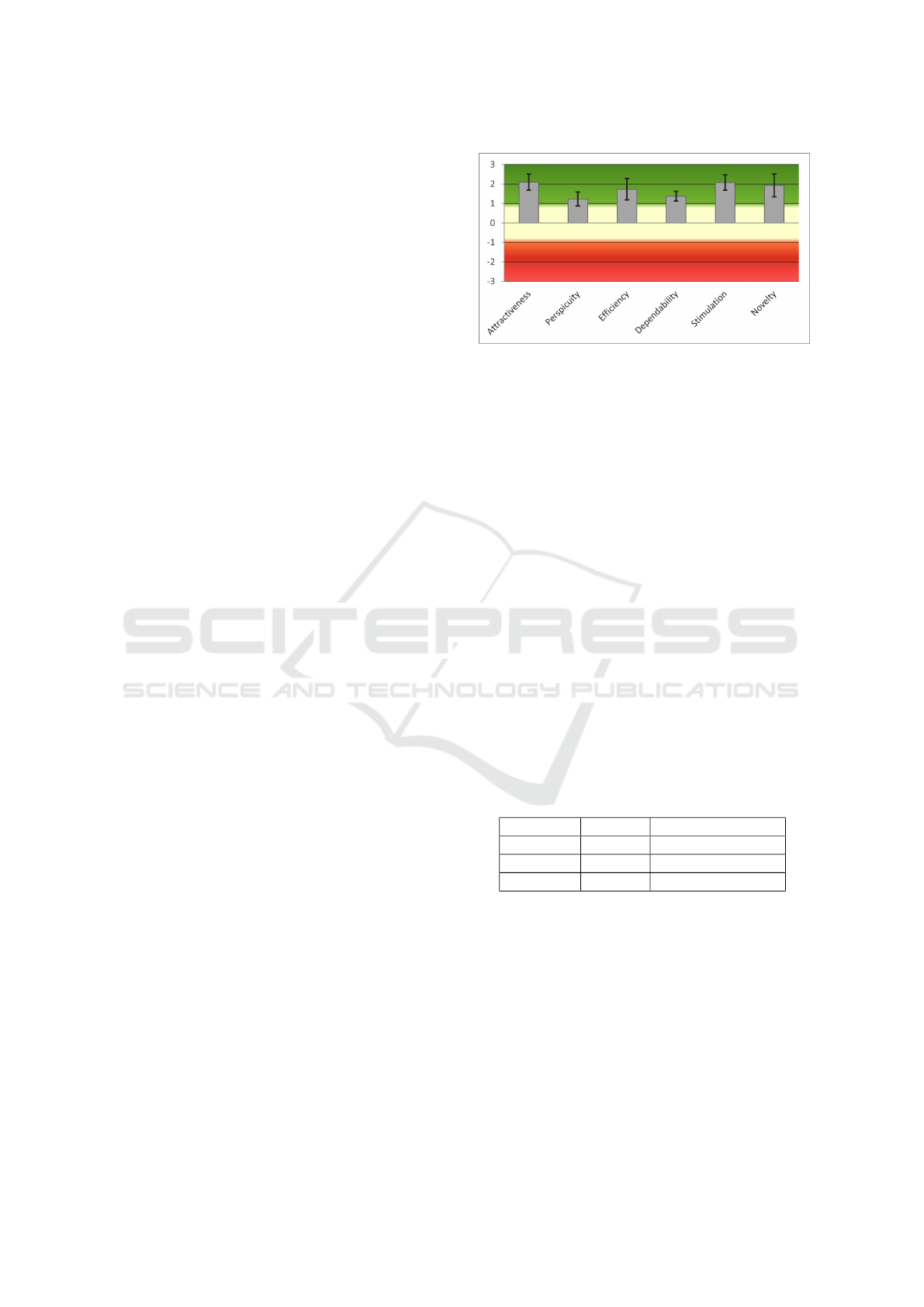
The UEQ is frequently used to measure the user
experience with a certain product. It evaluates the
user experience in six different categories: attractive-
ness, perspicuity, efficiency, dependability, stimula-
tion and novelty. If a category is above 0.8 it has a
positive evaluation and above 1.5 is considered and
excellent result. The results are presented in figure
9. It presents the average classification of each cat-
egory and its standard deviation. The attractiveness,
efficiency, stimulation and novelty categories were all
classified as excellent, although with a high standard
deviation due to the sample size. The perspicuity and
dependability had slightly lower scores with 1.225
and 1.375 respectively.
Perspicuity refers to how easy it is to get famil-
iar with the application and how easy it is to use it.
The application is a virtual reality serious game and
in the open answer questionnaire most of the individ-
uals lack of experience with VR so, being an VR ”Es-
cape Room” game it was expected some difficulties
in interacting with the environment at first try. De-
pendability refers to how in control of the interaction
the user feels. The serious game is a compilation of
puzzles and codes, so the fact that some individuals
felt they did not had control of the situation is not far
from the reality.
The Flow Short Scale Questionnaire evaluates
three aspects of the application on a scale of 1 to 7:
Figure 9: UEQ Questionnaire Results.
flow, anxiety level and challenge level. Flow level in-
dicates if the user is feeling engaged while playing the
game and if he feels like the activity is intrinsically in-
teresting and takes pleasure and enjoyment while in-
volved with it. Anxiety level translates to how much
anxiety the users felt while playing the game and chal-
lenge level to how challenging it was with 1 being too
easy and 7 too hard.
The results with the average and standard devia-
tion of each category are presented in table 1. The
challenge level was considered to be close to perfect
(with 4 being a perfectly adequate challenge level).
The anxiety level was not high but it presented a rel-
atively high standard deviation. In the open answer
questionnaire three individuals said to have anxiety
problems such as anticipation anxiety. This may ex-
plain why such high standard deviation. A flow level
of 5.04 indicates the users mostly enjoyed playing the
game but some aspects could be improved such as
adding descriptions of how the mini games are played
and maybe a scene without any game to allow the user
to get to know the VR environment.
Table 1: Flow Short Scale Questionnaire Results.
Average Stardard Deviation
Flow 5.04 0.527
Anxiety 3.867 1.124
Challenge 3.9 0.568
7 CONCLUSION
Exposure therapy is one of the best behavioural ther-
apy techniques as it allows the user to explore the dis-
order in a safe and controlled way. This paper we pre-
sented a serious game for that purpose, that explores
VR to expand the range of disorders that the treatment
can reach and allow the patients to train at home and
expose themselves to the anxiety source according to
their therapist recommendations.
GRAPP 2022 - 17th International Conference on Computer Graphics Theory and Applications
300

This type of application can be the starting point
for many people to learn how to manage their anxi-
ety and live life in a much better state of mind. As
the chosen game design can be so multifaceted, the
opportunities are endless. Not only can different dis-
orders like arachnophobia, PTS, OCD and ADHD be
improved, but the therapist can adequate the game to
each patient depending on the presented disorders and
the best anxiety intensity levels for each one.
REFERENCES
Anderson, P. L. and Molloy, A. (2020). Maximizing the
impact of virtual reality exposure therapy for anxiety
disorders. Current Opinion in Psychology, 36:153–
157. Cyberpsychology.
Botella, C., Breton-L
´
opez, J., Quero, S., Ba
˜
nos, R., Garc
´
ıa-
Palacios, A., Zaragoza, I., and Alcaniz, M. (2011).
Treating cockroach phobia using a serious game on
a mobile phone and augmented reality exposure: A
single case study. Computers in Human Behavior,
27(1):217–227. Current Research Topics in Cognitive
Load Theory.
Fischer, C., Malycha, C. P., and Schafmann, E. (2019). The
influence of intrinsic motivation and synergistic ex-
trinsic motivators on creativity and innovation. Fron-
tiers in Psychology, 10:137.
Fitzgerald, M. and Ratcliffe, G. (2020). Serious games,
gamification, and serious mental illness: A scoping
review. Psychiatric Services, 71(2):170–183. PMID:
31640521.
Hinze, J., R
¨
oder, A., Menzie, N., M
¨
uller, U., Domschke, K.,
Riemenschneider, M., and Noll-Hussong, M. (2021).
Spider phobia: Neural networks informing diagnosis
and (virtual/augmented reality-based) cognitive be-
havioral psychotherapy—a narrative review. Frontiers
in Psychiatry, 12:1435.
Krzystanek, M., Surma, S., Stokrocka, M., Roma
´
nczyk,
M., Przybyło, J., Krzystanek, N., and Borkowski, M.
(2021). Tips for effective implementation of virtual
reality exposure therapy in phobias—a systematic re-
view. Frontiers in Psychiatry, 12:1553.
Lau, H. M., Smit, J. H., Fleming, T. M., and Riper, H.
(2017). Serious games for mental health: Are they ac-
cessible, feasible, and effective? a systematic review
and meta-analysis. Frontiers in Psychiatry, 7:209.
Lievense, P., Vacaru, V. S., Kruithof, Y., Bronzewijker, N.,
Doeve, M., and Sterkenburg, P. S. (2021). Effective-
ness of a serious game on the self-concept of children
with visual impairments: A randomized controlled
trial. Disability and Health Journal, 14(2):101017.
Lindner, P., Miloff, A., Zetterlund, E., Reuterski
¨
old, L.,
Andersson, G., and Carlbring, P. (2019). Attitudes
toward and familiarity with virtual reality therapy
among practicing cognitive behavior therapists: A
cross-sectional survey study in the era of consumer vr
platforms. Frontiers in Psychology, 10:176.
Miloff, A., Lindner, P., Dafg
˚
ard, P., Deak, S., Garke, M.,
Hamilton, W., Heinsoo, J., Kristoffersson, G., Rafi, J.,
Sindemark, K., Sj
¨
olund, J., Zenger, M., Reuterski
¨
old,
L., Andersson, G., and Carlbring, P. (2019). Auto-
mated virtual reality exposure therapy for spider pho-
bia vs. in-vivo one-session treatment: A randomized
non-inferiority trial. Behaviour Research and Ther-
apy, 118:130–140.
Patr
˜
ao, B., Pedro, S. N., and Menezes, P. (2015). How to
deal with virtual reality sickness. In EPCGI’2015:
The 22nd Portuguese Conf. on Computer Graphics
and Interaction, Coimbra, Portugal.
Penn, R. A. and Hout, M. C. (2018). Making reality vir-
tual: How vr “tricks” your brain. Frontiers for Young
Minds, 6.
Saloni Dattani, H. R. and Roser, M. (2021).
Mental health. Our World in Data.
https://ourworldindata.org/mental-health.
Tao, G., Garrett, B., and Taverner, T. (2021). Immersive vir-
tual reality health games: a narrative review of game
design. Presence Teleoperators amp Virtual Environ-
ments.
Van Bennekom, M. J., de Koning, P. P., Gevonden, M. J.,
Kasanmoentalib, M. S., and Denys, D. (2021). A vir-
tual reality game to assess ocd symptoms. Frontiers
in Psychiatry, 11:1640.
A Controlled Virtual Reality Exposure Therapy Application for Smartphones
301
