
X-Ray Classification to Detect COVID-19 using Ensemble Model
Ishmam Ahmed Solaiman, Tasnim Islam Sanjana, Samila Sobhan, Tanzila Sultana Maria
and Md. Khalilur Rahman
Department of Computer Science and Engineering, BRAC University, 66 Mohakhali, Dhaka-1212, Bangladesh
Keywords:
COVID-19, Pneumonia, Coronavirus, Deep Learning, X-Rays, Convolutional Neural Network,
Ensemble Model, Transfer Learning, CAD.
Abstract:
Diagnosis with medical images has soared to new heights and play massive roles in assisting radiologists to
detect and analyse medical conditions. Computer-Aided Diagnosis systems are successfully used to detect
tuberculosis, pneumonia, etc. from CXR images. CNNs have been adopted by many studies and achieved
laudable results in the field of medical image diagnosis, having attained state-of-art performance by training on
labeled data. This paper aims to propose an Ensemble model using a combination of deep CNN architectures,
which are Xception, InceptionResnetV2, VGG19, DenseNet-201, and NasNetLarge, using image processing
and artificial intelligence algorithms to quickly and accurately identify COVID-19 and other coronary diseases
from X-Rays to stop the rapid transmission of the virus. We have used classifiers for the Xception model,
VGG19, and InceptionResnet model and compiled a CXR dataset from various open datasets. Since the
dataset lacked 1000 viral pneumonia images , we used image augmentation and focal loss to compensate for
the unbalanced data and to introduce more variation. After implementing the focal loss function, we got better
results. Moreover, we implemented transfer learning using ImageNet weights. Finally, we obtained a training
accuracy of 92% to 94% across all models. Our accuracy of the Ensemble Model was 96.25%.
1 INTRODUCTION
The Novel Coronavirus 2019 (COVID-19) was for-
mulated in Wuhan of the Hubei province of China and
spread drastically all over the world, risking millions
of lives and the world economy. The World Health
Organisation proclaimed the virus as a global pan-
demic on the 11th of March, 2020. The coronavirus
is highly contagious, transmitted through the form of
droplets from an infected person while sneezing or
coughing. It can also be transmitted from touching
contaminated surfaces and then the eyes, mouth, or
nose. Some of the most common symptoms are fever,
dry cough, experiencing breathing difficulties, sore
throat, fatigue and losing the sense of smell and taste.
A COVID-19 patient can carry the virus up to two
weeks from the appearance of any of the symptoms.
There are also many cases surrounding asymptomatic
patients who unknowingly spread the virus, affecting
others. This is why the transmission of the virus is
almost impossible to curb, making it a lethal disease
with a high fatality rate.
1.1 Motivation
With the appalling second wave and the growing
number of cases, timely detection and diagnosis of
COVID-19 are essential and demanding. The real-
time Reverse Transcription Polymerase Chain Reac-
tion (RT-PCR) is the definitive test used for COVID-
19 diagnosis but is not sensitive enough. It is unable
to cater to the increasing number of patients every
day. The process is not only time-consuming but also
prone to error in times of emergencies. The biggest
problem radiologists are facing now is dealing with
false-negative results. Many people are unable to af-
ford to take the test. A modern way to detect diseases
in extreme times and that too in an efficient, prompt
way, must be adapted. An effective method of di-
agnosis with minimum variance is by implementing
deep learning models on medical images. Detecting
abnormalities and diagnosing severe conditions using
medical images have had notable success such as de-
tecting lung cancer and breast cancer in comparison
to traditional analog techniques. Medical images dis-
play essential features such as complicated organ po-
sitions and tissue structure which are imperative for
diagnosis. The development in graphic processing
cards (GPU) hardware and deep learning techniques
allow automatic detection from Chest X-Ray images
Solaiman, I., Sanjana, T., Sobhan, S., Maria, T. and Rahman, M.
X-Ray Classification to Detect COVID-19 using Ensemble Model.
DOI: 10.5220/0010847200003116
In Proceedings of the 14th International Conference on Agents and Artificial Intelligence (ICAART 2022) - Volume 2, pages 375-386
ISBN: 978-989-758-547-0; ISSN: 2184-433X
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
375
with high rates of accuracy. Nevertheless, the use of
X-Rays is not entirely explored to its full potential. In
a developing, disease-prone country like Bangladesh,
with finite medical equipment, the supremacy of dis-
ease detection using medical imaging does not reach
out to the percentage of the population with limited
means. The aggravating ratio of doctors to patients
is 5.26:10000, therefore, providing immediate proper
care is certainly not a privilege. Considering the spike
in daily COVID cases, discrepancies in diagnosis are
also highly unaffordable. Radiological images are
useful in the diagnosis and assessing the after-effects
of COVID-19, for example, pneumonia. As many
patients experience pneumonia as an after-effect, ra-
diological examinations are necessary for follow-up
and to track the recovery process. There are some de-
tection systems available that utilize Chest Computed
Tomography (CT) scans which have outperformed the
RT-PCR test results. But these systems are expen-
sive to install and their routine burdens radiologists,
hence making them vaguely popular in developing
countries. The need to recognize and successfully
interpret COVID-19 features on Chest X-Rays is in-
creasing. X-Rays maintain the good potential to be a
cost-effective approach to the aforementioned issues.
In retrospect, there is a lack of widespread use of X-
Rays based detection systems in diagnosis (Oh et al.,
2020). There are several machine learning and deep
learning techniques designed to identify chest anoma-
lies from X-Rays (Ahmed et al., 2020). Deep learn-
ing is a subset of machine learning and deep learning
techniques are artificial neural networks, processing
data, focusing on automatic feature extraction and im-
age classification. The biggest hurdle researchers face
with developing deep learning-based diagnoses is that
there are very limited open and available COVID-19
datasets. The ever-changing structure of the virus,
coupled with the increasing number of patients makes
it difficult to collect data.
1.2 Research Objective
Our work is based on relatively more Covid-19 data
than any other papers, elaborated in the Dataset seg-
ment. Furthermore, we have trained our models us-
ing transfer learning, a process by which the knowl-
edge of a network, pre-trained initially with data,
used to perform a differently related task, using fresh
data (Apostolopoulos and Mpesiana, 2020). Transfer
learning has proven to enhance performance in a time-
effective manner (Joseph, 2020). It also produces bet-
ter results when the size of the dataset is small(Joseph,
2020), as in the case of COVID-19 datasets, since the
disease is still fresh and the volume of data is low.
We used image augmentation techniques to compen-
sate for this by providing random augmentation of the
images as they are fed into the models for training.
This greatly improves the variation of training im-
ages lowering the potential for over-fitting the dataset.
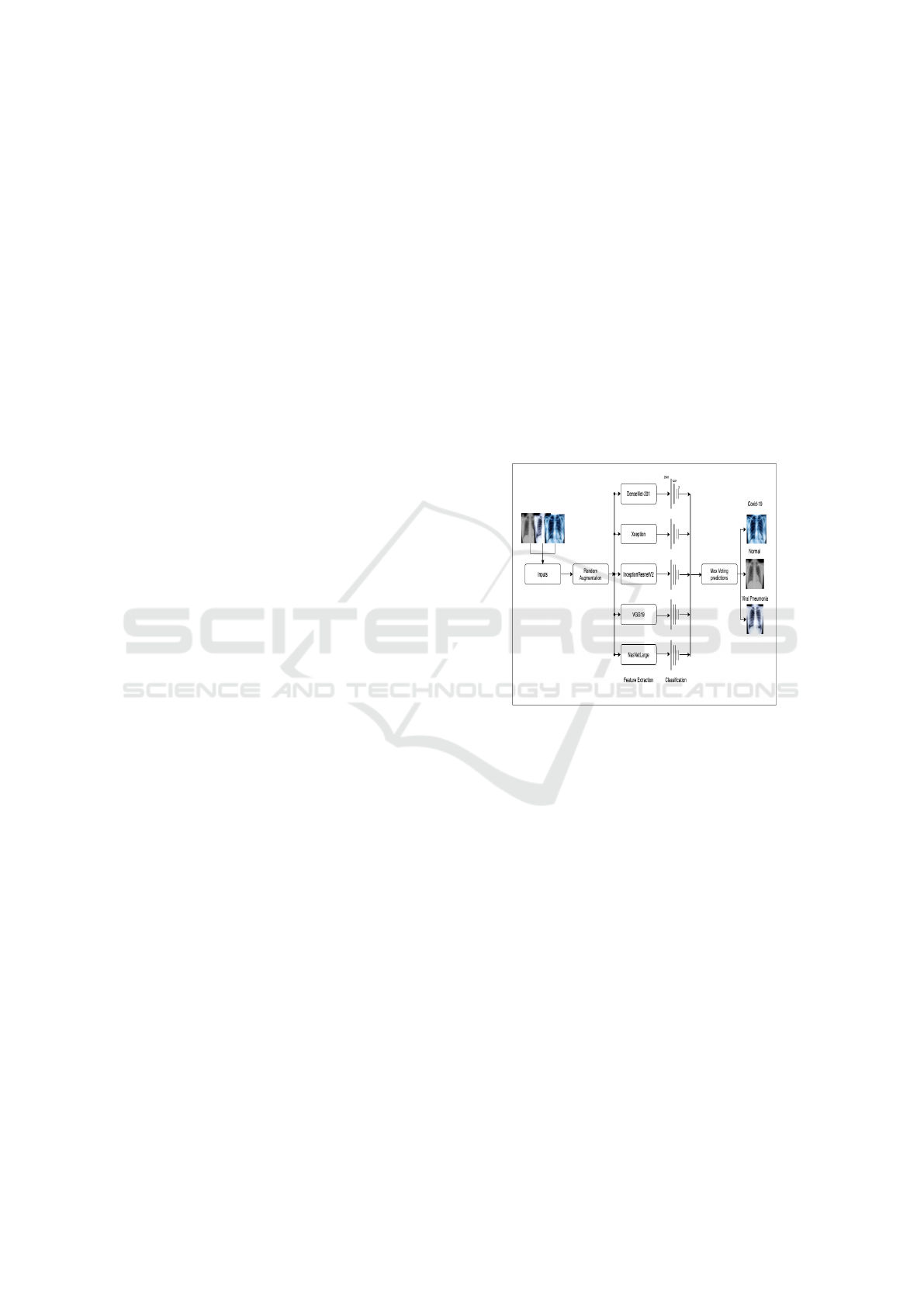
We used 5 different feature extraction networks with
a custom classification network to produce 5 X-ray
classification models. We used a fully connected 2048
dense layer with a 10% dropout rate followed by a
1024 unit dense layer with a 20% dropout rate, both
having a Relu activation function as shown in “Fig-
ure: 1”. Finally, the output layer is a 3 unit dense layer
with a softmax activation function for the classifica-
tion network. Along with that, we also used a Grad-
CAM (Gradient-weighted Class Activation Mapping)
to show the heatmap of the infections in the Chest X-
ray images.
Figure 1: Model Overview.
2 LITERATURE REVIEW
A Convolutional Neural Network (CNN) is a type of
deep neural network, widely used in the field of im-
age and signal processing, classification & image seg-
mentation. There have been numerous studies that
prove detection and diagnosis implementing CNNs
are quicker and successful, especially in detecting
pneumonia, tuberculosis, and lung cancer (Sethi et al.,
2020) (Bhagat and Bhaumik, 2019)(Stirenko et al.,
2018) (Tataru et al., 2017). CNNs have made ground-
breaking results in visualization tasks and CAD.
CADs help with the initial screening of images and
attempt to reduce the load on radiologists. While
the CT scan provides accurate diagnosis, X-Rays are
more favored as they are comparatively inexpensive
and easier to comprehend, with ample, scalable appli-
cations and extensively used in diagnosis and moni-
toring diseases. Datasets available on the public do-
main containing labeled images allowed researchers
ICAART 2022 - 14th International Conference on Agents and Artificial Intelligence
376

to apply deep learning algorithms for segmentation
purposes, anatomical structure detection, detection of
suspicious region anomalies and CAD. Prior research
includes thoracic disease identification and localiza-
tion, lung regional segmentation and disease report
generation. X-Rays portray crucial features such as
textures and tissue structures which yield fruitful re-
sults in diagnosing lung diseases. CNN is used to
extract a feature map out of images and the corre-
sponding branch structure. Wang et al. (Wang et al.,
2019) connect X-Rays and segmentation based on
deep learning to detect lesions. An instance segmen-
tation algorithm is applied to segment and label the
clavicles and ribs automatically. 180 CXRs were ran-
domly selected with the assistance of digital radio-
graphy machine. The basic network framework of
Mask R-CNN, an improved structure of the Faster
R CNN, for automatic segmentation and annotation
method was implemented. The feature map is ex-
tracted by the basic network, followed by the candi-
date regions being screened by RPN. Lastly, the seg-
mentation, classification, and mask tasks of image tar-
gets are completed by 3 branch structures. Contrary
to manual labeling, automatic labeling has great sig-
nificance for the auxiliary diagnosis and treatment of
computers. This paper is the first to propose an in-
stance segmentation algorithm that solves the prob-
lem of automatic segmentation annotation in med-
ical images. In (Tataru et al., 2017), the experi-
ment was carried out on a vast dataset, implement-
ing basic augmentation techniques to prevent overfit-
ting. GoogleNet, Inception V3, and ResidualNet ar-
chitectures were implemented. GoogleNet achieves
significant, random classification accuracy when la-
beling normal and abnormal. The results conveyed
that further fine-tuning architectures carry the poten-
tial to increase model performance but would not al-
ter the robust results significantly. Symmetry appears
to be a salient feature of normal CXR images de-
tected by the model. Although this model is not yet
ready for clinical adoption, it promises a future func-
tional classification network. The authors in (Ahmed
et al., 2020) propose an automatic COVID-19 clas-
sification model, where they have used both COVID
and non-COVID-19 images and implemented HRNet
for feature extraction purposes. Initially, the model
was trained for 25 epochs for each fold, with a 0.005
learning rate and a customized dice coefficient loss
function. The size of the input image was 512×512
pixels and was grayscale. The results surpass exist-
ing models in terms of accuracy, specificity, sensitiv-
ity, and other evaluation metrics. HRNet avoids the
loss of small target information in the feature map
since the convolutions are parallelly connected and
also for the high-resolution feature representation. A
segmented COVID dataset consisting of 910 images
was used for training purposes with ten-fold cross-
validation. By implementing the K-fold algorithm, 1
fold was used for testing while the remaining 9 folds
were used for training. The pre-trained Vgg16 and
ResNet-101 CNNs were compared with each other
to analyze lung images. Images were classified into
normal and abnormal, and achieved a 82% success
rate. Since the performance was relatively low, a
different approach was implemented to measure ac-
curacy. If the classification result was in the top
3 decisions determined by the network, the process
was considered successful with a 90% success rate.
Smaller network structures that provide higher per-
formances for Chest X-ray chest classification were
thus investigated. This model succeeded in detect-
ing diseases using only the X-ray image without any
prior knowledge about the patient’s history. Three
CNNs were examined comparatively increasing the
number of layers. The size of the input images was
reduced, sacrificing performance in order to reduce
the training time (Kesim et al., 2019). Transfer learn-
ing empowers a deep learning model to adequately
learn from a small dataset by transferring learned fea-
tures from another deep learning model that recently
learned from a similar, but larger sized dataset. An
automatic deep learning-based method using X-rays
to predict COVID-19 was proposed by Narin et al in
(2020)(El Asnaoui and Chawki, 2020). The method
used 3 CNNs and a dataset that consisted of 50 X-ray
images of COVID-19 patients and 50 normal X-ray
images and all the images were resized to 224×224.To
overcome the issue of the predetermined number of
dataset, the authors utilized transfer learning models.
The dataset was divided into two parts: 80% for train-
ing and 20% for testing. The developed deep CNN
was based on pre-trained models (ResNet50, Incep-
tionV3, and InceptionResNetV2) and allowed the au-
thors to differentiate COVID-19 from normal X-ray
images. Transfer learning with the K-fold method
was used as a cross-validation method with a k 1⁄4
(Apostolopoulos and Mpesiana, 2020). The final re-
sults showed a convincing accuracy of 96.78%. In
(Pardamean et al., 2018) the authors strive to con-
figure transfer learning from CheXNet to assimilate
mammogram data. Their findings show the best con-
figuration only employs the first two dense blocks
from the original CheXNet model. The optimal num-
ber of layers in the last used block is also fewer than
compared to the original model, i.e. 6 layers out of
12. A better procedure to search for hyperparameter,
for instance, grid search and random search might be
able to discover a more ideal configuration as opposed
X-Ray Classification to Detect COVID-19 using Ensemble Model
377

to the trial-and-error approach that is employed in this
research. InceptionV3 is a state-of-the-art model that
is pre-trained and is used for transfer learning in this
research (Gordienko et al., 2018). This research anal-
ysis contributes notably with regards to GAN based
synthetic data and 4 different types of deep learn-
ing based models which brought forth state-of-the-art
comparable results (Albahli, 2020). InceptionV3 is
used as transfer learning is because of the lower er-
ror rate. The authors discussed how coronavirus can
be the real trigger to open the course for rapid inte-
gration and installation of Deep Learning in hospitals
and medical centers. They review the improvement of
deep learning applications in medical image analysis,
focusing on pulmonary imaging and giving insights
into contributions to COVID-19. [22] Apostolopou-
los and Mpesiana in (Apostolopoulos and Mpesiana,
2020) evaluated various state-of-the-art deep architec-
tures on CXR images. VGG19 managed to achieve
an accuracy of 98.75% and 93.48% for 2-class and 3-
class classification functions respectively, thus prov-
ing to be the best model. U-nets and Mask RCNNs
are used for segmentation tasks to label each pixel
of images and are also widely used in medical im-
age classification. However, obtaining successful re-
sults are often hindered since Computer Aided De-
signs (CADs) have stunt development courtesy of the
overwhelming absence of labeled data and immense
variations in chest X-Rays (Tataru et al., 2017). More-
over, segmentation plays a crucial role in training a
model by getting rid of redundant data on the avail-
able image dataset in order for the model to converge
on the infected areas. But it has been overlooked in
several previous research. Therefore UNet has been
tried and tested for segmentation purposes in (Ahmed
et al., 2020), where they used High-Resolution Net-
work (HRNet) for feature extraction embedding and
the UNet for segmentation purposes. In (Wiysobunri
et al., 2020) the authors talk about the importance
of diagnosis with Chest X Rays since the virus has
also proven to transmit through asymptomatic pa-
tients. They discuss the ease of image diagnosis with
the existence of state-of-the-art AI algorithms and ac-
cess to huge data. These models can bridge the gap
between diagnosis and result delivery time to sim-
ply minutes. The authors suggest that depending
on one model can be restrictive since every model
has a different method for extracting features from
training samples. Thus keeping in mind the urgent
need for correct diagnosis, they suggest an ensemble
model comprising 5 state-of-the-art deep CNN mod-
els: VGG19, DenseNet201, ResNet50, ResNet34,
and MobilNetV2, to automatically detect COVID-19
in X-Rays. The authors plan to increase the prediction
accuracy of COVID-19, while attempting to lower
the percentage of error and increase robustness by
putting together all the strengths of the existing mod-
els, using X-ray images collected from Kaggle web-
sites and Github repositories. Their model consists
of 2 main techniques: transfer learning and ensem-
bling to be able to architect a robust detection model.
The images were divided for training and validation
in the ratio of 80:20. By applying the max voting
system their ensemble model results attained a per-
formance accuracy of 99%. The authors are confident
that their versatile model has the potential to expand
to detecting other chest-related diseases, for example,
tuberculosis. Following the circumstances surround-
ing restricted medical image datasets and motivated
by the success of deep learning and image processing,
the present work is going to apply transfer learning
techniques that were pre-trained by ImageNet data to
overcome lengthy training time and insufficient data.
Transfer learning also plays a vital role in upgrading
the accuracy of detection.
3 DATASET
3.1 Data Description
The cardinal element in deep learning is data. For
this experiment, we have accumulated radiography
images from several public repositories and clas-
sified the images as - Viral Pneumonia, Normal
and Covid-19. From the dataset by Tawsifur Rah-
man (COVID-19 Radiography Database) (Chowd-
hury et al., 2020)(Rahman et al., 2021) we acquired
3616 COVID-19 images, 10192 Normal images from
which we examine 3620 and 1345 Pneumonia im-
ages. The Chexpert dataset is a large compilation
of 224,316 chest X-Ray images of 65,240 patients
from Stanford University Medical Centre (CheXpert:
A Large Chest Radiograph Dataset with Uncertainty
Labels and Expert Comparison) (Irvin et al., 2019).
We have taken 566 Pneumonia cases from this dataset
for our research. 176 Pneumonia images were taken
from The National Institutes of Health Clinical Cen-
tre Chest X-Rays dataset which is the most popu-
lar dataset used in the field of medical imaging re-
search and diagnosis. It is the largest available in the
public domain containing radiographies of many ad-
vanced cases of diseases (NIH Chest X-rays) (Wang
et al., 2017). As COVID-19 is a fairly new disease
even though there were previous cases of coronavirus
diseases namely SARS in 2002-2003 and MERS in
2012, datasets are very hard to access from hospi-
tals. Thus, we had to solely rely on publicly available
ICAART 2022 - 14th International Conference on Agents and Artificial Intelligence
378
datasets for the course of our experiment. Other dis-
eases and multiclass labels, for example, images con-
taining both pneumonia and some other disease, were
eliminated from the NIHCC and Chexpert dataset, fo-
cusing only on the aforementioned classes. All the
images were read as RGB. Posteroanterior viewing
images were only selected to maintain uniformity. Af-
ter compilation and creation of our dataset, we ran-
domly split 80% of the dataset for training and test-
ing the remaining 20% for validation purposes. The
resulting dataset was further split into train and test
sets, maintaining a ratio of 80:20 once again. The
training set contained 2492 Covid, 1675 Pneumonia,
and 2496 normal images whereas the testing set con-
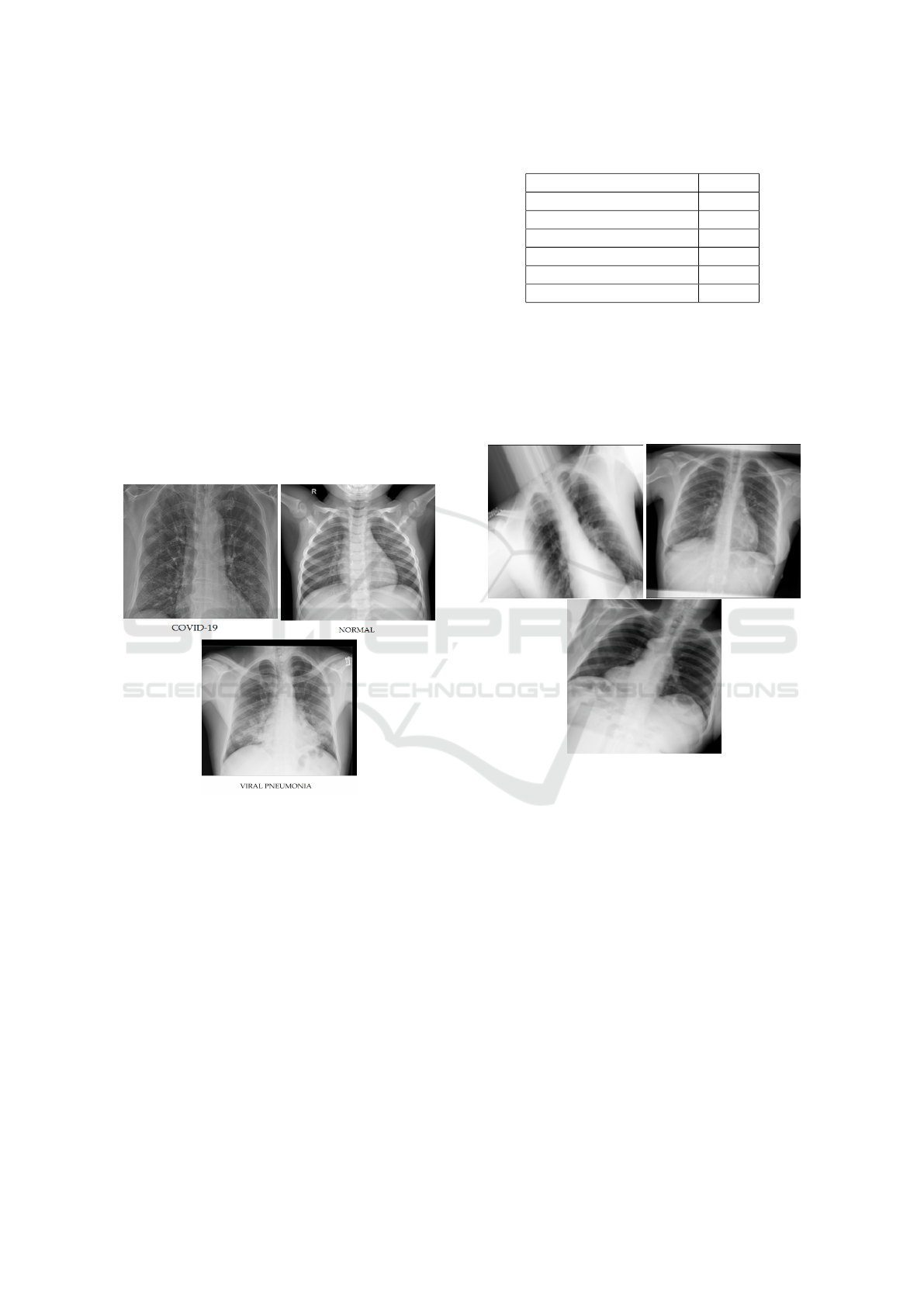
tained 400 images of each class. Some of the Chest
X-Ray Images of COVID-19, Viral Pneumonia, and
Normal Patients from our dataset are demonstrated in
“Figure: 2”.
Figure 2: Sample Chest X-Ray Images of COVID-19, Viral
Pneumonia and Normal Patients.
3.2 Data Augmentation
We used ImageDataGenerator from TensorFlow
which allows us to perform image augmentation
while the data is being fed into the models each epoch.
The images were resized to 299 x 299 pixels and
augmented over a range of parameters. All the im-
ages are normalized and then a random combination
and range of augmentation are applied to each im-
age. This process occurs every epoch producing var-
ied training data each epoch with random augmenta-
tion each time. The primary reason to augment our
dataset is to increase the size of the dataset, prevent
overfitting and add variation. The images were fur-
ther tuned as shown in “Table: 1”:-
Table 1: Data Augmentation.
Random Augmentation Range
Rotation range 0 - 30
Width Shift Range 0 - 0.2
Shear Range 0 - 0.2
Height Shift Range 0 - 0.2
Zoom Range 0 - 0.2
Channel Shift Range 0 - 0.1
For every epoch that’s training, a new image was
augmented. For example, each image was rotated
a number of times. Even though our dataset was
limited, data augmentation allowed us to get reliable
training without overfitting. “Figure: 3” shows the
state of the images after augmentation.
Figure 3: CXR Images after Augmentation.
4 METHODOLOGY
For the course of this experiment, we have imple-
mented 5 CNN architectures for feature extraction-
InceptionResnetV2, Densenet201, VGG19, NasNet-
Large and Xception. The last layers of all the afore-
mentioned models were removed before our experi-
ment, keeping only the convolutional layers and pool-
ing layers. The structure of our model comprises of
the CNN architectures followed by a global average
pooling layer then advances towards a dense layer
with 2048 neurons using ReLu activation function and
a 10% random dropout rate. Following that is struc-
tured another dense layer comprising 1024 neurons,
Relu activation function in addition and a dropout of
20%. Lastly, there is a dense layer consisting of 3 neu-
rons for the output class with Softmax activation. A
X-Ray Classification to Detect COVID-19 using Ensemble Model
379
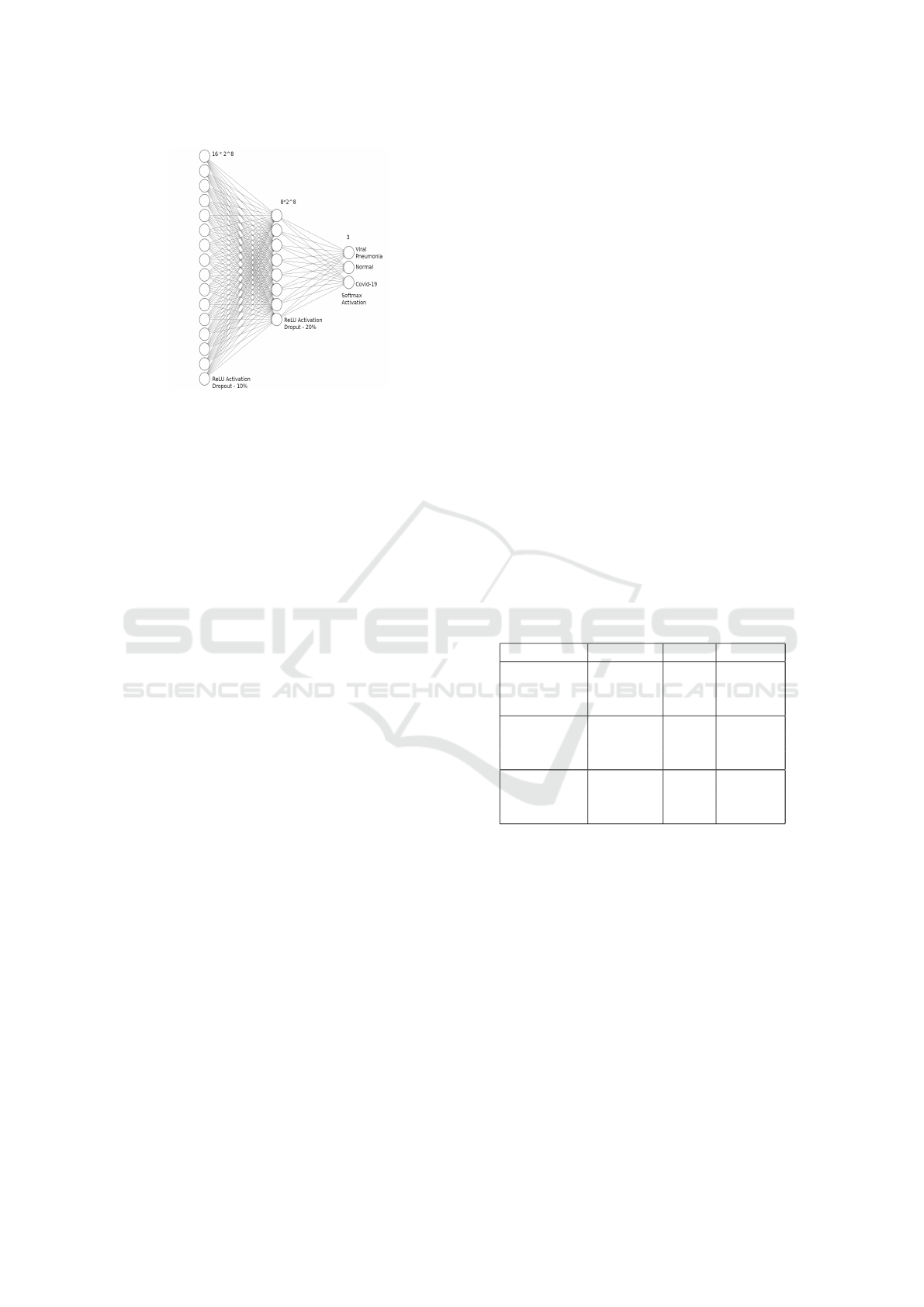
Figure 4: Architecture of the Classification Network.
detailed overview of our classification model is shown
in “Figure: 4” .
In (Khan et al., 2020), the Coronet architecture
is based on Xception with a dropout layer and 2
fully connected layers at the end. This study accom-
plished an overall accuracy of 89.6% for 4 classes
(Viral Pneumonia, Bacterial Pneumonia, COVID-19
and Normal) while we reached an accuracy as high
as 92.53% when we implemented the same architec-
ture. For a ternary classification among COVID-19,
Pneumonia and Normal, much likely to our approach,
Coronet yielded an accuracy of 95%. On the brighter
side, when we implemented Xception with our exist-
ing architecture we were able to produce an accuracy
of 93.67%. The adversity we faced were that the im-
ages were not generalised in the right manner as there
was an excessive number of cases of False Positive
and False Negative. However, with the addition of the
layer with 2048 neurons as depicted in the model ar-
chitecture, the dataset was better graphed and classi-
fied, with a lower number of False Positives and False
Negatives. There were some oscillations in the re-
sults due to every epoch creating a newly augmented
image, causing fluctuations.
4.1 Proposed Model
Compared to other approaches, we present an ensem-
ble deep learning method that will aid to improve
deep learning prediction accuracies of COVID-19 and
decrease the error-rate of misclassification by com-
bining 5 different models. These models include: In-
ceptionResNetV2, VGG19, NasNetLarge, Xception,
and DenseNet201. Shifting from a single model, this
approach allows the production of a better predic-
tive performance model.A detailed explanation of the
models is mentioned below. For Xception, VGG19,
Densenet and InceptionResnetV2 models, adam opti-
mizer and focal loss function were used. However, for
Nasnet, the focal loss function did not show promis-
ing results. Therefore we switched to adamax opti-
mizer replacing Adam optimizer to see if it worked.
After showing unsatisfactory results, we switched to
categorical cross-entropy loss function alongside the
adamax optimizer.The Focal Loss and the Categorical
Crossentropy Functions are defined as:
FL(p
t
) = −α
t
(1 − p
t
)
γ
log(p
t
) (1)
CL = −
out putsize
∑
i=1
y
i
· log(
b
y
i
) (2)
All the models were initialized with imagenet train-
ing weights and were trained for 70 epochs where
the test report was recorded at the 25th, 50th and the
70th epoch measuring precision, recall and F1-score
along with accuracy and loss. For the first 50 epochs
the weights for the feature extraction network of each
model was frozen during training. After 50 epochs all
the layers except batch normalization were unfrozen
and trained a further 20 epochs. It can be observed
that the accuracy has upgraded as more epochs were
run.
4.1.1 InceptionResnetV2
Table 2: InceptionResnetV2 after 25, 50, 70 epochs.
precision recall f1-score
COVID-19 0.96 0.79 0.87
Normal 0.75 0.96 0.84
Pneumonia 0.97 0.87 0.91
COVID-19 0.96 0.90 0.93
Normal 0.86 0.96 0.91
Pneumonia 0.98 0.93 0.95
COVID-19 0.95 0.93 0.94
Normal 0.89 0.94 0.92
Pneumonia 0.98 0.94 0.96
InceptionResNetV2 is a CNN architecture trained
on more than a million images from the ImageNet
database. It delivers good performance at a com-
paratively low computation cost. This difference in-
dicates that the batch-normalization concept is used
only on top of the traditional layer and not above the
residual summations(Hira et al., 2021). InceptionRes-
NetV2 is naturally 164 layers deep and after adding
the 3 layers in our approach it is at 167 layers. The
model consists of a total of 55,919,843 parameters
of which 1,580,035 are trainable and 54,339,808 are
nontrainable. During the first 25 epochs, the training
and loss accuracy rested at 0.8837 and 2.1172 respec-
tively. Following running the model for 50 epochs it
exhibited a training accuracy of 0.9233 and a train-
ing loss of 1.7106. After unfreezing the layers, the
ICAART 2022 - 14th International Conference on Agents and Artificial Intelligence
380
nontrainable parameters were made active and a total
of 55,919,843 parameters were trained for 70 epochs.
The InceptionResnetV2 model achieved a training ac-
curacy of 94.98% and testing accuracy of 92.75%.
4.1.2 DenseNet201
Table 3: DenseNet201 after 25, 50, 70 epochs.
precision recall f1-score
COVID-19 0.95 0.94 0.95
Normal 0.88 0.95 0.91
Pneumonia 0.98 0.92 0.95
COVID-19 0.97 0.94 0.95
Normal 0.89 0.96 0.92
Pneumonia 0.97 0.93 0.95
COVID-19 0.95 0.95 0.95
Normal 0.91 0.94 0.93
Pneumonia 0.97 0.93 0.95
In DenseNet, proposed by Gao Huang et al
(Huang et al., 2017) and 201 layers deep, each layer
inherits additional inputs from all preceding layers
and passes on its own feature-maps to all succeeding
layers. It has 2 characteristics: simplicity in the train-
ing process and exceptionally, parametrically efficient
models, due to the potential of feature reuse by vari-
ous layers. This intensifies the chances of variation in
the subsequent layer inputs. Densenet201 portrays the
best results in terms of accuracy, precision and espe-
cially in F1-score compared with the rest of the mod-
els. The model achieved a training accuracy of 0.9574
after 25 epochs and increased to 0.9760 following an-
other 25 epochs. DenseNet consists of 20,299,843
parameters of which 1,974,019 were trainable. Un-
freezing and training for a total of 70 epochs,the re-
maining 18,325,824 parameters were activated and
the DenseNet model achieved a training accuracy of
96.53% and testing accuracy of 94.83% after training
on 20,299,843 in total.
4.1.3 NasnetLarge
Table 4: NasNetLarge after 25, 50, 70 epochs.
precision recall f1-score
COVID-19 0.94 0.87 0.90
Normal 0.82 0.94 0.87
Pneumonia 0.97 0.90 0.93
COVID-19 0.97 0.93 0.95
Normal 0.89 0.96 0.92
Pneumonia 0.97 0.94 0.96
COVID-19 0.95 0.93 0.94
Normal 0.89 0.94 0.91
Pneumonia 0.96 0.93 0.95
NasNet, which is Neural Architectural Search
(NAS) Network, was manufactured by the Google
ML team. It’s architecture depends on reinforcement
learning. NASNetLarge has been trained on over a
million images from the Imagenet database and has
the capability to classify images into 1000 class cate-
gories. NASNet-Large consists of 89,065,813 param-
eters, 4,140,931 trainable and 84,924,882 nontrain-
able. It is a CNN architecture with an image input size
of 331 x 331. The parts of the architecture incorporate
a Controller Recurrent Neural Network (CRNN) and
a CNN block. NASNet includes two sorts of cells: A
normal cell that returns a feature map of the same di-
mension and reduced cell that returns a feature map
where the height and width of the said feature map
is reduced by a factor. We also implemented Cate-
gorical loss for NasNet instead of focal loss. And
instead of using Adam optimizer as an optimizer,
we used Adamax. After the first 25 epochs, normal
class accuracy was a little less; the training accuracy
amounted to 0.9222 and training loss of 0.2049. After
50 epochs, training accuracy improved to 0.9457 and
loss fell to 0.1492 with improvement of f1-score of
all classes being above 92%. At 70 epochs, after ac-
tivating the nontrainable parameters and running on
89,065,813, the model achieved a training accuracy
of 95.11% and a testing accuracy of 94.42%.
4.1.4 Xception
Table 5: Xception after 25, 50, 70 epochs.
precision recall f1-score
COVID-19 0.92 0.90 0.91
Normal 0.84 0.90 0.87
Pneumonia 0.95 0.91 0.93
COVID-19 0.95 0.92 0.93
Normal 0.86 0.96 0.91
Pneumonia 0.99 0.91 0.95
COVID-19 0.96 0.91 0.93
Normal 0.88 0.94 0.91
Pneumonia 0.96 0.94 0.95
The Xception is a CNN architecture with 71 lay-
ers and is an extension of the Inception model pro-
posed by Francois Chollet in (Chollet, 2017). Xcep-
tion is known to outperform Inception v3 on the Im-
ageNet dataset.This architecture reestablishes the in-
ception module with depthwise separable convolu-
tions operations, in which the convolutions are not
only in a depthwise manner but also as a pointwise
one. It has 22,970,923 parameters in total, among
which 2,105,347 were trainable and consists of depth-
wise convolution layers which are independent in-
stead of the conventional convolution layers. It takes
X-Ray Classification to Detect COVID-19 using Ensemble Model
381
into account the mapping of spatial correlations and
cross-channel correlations which can be decoupled in
CNN feature maps in their entirety. Another approach
to utilize a pre-trained model is to train not only a new
classifier but also fine-tune higher convolutional lay-
ers of the pre-trained model that are responsible for
significant feature extraction. For the first 25 epochs,
the model was successful in achieving 0.9084 training
accuracy and 1.6731 training loss.The model was ini-
tialized with Imagenet training weights. The accuracy
improved to 0.9409 after the second 25 epochs. Non-
trainable 20,865,576 parameters were made trainable
and a training accuracy of 94.92% was obtained and
93.67% accuracy on testing at 70 epochs.
4.1.5 VGG19
VGG19 is a CNN architecture that is a descen-
dant of VGG-16 with 19 weight layers (16 convolu-
tional and 3 dense) and is used as a pre-processing
model.Compared with traditional CNNs, it has been
improved in network depth. It utilizes a substituting
structure of different convolutional layers and non-
linear activation layers. VGG19 has 20,554,819 pa-
rameters which includes 529,411 trainable parame-
ters.Hence, the network has learned rich feature rep-
resentations for a wide range of images.The training
accuracy and loss accuracy is 0.8906 and 1.9317 re-
spectively after 25 epochs and 0.9220 and 1.4485 af-
ter 50 epochs. After unfreezing the layers, activat-
ing the remaining 20,025,408 parameters and training
for 70 epochs, the VGG19 model achieved a training
accuracy of 92.73% and testing accuracy of 91.92%.
Even though VGG19 takes time to learn, they are uti-
lized in image classifications because of their good
accuracy results.
Table 6: VGG19 after 25, 50, 70 epochs.
precision recall f1-score
COVID-19 0.90 0.92 0.91
Normal 0.86 0.92 0.89
Pneumonia 0.96 0.88 0.92
COVID-19 0.91 0.95 0.93
Normal 0.90 0.92 0.91
Pneumonia 0.98 0.93 0.95
COVID-19 0.90 0.92 0.91
Normal 0.87 0.92 0.89
Pneumonia 0.98 0.91 0.94
4.2 Transfer Learning
In our experiment, we also implemented transfer
learning on these models using ImageNet weights.
Transfer learning is a widespread Machine Learn-
ing technique which presumes utilizing an prevail-
ing, trained Neural Network, that has been engineered
for one task, as the core foundation for another task.
Transfer learning is favoured as it removes the neces-
sity of training vast amounts of data for completing a
task since the basic features required to train a model
are imported from previously accomplished analyses.
The most prominent challenge associated with trans-
fer learning is to retain the existing knowledge in the
model while adapting the model to new tasks as it
leads to the problem of the number of layers or param-
eters required to be re-trained to achieve optimal re-
sults. The primary steps of transfer learning involves
finding the sustainable pre-trained model, secondly,
replacing the ultimate layer of the model consistent
with the amount of output layers for the upcoming
task and eventually, resume training the model with
fresh data and fine-tuning the model till the accu-
racy converges towards a higher and acceptable value.
To begin with, the models were initialised with pre-
trained Imagenet weights. For the first 50 epochs, we
froze the feature extraction layers of the model mean-
ing that the trainable weights will not be updated. We
kept the batch normalization layer on inference mode
and trained the classifier. During inference mode, the
layer normalizes the current batch using a moving av-
erage of the mean and standard deviation, rather than
using the mean and variance of the current batch. The
moving mean and moving variance are nontrainable
variables that are updated each time the layer is called
in training mode. For the next 20 epochs, we unfroze
the feature extraction layers allowing the weights to
be updated and fine tuned the upper convolutional lay-
ers. The batch normalization layer was switched to
training mode during which the layer normalizes the
current batch using the mean and variance of the cur-
rent batch of inputs.
4.3 Ensembling
There are several ways to perform ensembling on the
trained model. The methods include linear averag-
ing, bagging, boosting, max voting etc.The Ensem-
ble model has two types of averaging results from the
base learners - Linear average and Weighted average.
We implemented Ensembling of models which is a
standard approach in Applied Machine Learning to
make sure that the foremost stable and absolute best
prediction is formed. Generally, ensemble learning
involves training quite one network on an equivalent
dataset, then using each of the trained models to form
a prediction before combining the predictions in some
way to configure a final outcome or prediction. After
ICAART 2022 - 14th International Conference on Agents and Artificial Intelligence
382
taking into account all the test predictions of the 5
models used, we implemented a max voting system
and a linear averaging system. A max voting system
is where each of the multiple models used will pre-
dict and vote for a particular class. The image will be
then classified as the class with the maximum num-
ber of votes since most of the models predicted the
image as that corresponding class. Linear averaging
was achieved by taking the average of the possibili-
ties predicted by the individual models. Comparing
between max voting and averaging, max voting gave
better results. Results show that the f1 score for all
the 3 classes are all good, especially for COVID-19
which has the highest f1 score.
5 RESULTS
The performance of each model was evaluated based
on the precision, recall and f-1 score metrics, as
shown in the previous section. The training and test-
ing accuracy can be seen in “Table: 7”.
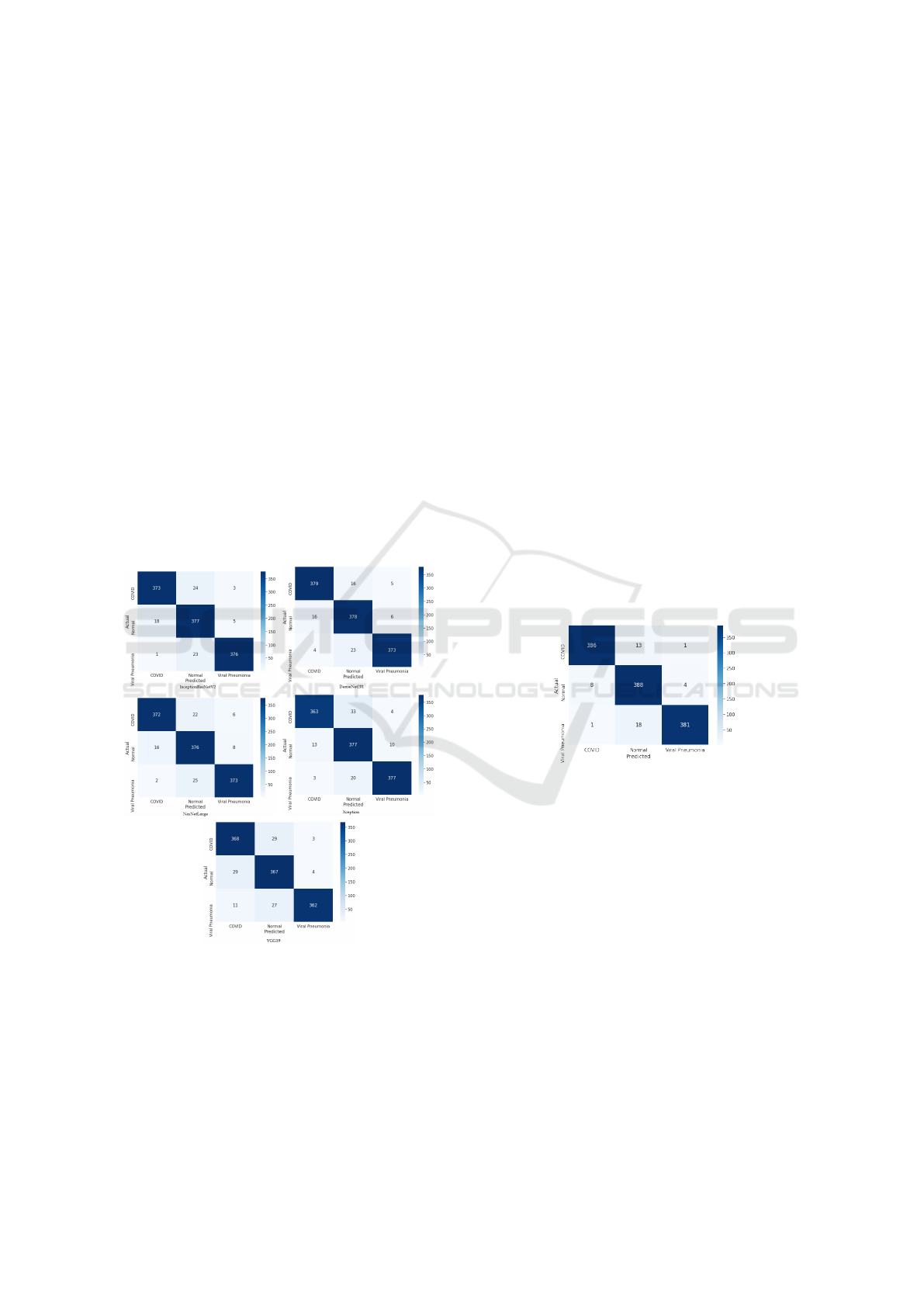
Figure 5: Confusion Matrices after 70 Epochs.
From the confusion matrices of the 5 classification
models after a total of 70 epochs in “Figure: 5, we can
observe that DenseNet201 has identified 379 COVID
images correctly and identified 16 as Normal cases
and 5 as Pneumonia. Densenet also classified 378
Normal classes and 373 Viral Pneumonia correctly.
On the other hand, InceptionResNetV2 classified 376
Viral Pneumonia cases without fail, which is an incre-
ment compared to DenseNet201, while the detection
of other classes fall a little behind. VGG19 and Nas-
NetLarge have performed similarly to DenseNet and
InceptionResNetV2, however, NasNetLarge detected
22 COVID images as Normal and 25 Viral Pneumo-
nia images wrongly as Normal. VGG19 detected
368 COVID, 367 Normal and 362 Pneumonia im-
ages correctly, mistaking 29 COVID images as Nor-
mal. Lastly, the Xception model has identified 377
images correctly in both the Normal and Viral Pneu-
monia classes, with 363 correctly identified COVID-
19 images and falling a little back with identifying
33 COVID images as Normal images. Therefore we
can conclude that DenseNet201 has out-performed all
the other classifiers in terms of both correct class de-
tection and f-1 scores for all the classes: 0.95 for
COVID, 0.93 for Normal cases and 0.95 for Viral
Pneumonia. Also, we have observed that all of the
models have the lowest f1-score for Normal images
among the 3 disease classes. Low image quality and
not enough pre-processing might have affected the re-
sults.
5.1 Max Voting and Ensemble Linear
Average
Figure 6: Max Voting Results.
Max voting is a very commonly used classification
scheme where the predictions from the classification
models are votes and the majority of the votes are con-
sidered as the final prediction. Max Voting identified
386 COVID images accurately and identified only 1
image wrongly as Pneumonia, which is by far the
best and most accurate. Furthermore it has been suc-
cessful in predicting 388 Normal images and 381 Vi-
ral Pneumonia images without fail and only mistook
one Pneumonia image for a COVID case. The over-
all performance of the max voting system was out-
standing, attaining an accuracy of 96.25%. The f-1
scores for COVID-19, Normal and Viral Pneumonia
classes were also very high at 97%, 95% and 97% re-
spectively. Alongside max voting, we implemented
Ensemble Linear Averaging for final prediction, com-
prising the prediction from all 5 of our models to com-
pare with Max Voting results. The accuracy of linear
X-Ray Classification to Detect COVID-19 using Ensemble Model
383
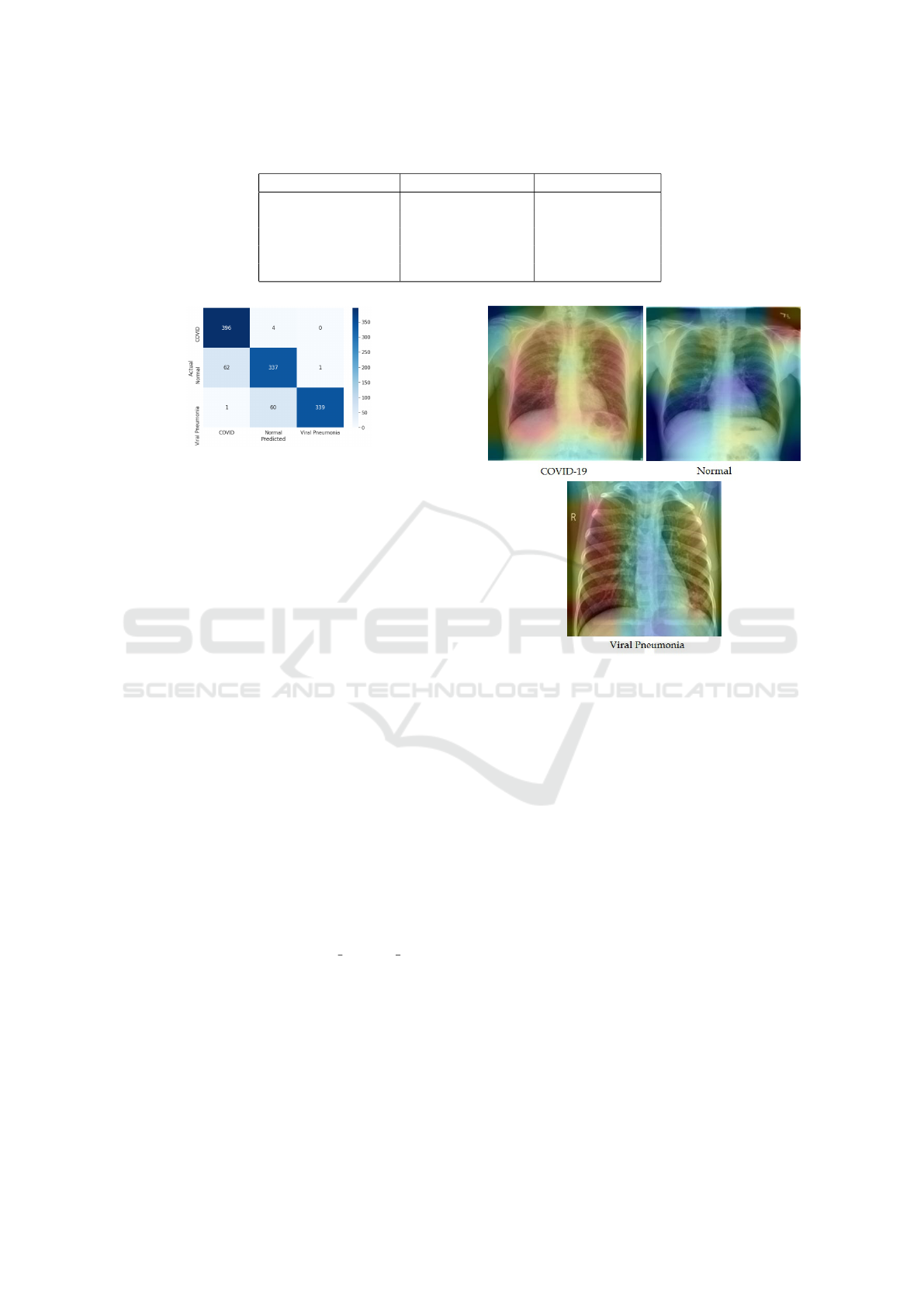
Table 7: Final Accuracy after 70 Epochs.
Models Training Accuracy Testing Accuracy
InceptionResNetV2 94.98% 92.75%
DenseNet201 96.53% 94.83%
NasNetLarge 95.11% 94.42%
Xception 94.92% 93.67%
VGG19 92.73% 91.92%
Figure 7: Ensemble Linear Averaging.
average is at 89.33%, with f-1 score of COVID-19,
Normal and Pneumonia at 92%, 84% and 92% respec-
tively, making Max Voting results a clear winner.
5.2 GradDCAM Results
In order to find out about the COVID-19 detection
transparency, we have used Gradient Class Activation
Map (Grad-CAM) based color visualization approach
for identifying the regions where the model paid more
attention during the classification. The procedure of
Grad-CAM provides a visual interpretation for any
deeply related neural network and aids with verify-
ing where the model is looking at while predicting. It
also allows us to verify whether the model is activat-
ing at the correct locations and how well is it actually
performing. We have implemented Grad-CAM using
Keras and Tensorflow. DenseNet was selected as the
model to be used with Grad-CAM because it has the
highest average precision, recall and f1-score among
the other models and we expected it to give the best
results for activation maps as well. Grad-CAM works
by taking an image as an input and computes a heat-
map by examining the gradient information flowing
into the last Convolutional layer or a specific layer of
the model. We have selected Conv5 Block32 Concat
layer of the DenseNet model to visualize heat-maps.
“Figure: 8” demonstrates some sample GradCAM im-
ages below.
Figure 8: Confusion Matrices after 70 Epochs.
6 DISCUSSIONS
6.1 Performance Comparison
While in (Wiysobunri et al., 2020) the authors opt
out for binary classification (COVID-19 and Non-
COVID-19) and achieved a performance accuracy of
99%, our model is a ternary classification, classify-
ing among Viral Pneumonia, COVID-19 and Normal
cases and we achieved an accuracy of 96.25%. Our
experiment is different from their approach in terms
of the number of classes and the classifiers, wherein
they implemented VGG19, ResNet34, ResNet50,
MobileNetV2 and DenseNet201. A deep CNN based
solution using Ensemble learning modelled by the
authors in (Das et al., 2021) to perform a binary
classification between COVID-19 and Non-COVID
cases had 538 images of COVID positive patients and
468 of negative patients. Three pre-trained models-
DenseNet, ResNet50V2 and InceptionV3 were ap-
plied. Their approach showed an overall classifica-
tion accuracy of 95.7% while ours had an accuracy
ICAART 2022 - 14th International Conference on Agents and Artificial Intelligence
384

of 96.25% with 5 pre-trained models and a ternary
classification. In another related study, the authors
of (Santa Cruz, 2021) proposed a model compris-
ing a 2-stage transfer learning training process and
an ensemble learning method. They implemented six
pre-trained CNNs - VGG16, ResNet50 , ResNet50-
2, DenseNet161, DenseNet169and InceptionV3. 746
CT scan images, inclusive of 349 COVID-19 and 397
Normal cases were used. The model achieved an ac-
curacy of 86.70%, implying our model, with 5 clas-
sifiers greatly surpasses said model in terms of accu-
racy. Moreover it can also be observed that an ensem-
ble model has a better classification accuracy com-
pared to existing models with one or multiple classi-
fiers. In (Apostolopoulos and Mpesiana, 2020) Apos-
tolopoulos et al. successfully obtained an accuracy of
93.48% for a 3-class classification, but falls behind
when compared to our Ensemble approach, further
proving our point.
6.2 Limitations
The lack of computer resources was one of the limita-
tions that we had to face, i.e use of cloud computing
or distributed learning. The training time could have
been reduced. In-depth analysis would have been
achievable had we obtained more datasets, which can
be a possible extension to our study once more pa-
tient data becomes available. The perennial pandemic
and the lockdown hindered us in getting medical im-
ages from hospitals, thus having to rely on public
repositories. There are several scopes of bringing im-
provement to our work. For example, testing more
feature extraction models and combinations of clas-
sifier networks are to name a few. Furthermore, we
could have implemented segmentation. Moreover this
approach can also be implemented by incorporating
a larger dataset to attain a better predictive perfor-
mance. Some of the adversities faced during experi-
ments were the lack of annotated medical images and
classified datasets. Also, more image pre-processing
techniques can be applied for better results.
7 FUTURE PROSPECTS
Future prospects may include formulating new archi-
tectures based on CNN for the detection of COVID-
19 alongside other diseases in the medical domain.
The aforementioned models can be deployed in Web
and Mobile applications, where patients can self diag-
nose their ailments at their ease, thus saving valuable
seconds in dire time. Such applications can also be
extended towards hospital IT systems where patients
can receive budget-friendly and quick COVID-19 di-
agnosis alongside the in-action RT-PCR tests. Fu-
ture directions include to extend the proposed model
to risk stratification for survival analysis, anticipating
risk status of patients, and predicting hospitalization
duration which would be valuable for triaging, pa-
tient population management, and individualized care
planning.
8 CONCLUSION
Detection of the infamous Coronavirus is more im-
portant now than ever because of the ever-evolving
nature of the virus variants. As our contribution to-
wards faster diagnosis to curb cases, we propose an
ensemble model using 5 feature extraction state-of-
the-art CNN models, training on 2492 COVID im-
ages, 1675 Pneumonia images and 2496 Normal im-
ages. The testing set consisted of 400 images of each
class. Deep learning based recommender systems can
be of great help in this scenario when the volume of
patients is very high and required radiological exper-
tise is low. Detection of diseases from X-ray images
is in itself a challenging task thus requires consider-
ation from the research industry. Transfer learning
plays a major role in improving the accuracy of de-
tection. Our results prove that an ensemble model
surpasses an individual classification model, attaining
an accuracy of 96.25% and greater f-1 scores for all
the classes. As the number of patients are increasing
and the symptoms and development of the virus are
changing gradually, with the continuous collection of
data, we intend to extend the experiment further and
upgrade the usability of the model. Our methodol-
ogy achieved promising outcomes on the assembled
dataset and we believe it can be beneficial for radiolo-
gists and health experts to gain deeper understandings
into critical aspects related to COVID-19 cases. Such
a technique can be sent in remote areas to help analyze
respiratory illnesses and save lives. If COVID data
were readily available, better documented and anno-
tated it could bear the potential to open several path-
ways for more data-driven studies in the future. With
all that being said, we would also like to thank spe-
cialists, medical attendants and all the medical care
suppliers who are placing their lives in the front lines
to battle the COVID-19 outbreak.
REFERENCES
Ahmed, S., Hossain, T., Hoque, O. B., Sarker, S., Rahman,
S., and Shah, F. M. (2020). Automated covid-19 de-
X-Ray Classification to Detect COVID-19 using Ensemble Model
385

tection from chest x-ray images: A high resolution
network (hrnet) approach.
Albahli, S. (2020). Efficient gan-based chest radiographs
(cxr) augmentation to diagnose coronavirus disease
pneumonia. International journal of medical sciences,
17(10):1439.
Apostolopoulos, I. D. and Mpesiana, T. A. (2020). Covid-
19: automatic detection from x-ray images utilizing
transfer learning with convolutional neural networks.
Physical and Engineering Sciences in Medicine,
43(2):635–640.
Bhagat, V. and Bhaumik, S. (2019). Data augmentation
using generative adversarial networks for pneumonia
classification in chest xrays. In 2019 Fifth Interna-
tional Conference on Image Information Processing
(ICIIP), pages 574–579. IEEE.
Chollet, F. (2017). Xception: Deep learning with depthwise
separable convolutions. In Proceedings of the IEEE
conference on computer vision and pattern recogni-
tion, pages 1251–1258.
Chowdhury, M. E., Rahman, T., Khandakar, A., Mazhar,
R., Kadir, M. A., Mahbub, Z. B., Islam, K. R., Khan,
M. S., Iqbal, A., Al Emadi, N., et al. (2020). Can
ai help in screening viral and covid-19 pneumonia?
IEEE Access, 8:132665–132676.
Das, A. K., Ghosh, S., Thunder, S., Dutta, R., Agarwal,
S., and Chakrabarti, A. (2021). Automatic covid-19
detection from x-ray images using ensemble learning
with convolutional neural network. Pattern Analysis
and Applications, pages 1–14.
El Asnaoui, K. and Chawki, Y. (2020). Using x-ray images
and deep learning for automated detection of coron-
avirus disease. Journal of Biomolecular Structure and
Dynamics, pages 1–12.
Gordienko, Y., Gang, P., Hui, J., Zeng, W., Kochura, Y.,
Alienin, O., Rokovyi, O., and Stirenko, S. (2018).
Deep learning with lung segmentation and bone
shadow exclusion techniques for chest x-ray analy-
sis of lung cancer. In International Conference on
Computer Science, Engineering and Education Appli-
cations, pages 638–647. Springer.
Hira, S., Bai, A., and Hira, S. (2021). An automatic ap-
proach based on cnn architecture to detect covid-19
disease from chest x-ray images. Applied Intelligence,
51(5):2864–2889.
Huang, G., Liu, Z., Van Der Maaten, L., and Weinberger,
K. Q. (2017). Densely connected convolutional net-
works. In Proceedings of the IEEE conference on
computer vision and pattern recognition, pages 4700–
4708.
Irvin, J., Rajpurkar, P., Ko, M., Yu, Y., Ciurea-Ilcus, S.,
Chute, C., Marklund, H., Haghgoo, B., Ball, R., Sh-
panskaya, K., et al. (2019). Chexpert: A large chest
radiograph dataset with uncertainty labels and expert
comparison. In Proceedings of the AAAI Conference
on Artificial Intelligence, volume 33, pages 590–597.
Joseph, M. (2020). Does imagenet pretraining work for
chest radiography images(covid-19)?
Kesim, E., Dokur, Z., and Olmez, T. (2019). X-ray chest im-
age classification by a small-sized convolutional neu-
ral network. In 2019 scientific meeting on electrical-
electronics & biomedical engineering and computer
science (EBBT), pages 1–5. IEEE.
Khan, A. I., Shah, J. L., and Bhat, M. M. (2020). Coronet:
A deep neural network for detection and diagnosis of
covid-19 from chest x-ray images. Computer Methods
and Programs in Biomedicine, 196:105581.
Oh, Y., Park, S., and Ye, J. C. (2020). Deep learning covid-
19 features on cxr using limited training data sets.
IEEE Transactions on Medical Imaging, 39(8):2688–
2700.
Pardamean, B., Cenggoro, T. W., Rahutomo, R., Budiarto,
A., and Karuppiah, E. K. (2018). Transfer learning
from chest x-ray pre-trained convolutional neural net-
work for learning mammogram data. Procedia Com-
puter Science, 135:400–407.
Rahman, T., Khandakar, A., Qiblawey, Y., Tahir, A.,
Kiranyaz, S., Kashem, S. B. A., Islam, M. T.,
Al Maadeed, S., Zughaier, S. M., Khan, M. S.,
et al. (2021). Exploring the effect of image enhance-
ment techniques on covid-19 detection using chest
x-ray images. Computers in biology and medicine,
132:104319.
Santa Cruz, J. F. H. (2021). An ensemble approach
for multi-stage transfer learning models for covid-
19 detection from chest ct scans. Intelligence-Based
Medicine, 5:100027.
Sethi, R., Mehrotra, M., and Sethi, D. (2020). Deep learn-
ing based diagnosis recommendation for covid-19 us-
ing chest x-rays images. In 2020 Second International
Conference on Inventive Research in Computing Ap-
plications (ICIRCA), pages 1–4.
Stirenko, S., Kochura, Y., Alienin, O., Rokovyi, O., Gor-
dienko, Y., Gang, P., and Zeng, W. (2018). Chest x-
ray analysis of tuberculosis by deep learning with seg-
mentation and augmentation. In 2018 IEEE 38th In-
ternational Conference on Electronics and Nanotech-
nology (ELNANO), pages 422–428. IEEE.
Tataru, C., Yi, D., Shenoyas, A., and Ma, A. (2017). Deep
learning for abnormality detection in chest x-ray im-
ages. In IEEE Conference on Deep Learning.
Wang, B., Wu, Z., Khan, Z. U., Liu, C., and Zhu, M.
(2019). Deep convolutional neural network with seg-
mentation techniques for chest x-ray analysis. In 2019
14th IEEE Conference on Industrial Electronics and
Applications (ICIEA), pages 1212–1216. IEEE.
Wang, X., Peng, Y., Lu, L., Lu, Z., Bagheri, M., and Sum-
mers, R. M. (2017). Chestx-ray8: Hospital-scale chest
x-ray database and benchmarks on weakly-supervised
classification and localization of common thorax dis-
eases. In Proceedings of the IEEE conference on
computer vision and pattern recognition, pages 2097–
2106.
Wiysobunri, B. N., Erden, H. S., and Toreyin, B. U. (2020).
An ensemble deep learning system for the automatic
detection of covid-19 in x-ray images.
ICAART 2022 - 14th International Conference on Agents and Artificial Intelligence
386
