
Evaluation and Usage Analysis of IBD Tool: A Telemonitoring
Platform for Inflammatory Bowel Disease
Caterina Lia
1a
, Matteo Bonina
1b
, Marco Daperno
2c
, Valeria Figini
3d
,
Flavio Martinez De Carnero
1e
and Guido Pagana
1f
1
Politecnico di Torino, Turin, Italy
2
Department of Gastroenterology of Mauriziano Hospital, Turin, Italy
3
LINKS Foundation, Turin, Italy
Keywords: Telemedicine, e-Health, Telemonitoring, Inflammatory Bowel Disease, Questionnaires.
Abstract: Telemedicine brings numerous benefits to healthcare as a support to traditional medicine. On this basis, IBD
Tool was developed. It consists of a web-app through which some of the patients suffering from Inflammatory
Bowel Disease (IBD) of the Mauriziano Hospital of Turin are followed. Thanks to IBD Tool, physicians can
follow the evolution of the disease over time, having the ability to identify periods of remission and relapse
and to reduce hospitalization’s frequency of patients. Furthermore, IBD Tool is a powerful tool also for
patients, who thanks to the web-app are always in close contact with the healthcare staff and do not feel
neglected in the months that normally elapse between a visit and the other. In this first year of use of the
platform, telemedicine has proved to be a valid support for the treatment of chronic intestinal diseases,
providing clinicians a versatile telemonitoring tool. Considering the current health situation, it is increasingly
evident that the health system cannot ignore telemedicine. In this study, we have investigated the results
collected in this first period of use of the platform, monitoring the activity state of the web-app and patients’
evaluations about the tool.
1 INTRODUCTION
The current coronavirus pandemic of 2019 has caused
a significant strain on medical center resources. Thus,
the COVID-19 pandemic has radically and rapidly
changed the way physicians deliver patient care. In
early 2020 there has been a rapid adoption of digital
tools and technologies such as telemedicine and
virtual assistance which refer to the provision of
digital or remote healthcare services using
information and communication technologies for the
treatment of patients (
Bokolo, 2020
).
In this scenario IBD Tool web-app was developed
and tested. The goal is to provide timely care while
minimizing the need for patients to travel to the
hospital. This study provides information on the
a
https://orcid.org/0000-0002-6709-6866
b
https://orcid.org/0000-0001-6366-9447
c
https://orcid.org/0000-0002-0217-6603
d
https://orcid.org/0000-0003-3944-1471
e
https://orcid.org/0000-0002-8809-6312
f
https://orcid.org/0000-0003-0272-3395
possible implications and potential of using virtual
assistance solutions.
IBD Tool consists of a web-app through which
some patients of the Mauriziano Hospital of Turin
suffering from Inflammatory Bowel Diseases (IBD)
are monitored. The IBDs are pathologies that
accompany patients throughout their life. Therefore,
for these patients a periodic check-up is essential to
avoid degenerations of pathology. However, the IBDs
can remain silent even for long periods of time.
Telemedicine in this field has the role of ensuring that
the patient goes to hospital only if strictly necessary.
This web-app administers specific questionnaires to
patients, focusing on the disease but also on habits
and quality of life. In this way IBD Tool monitors the
overall health of patients and provides them with an
186
Lia, C., Bonina, M., Daperno, M., Figini, V., Martinez De Carnero, F. and Pagana, G.
Evaluation and Usage Analysis of IBD Tool: A Telemonitoring Platform for Inflammatory Bowel Disease.
DOI: 10.5220/0010986600003188
In Proceedings of the 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2022), pages 186-195
ISBN: 978-989-758-566-1; ISSN: 2184-4984
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

integrated communication tool that puts them in
contact with the physicians of the Mauriziano
Hospital in Turin.
This project arises from a scientific
experimentation which is evaluating over time the
effects of telemedicine usage on patients.
IBD Tool collects questionnaires filled out by
patients since March 2020 and has evolved over time
following user requests. The platform includes
several sections: the section for receiving, sending,
and reading questionnaires for both physicians and
patients, a section with clinical data, a dedicated chat
and a dashboard to view the progress of patients
considering several parameters (which we will see
later in this paper).
IBD Tool was developed with the aim of making
the application easy to use for both clinicians and
patients.
Physicians recruited volunteer during the first
follow-up visit after the start of the platform testing
phase. The patients who joined the trial signed an
informed agreement, and they were then registered by
the physicians on the web-app. Among the patients
who joined the trial, not all had the same type of
access to the platform. The 50% were randomly
referred to telemedicine care and the remaining 50%
to standard care. It is a compromise between ethical
aspects (to not deprive the patient of a potentially
useful tool especially in the pandemic period) and the
need to have a control sample. The difference
between patients in telemedicine and those in
standard care is the administration frequency of
questionnaires, which are more frequent in the first
group.
In a year and a half of use, physicians have always
been able to give direct feedback to improve the web-
app. In this study, we investigate patient feedback to
assess whether the objectives of simplicity of use
have been achieved and possibly accept proposals for
changes to improve it. Main focus is the use of the
web-app among patients-users, their involvement,
and their activity rate with respect to the application.
2 METHODS
2.1 Questionnaires
The monitoring function of IBD Tool is based on
questionnaires. IBD Tool automatically administers
specific questionnaires to patients based on their
category. Presence of a new questionnaire is notified
by mail and by the platform through the notification
section. When a user-patient is registered on the
platform by the clinician, he is automatically and
randomly assigned to a specific treatment category,
STANDARD or TELEMEDICINE, which identifies
two different levels of remote assistance.
The differences between the two categories are:
▪ The administration frequency of questionnaires:
patients in “TELEMEDICINE” category fill out
questionnaires more intensively than patients in
“STANDARD” category.
▪ The type of sent questionnaires: patients in
“TELEMEDICINE” category fill out more
types of questionnaires than patients in
“STANDARD” category.
The IBD Tool’s questionnaires assess various life
aspects. Monthly questionnaires are:
▪ HBI (Harvey Bradshaw Index): it consists of 5
questions, and it is used only for Crohn’s
patients (Harvey, 1980). It evaluates the
patient’s well-being, abdominal pain, the
number of liquid or soft bowel movements, the
presence of abdominal mass and the presence of
complications. It is sometimes compiled by
clinicians to compare the results with patient
scores.
▪ SCCAI (Simple Clinical Colitis Activity Index):
it is used only for ulcerative colitis patients, and
it is composed by 13 questions that refer to the
symptoms of the last week, to bowel
movements, episodes of fecal incontinence,
blood in the stool, joint pain, erythema and any
infections (Bennebroek Evertsz’, 2013). It is
sometimes compiled by clinicians to compare
the results with patient scores.
▪ MIAH (Monitor IBD at Home): it is constructed
in both a version for patients with Crohn’s
disease (MIAH-CD) and for patients with
ulcerative colitis (MIAH-UC), with respectively
6 and 5 questions (de Jong, 2018).
▪ IBD-DISK (Inflammatory Bowel Disease -
Disability Index disk form): it was validated
starting from a previous questionnaire (the IBD-
DI: Inflammatory-Bowel-Disease Disability
Index) with some modifications; it is based on
10 items, about abdominal pain, regulating
defecation, education and work, sleep, energy,
emotions, body image, sexual functions, and
joint pain (Gosh et al., 2017).
3-Monthly Questionnaire are:
▪ PRISM (Pictorial Representation of Illness and
Self Measure): it is not made up of questions,
but of two circles, one represents the disease, the
other represents the patient; the user must
indicate, by moving the circles, how much he
Evaluation and Usage Analysis of IBD Tool: A Telemonitoring Platform for Inflammatory Bowel Disease
187

suffers due to his illness. The final score is
returned in terms of distance (Gosh et al., 2020).
It is sometimes compiled by clinicians to
compare the results with patient scores.
▪ PHQ9 (Patient Health Questionnaire 9 items): it
is used for the diagnosis of depression
consisting of two questions, the first of which
evaluates the symptoms of depression
(Kroenke, 2001).
▪ IPAQ-SF (International Physical Activity
Questionnaire - Short Form): it is aimed at
measuring the amount and type of physical
activity performed in the last seven days (Craig
CL, 2003).
▪ WPAI (Work Productivity and Activity Index):
it is used to assess the impact of the disease, both
Crohn’s disease and ulcerative colitis, on work
and daily activities (Reilly MC, 1993).
▪ IBDQ (Inflammatory Bowel Disease
Questionnaire): it is for quality of life
assessment. Its composition consists of 32
questions, which take into consideration
different fields about social life, emotional
health, and symptoms (Hlavaty, 2006)
(Ciccocioppo
, R., 2011).
▪ MMAS8 (Morisky Medication Scale 8 items): it
is based on 8 questions that assess adherence to
therapy. The questions relate to times when a
patient forgets to take the tablet or stops taking
it because it is believed to be ineffective or
causes discomfort (Hu W, 2020).
▪ TSQM (Treatment Satisfaction Questionnaire
for Medication): it is used to assess the level of
satisfaction or dissatisfaction with the drug that
the patient is taking. In particular, the
effectiveness, the side effects, the use of the
drug, its planning and the convenience or
inconvenience of taking it are evaluated
(Vermersch, P., 2017).
6-monthly Questionnaire are:
▪ EQ5D5L (European Quality version 5D - 5
Levels): it is about the measurement of the
quality of life, work, personal care, physical and
psychological health, usual activities, pain, and
discomfort (Herdman, 2011).
▪ PSQI (Pittsburgh Sleep Quality Index): it is for
the evaluation of sleep in the last month, with
questions regarding the time a person fell asleep,
the time taken to fall asleep, the wake-up time in
the morning, the total hours of sleep, the general
sleep quality, how many times a person wakes
up during sleep, whether a person has been
taking sleep medications, etc. (Curcio, 2012).
Patients in “standard of care” category only compile:
HBI, IBD-DISK, MIAH-CD if they suffer of Crohn’s
disease, PATIENT-SCCAI, IBD-DISK and MIAH-
UC if they suffer of ulcerative colitis, IBD-DISK if
the pathology is undefined; the administration
frequency is of three months.
Patients in “telemedicine” compile all the
questionnaires with their regular administration
frequency.
2.2 Platform Structure
The web-app was built by using different
technologies. IBD Tool comprises two parts: the
frontend and the backend. The frontend is the user
interface of the platform, and it is the visible part of
it, which can be reached from every browser.
The used framework is Angular, an open-source
framework for the creation of single page client
applications, based on Typescript, an object-oriented
programming language, CSS (Cascading Style
Sheet), and HTML (HyperText Markup Language).
Furthermore, Angular is a tool for developing multi-
platform applications. Through some toolkits, it is
possible to develop responsive applications.
To implement the backend, Java programming
language is chosen. This language is an object-
oriented programming language, and it can be used
on Spring Boot, one of the frameworks for creating
web applications based on microservices. The IBD
Tool backend is organized following the multitier
architecture, which matches perfectly with the
instruments made available by Spring. Specifically,
IBD Tool is a 4-tier architecture, and these layers are:
▪ Presentation Layer
▪ Service Layer
▪ Data Domain Layer
▪ Data Access Layer
Communication between frontend and backend is
done by the HTTP (HyperText Transfer Protocol).
For all the features, IBD Tool can be defined as a
REST (Representational State Transfer) architecture,
completely compatible with the HTTP (Figure 1).
Security issues were considered by guaranteeing
the access to the platform by username and password
and checking the role of the user who logs into the
application. Furthermore, Spring Security and use of
a JWT (Json-Web Token) permit an additional
security level.
All data is saved in some collections of a
MongoDB cluster, specifically created for IBD Tool.
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
188
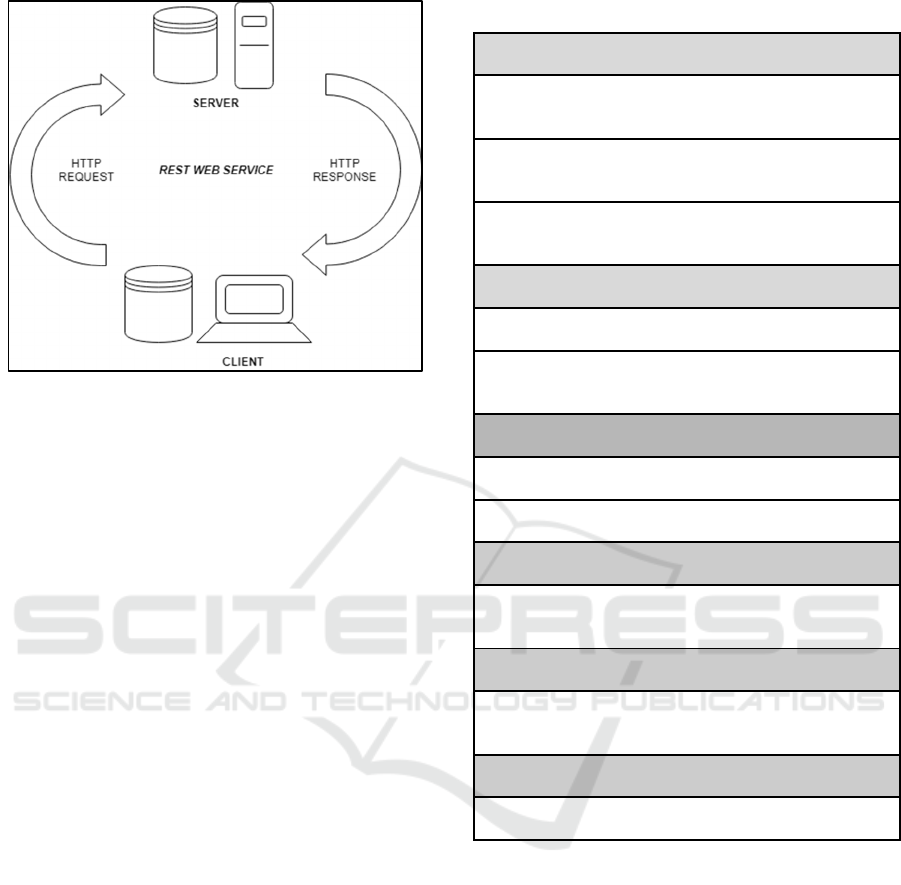
Figure 1: Web-Platform Architecture. the Figure Shows
How the Web-Client and the Web-Server Interact through
the HTTP.
2.2.1 Supporting Instruments for
Development
Some other tools are used to support the development
and the release of the web-app. GitHub is used to host
all the code of the backend and the frontend,
facilitating updates, and merging code’s procedures.
Heroku is used as a server service, where the backend
is hosted and directly linked to the GitHub code.
Firebase Hosting is used to host the frontend of the
web-app, while Firebase Cloud Messaging is used to
manage the real-time communication. IBD Tool also
relies on a Gmail account to send emails to users.
2.3 Validation’s Instruments for the
Platform
To assess the web-platform’s efficiency, a new
satisfaction questionnaire was created by consulting
widespread questionnaires for the evaluation of
telemedicine services, as TUQ (Telehealth Usability
Questionnaire) (Parmanto, 2016) and TSQ
(Telemedicine Satisfaction Questionnaire) (Yip,
2003).
This new questionnaire is composed of 10
questions about the quality of care provided, the ease
of use and learnability, the satisfaction and future use,
and the interaction quality. Last question is an empty
box where users can give their suggestions. This
questionnaire is administered only to patients. Each
answer can be in a range of 1-10, where 1 means “not-
at-all” and 10 “very much”. The structure of the
questionnaire is in Table 1.
Table 1: Satisfaction Questionnaire for IBD Tool.
Qualit
y
of care
p
rovide
d
I think that IBD Tool improved the quality of service
offered b
y
Mauriziano Hos
p
ital of Turin
I think the service I obtained was better thanks to IBD
Tool
Thanks to IBD Tool, I felt more followed between a visit
and anothe
r
Satisfaction and future use
I will continue to use IBD Tool in the future
I am satisfied of the quality of service offered by IBD
Tool
Ease of use and learnabilit
y
I need assistance to use IBD Tool
IBD Tool is eas
y
and intuitive to use
Usefulness
I think IBD Tool lets me go to the hospital only when
strictly necessary
Interaction
q
ualit
y
IBD Tool made the communication with Mauriziano
Hospital’s clinicians faste
r
Suggestion box
Blank
(
To fill
)
2.4 Analysis Method
All information about patients registered on the
platform are saved in different collections of a
MongoDB cluster, specifically created for IBD Tool.
In order to communicate with MongoDB, the
repository support offered by Spring is used, making
this communication much easier than traditional
implementations.
2.4.1 User Activity Analysis
In the ‘user’ collection of MongoDB cluster, there is
a record for each enrolled patient containing clinical
variables such as, pathology, presence or absence of
previous surgery, sex, type of active therapy, age etc.
Evaluation and Usage Analysis of IBD Tool: A Telemonitoring Platform for Inflammatory Bowel Disease
189
A “lastLogin” field indicates the timestamp of the
user's last login.
This configuration allows division of patients into
different subgroups with the aim of analysing whether
the use of the platform was influenced by certain
characteristics, such as patient age or the duration of
the disease. Patients are divided in the following
subgroups:
▪ Category: Telemedicine or Standard of care
▪ Pathology: Crohn disease, Ulcerative colitis or
other
▪ Sex: Men or Women
▪ Age – Age at diagnosis: Four different ranges
(0-20, 20-40, 40-60, 60 or more years)
▪ Pathology duration: Four different ranges (0-10,
10-20, 20-30, 30 or more years)
▪ Active therapy: 5ASA-OS, TOPICA, GCS-OS,
IMM., BIO
▪ Presence of previous surgery
For each of the subgroups, activity and inactivity rate
of patients are calculated, considering:
activity rate =
(1)
inactivity rate =
(2)
Being inactive has a different meaning if users are in
“telemedicine” or “standard of care” category. When
a user of category “telemedicine” is inactive he/she
has not accessed the platform for 4 months or more.
When a user of the category “standard of care” is
inactive he/she has not accessed the platform for 7
months or more. Furthermore, users who are
classified as “unlogged in” are those who did not log
in the platform after at least 2 weeks from the
registration phase.
2.4.2 Questionnaires Filling Frequency
Analysis
All the compiled questionnaires are saved into a
‘questionnaire’ collection of MongoDB cluster. Each
record contains the answers given by the patient, final
score, and type of questionnaire.
Mean number of compiled questionnaires per
patient is calculated with the aim of analysing user
activity, considering:
mean per user =
(3)
This number is calculated for each type of
questionnaire. Furthermore, questionnaires are
addressed to different patients, based on category
and/or pathology.
Regarding the satisfaction questionnaire, it was
created following the template of the clinical
questionnaires. To warn all the users of the platform,
a new section was added to the user "personal page"
and an email was sent to each patient with the link to
the questionnaire.
3 RESULTS AND DISCUSSION
3.1 Results
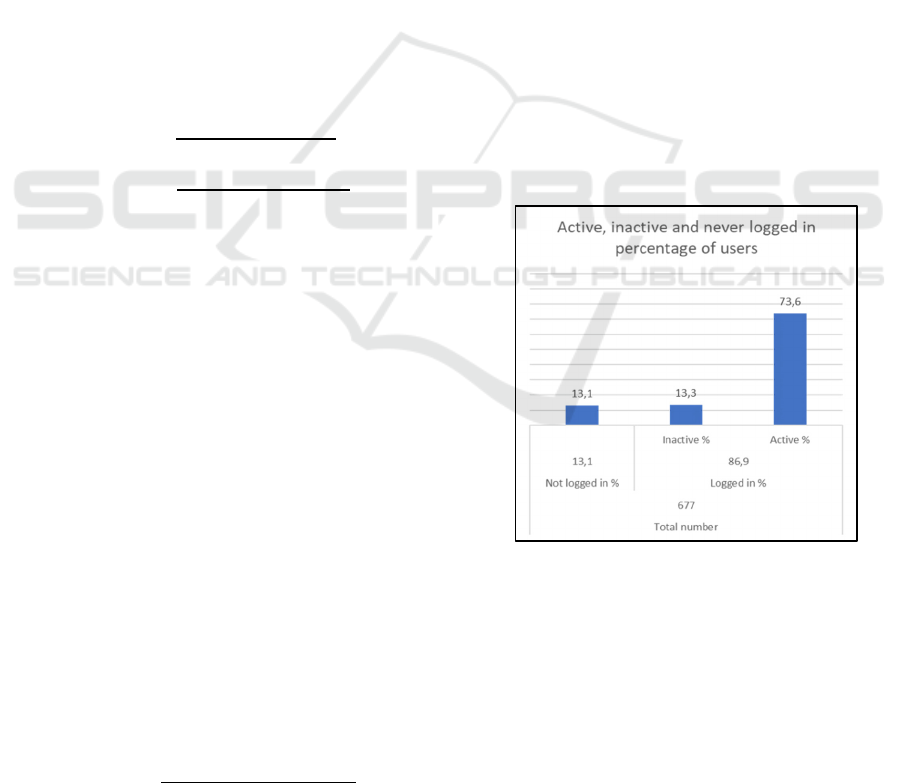
From the analysis of how many users are active or
inactive, referring to the access and the utilization of
the platform, it was found that among a total number
of patients of 677, 86,9% logged in the platform at
least once, while the 13,1 % did not. Among users
who logged in at least once, the 73,6% are active, so
they constantly access the platform, compile
questionnaires and/or write some chat messages to the
clinician, while the 13,3% are inactive (Figure 2).
Figure 2: Distribution of the 677 registered users in logged
and unlogged in. Logged in users are divided into active and
inactive. Only active users are those who regularly use the
web-platform.
Analysis of registered users reveals that there are 677
global users (constantly increasing), who can be
differently distributed depending on variables of
interest (category, age, sex, pathology, pathology
duration, etc.). The balance between telemedicine and
standard of care users is about equal, as well as among
users suffering from Crohn's disease (CD) and
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
190
ulcerative colitis (UC), while there is a small
percentage of patients (1,6%) whose disease is still
unclassified (IBD-U). In the web-platform male and
female are balanced. Most of the recruited users
belong to the age groups 20-40 and 40-60, followed
by the age group 60+ and only lastly by the age group
0-20. This is because pediatric users have never been
foreseen until now. In these data, pathologies are
mostly diagnosed in the age range of 20-40 (52,9%),
followed by 0-20 (23,5%), 40-60 (20,5%), and 60+
(2,2%). Then, pathology duration in this population
of users is mostly about 0-20 years (40,8%), followed
by 20-40 (30,4%), 40-60 (19,6%) and 60+ (8,3%).
Furthermore, in the field of ongoing therapies, the
most frequent therapy is the 5-ASA-OS because
52,9% of users are undergoing this therapy and some
of them in combination with another. The second
most frequent therapy is biologic, which involves
38,7% of users. All this information is reported in
Table 2.
Table 2: Distribution of registered users by category,
disease, sex, age, age at diagnosis, pathology duration,
ongoing therapy, and previous surgery. For both age at
diagnosis and pathology duration, there is information on
671 instead of 677 people because for 6 patients there are
not information about these fields.
Users Total
Global 677
Category Total
Telemedicine 338 49,9%
Standar
d
339 50,1%
Disease Total
CD 354 52,3%
UC 312 46,1%
IBD-U 11 1,6%
Sex Total
Men 333 49,2%
Women 336 49,6%
Missing 8 1,2%
Age Total
0-20 years 13 1,9%
20-40 years 265 39,1%
40-60 years 284 41,9%
60+ years 115 17,0%
Age at diagnosis Total
0-20 years 159 23,5%
20-40 years 358 52,9%
40-60 years 139 20,5%
60+ years 15 2,2%
Pathology
duration
Total
0-20 years 276 40,8%
10-20 years 206 30,4%
20-30 years 133 19,6%
30+ years 56 8,3%
Ongoing therapy Total
5-ASA-OS 358 52,9%
TOPIC 71 10,5%
GCS-OS 79 11,7%
IMM. 37 5,5%
BIO. 262 38,7%
Previous surgery Total
Yes 266 39,3%
No 411 60,7%
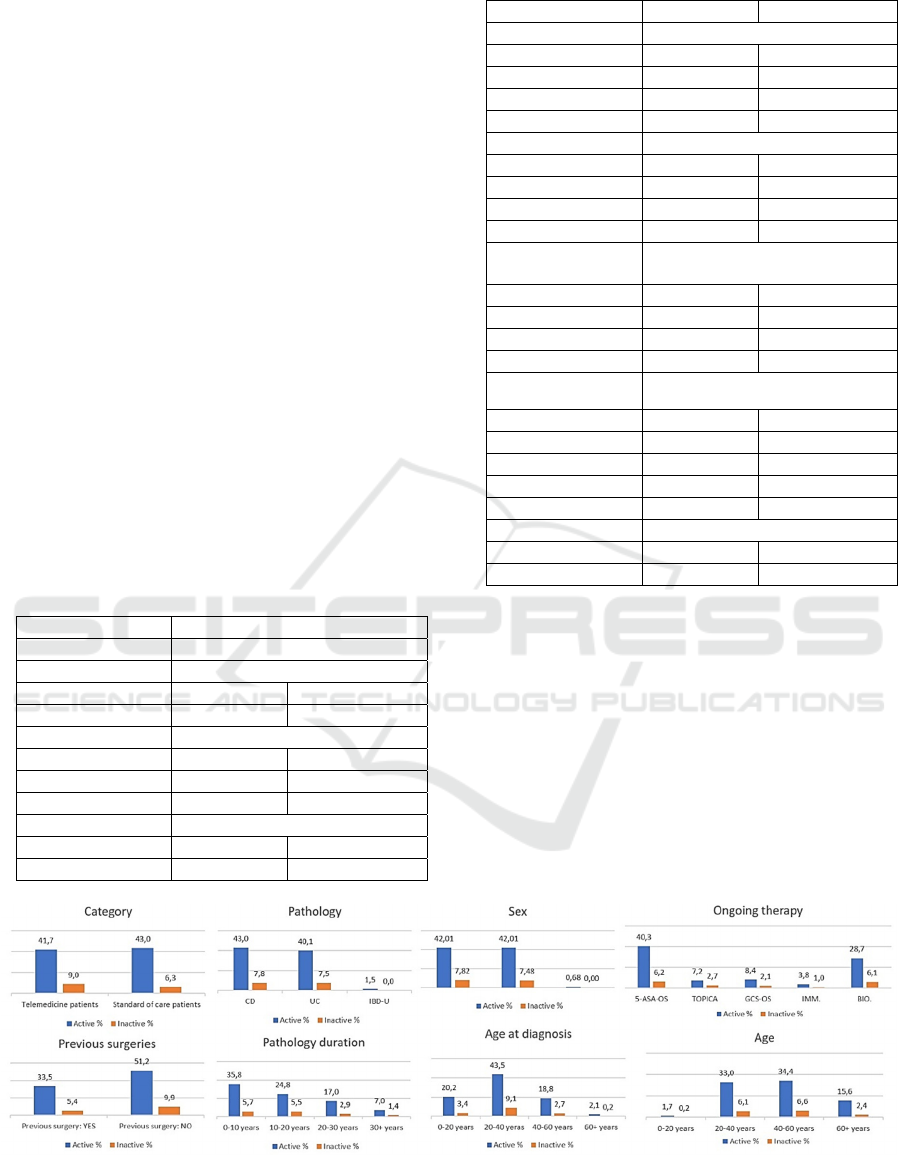
Distribution of logged in users (both active and
inactive) is analysed by considering different sub-
groups (category, sex, pathology, age, pathology
duration, ongoing therapy, age at diagnosis, and
previous surgeries) (Figure 3).
The difference in the involvement in the
application is analysed in terms of activity rate and
inactivity rate between each sub-group
(telemedicine/standard of care, men/women, etc)
(Figure 4).
Figure 3: Active and inactive patient percentage divided by sub-groups. Each single graph is referred to a different patient
distribution: category, pathology, sex, ongoing therapy, previous surgery, pathology duration, age at diagnosis, and age. Each
percentage.
Evaluation and Usage Analysis of IBD Tool: A Telemonitoring Platform for Inflammatory Bowel Disease
191
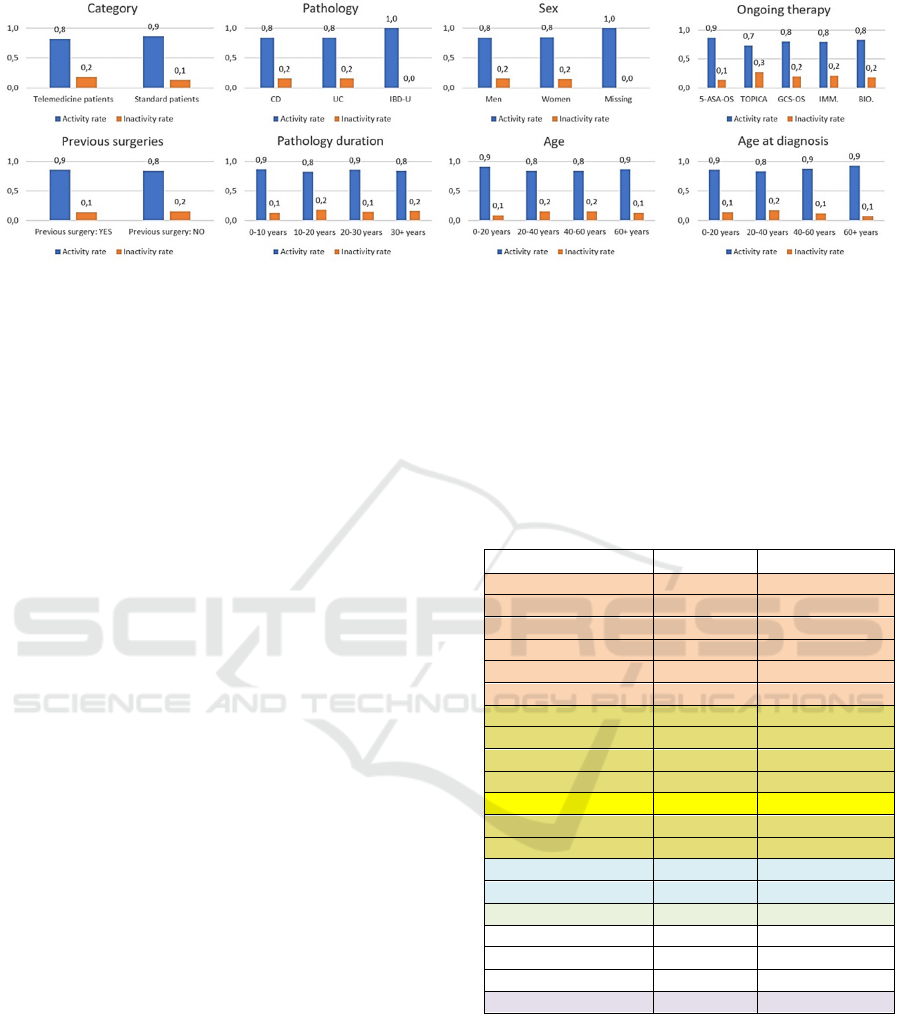
Figure 4: Activity and inactivity rate in each sub-group. Each single graph is referred to a different patient distribution:
category, pathology, sex, ongoing therapy, previous surgery, pathology duration, age at diagnosis, and age. The figure shows
high activity.
For each sub-group the number of users is different,
except for category and sex, in which there is a major
balance (Table 2). Considering the category, 50% of
users belong to the “telemedicine” program (338
users) and 50% belong to the “standard of care”
program (339 users). Active telemedicine users are
41,7%, while inactive are 9,0%; active standard of
care users are 43,0%, while inactive are 6,3% (Figure
3). The inactivity rate of telemedicine users is 0,2
against the 0,1 of standard of care users (Figure 4).
Considering pathology and sex, the balance between
active and inactive users is quite the same. Although
the percentage of active Crohn’s disease users is
43,0% against the 40,1% of ulcerative colitis, the total
number of Crohn’s users (354) is higher than those
who suffer from ulcerative colitis (312) (Figure 3).
Considering sex, the activity rate of men is 0,8, for
women is 0,8 (Figure 4). Considering age groups, it
can be observed that they all have a similar degree of
participation in the platform and the activity rate is in
the range 0,8-0,9 for each group (Figure 4). Same can
be said if the population is divided by pathology
duration (activity range: 0,8-0,9) and age at diagnosis
(activity range: 0,8-0.9) (Figure 4).
Furthermore, those who have had surgery
(activity rate of 0,9) have a degree of involvement in
the application quite higher to those who have not had
any (activity rate of 0,8) (Figure 4). Considering the
ongoing therapy, each group has an activity rate in the
range of 0,7-0,9 (Figure 4).
The activity of users was also taken into
consideration in terms of compiled questionnaires
(Table 3). Clinician’s questionnaires have a mean per
user higher because all the patients are followed by 3
physician users.
Table 3: Compiled questionnaires and corresponding mean
per users. Red part of the table indicates monthly
questionnaires; light yellow part of the table scheduled 3-
monthly questionnaires (except for PRISM which has been
compiled also during the face-to-face visit with physicians);
light blue part of the table indicates 6-monthly
questionnaires; grey part represents satisfaction
questionnaire; white represents questionnaires compiled by
physicians.
Questionnaire Number
Mean per user
HBI 1764 5
PATIENT-SSCAI 1586 5,1
IBD-DIS
K
3068 9,5
MIAH-CD 1626 4,6
MIAH-UC 1420 4,6
PATIENT-SSCAI 1586 5,1
MMAS8 507 1,5
PHQ9 552 1,6
IBDQ 395 1,2
IPAQ-SF 529 1,6
PRISM 1165 3,4
TSQM 475 1,4
WPAI 484 1,4
PSQI 226 0,7
EQ5D5L 238 0,7
SATISFACTION 285 0,4
CLINICAL-HBI 561 187
CLINICAL-SCCAI 510 170
CLINICAL-PRISM 1071 357
Total 16439
The last analysis section is about the user
valuation of the web-platform through the satisfaction
questionnaire. In the following analysis, only
questionnaires completed within 5 days of
publication and notification of the satisfaction
questionnaire were considered. 285 over 677 users
compiled the questionnaire, and they were mostly
active users (only 2 over 285 inactive users compiled
the questionnaire). IBD Tool obtained a global mean
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
192
score of 7,4 over 10 in “quality of care provided”, 8,1
over 10 in “satisfaction and future use”, 8,5 over 10
on “ease of use and learnability”, 6,4 over 10 in
“usefulness”, and 6,9 over 10 in “interaction quality”
(Table 4).
Table 4: Average score resulting from the analysis of the
285 satisfaction questionnaires.
Quality of care provided Mean
score
I think that IBD Tool improved the quality of
service offered by Mauriziano Hospital of
Turin
7,5
I think the service I obtained was better
thanks to IBD Tool
7,1
Thanks to IBD Tool, I felt more followed
b
etween a visit and anothe
r
7,6
Satisfaction and future use
I will continue to use IBD Tool in the future 8,4
I am satisfied of the quality of service
offered by IBD Tool
7,8
Ease of use and learnabilit
y
I need assistance to use IBD Tool 1,7
IBD Tool is eas
y
and intuitive to use 8,7
Usefulness
I think IBD Tool lets me go to the hospital
onl
y
when strictl
y
necessar
y
6,4
Interaction
q
ualit
y
IBD Tool made the communication with
Mauriziano Hos
p
ital’s clinicians faste
r
6,9
Su
gg
estion box
Blank
(
To fill
)
3.2 Discussion
Rate of users who constantly access and use the
platform is high, the 73,6%. Users who are classified
as “unlogged in” are those who have been registered
by the physician, but have never accessed the web-
app. These users declared interest on the
telemonitoring program, but never joined the service.
Active users compile with diligence all the
received questionnaires; the different values of
compiled questionnaires per patient are since not all
the questionnaires are administered to the patients
with the same frequency. Questionnaires like HBI,
Patient-SCCAI, MIAH-UC, MIAH-CD and IBD-
DISK are administered monthly to telemedicine users
and, consequently, the number of compiled
questionnaires of this type is higher. The number of
questionnaires like PRISM, HBI, Patient-SCCAI or
clinical ones is higher because they are compiled even
at the time of the visit.
Evaluation results on satisfaction questionnaire
show that most of analysis fields obtained good
marks. Critical issues came from limitations of
hospital face-to-face visits. Most of users think that
IBD Tool is easy to use, intuitive and that there is no
need of help for using it and answering to
questionnaires. Most of them will continue to use IBD
Tool in the future. Generally, satisfaction is good
among active users.
4 CONCLUSIONS
Potential of this web-app is manifold, both in the
short term and in the long term. In the short term, it
has a direct effect on patients, allowing them to feel
followed and accompanied by physicians even at a
distance. This allows the consequent monitoring and
prevention of the disease degeneration.
In the long term, the development of a machine
learning algorithm is planned. The goal is to process
the collected data, to assess the risk of degeneration
considering combinations of variables present in the
questionnaires.
Patient point of view should be highlighted.
Therefore, they were provided with a satisfaction
questionnaire. This questionnaire allows the
evaluation of the application on the patient side. One
of the goals was to facilitate all-ages patients to easily
utilize the application.
In this questionnaire the possibility to add any
suggestions was given. From the analysis of all the
suggestions, it emerged that a considerable number of
patients would like a notes section at the end of the
questionnaires to be able to argue their answers when
multiple choices are not enough.
Evaluation and Usage Analysis of IBD Tool: A Telemonitoring Platform for Inflammatory Bowel Disease
193

Another emerging need concerns having a patient
section where it is possible to have information about
the disease using graphs that summarize the course of
the pathology to have a greater awareness of their
state of health.
Results of the analysis on the activity and on the
use of IBD Tool have shown a great involvement.
Patients constantly compile questionnaires, contact
the clinicians through the platform for any kind of
technical or medical problem. Also, clinicians
constantly use the web-platform and take into
consideration the questionnaire scores to make their
clinical evaluations.
The results of this study encourage us to improve
the platform and service by trying to consider patient
suggestions.
REFERENCES
Bokolo Anthony Jnr. Use of Telemedicine and Virtual Care
for Remote Treatment in Response to COVID-19
Pandemic. J Med Syst 44, 132 (2020).
https://doi.org/10.1007/s10916-020-01596-5
Harvey, R., & Bradshaw, J. (1980). A simple Index of
Crohn’s-Disease Activity. The Lancet, 315(8167),514.
https://doi.org/10.1016/s0140-6736(80)92767-1
Bennebroek Evertsz’, F., Nieuwkerk, P. T., Stokkers, P. C.,
Ponsioen, C. Y., Bockting, C. L., Sanderman, R., &
Sprangers, M. A. (2013). The Patient Simple Clinical
Colitis Activity Index (P-SCCAI) can detect ulcerative
colitis (UC) disease activity in remission: A comparison
of the P-SCCAI with clinician-based SCCAI and
biological markers. Journal of Crohn’s and Colitis,
7(11), 890–900. https://doi.org/10.1016/j.crohns.
2012.11.007
de Jong, M. J., Roosen, D., Degens, J. H. R. J., van den
Heuvel, T. R. A., Romberg-Camps, M., Hameeteman,
W., Bodelier, A. G. L., Romanko, I., Lukas, M.,
Winkens, B., Markus, T., Masclee, A. A. M., van
Tubergen, A., Jonkers, D. M. A. E., & Pierik, M. J.
(2018). Development and Validation of a Patient-
reported Score to Screen for Mucosal Inflammation in
Inflammatory Bowel Disease. Journal of Crohn’s and
Colitis, 13(5), 555–563. https://doi.org/10.1093/ecco-
jcc/jjy196
Ghosh, S., Sensky, T., Casellas, F., Rioux, L. C., Ahmad,
T., Márquez, J. R., Vanasek, T., Gubonina, I., Sezgin,
O., Ardizzone, S., Kligys, K., Petersson, J., Suzuki, Y.,
& Peyrin-Biroulet, L. (2020). A Global, Prospective,
Observational Study Measuring Disease Burden and
Suffering in Patients With Ulcerative Colitis, Using the
Pictorial Representation of Illness and Self-measure
Tool. Journal of Crohn’s and Colitis, 15(2), 228–237.
https://doi.org/10.1093/ecco-jcc/jjaa159
Ghosh, S., Louis, E., Beaugerie, L., Bossuyt, P., Bouguen,
G., Bourreille, A., Ferrante, M., Franchimont, D., Frost,
K., Hebuterne, X., Marshall, J. K., OʼShea, C.,
Rosenfeld, G., Williams, C., & Peyrin-Biroulet, L.
(2017). Development of the IBD Disk. Inflammatory
Bowel Diseases, 23(3), 333–340. https://doi.org/10
.1097/mib.0000000000001033
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001).
The PHQ-9. Journal of General Internal Medicine,
16(9), 606–613. https://doi.org/10.1046/j.1525-497.
2001.016009606.x
Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth
ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A,
Sallis JF, Oja P. International physical activity
questionnaire: 12-country reliability and validity. Med
Sci Sports Exerc. 2003 Aug;35(8):1381-95. doi:
10.1249/01.MSS.0000078924.61453.FB. PMID: 1290
0694.
Reilly MC, Zbrozek AS, Dukes EM. The validity and
reproducibility of a work productivity and activity
impairment instrument. Pharmacoeconomics. 1993
Nov;4(5):353-65. doi: 10.2165/00019053-199304050-
00006. PMID: 10146874.
Curcio, G., Tempesta, D., Scarlata, S., Marzano, C.,
Moroni, F., Rossini, P. M., Ferrara, M., & de Gennaro,
L. (2012). Validity of the Italian Version of the
Pittsburgh Sleep Quality Index (PSQI). Neurological
Sciences, 34(4), 511–519. https://doi.org/10.1007/s
10072-012-1085-y
Hlavaty, T., Persoons, P., Vermeire, S., Ferrante, M.,
Pierik, M., van Assche, G., & Rutgeerts, P. (2006).
Evaluation of short-term responsiveness and cutoff
values of inflammatory bowel disease questionnaire in
Crohnʼs disease. Inflammatory Bowel Diseases, 12(3),
199–204. https://doi.org/10.1097/01.mib.0000217768.3
Ciccocioppo, R., Klersy, C., Russo, M. L., Valli, M.,
Boccaccio, V., Imbesi, V., Ardizzone, S., Porro, G. B.,
& Corazza, G. R. (2011). Validation of the Italian
translation of the Inflammatory Bowel Disease
Questionnaire. Digestive and Liver Disease, 43(7),
535–541. https://doi.org/10.1016/j.dld.2010.12.014
Hu W, Hu S, Zhu Y, Chen H, Chen Y. Assessing Oral
Medication Adherence and Identifying Predictors of
Low Adherence in Chinese Inflammatory Bowel
Disease Patients. Patient Prefer Adherence. 2020 Jul
2;14:1083-1092. doi: 10.2147/PPA.S250935. PMID:
32669838; PMCID: PMC7337442.
Vermersch, P., Hobart, J., Dive-Pouletty, C., Bozzi, S.,
Hass, S., & Coyle, P. K. (2017). Measuring treatment
satisfaction in MS: Is the Treatment Satisfaction
Questionnaire for Medication fit for purpose?. Multiple
sclerosis (Houndmills, Basingstoke, England), 23(4),
604–613. https://doi.org/10.1177/1352458516657441
Herdman, M., Gudex, C., Lloyd, A., Janssen, M., Kind, P.,
Parkin, D., Bonsel, G., & Badia, X. (2011).
Development and preliminary testing of the new five-
level version of EQ-5D (EQ-5D-5L). Quality of Life
Research, 20(10), 1727–1736. https://doi.org/10.1
007/s11136-011-9903-x
ICT4AWE 2022 - 8th International Conference on Information and Communication Technologies for Ageing Well and e-Health
194

Parmanto, B., Lewis, A. N., Jr, Graham, K. M., & Bertolet,
M. H. (2016). Development of the Telehealth Usability
Questionnaire (TUQ). International journal of
telerehabilitation, 8(1), 3–10. https://doi.org/10.5195/
ijt.2016.6196
Yip, M. P., Chang, A. M., Chan, J., & MacKenzie, A. E.
(2003). Development of the Telemedicine Satisfaction
Questionnaire to evaluate patient satisfaction with
telemedicine: a preliminary study. Journal of
Telemedicine and Telecare, 9(1), 46–50. https:/
/doi.org/10.1258/135763303321159693
Evaluation and Usage Analysis of IBD Tool: A Telemonitoring Platform for Inflammatory Bowel Disease
195
