
Emergency Health Protocols Supporting Health Data Exchange,
Cloud Storage, and Indexing
Konstantinos Koutsoukos
1,2
, Chrysostomos Symvoulidis
1,2
, Athanasios Kiourtis
1
,
Argyro Mavrogiorgou
1
, Stella Dimopoulou
1,2
and Dimosthenis Kyriazis
1
1
Department of Digital Systems, University of Piraeus, Piraeus, Greece
2
BYTE S.A., Athens, Greece
Keywords: Emergency, Electronic Health Records, EHR Cloud, Remote-to-Device.
Abstract: The health industry has evolved significantly through the last years by adapting to the new technologies and
exploiting them in order to upgrade the services that provides to the people. In this context, a lot of effort has
been focused on converting medical documents to electronic health records and storing them online. However,
taking into consideration the current innovations, it is doubtless that there are many limitations when these
proposals are applied in a real-life scenario. For this reason, this paper proposes a system that combines
electronic data storage and health record exchange between individuals and authenticated medical staff in a
secure way. The specific recommendation is being evaluated through the corresponding applications and
protocols that are developed and finally, the results exhibit the solutions over existing gaps.
1 INTRODUCTION
The Healthcare industry is increasingly adopting new
technologies to enhance and facilitate citizens’ care.
Over the years, paper-based medical records have
been replaced with Electronic Health Records (EHR).
EHRs offer real-time updates of data and access from
any authorized user all around the world. Healthcare
organizations are taking advantage of modern
technology and devices such as mobiles, wearables,
sensors, etc., to gather more precise information
about the citizens and eventually offer appropriate
treatment (Zewe, 2021). The long-range scope of this
initiative is to improve the quality of life by predicting
deadly diseases, monitoring citizens’ habits, and
intervening when it is needed.
Even though almost every Health Organization
uses EHR technologies, in most cases, it is
implemented locally or in association with limited
health centers. Therefore, when a citizen needs to get
treatment and has to interact with multiple Healthcare
Practitioners (HCP), the health information is not
exchanged among them and needs to be done
traditionally, since they are not connected to a central
health network.
Consequently, a common mechanism that is used
by every healthcare organization can enhance the
HCPs’ services and offer a better treatment service to
the citizens. By exploiting two communication
protocols that will be analyzed later in Section 3 of
the paper, the EHR can be uploaded to any available
cloud service and be safely stored. Additionally,
whenever an HCP needs access to the citizen’s health
record, an intermediate mechanism will redirect her
to the health record location where the information
will be up to date. For example, in the case a citizen
has multiple appointments to attend, the data will be
immediately updated after treatment for the next HCP
to use.
The vital importance of such a mechanism is
becoming better understood by applying it to an
emergency scenario. In the case a citizen needs
immediate treatment, multiple stakeholders should be
able to gain access without any delays and the
information must be accurate and up to date. By
assuming that the citizen has made some changes or
has visited a doctor a short time before the accident,
there is a high risk that the newly generated data will
not be available to the HCPs. And in such cases, there
is no room for unnecessary risks. In this context, this
paper proposes the protocols that are responsible for
the proper communication and data exchange
between citizens, healthcare practitioners, and cloud
providers. Moreover, it suggests a background
service which facilitates the handling of urgent
Koutsoukos, K., Symvoulidis, C., Kiourtis, A., Mavrogiorgou, A., Dimopoulou, S. and Kyriazis, D.
Emergency Health Protocols Supporting Health Data Exchange, Cloud Storage, and Indexing.
DOI: 10.5220/0010878900003123
In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2022) - Volume 5: HEALTHINF, pages 597-604
ISBN: 978-989-758-552-4; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
597

situations, when the citizen is not able to grant access
to the uploaded data.
The rest of the paper is organized in the following
sections. Section 2 introduces the related work and
research that has been conducted regarding the
communication between the involved entities, the
techniques used to redirect users to the proper
services, and the security aspect of the data exchange.
It also highlights the deficiencies of these systems and
recites the features that the proposed mechanism
should cover. Afterwards, the overall methodology is
presented in section 3 by analyzing the involved
applications and by explaining the real-life scenario
step by step. Section 4 includes a demonstration of the
system’s functionality and makes a thorough
evaluation. Finally, section 5 introduces the research
conclusions and results as well as future plans.
2 RELATED WORK
2.1 Remote-to-Device (R2D) Backup
Protocol
The communication between user applications and
cloud providers is rapidly becoming a common
occurrence since it facilitates the storage of vital
personal data and its fast and constant retrieval. To
begin with, Dropbox (Dropbox for HTTP
Developers, 2021) offers the possibility to connect an
application with the cloud and interact with each
other by exchanging data. This is achieved by a group
of APIs that support the communication through a set
of HTTP endpoints that are used to establish the
communication between the two entities. In the same
direction, DataVaults (DataVaults Empowering
Secure Data Storage, Sharing and Monetisation,
2021) aims to give users the ability to fully
manipulate their data and share it with other
organizations or individuals by adopting adjustable
sharing schemes. Meanwhile, it offers an innovative
framework whose main scope is to gather information
derived from several sources and finally provide them
in a secure and interoperable manner to the users. As
the overall purpose of the paper suggests, these
technologies offer limited functionalities when it
comes to time efficiency. Therefore, it makes sense
that this kind of services should not be trusted with
vital data such as EHR.
2.2 Remote-to-Device (R2D)
Emergency Protocol
Many cloud providers offer the opportunity to handle
emergencies and other situations where data access
from third parties has a vital significance. Concerning
this, some services provide APIs that are responsible
for sharing the data with one or more stakeholders
when needed. At the same time, several studies have
proposed ways to cope with health-related incidents.
In (Oliveira et al., 2020) the authors suggest a Red
Alert Protocol (RAP) to address situations when the
citizen is not conscious. In the emergency session, a
central authority links the responsible treatment
teams to the citizen’s EHR which is stored in the
cloud. Using an access token to download the data
and an emergency key to decrypt it, the medical staff
acquires access to the medical records. After the
procedure, the access tokens are either removed or
expired and the HCPs can no longer use the citizen’s
information. Although this approach offers an
innovative way to deal with emergencies, it cannot be
used in other occasions such as medical visits. In that
way, a health organization should integrate more
systems for different situations and create a complex
procedure. In a similar manner, (Banerjee et al., 2013)
talks about a centralized cloud database that will store
every user’s medical history in a single standard-
formatted and interoperable document. By exploiting
the multi-document summarization technique, the
system creates a single summarised document that
contains the complete medical history of that person.
Using a graph-based ranking algorithm the system
creates a summary for every single document and
then a meta-document is produced to generate the
result. The main concept is to authenticate the citizen
with the use of biometric data and finally retrieve the
appropriate data to use for the operation. Even though
biometric authentication is an efficient way to access
personal records, it should not be the only option
since, in emergency cases the citizens’ condition may
not support this procedure.
2.3 Health Record Index
Health record indexing is a very crucial procedure
since the quick response and retrieval of the requested
data can be lifesaving. Especially when there are
more than one sources that EHR can be stored to, this
challenge is a lot more demanding. Several types of
research and studies take into consideration that the
needed information may be distributed in different
sources and need to be gathered. Primarily, the
authors of (Ehler et al., 2007) proposed an
HEALTHINF 2022 - 15th International Conference on Health Informatics
598

Information Retrieval (IR) tool to index and retrieve
citizens’ EHR. The system creates a table for each
document which contains a table with every word in
the document along with its frequency rate. Taking
into consideration the query, the system locates and
retrieves the documents that contain the query
keywords at a high-frequency rate. The authors in
(Wan et al., 2019) dealt with geographic data
collected from the real world through sensors. Real-
time data creates a challenge since it can be
unpredictable. Hence, they proposed a
multidimensional data indexing scheme to handle
large queries. The proposed methods are utilizing
hierarchical indexing structures by running binary
space partitioning (BSP) algorithms like kd-tree,
quad-tree, k-means clustering, and Voronoi-based
methods striving for better efficiency with less
latency. After a set of detailed simulations, it resulted
that the Voronoi diagram data index model is the most
suitable since it minimizes the average query
response time and energy consumption. These are the
parameters that have stimulated the interest of the
researchers. Finally, a recent study (Yao et al., 2018)
demonstrates an indexing mechanism over EHRs.
The overall concept is referring to citizens as data
owners and they are responsible of their own data.
Doctors, health sensors or any source that can
generate data is referred as data provider. Given the
owner’s consent, they can upload EHR to the cloud
along with an index which will be used for the
retrieval. Coming from any source, the data is always
encrypted before being uploaded to the cloud. The
request for the health records is performed in the form
of a query from an authorized health provider. The
cloud service indexes the stored data according to the
corresponding indexes and returns the proper medical
data without decrypting it. Eventually, the provider
can access the records with the use of a decryption
key. The idea of uploading EHR to a publicly
reachable location with the proper security has
significantly enhanced the communication between
medical personnel and citizens. However, these
techniques have limited efficiency when it comes to
emergencies. In most cases, the proposed way to
identify the citizen is through credentials, which it
will be a major obstacle when the data accessing is
vital. Furthermore, the proposals are trying to deal
with specific problems and circumstances and are not
flexible enough to accommodate different conditions.
2.4 Encryption Mechanisms
When it comes to personal health data it is crucial to
study thoroughly the security aspects of the proposed
system. Therefore, encryption techniques are used to
prevent internal attacks as long as secure data
transfer. Since there is a large number of security
techniques, there are studies that focus on choosing
those that can be used in the health industry.
According to (Madnani et al., 2013) these are
symmetric-key cryptography, public-key
cryptography, and attribute-based encryption. In
(Abbas et al., 2014) the proposed system encrypts the
data using an encryption key known by the cloud
provider. However, this approach raises the concern
of internal attacks considering that acquiring that key
gives access to all the stored data connected to it. The
proposal in (Yang et al., 2019) presents a system that
combines attribute-based encryption and password-
based break-glass (Scafuro et al., 2019) key to create
a self-adaptive access control scheme. More recently,
(Oliveira et al., 2020) suggests the involvement of
ciphertext-policy ABE (CP-ABE) associated with
emergency situations’ policies.
2.5 Advancements beyond the Related
Work
Resulting from the previous studies and works it has
been obvious that the storage of medical records in
cloud repositories has been rapidly evolved regarding
the plurality of services, techniques, and consistency.
Nevertheless, the ability to handle emergency
situations is what challenges the researchers since it
is very demanding to combine punctual reaction and
security. Additionally, most of the proposals are
restricted to a certain country’s infrastructure or
adjusted to a specific scenario with known and tested
circumstances. As a result, this paper proposes a
system that tries to eliminate these gaps. This is
achieved by making the service centralized so that
authenticated personnel can gain access regardless of
the country where the citizen comes from. Moreover,
it attempts to create a paradigm that HCPs can use to
download the EHR even when the citizen is
unconscious. It is important to propose a way to
secure the data in every stage of the process. Finally,
the recommended service should be applicable to any
possible scenario while it complies with all the
parameters.
3 METHODOLOGY
3.1 Involved Applications
To better understand the overall methodology, the
involved terminologies should be presented and
Emergency Health Protocols Supporting Health Data Exchange, Cloud Storage, and Indexing
599
analyzed. All the following applications are
developed in the context of the Interopehrate research
project for this research.
3.1.1 S-EHR Application
The Smart-EHR application is a mobile application
developed to be used by citizens. This application
stores locally the user’s EHR and data generated by
sensors or after a medical visit. Additionally, the user
can use the application in order to upload the EHR to
a S-EHR Cloud of their choice. Finally, as will be
thoroughly described in the following section,
citizens may give their consent for the EHR to be
accessed by authorized HCPs in emergency
situations. When a citizen registers to the service, a
Quick Response (QR) code is generated. This QR
code contains crucial information such as the
citizenId, an emergency token, an encryption key, and
the Health Record Index (HRI) location (Kiourtis et
al., 2021).
3.1.2 S-EHR Cloud
The Smart-EHR Cloud as presented in (Symvoulidis
et al., 2021) is a cloud service that provides storage
for EHRs. Taking into consideration that users have
previously agreed to share this data when needed,
authorized HCPs can access these records and use
them to treat the citizen as will be depicted later.
Furthermore, storing health data in the cloud can be
used as a backup in case the citizen’s device is
damaged or unreachable. Lastly, the S-EHR Cloud
stores audit information that keep track of every
procedure made by clinicians or citizens and can be
accessed through the citizen’s S-EHR app.
3.1.3 HCP Application
HCP application is a software application, operated
by medical staff and provides a way to access cloud
storage and download citizens’ health data assuming
that it is encrypted, and authentication operations
have been completed. More precisely, by exploiting a
set of credentials that identify both the clinician and
the healthcare organization, the system confirms that
the request is originated from an eligible and
authenticated source. Since the overall system needs
to be supported across Europe, every HCP app uses
an integrated translation system that converts the
crucial information into the appropriate language
(Bella et al., 2021).
3.2 Emergency Scenario Overview
This section demonstrates the precise procedure that
every entity is going through by the time an
emergency occurs. Moreover, the actions that need to
be done prior to this incident are also analysed by
examining the protocols.
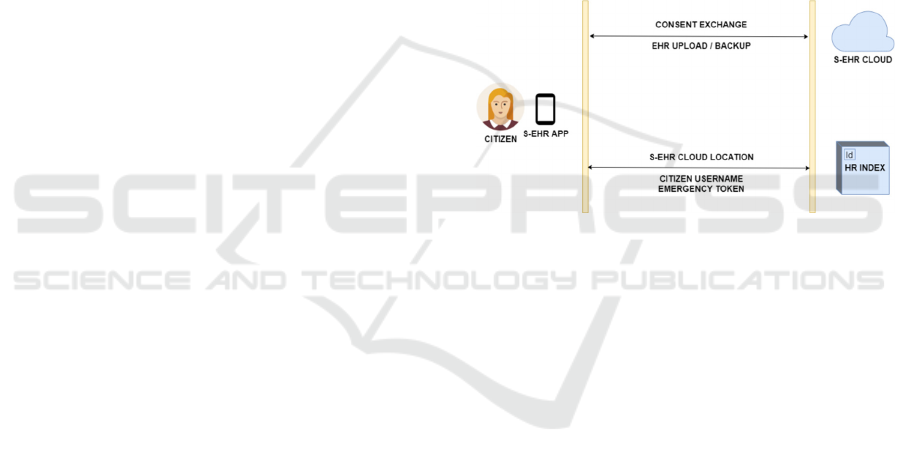
3.2.1 R2D Backup Protocol
This protocol focuses on the preliminary actions that
need to be done when a citizen starts using the S-EHR
application. Its purpose is to allow users to safely
backup their health records in a remote repository and
correspondingly download them at any time
(Symvoulidis et al., in press). Likewise, in this stage,
the citizen may sign a consent that allows HCPs to
have access to the stored data if it is necessary.
Figure 1: R2D Backup Protocol.
In Figure 1 the general idea of the protocol’s
functionality is depicted by presenting the main
operations taking place between the entities. As
detailed below, the complete procedure consists of
the following stages. Formerly, the user registers to
the preferred cloud service through the Smart-EHR
application. Later, several consents need to be signed
by the user to allow the S- EHR Cloud to store the
data and agree with the sharing of the medical record
with authorized medical staff. It is important to note
that the latter is an optional consent. In the case the
user accepts the first term, it results in generating an
access token which is sent to the mobile device. As a
result, the S-EHR application generates an encryption
key which will encrypt the data before uploading it to
the cloud. By the time the citizen agrees with the
second term, there is a sequence of actions that are
taking place. Firstly, an emergency token is generated
and stored in the app. Secondly, Smart-EHR sends
information to the HR Index, containing the cloud
provider, the citizen’s username, and the emergency
token. Then a QR code is created, containing the
encryption key, the emergency token and information
regarding the user’s HRI entry such as a citizen ID.
HEALTHINF 2022 - 15th International Conference on Health Informatics
600
However, if the latter consent is not signed, the cloud
will not be able to share the data with any third parties
and the selected service will be only used as a backup.
Taking into consideration that the first consent has
been signed, the user is able to upload the EHR to the
cloud. Using the encryption key, which is stored in
the app, the health data is being encrypted and
uploaded to the S-EHR Cloud. From now on, the
uploaded records will be automatically updated if any
changes are made to the local files. Finally, in case
the citizen uses a different device, it is always
possible to login to the S-EHR application using the
credentials and download the health records from the
cloud which will then be decrypted and accessible
through the application. It is worth mentioning that
the user can any time withdraw the consent and
change the permissions to the data.
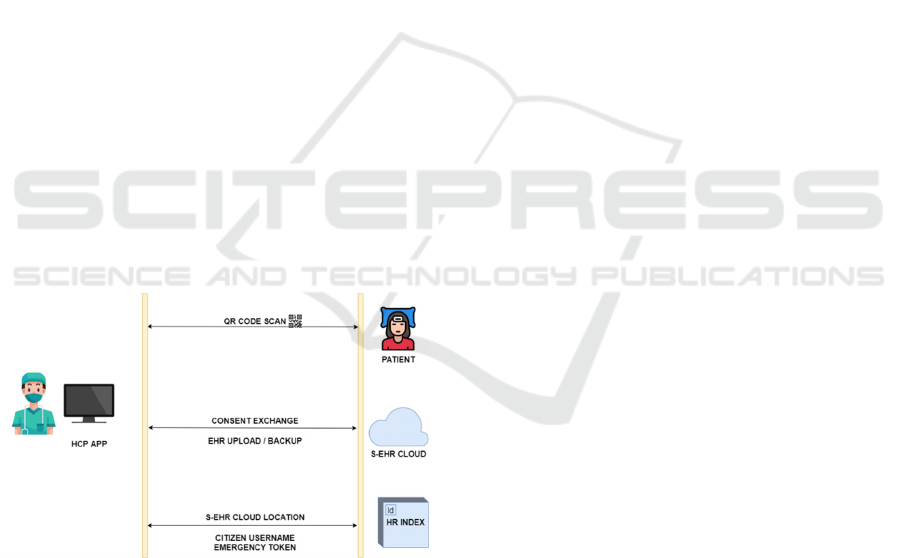
3.2.2 R2D Emergency Protocol
The R2D Emergency protocol is an internet-based
protocol which defines the actions that are taking
place between the S-EHR Cloud and the HCP
application when an emergency occurs in order to
allow the HCP to access the citizen’s health data from
the S-EHR Cloud (Symvoulidis et al., in press). Both
protocols support Fast Healthcare Interoperability
Resources (FHIR) for the exchange of EHRs
(Kiourtis et al., 2018). Moreover, compliance
checking is performed to the exchangeable files to
assure advanced interoperability.
Figure 2: R2D Emergency Protocol.
Figure 2 shows the sequence of the performed
operations when a citizen is admitted to the hospital
due to an emergency. At the initial phase of the
emergency, the HCP who is responsible for the
patient’s treatment needs to collect the QR code and
scan it to acquire the necessary information for the
operation. As described in section 3.2.1 the QR
scanning provides the emergency token which will be
used to make the request to the S-EHR Cloud, the
encryption key that will decrypt the data as long as it
is downloaded, and finally, information about the HR
Index entry to retrieve the cloud location. Following
the successful scanning, an automatic request is sent
to the HRI, and the cloud provider used by the citizen
is returned as a response. Hence, the HCP has
everything that is needed to request the citizen’s EHR
from the cloud. With the use of the emergency token
along with the HCP and healthcare center attributes,
the S-EHR Cloud approves or declines the request. In
the first case, the data is downloaded in an encrypted
format and can then be decrypted locally using the
encryption key. Otherwise, the connection is
terminated and no interaction with the data is
possible. It is worth mentioning that after the
completed verification, the connection remains open
so that the medical records on the cloud will be
updated with the new encrypted data after the
treatment is completed and the patient is discharged.
All this time, the S-EHR application creates a
notification to the citizen’s mobile regarding the
actions made by the HCP over their medical records.
3.2.3 Health Record Index
The role of the HR Index has been stated previously
with the description of the protocols. To better
understand its utility, the scenario needs to be tested
on a situation with special parameters. As it was
explained previously, the citizen chooses a cloud
provider to upload the medical information and then
acquires a QR code which will be printed also on a
card for easier access. Without the HRI, the QR code
would contain a direct link to the cloud service. On
the assumption that the user decides to use a different
cloud service, the records will be removed from the
first cloud and be encrypted and uploaded to the new
one. Supposing that an emergency occurs, and the
citizen needs to be treated immediately, the HCP will
scan the QR code as depicted earlier and will be
redirected to the wrong cloud location which does not
store the user’s records. Health Record Index
overcomes this issue since it is automatically updated
when the cloud is changed and functions as a
mediator between the HCP and the cloud. As a result,
the scanning will always return real-time information
to the health center and will prevent vital
implications. It is worth mentioning that the HR Index
is a background service and neither the S-EHR
application user nor the HCP has direct interaction
with it.
Emergency Health Protocols Supporting Health Data Exchange, Cloud Storage, and Indexing
601
3.2.4 Encryption Mechanisms
Every stage of the overall process should be
characterized by indisputable security. When it comes
to personal health data, any risks should be eliminated
on data storage and on data transit. Therefore, both
protocols are using a set of encryption technologies to
safely transfer the data and also to allow only certified
entities to have access. R2D Backup protocol uses the
Advanced Encryption Standard 256 (AES-256)
which is a symmetric-key algorithm to encrypt the
data locally in the S-EHR app. This means that a
single key is used for both encryption and decryption.
This key is exchanged between citizens and medical
staff through the QR code after scanning.
Additionally, when citizens use their credentials to
log into the S-EHR Cloud, a JSON Web Token is
returned to the mobile application. Then with the
proper JWT authorization, the encrypted data can be
uploaded to the cloud.
4 EXPERIMENTATION
4.1 Working Environment & Scenario
In this research, a set of services and libraries were
developed to demonstrate and test the functionality.
Specifically, the HCP application and the HR index
have been developed in Java v.8.0 while the S-EHR
application runs on Android v4.3.1 and above.
Regarding the two protocols, a set of Java libraries
were built to implement the communication of the
components according to the protocols’
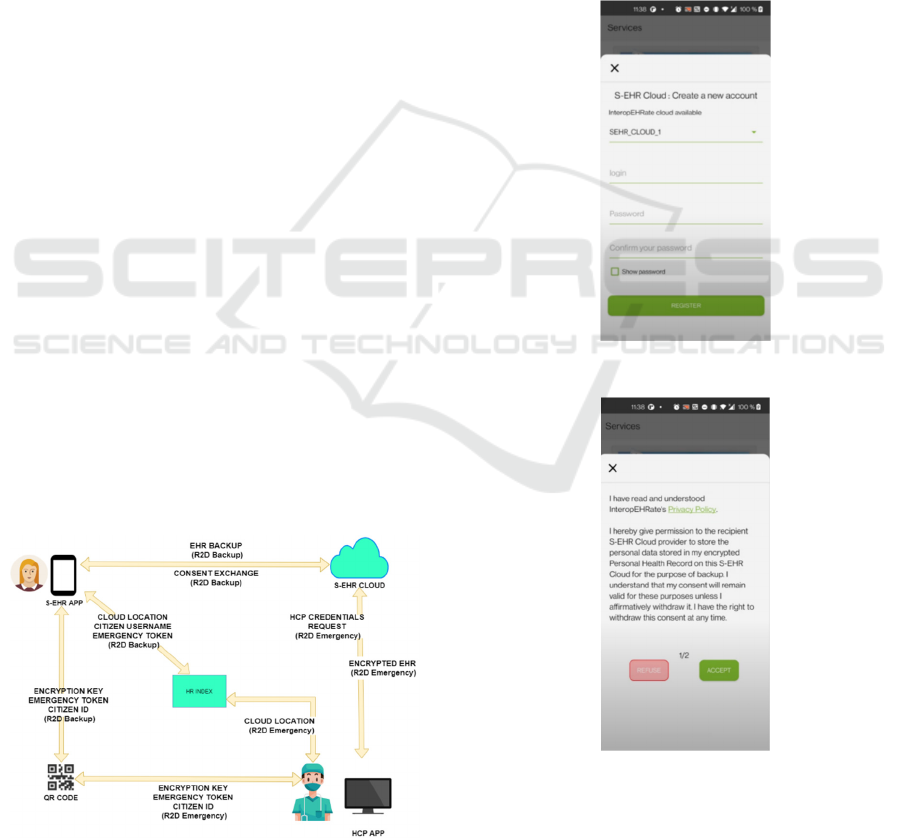
specifications. Figure 3 demonstrates all the involved
entities and the interactions between them, in the
context of the evaluation scenario that has been
implemented.
Figure 3: Overall scenario and interactions.
4.2 Preliminary Evaluation
To practically test the operational qualification of the
system, the developed services were used to
demonstrate the citizen’s user experience. At the
beginning, the citizen registers to one of the available
S-EHR Cloud providers through the S-EHR
application as shown in Figure 4. Later, two consents
need to be signed regarding the health record storage
on the cloud for backup purposes and then to allow
authorized HCPs access the health data. The
corresponding functionality is depicted in Figure 5,
Given that the consents are signed, the citizen uploads
the EHR to the S-EHR Cloud provider via the R2D
Backup protocol.
Figure 4: S-EHR Cloud registration.
Figure 5: Consent approval option.
After the successful registration, the encrypted
data is uploaded to the cloud and the QR code is
created and presented to the users along with options
to change their preferences and optionally revoke
HEALTHINF 2022 - 15th International Conference on Health Informatics
602

their signed consents. From this time, the local files
are periodically synchronized with the cloud to keep
them up-to-date. This step summarizes the user
interface regarding the Smart EHR application.
At a later time, an emergency occurs and the
citizen is transferred to the Healthcare organisasation
where HCPs need to address it in order to offer direct
treatment. To do so, they must provide their attributed
credentials to log into the HCP app. Since the citizen
is unable to assist the clinicians with vital personal
information, the unique QR code is scanned through
the HCP app. Following the scanning, the involved
information is presented encrypted in the application
interface. At this point, the HCP can request access to
the EHR. Providing the information is right and the
credentials are validated by the S-EHR Cloud, a
success message will inform the medical staff that the
connection has been established and they can access
all the citizen’s data in a structured way, via the R2D
Emergency protocol, as depicted in Figure 6.
Figure 6: EHR through the HCP app.
After the treatment, the HCP compiles a
Discharge Report with the procedure details along
with therapy and future recommendations and
uploads it with the updated data to the S-EHR Cloud.
5 CONCLUSIONS
The healthcare field has recently presented many
advancments regarding the exchange of data between
HCPs and citizens. However the limitations of the
existing systems have created the need of a proposal
that offers a functionality beyond these restrictions.
This paper, proposed a system that can take these
studies a step further. For this reason, two protocols
were defined to facilitate the secure backup of
medical data to EHR-based cloud providers and
enhance the exchange of crucial data between
Healthcare Professionals and citizens during
emergency situations. Additionally, HRI is offered to
deal with the case there are multiple cloud services
and redirect the medical staff to the proper one.
During the evaluation process, some restrictions
came up that did not comply with the initial scenario
design. For example, there is no assurance that the
citizen’s QR code will always be reachable. Morever,
the effort has been focused on handling emergency
occasions. This approach could also be applied in
other situations such as everyday medical visits but
without the proper functionalities since this paper
does not cover that view.
Therefore, concerning the following steps, the
goal is to extend the area where the protocols function
in order to be applicable in more scenarios with the
same performance. Besides, the QR code accessing
should be evaluated and saved in a way to be always
available. For the time being, QR code is the main
tool for data accessing in emergency scenarios, but
the fact that its complexity is increased as more
information is stored, it may create the need to
examine other possibilities like Near-Field
Communication (NFC) tags (Vidakis et al., 2020).
Finally, it is important to constantly improve the
performance of the protocols as far as efficiency and
security is conserned, since the needs and the figures
are always changing.
ACKNOWLEDGEMENTS
The research leading to this result has received
funding from the European Union’s Horizon 2020
research and innovation programme under grant
agreement No 826106 (InteropEHRate project).
REFERENCES
Abbas, A., & Khan, S. U. (2014). A Review on the State-
of-the-Art Privacy-Preserving Approaches in the e-
Health Clouds. IEEE Journal of Biomedical and Health
Informatics, 1431–1441.
Banerjee, A., Agrawal, P., & Rajkumar, R. (2013). Design
of a cloud based emergency healthcare service model.
2261–2264.
Bella, G., Bocca, S., Torelli, F., Dalmiani, S., & Duflot, P.
(2021, February). Design of information extractor and
natural language translator - v1. https://
www.interopehrate.eu/wp-content/uploads/2021/04/
InteropEHRate-D5.11-Design-of-information-
extractor-and-natural-language-translator-v1.pdf
DataVaults Empowering Secure Data Storage, Sharing and
Emergency Health Protocols Supporting Health Data Exchange, Cloud Storage, and Indexing
603

Monetisation. (2021). DataVaults. Retrieved 2021,
from https://www.datavaults.eu/about/
Dropbox for HTTP Developers. (2021). Dropbox.
Retrieved 2021, from https://www.dropbox.com/
developers/documentation/http/overview
Ehler, F., Ruch, P., Geissbuhler, A., & Lovis, C. (2007).
Challenges and methodology for indexing the
computerized patient record. 129(Pt 1):417–21.
Kiourtis, A., Mavrogiorgou, A., Symvoulidis, C.,
Tsigkounis, C., & Kyriazis, D. (2021, January).
Indexing of Cloud Stored Electronic Health Records for
Consented Third Party Accessing. In 2021 28th
Conference of Open Innovations Association (FRUCT)
(pp. 158-166). IEEE.
Kiourtis, A., Mavrogiorgou, A., & Kyriazis, D. (2018,
September). FHIR Ontology Mapper (FOM):
Aggregating Structural and Semantic Similarities of
Ontologies towards their Alignment to HL7 FHIR.
2018 IEEE 20th International Conference on E-Health
Networking, Applications and Services (Healthcom).
Li, M., Yu, S., Ren, K., & Lou, W. (2010). Securing
Personal Health Records in Cloud Computing: Patient-
Centric and Fine-Grained Data Access Control in
Multi-owner Settings. Lecture Notes of the Institute for
Computer Sciences, Social Informatics and
Telecommunications Engineering, 89–106.
Madnani, B., & Sreedevi, N. (2013). Attribute Based
Encryption for Scalable and Secure Sharing of Medical
Records in Cloud Computing Design and
Implementation. 2320–9801.
Scafuro, A. (2019). Break-glass Encryption. IACR
International Workshop on Public-Key Cryptography –
PKC 2019, 34–62.
Symvoulidis, C., Kiourtis, A., Mavrogiorgou, A., &
Kyriazis, D. (2021). Healthcare Provision in the Cloud:
An EHR Object Store-based Cloud Used for
Emergency. In HEALTHINF (pp. 435-442).
Symvoulidis, C., Mavrogiorgou, A., Kiourtis, A., Marinos
G., Kyriazis D. (in press). Facilitating Health
Information Exchange in Medical Emergencies. In
2021 E-Health and Bioengineering Conference (EHB).
IEEE.
T. De Oliveira, M., Bakas, A., Frimpong, E., Groot, A. E.
D., Marquering, H. A., Michalas, A., & Olabarriaga, S.
D. (2020). A break-glass protocol based on ciphertext-
policy attribute-based encryption to access medical
records in the cloud. Annals of Telecommunications,
103–119.
Vidakis, K., Mavrogiorgou, A., Kiourtis, A., & Kyriazis, D.
(2020, June). A Comparative Study of Short-Range
Wireless Communication Technologies for Health
Information Exchange. 2020 International Conference
on Electrical, Communication, and Computer
Engineering (ICECCE).
Wan, S., Zhao, Y., Wang, T., Gu, Z., Abbasi, Q. H., &
Choo, K. K. R. (2019). Multi-dimensional data
indexing and range query processing via Voronoi
diagram for internet of things. Future Generation
Computer Systems, 382–391.
Yang, Y., Zheng, X., Guo, W., Liu, X., & Chang, V. (2019).
Privacy-preserving smart IoT-based healthcare big data
storage and self-adaptive access control system.
Information Sciences, 567–592.
Yao, X., Lin, Y., Liu, Q., & Zhang, J. (2018). Privacy-
Preserving Search Over Encrypted Personal Health
Record In Multi-Source Cloud. IEEE Access, 3809–
3823.
Zewe, A. (2021, September 23). Toward a smarter
electronic health record. MIT News. Retrieved 2021,
from https://news.mit.edu/2021/medknowts-electronic-
health-record-0923
HEALTHINF 2022 - 15th International Conference on Health Informatics
604
