
STREAM: Prototype Development of a Digital Language Identifier
Rebecca Meehan
1
, Manisha Kumari
2
, Qiang Guan
2
, Sanda Katila
3
, Joel Davidson
4
and Nichole Egbert
5
1
School of Information, Kent State University, U.S.A.
2
Department of Computer Science, Kent State University, U.S.A.
3
Visual Communication Design, Kent State University, U.S.A.
4
Akron Children’s Hospital, U.S.A.
5
Communication Studies, Kent State University, U.S.A.
Keywords: Digital Innovation, Health, Language Identifier, First Responders.
Abstract: This paper describes the development of a prototype digital language identifier (STREAM™), designed to
help improve health by shortening the time it takes for healthcare professionals and first responders working
with non-native speakers to identify a patient’s language so that the correct interpreter can be called,
enabling the patient to more quickly get the care they need. The innovation was originally designed to
address the needs for health care professionals caring for the emergent Bhutanese and Nepali community of
newcomers in Akron, Ohio, USA. Language access support through in person and electronic interpreters
continues to improve, however, there remains a need to quickly identify spoken language at points of entry
or in emergent situations. We developed and tested a digital prototype solution (Smart Translation
Enabling and Aiding Multicultural populations, aka “STREAM™” tool, patent pending) based on the
Nepali language that can be later extended to identify multiple languages. Prototype testing of STREAM™
showed that although the model predicted the correct language better than chance, accuracy needs to be
improved. Next steps include refining the model to identify spoken language in a shorter amount of time,
adding other languages to the model, and user testing among medical and emergency services professionals.
1 OBJECTIVES
This paper describes the pilot development of a
prototype digital language identifier
(“STREAM™”). The objectives of the paper include
a report of the pilot development process and
testing: (1) purpose of the prototype, (2) status of the
prototype, (3) navigation flow of the prototype, (4)
technical specifications, (5) testing and results
demonstrating successful identification of the Nepali
spoken language, and (6) next steps.
2 PURPOSE OF PROTOTYPE
The purpose of the prototype, “STREAM™”, is to
help first responders and health care professionals
when they encounter community members in need of
health care or emergency services, and whose
spoken language is unclear. This situation often
arises within cities and regions that have a new or
growing population of refugees or newcomers who
may not speak the regional language, and where first
responder and health care professionals are unable to
discern the language of these newcomers or
refugees. Currently, first responders and health care
professionals may employ tactics such as displaying
language identification cards for the patient to point
to their spoken language. They may also rely on
their best guess and initiate interpreters for the
language they suspect the person is speaking.
However, problems arise when the wrong language
is identified, the speaker cannot read, the
card/poster is not present or used, or the language is
not listed on the resource. STREAM™ (Smart
Translation Enabling and Aiding Multi-cultural
populations) is a digital language identifier used to
identify a patient’s spoken language, so that the
appropriate interpreter can be engaged in a health
care (arriving in person or calling for an
appointment) or emergency situation. STREAM™
will use spoken words from the patient, process
664
Meehan, R., Kumari, M., Guan, Q., Katila, S., Davidson, J. and Egbert, N.
STREAM: Prototype Development of a Digital Language Identifier.
DOI: 10.5220/0010893200003123
In Proceedings of the 15th Inter national Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2022) - Volume 5: HEALTHINF, pages 664-670
ISBN: 978-989-758-552-4; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

audio through an artificial intelligence (AI)
algorithm and then display the language results with
words, visual symbols and audio clues. Identifying a
patient’s language faster will assist service providers
in communicating vital health or emergency
information, expediting appropriate care, promoting
better health outcomes and improved satisfaction of
staff and patients. STREAM™ (patent pending)
aims to improve refugee health by reducing the time
it takes to connect with the right interpreter,
facilitating care delivery to the person in need.
2.1 Background
STREAM™ was developed to address the concerns
of local health care leaders in the Akron, Ohio area
who witnessed how difficult it became for health
care professionals and first responders toquickly
identify the language of a group of newcomers or
refugees. Akron, Ohio’s largest group of newcomers
is ethnically Bhutanese and Nepali speaking. Since
2008, approximately 80,000 Nepali speaking
Bhutanese adults and children have resettled in the
United States (Roka, 2017). As of 2020, estimates of
the Bhutanese community in our local area of
Akron, Ohio within Summit County, range between
4,000 and 5,000 people (Case Western Reserve
University, 2020). In 2013 Akron’s foreign-born
population held $137 million in spending power and
between 2000-2013 has increased the total housing
value in Summit County by $207 million
(Partnership for a New American Economy &
Knight Foundation, 2016; Vigdor et al., 2013). The
community is growing and showing signs of thriving
as evidenced by Bhutanese – Nepali specialty food
stores, religious services, traditional music and
community festivals (Chmura Economics &
Analytics, 2017).
2.2 Health Care
Health care professionals can encounter patients
over the phone, or in person, both in
emergency/acute or non-emergency situations, for
example setting up an appointment or asking for
information. Whether a patient calls on the phone or
arrives in person, a nurse or receptionist may notice
the person struggling with English, ask the person
what language they speak, or make a best guess,
then initiate interpreter services or choose to proceed
without connecting with an appropriate and
available interpreter. In order to help address the
health concerns of the patient efficiently, before an
interpreter is called, the health care worker needs to
know the language of the speaker. First responders
encounter these issues as well.
2.3 First Responders
First responders include police, emergency services/
911 dispatchers, EMS, and firefighters. Emergency
services/ 911 dispatchers receive thousands of calls
each year, including calls where a non-English
speaker is trying to obtain first responder help. If the
911 dispatcher cannot understand the language, they
often leverage an Emergency Interpreter Service
(Zimmermann, 1996) to interact with the caller.
Despite the availability of this resource, the 911
dispatcher still needs to know what language the
speaker is using so that the appropriate interpreter
can be utilized as quickly as possible. The moments
waiting for the appropriate translator to join the call
have been characterized as “tense,” especially when
the dispatcher does not recognize the language
spoken (VOA, 2014). Because time is critical to
addressing emergency situations, any mechanism to
bring a successful resolution to the call is valuable,
to address the emergency appropriately. Other first
responders, including the police, may seek to
understand someone’s spoken language by using a
protocol for helping someone with limited English
proficiency (LEP) (Under VI of the Civil Rights Act
of 1964 (42 U.S.C. §2000d et seq.). While the
process can vary, the protocol involves asking for a
person’s language identification card, or providing a
list of languages that a person could look through
and point to their spoken language. Other officers
may troubleshoot by asking bi-lingual colleagues to
assist them. Still, the language of the patient or
person in need may still be unknown.
2.4 Current Tools for Language
Identification
The U.S. Department of Health and Human Services
(DHHS) and the Department of Homeland Security
(DHS) developed specific tools to help someone with
LEP to communicate their language in order to seek
help from first responders or health care
professionals. These include Language Identification
cards and the “I Speak” resources. A person who
does not speak English can carry a language
identification card to show in case of emergency or
in everyday activities. The “I Speak” resource
includes both poster form and a booklet listing 70
languages written in those languages. Additionally,
health care facilities often display a poster at the
check in area of a health care office, including a
STREAM: Prototype Development of a Digital Language Identifier
665
number of languages, and allowing a non-English
speaking patient to identify the language they speak.
All of these visual tools, however, are not helpful if
the person or patient is not literate, nor if they do not
have the visual cue (poster, booklet or identification
card) with them at the time of the health encounter
or emergency. A digital solution, like STREAM™,
with both visual and audio cues, accessible from any
mobile device with access to the internet, would
allow for greater flexibility in identifying a person’s
language.
3 STATUS OF PROTOTYPE:
STREAM™
STREAM™ (patent pending) is in the early stages
of development and pilot testing. STREAM™ is a
digital solution, accessed on a smartphone, tablet or
computer, that “listens” to phrases spoken in the
speaker’s language for about 20 seconds and then,
through using an artificial intelligence (AI) and
machine learning (ML) multi-language classifier
algorithm, visually displays to the health care
professional or first responder and the speaker
(patient) what language is being spoken. Once there
is a confirmation between patient and health care
professional or first responder, the correct interpreter
can be called to help with the emergency or the
medical appointment. This process can also facilitate
an initial set of pre-programmed instructions or
phrases for the patient as to where they should go or
do next.
The STREAM™ prototype was built to address
current gaps in the Akron, Ohio community for
identifying Nepali language speakers, Akron’s
largest newcomer group. This manuscript does not
involve human subjects and does not require IRB
approval. There are about 7,117 languages which are
spoken in the world (Eberhard et al., 2020). While
the STREAM™ tool uses a multi-language classifier
algorithm and natural language samples from over
176 languages, for the purposes of prototype testing,
the tool is currently built to identify one language of
lesser diffusion (National Council on Interpreting in
Health Care, n.d.): Nepali. In future development,
STREAM™ will be trained to identify other spoken
languages to meet the needs of diverse populations.
This prototype demonstrates it is possible to identify
spoken language for those languages of lesser
diffusion. The intended primary end-users of
STREAM™ include health care professionals and
first responders (e.g. police, 911 dispatchers,
firefighters, EMS, etc.). STREAM™ is not built as
an app, but instead, it is designed in a “software as a
service” (SAAS) model, a cloud-based system,
allowing for seamless updates without requiring the
end user to reload or update their app. End users
will bookmark the URL website for STREAM™ on
their mobile phone, tablet or computer and keep it
open or easily accessible to begin an interaction
whenever needed.
4 NAVIGATION WORKFLOW OF
THE PROTOTYPE
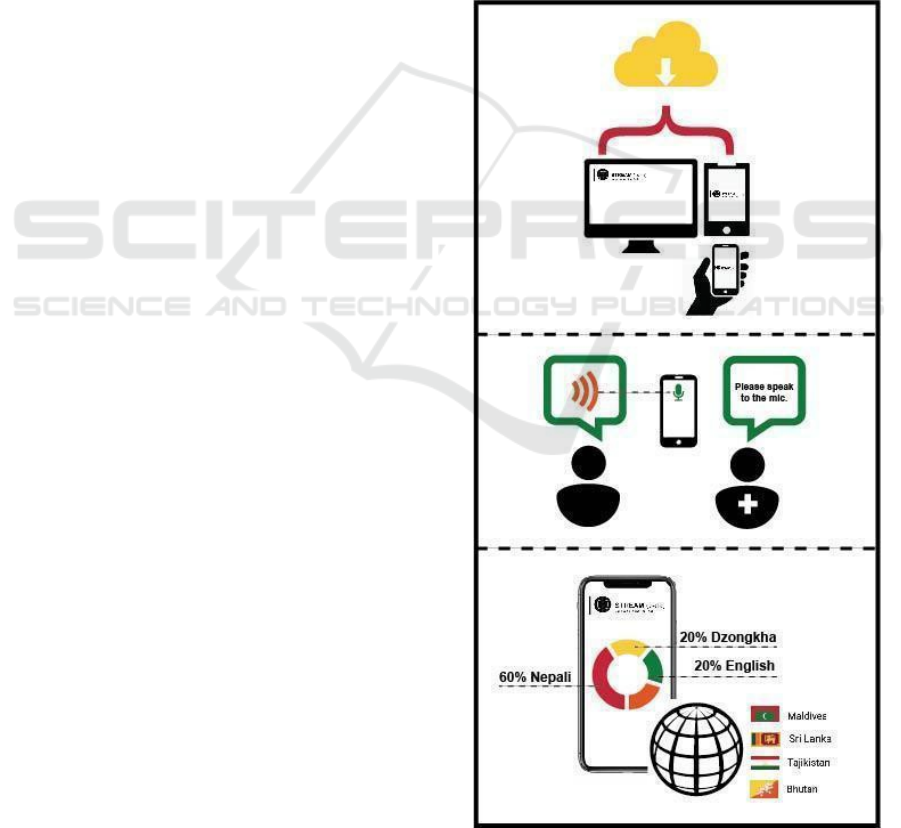
A typical use case and navigation workflow for
STREAM™ is pictured in Figure 1 and outlined in
the steps below:
Figure 1: Process for Using Stream.
HEALTHINF 2022 - 15th International Conference on Health Informatics
666
1. Health care professional or first responder (end-
user) opens the STREAM™ site.
2. When the patient is ready, the end-user clicks on
the “Identify Language” button, and has the
patient speak into the microphone of the user’s
device (e.g. mobile phone, computer, tablet, etc.)
that will “listen” to the person speaking. Visual
cues will prompt users to speak into the system.
3. After about 20 seconds, the STREAM™ tool
determines results by displaying a list of the most
likely languages, with the most likely spoken
language displayed prominently along with other
visual cues.
4. STREAM™ then prompts by displaying the
phrase: “Were you speaking X language?” along
with visual symbols and auditory cues of the
language (e.g. flags, maps, etc.)
● If yes, the user (health care professional or first
responder) then initiates connection with
the
appropriate interpreter or follows their next
intake protocol steps.
● If no, the user can point to the 4 other likely
languages on display to see if one of them is the
correct language.
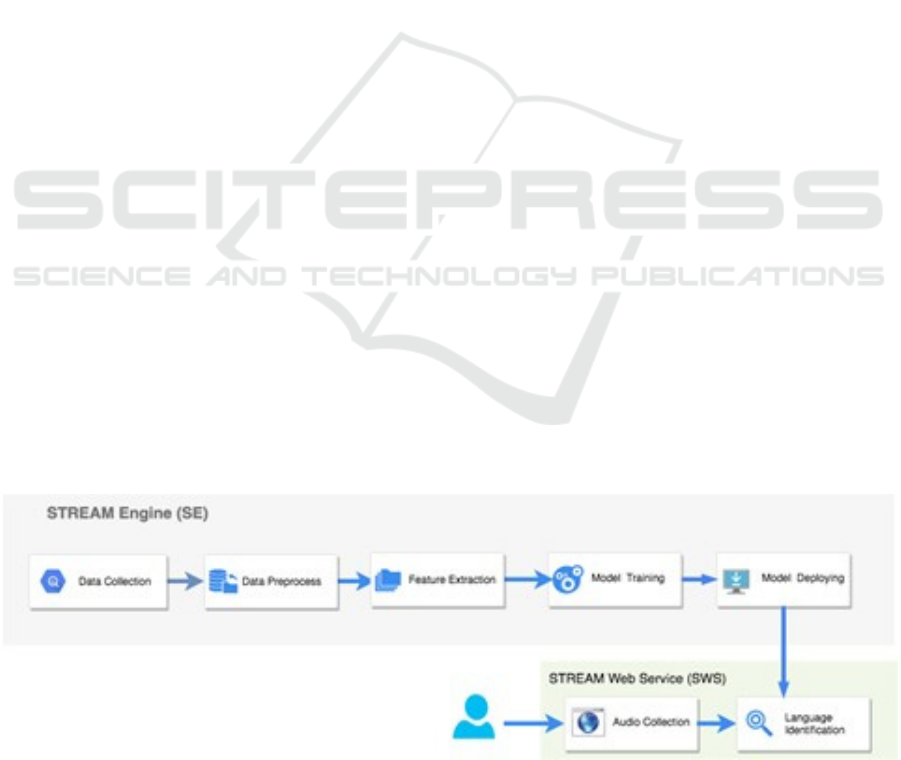
5 TECHNICAL SPECIFICATIONS
The STREAM™ prototype is based on a software
stack that includes two major components:
STREAM™ Engine (SE) and STREAM™ Web
Service (SWS), shown in Figures 2 and 3,
respectively. The SE (Fig. 2) is the heart of this
prototype, as it addresses the tasks of audio-data pre-
processing, model training and model deployment.
Our language prediction algorithm is trained on a
blended speech audio dataset including over 90,000
audio clips from 176 different languages. Audio
clips are preprocessed in the same length, same file
format as WAV files and converted into the numeric
array after extracting the features using Mel
Frequency Cepstral Coefficients (MFCCs) feature
extraction method (Bhandari, 2020; Koolagudi et al.,
2012; Shmueli, 2019). The noise removal filters are
also applied to enhance the prediction precision. The
project utilizes a multi-classification model to show
multiple possible results of spoken language, with
language with the highest prediction at the top of the
list, followed by four others. Although the model
started with using 176 + 1(Nepali) languages, the
accuracy of the prototype was lower than desired
(around 60%), the final iteration of the prototype
demo used 12 languages and added new sample data
from YouTube for each of the 12 languages. The
final datasets for the model have some variations
(different speakers, male and female voices). We
gave more preferences to Nepali by adding more
sample data compared to other 11 languages in the
final model. You can see these 12 languages in the
F1 score picture (see Table 2).
After audio data preprocessing, we applied
multiple machine learning algorithms including
eXtreme Gradient Boosting (XGBoost), Support
Vector Machine (SVM), Long Short-Term Memory
(LSTM) etc. to develop the classification models
and used ensemble techniques to combine the
models to increase the accuracy. We also
performed hyper parameter tuning and audio data
augmentation to optimize the model performance.
The accuracy of the model is identified using
Confusion Matrix and Area Under the Receiver
Operating Characteristic Curve (AUC-ROC) score.
For the final solution, to increase the model
performance we have compromised the model
accuracy very slightly and use only the XGBoost
Figure 2: STREAM™ System Architecture / STREAM Engine (SE).
STREAM: Prototype Development of a Digital Language Identifier
667
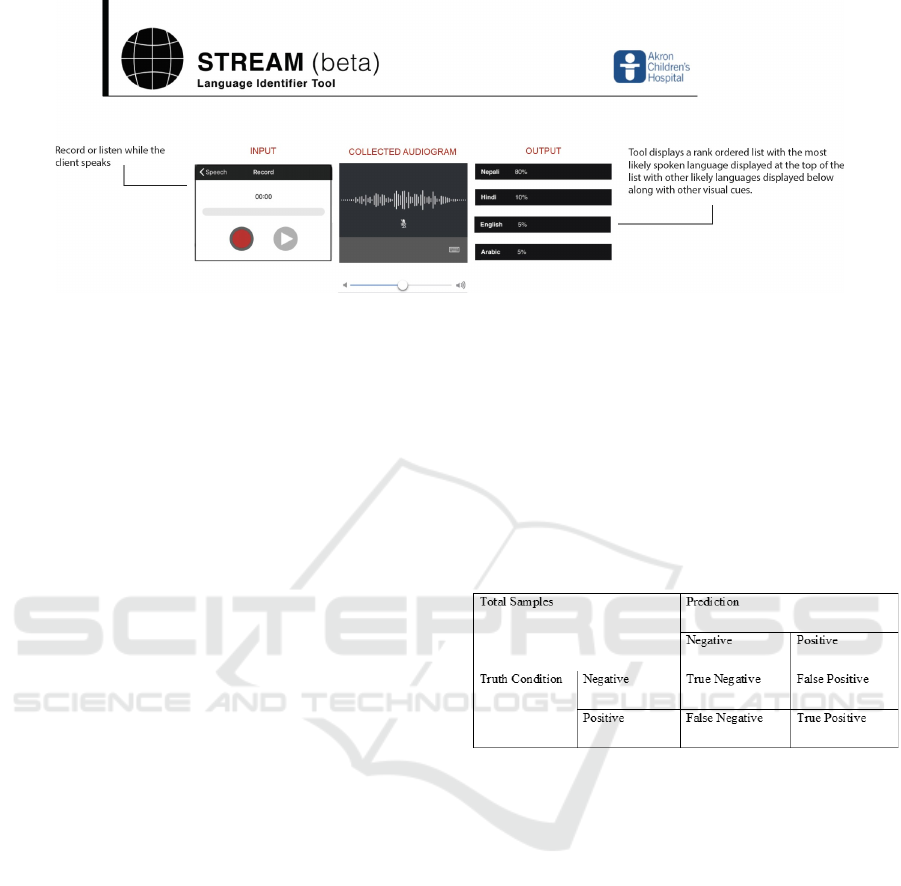
Figure 3: Prototype of STREAM™ Web Service (SWS).
multiclass algorithm to train the language prediction
model with fine-tuned parameters for the Nepali
language specifically as the target language for the
prototype. After the model is evaluated, if it satisfies
the required prediction accuracy, it will be deployed
to the STREAM™ Web Service (SWS) host for the
prototype (shown in Fig 3).
SWS provides human-computer interactive
service, which allows the end users to input a short
sample of speaking (20 seconds currently). SWS
will automatically process the audio data and
parallelly feed the model(s) with the input clips of
the audio file. The SWS user interface will be tested
and modified in upcoming research and
development. (See future research section below.)
6 TESTING AND RESULTS
In training the prototype algorithm, the whole
dataset is split into a training dataset and a testing
dataset. An independent validation dataset was
collected from YouTube (with Nepali Speakers).
In order to avoid an overfitting problem, we utilize a
k-folder mechanism to split the dataset into k
folders and each time one folder is selected as the
validation dataset and the rest of the folders are used
for training the model. After k iterations, we
average the accuracy. After training the model, we
validate the model and use the independent dataset.
While used on site, the prototype we built requires
the audio inputs from speakers with the length of
20-30 seconds. The audio captured will be further
duplicated with multiple copies (in our case, we use
five copies) to feed different identifier models. The
final language identification will be determined
after summarizing the predictions from different
models.
6.1 Prediction Results
In order to evaluate the results of the prototype
predicting or identifying the correct spoken language
(Nepali), we use precision, recall, and F1-score to
illustrate the performance of our model detection
capability. We show the truth and prediction
condition in the following table (Table 1):
Table 1: Prediction Results Format.
Precision, recall and f1-score are defined
accordingly:
Precision= (True Positive)/(True Positive +
False Positive)
(1)
Recall= (True Positive)/(True Positive+
False Negative)
(2)
F1= 2x(Precision Recall)/(Precision+Recall) (3)
Precision explains how accurate the model is
out of the predicted positives. Precision value will be
between 0 and 1 (a higher value means the model is
more accurate). Recall addresses if the model has
found out all positives with value between 0 and 1
(a higher value means the model is more robust to
the false negatives). F1-score is based on precision
and recall to balance between precision and recall
with its best value at 1 and worst at 0.
HEALTHINF 2022 - 15th International Conference on Health Informatics
668
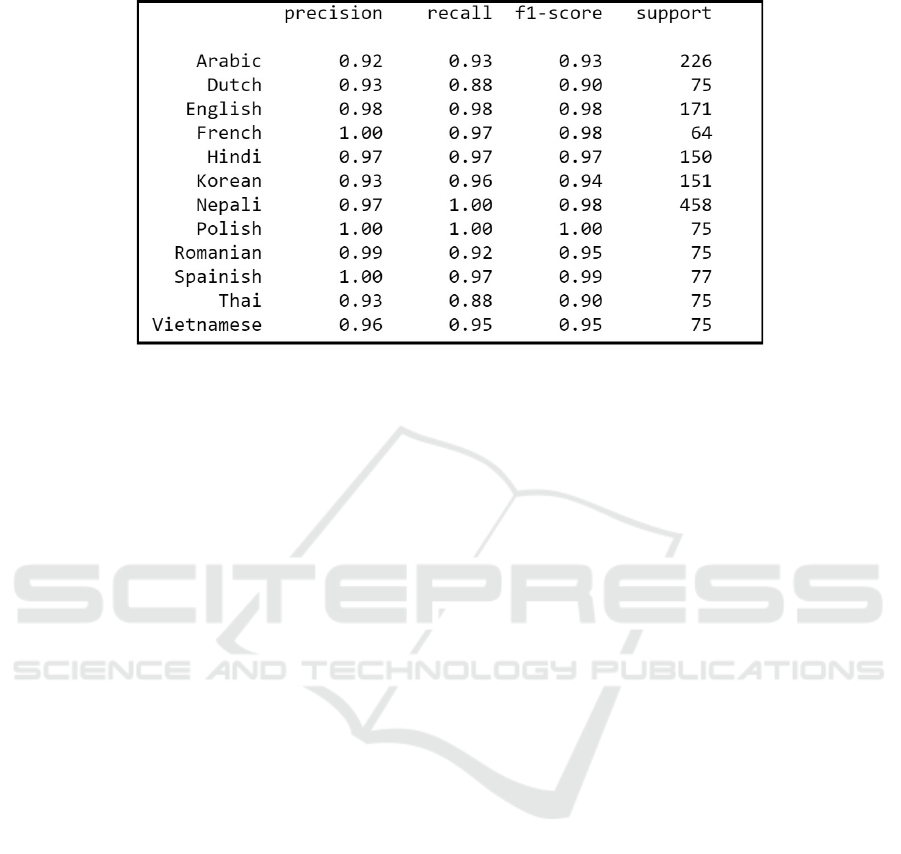
Table 2: XGBoost Multi-Classification Report.
The prototype was successful in meeting the
objective of identifying the Nepali spoken language.
This is demonstrated by the final XGBoost model
for identifying Nepali showing 97% of precision and
100% of recall with F1-score as 0.98. The F1 score
for all different languages was more than 90%
shown in the table above (Table 2).
7 NEXT STEPS
The language identifier, STREAM™, is currently in
a prototype phase, using AI to generate a list of the
top 5 potential languages that a patient is speaking.
Next steps in the prototype development
development include further refining the tool to a)
improve accuracy of results; b) accurately identify
the Nepali language (Nepali) in a shorter amount
of time; c) training the tool to identify additional
languages and dialects with greater accuracy, and
d) conducting user testing for feedback on
improving workflow and user experience of the tool.
The benefit of using the AI algorithm is that it will
continue to improve in accuracy as it is trained and
used, as it continues to learn. Further development
will use not only more languages and dialects, but
also greater volume of samples, so as to improve
accuracy of results. Moreover, development will
incorporate contextual application differences for in
person, emergency and telephone uses.
The best opportunity for developing the
prototype to be most effective is by evaluating the
use of the device in the context of applied user
scenarios. To that end, user testing of the tool will be
conducted to examine the process for identifying
unknown spoken languages in multiple settings (e.g.
911 dispatch centers, community calls by police and
firefighters, emergency departments, and health care
centers) and in multiple modalities (e.g. telephone
and in person). Specifically, user testing will look at
how the end-user accesses the STREAM™ system,
how they prompt patients to speak into the system,
and the reaction, results and follow up questions
when the results are made known. Future research
will examine the influence of STREAM™ on
reduced wait time for patients; reduced costs for
emergency and health care systems; patient
satisfaction; and satisfaction of both health care
professionals and first responders.
REFERENCES
Bhandari, A. (2020). AUC-ROC Curve in Machine
Learning Clearly Explained. https://www.analytics
vidhya.com/blog/2020/06/auc-roc-curve-machine-
learning/
Case Western Reserve University. (2020). Encyclopedia of
Cleveland History. https://case.edu/ech/
Chmura Economics & Analytics. (2017). Economic
Impact of Refugees in the Cleveland Area, Calendar
Year 2016. Refugee Services Collaborative of Greater
Cleveland. http://rsccleveland.org/wp-content/uploads/
2016/12/ EconomicImpactStudy2017FINAL.pdf
Eberhard, D. M., Simons, G. F., & Fennig, C. D. (2020).
Ethnologue: Languages of the world. 23rd edn. Dallas:
SIL International. Online: https://www. Ethnologue.
Com.
Koolagudi, S. G., Rastogi, D., & Rao, K. S. (2012).
Identification of language using mel-frequency
cepstral coefficients (MFCC). Procedia Engineering,
38. https://doi.org/10.1016/j.proeng.2012.06.392
National Council on Interpreting in Health Care. (n.d.).
Languages of Limited Diffusione. Retrieved September
STREAM: Prototype Development of a Digital Language Identifier
669

6, 2020, from https://www.ncihc.org/ languages-of-
limited-diffusion
Partnership for a New American Economy, & Knight
Foundation. (2016). Welcome to Akron: How
Immigrants and Refugees Are Contributing To
Akron’s Economic Growth. https://www.new
americaneconomy.org/wp-content/uploads/2016/06/
Welcome-to-Akron_Partnership-for-a-New-American-
Economy_June-2016.pdf
Roka, K. (2017). Adjusting to the New World: A Study of
Bhutanese Refugees’ Adaptation in the US. Journal of
Sociology and Social Work, 5(2).
https://doi.org/10.15640/jssw.v5n2a11
Shmueli, B. (2019). Multi-Class Metrics Made Simple,
Part II: the F1-score. https://towardsdata
science.com/multi-class-metrics-made-simple-part-ii-
the-f1-score-ebe8b2c2ca1
Vigdor, J. L., Calcagni, G., & Valvekhar, M. (2013).
Immigration and the Revival of American Cities: From
Preserving Manufacturing Jobs to Strengthening the
Housing Market. [online] Washington, DC:
Partnership for a New American Economy. Available
at: [Accessed 24 March 2017]. White.
VOA. (2014). It’s an Emergency in Any Language.
https://learningenglish.voanews.com/a/emergency-9
11-multi-language/2429774.html
Zimmermann, P. G. (1996). Use of interpreters in the
emergency department. Journal of Emergency
Nursing: JEN: Official Publication of the Emergency
Department Nurses Association, 22(3).
https://doi.org/10.1016/S0099-1767(96)80114-0
HEALTHINF 2022 - 15th International Conference on Health Informatics
670
