
Operationalizing Behavior Change Techniques in Conversational Agents
Maria In
ˆ
es Bastos
1 a
, Ana Paula Cl
´
audio
1 b
, Isa Brito F
´
elix
2 c
, Mara Pereira Guerreiro
2 d
,
Maria Beatriz Carmo
1 e
and Jo
˜
ao Balsa
1 f
1
LASIGE, Dep. Inform
´
atica, Faculdade de Ci
ˆ
encias, Universidade de Lisboa, Portugal
2
Nursing Research, Innovation and Development Centre of Lisbon (CIDNUR), Nursing School of Lisbon, Lisbon, Portugal
Keywords:
Conversational Agents, Ontologies, Behavior Change Techniques, Dialogue Platforms.
Abstract:
Departing from previous work on the use of well-established behavior change techniques in an mHealth in-
tervention based on a conversational agent (CA), we propose in this contribution a new architecture for the
design of behavior change CAs. This novel approach combines the use of an advanced natural language plat-
form (Dialogflow) with the explicit representation, in an ontology, of how behavior change techniques can be
operationalized. The integration of these two components is explained, as well as the most challenging aspect
of using the advanced features of the platform in a way that allowed the agent to lead the dialogue flow, when
needed. A successful proof of concept was built, which can be the basis for the development of advanced
conversational agents, combining natural language tools with ontology-based knowledge representation.
1 INTRODUCTION
We present a novel approach to the development of
conversational agents that combines the design and
development features offered by advanced natural
language tools with the use of knowledge needed to
support agents in the pursuit of their goals.
Besides the importance of building more ad-
vanced and versatile conversational agents, the drive
for this work comes from other two dimensions: the
importance of the role of conversational assistants in
healthcare (Guerreiro et al., 2021) and the incorpora-
tion of mechanisms that allow agents to induce behav-
ior change in their interlocutor.
In this work, we focus on how to provide agents
with the ability of operationalizing specific behavior
change techniques (BCTs), which are components of
an intervention designed to change behavior (Michie
et al., 2013).
The fact that noncommunicable diseases, like
Type 2 diabetes (T2D), account for a considerable
number of deaths (71% of deaths worldwide in 2016
a
https://orcid.org/0000-0002-5200-4981
b
https://orcid.org/0000-0002-4594-8087
c
https://orcid.org/0000-0001-8186-9506
d
https://orcid.org/0000-0001-8192-6080
e
https://orcid.org/0000-0002-4768-9517
f
https://orcid.org/0000-0001-8896-8152
(World Health Organization, 2021)) is a key indica-
tor of the importance of developing mechanisms that
help people preventing and managing this type of dis-
eases. Besides, the consistent growing availability of
mobile devices led to the development of thousands
of mHealth apps (mobile health applications); in a re-
cent scoping review (Wattanapisit et al., 2020), the
authors concluded that tasks such as ’disease-specific
care’ and ’health promotion’ can be successfully ful-
filled with the support of mHealth apps.
As behavior change interventions require multiple
interactions with a patient/user, the idea of a relational
agent (one that is designed to build and maintain long-
term social-emotional relationships) (Bickmore et al.,
2005) became crucial since the development of the
first stage of our work (F
´
elix et al., 2019; Balsa et al.,
2020). In our previous work, we developed a rule-
based prototype of a mobile application with an intel-
ligent virtual assistant to be used in an intervention to
promote the self-care of older people with T2D.
In order to extend this work so that it could be used
in a wider range of situations (other chronic diseases,
multi-morbidity, or targeting diverse types of users,
for instance), we had to overcome two of its limita-
tions: the input from the user had to be chosen from
a limited set of options, and the fact that the BCTs
were to a greater than ideal extent hard coded in the
dialogues definition.
216
Bastos, M., Cláudio, A., Félix, I., Guerreiro, M., Carmo, M. and Balsa, J.
Operationalizing Behavior Change Techniques in Conversational Agents.
DOI: 10.5220/0010826800003116
In Proceedings of the 14th International Conference on Agents and Artificial Intelligence (ICAART 2022) - Volume 1, pages 216-224
ISBN: 978-989-758-547-0; ISSN: 2184-433X
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
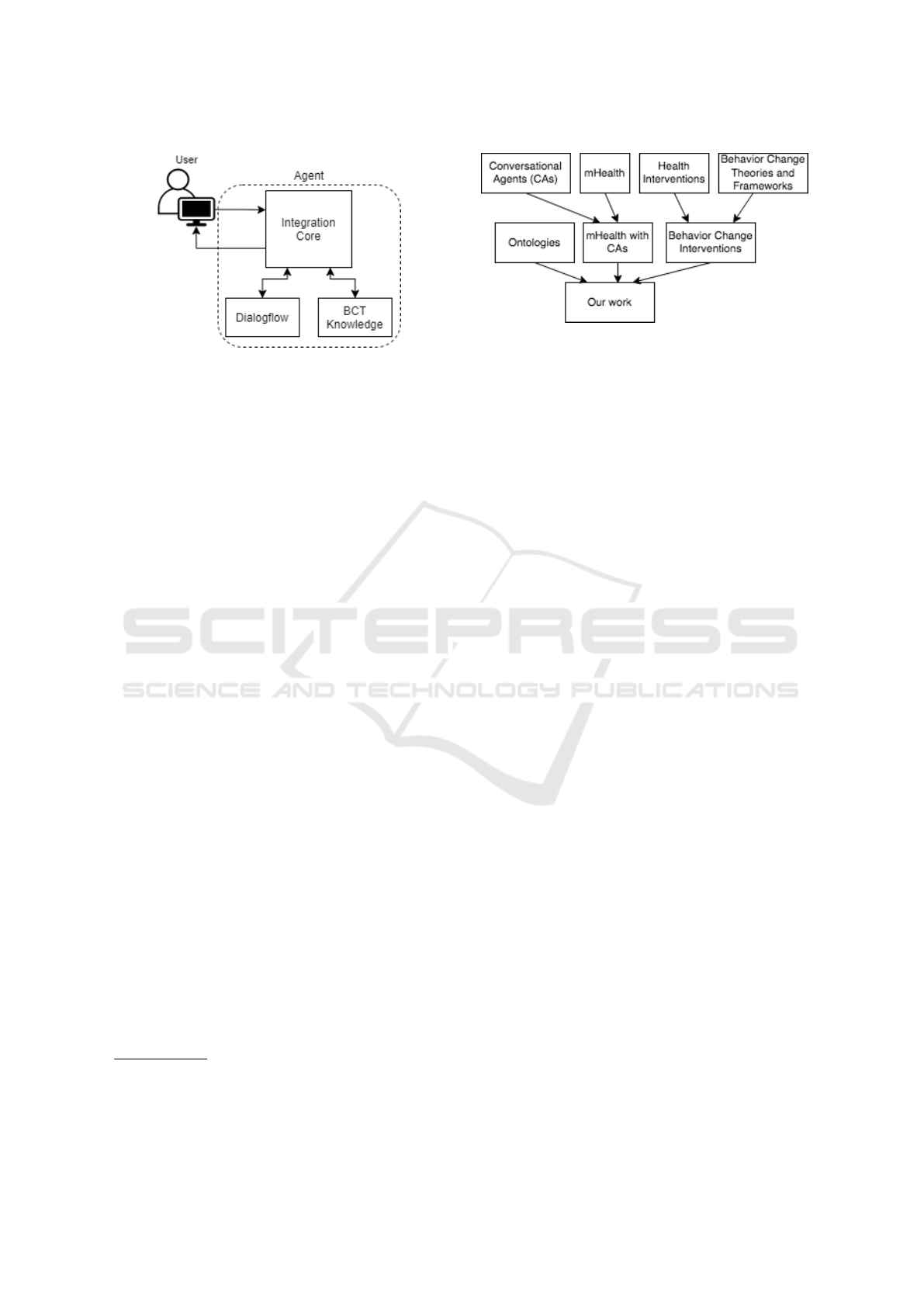
Figure 1: Simplified system’s architecture.
Continuing this work, we developed, and present
here, a new type of agent that allows us to overcome
the above mentioned limitations, while illustrating it
with BCTs operationalization.
As it is sketched in Figure 1, in which we present
a simplified view of the architecture, the use of Di-
alogflow
1
allowed us to deal with the first limitation.
To tackle the second limitation, we added a module
that allows the explicit representation of knowledge
on BCTs operationalization.
The core sections of this paper will describe in de-
tail these components and how they interconnect. But
first, in section 2, we highlight and discuss some re-
lated work. In section 3, we present the knowledge
component of our agent, namely the ontology that al-
lows us to better characterize BCTs operationaliza-
tion. In section 4, we describe the dialogue engine and
how Dialogflow was used. In section 5, we present
the detailed architecture and explain how the agent
works, illustrating it with a demo in section 6. Fi-
nally, in section 7, we present some conclusions and
directions for future work.
2 RELATED WORK
Our work derives from contributions in several di-
verse scientific areas. In Figure 2 we schematize how
those different areas directly or indirectly contribute
to our work.
The widespread use of mobile equipment across
people from all generations has been responsible for
the dissemination of mobile applications with diverse
purposes. Among these, a great number of develop-
ments were made in mHealth applications, the ones
that somehow “support the achievement of health ob-
jectives” (World Health Organization, 2011). A re-
1
A platform for the development of natural lan-
guage conversation interfaces (https://cloud.google.com/
dialogflow/)
Figure 2: Context of our contribution.
search carried out by Bhuyan et al. concluded that
60% of the adults who were mHealth apps users con-
sidered them useful in achieving health behavior goals
(Bhuyan et al., 2016). Moreover, mHealth applica-
tions are often used by people with little experience
of technology, as noted by Zapata et al. (Zapata et al.,
2015). So, mHealth offers a vast terrain of opportu-
nity to design digital solutions as tools to help im-
prove self-care, which can have a positive effect in
individual health outcomes and reduce the burden on
health systems. However, the conception of such ap-
plications entails high responsibility and the process
must be grounded on valid scientific studies.
The use of embodied conversational agents (ECA)
playing the role of virtual assistants has proved to be
well accepted by users in several health applications
(Baptista et al., 2020; Gong et al., 2020). In particu-
lar, Baptista et al. conducted a study to evaluate the
acceptability of an ECA (called Laura) to deliver self-
management education and support for patients with
T2D. The users are prompted to complete weekly in-
teractive sessions with Laura. This virtual assistant
provides education, feedback and motivational sup-
port for glucose level monitoring, taking medication,
physical activity, healthy eating and foot care. The
study had 66 respondents (mean age 55 years) and
the results identified positive reaction of the majority
of users for having a friendly, nonjudgmental, emo-
tional and motivational support provided by a human-
like character. Just around a third of them consid-
ered Laura not real, boring and annoying (Baptista
et al., 2020). Users respond to Laura by choosing
or by speaking out one of the options displayed in
the screen. The authors refer a “sophisticated script
logic” enabling the user to interact with Laura in sev-
eral predetermined variations. The solution was im-
plemented by a company that provides chatbots and
no details are given about these scripts. A more recent
12 months trial with 187 adults with T2D (age around
57) study resorting to the same solution, performed
during 12 months involving 187 adults suffering from
T2D (mean age 57), found a successful adoption of
Operationalizing Behavior Change Techniques in Conversational Agents
217

the program and a significant improvement in partic-
ipants’ health-related quality of life (HRQOL) (Gong
et al., 2020).
A recent systematic review about Artificial
Intelligence-Based Conversational Agents for
Chronic Conditions (Schachner et al., 2020) revealed
the immaturity of the field, using the authors’ own
words. They concluded that there is a lack of
evidence-based evaluation of the solutions, most
of them quasi-experimental studies. These authors
suggest that important future research would be
the definition of the AI architecture that should be
adopted and the adequate assessment process for the
overall solution.
As mentioned before, our research started some
time ago (Buinhas et al., 2019) with the development
of a first prototype. Key project features were re-
sorting to an anthropomorphic assistant with a rel-
evant role in the interaction with the user, and to
support the intervention design in a well-defined
theoretical framework, the Behavior Change Wheel
(Michie et al., 2014). This theoretical framework pro-
vides guidance to choose the more adequate behavior
change techniques in specific contexts.
A BCT is an observable, replicable, and irre-
ducible component of an intervention designed to
change behavior. They have been organized in a tax-
onomy (BCTTv1) (Michie et al., 2013; Cane et al.,
2015), which provides a definition for each of the
93 techniques. An example of a BCT is “problem
solving”; it requires users to pinpoint factors influenc-
ing the behavior and subsequently select strategies to
achieve it. After surveying 166 medication adherence
apps to ascertain whether they incorporated BCTs,
Morrissey et al. concluded that, from the 93 possi-
ble techniques only a dozen were found in the evalu-
ated apps (Morrissey et al., 2016). This result clearly
shows that more work is needed in incorporating evi-
dence on BCTs in available applications.
Although conversational agents (CA) have been
researched for decades, namely since the seminal
ELIZA (Weizenbaum, 1966), the shift towards be-
havior change is more recent (for instance, to pro-
mote a healthier lifestyle – typically regarding physi-
cal activity and type of diet). As reported by (Kramer
et al., 2020), CAs were found to have an important
value regarding the use of persuasive communication
in the health domain (Kramer et al., 2020), namely
when targeting coaching tasks. As Zhang et al. point
out, there is a “lack of understanding around the-
oretical guidance and practical recommendations on
designing AI chatbots for lifestyle modification pro-
grams” (Zhang et al., 2020). In order to overcome
this, these authors developed an AI chatbot behav-
ior change model that has persuasive conversational
capacity as a central component. Our work has this
same feature, although the architecture we present
goes beyond the coverage of just two specific topics,
as Zhang and his colleagues do.
Regarding the use of ontologies, it is worth men-
tioning two recent works that, in a different way,
stress the importance of its use in the context of our
work.
Within the Human Behaviour-Change Project
(Michie et al., 2017), an ontology is being developed
for representing behavior change interventions (BCIs)
and their evaluation (Michie et al., 2021). Although
it focuses on the more general aspects that character-
ize BCIs, it clearly opens the possibility of a link to
our work, via the common BCT concept that, having
a different perspective, has in our work the grounds
for the representation of its operationalization.
Also relevant to us is the recent work on the de-
velopment of dialogue managers combining ontolo-
gies and planning. Teixeira et al. combine a conver-
sational ontology and Artificial Intelligence planning
to generate dialogue managers capable of performing
goal-oriented dialogues in the health domain (Teixeira
et al., 2021). As the authors note, in the health domain
it is critical to have predictable and reliable systems,
making a knowledge component crucial to guarantee
that, even if complemented, as it is in our case, with
other resources, namely for natural language under-
standing tasks.
2.1 Dialogue Engines
In order to create our conversational agent, we chose
to adopt an existing tool, since many excellent tools
are currently available. The two main features we
wanted were: the possibility of having natural lan-
guage interaction and some control of the dialogue
flow, in order to address situations where the agent is
the one responsible for leading the dialogue (and not
the opposite, like what happens in question/answering
contexts, for instance).
Several dialogue tools were analyzed and tested
before choosing the most adequate. Due to space lim-
itation, we will just enumerate the tools we consid-
ered: Twine
2
, Yarn Spinner
3
, WOOL
4
, Watson As-
sistant
5
, FAtiMA Toolkit
6
, and Dialogflow.
As stated before, in this work, one of our main
interests was to make the dialogue more dynamic.
2
https://twinery.org/
3
https://yarnspinner.dev/
4
https://www.woolplatform.eu/
5
https://www.ibm.com/cloud/watson-assistant
6
https://fatima-toolkit.eu/
ICAART 2022 - 14th International Conference on Agents and Artificial Intelligence
218
Dialogflow, being a natural language understanding
platform, has proven to be quite useful in that aspect,
making it easier to build and deliver the agent mes-
sages and capturing the user’s response. In previous
work, the dialogue portions corresponding to BCTs
operationalization were initially created in YARN
(Balsa et al., 2020). Besides the fact that defining di-
alogs with that type of tool is a time-consuming task,
the definition of the whole logic of the interaction was
also harder than what we have with Dialogflow. Be-
sides, with this tool, the only user dialogue we have
to provide is the training phrases, and the agent will
learn from over time and usage.
3 AN ONTOLOGY OF BEHAVIOR
CHANGE CONCEPTS
One of the main limitations of the antecedent agent
was that BCT operationalization was too rigid, i.e. the
dialogue flow was too dependent on the way the cor-
responding dialogues were defined. In order to make
dialogues more natural and flexible, we decided to
characterize BCT operationalization in a more gen-
eral way. For that, we needed to identify the main
concepts involved and the relations between them.
We did this by defining an ontology representing the
relevant behavior change intervention concepts. Since
the operationalization of a BCT depends also on user
specific information, in order to characterize a spe-
cific way of operationalizing a BCT we had to incor-
porate concepts related to the user’s characteristics.
The resulting ontology can be divided in two main
class entities: Behavior Change Intervention (BCI)
and User. The first one, BCI, includes several classes
representing both general concepts (like BCT or Be-
havior determinant – see below) and specific ones
(like Food Topic, representing the relevant topics re-
lated to a healthy diet). As a starting point, our illus-
trative domain is healthy nutrition, as it should be an
universal concern, independent of age or health con-
dition. The User class includes concepts critical to
the operationalization, like the age category (adult, se-
nior, . . . ) or the identification of some risk condition.
Some of these entities are related by six object
properties: has active goals, has active topic, re-
lated to, targeted during, triggered by, and triggers.
For further characterization, there are also eight data
properties: BCT order, has age, has BMI (Body Mass
Index), has competence score, has genre, has height,
has risk level, and has weight.
The classes that the current work focuses on and
are: Behavior Change Intervention (an intervention
that has the aim of influencing human behavior);
Behavior Change Technique (an observable, replica-
ble, and irreducible component of an intervention de-
signed to alter or redirect causal processes that regu-
late behavior — an “active ingredient” on an inter-
vention (Michie et al., 2013); Behavior Determinant
(a factor that influences positively or negatively a be-
havior). For instance, a reason of non-adherence to
the user’s agreed goal – lack of motivation, forget-
fulness, . . . ); Behavior Goal (a goal defined in terms
of the behavior to be achieved); Behavior Topic (a
topic that is targeted during the intervention, aimed to
help achieve/maintain the desired behaviors); Opera-
tionalization (the act of delivering one or more BCTs,
based on several conditions); User (a person who’s
being subjected to the Behavior Change Intervention).
3.1 How the Ontology Is Used
This ontology can be used for several purposes within
the development of a dynamic Behavior Change In-
tervention, making it easier to connect the concepts
involved and shape the structure of the intervention.
When creating an application aimed at influencing
the human behavior, the use of an ontology can be
useful to detach the logic of the application from the
specific data (the individuals and their relationships).
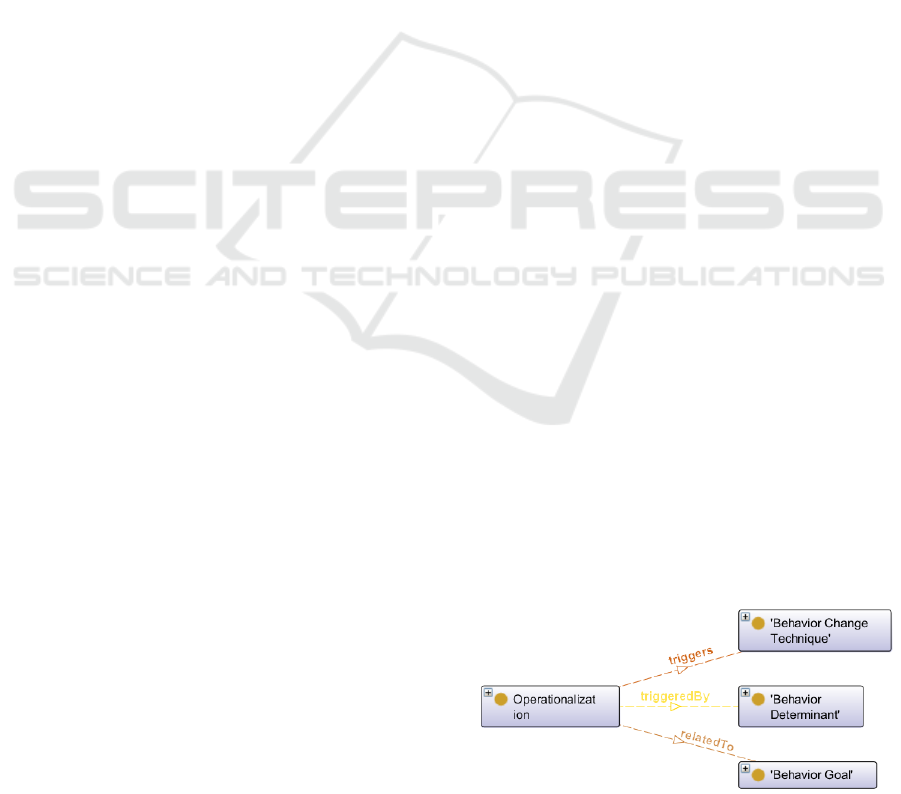
In order to understand better, the following para-
graphs describe a scenario where the ontology is used
during the interaction with the user. Figure 3 shows
the classes and relationships that are relevant to the
scenario described.
During Review Tasks (one of the dialogue stages,
as explained in the next section), the user is asked
whether he/she completed or not a previously agreed
goal. When the user answers negatively, the agent
will ask about the reason for not meeting the goal, and
the reason the user gives is denominated determinant.
The determinants of non-adherence can be as simple
as lack of motivation, or reluctance in changing their
habits, so the individuals of the class Behavior Deter-
minant are key words of such motives (so far, the de-
terminants included are motivation, habits, difficulty,
appetite, and loneliness). These determinants are ex-
amples and are not related with a particular behavior.
Figure 3: Ontology entities relevant to BCTs operational-
ization.
Operationalizing Behavior Change Techniques in Conversational Agents
219
After the user gives an answer (providing a deter-
minant), the agent queries the ontology to see which
operationalization related to the active goal is trig-
gered by that determinant. When the right opera-
tionalization is identified, the agent chooses the right
BCT to trigger. If it is the case that the operationaliza-
tion is sequential, the agent also determines the trig-
gering order. After that, it searches the dialogue file
and fetches the dialogue that is supposed to be deliv-
ered to complete the execution of a specific BCT.
4 DIALOGUE ENGINE
As stated before, we chose to use Dialogflow CX as
the dialogue engine. In this section, we describe how
our Dialogflow agent is built and used, along with the
details regarding the training process and the way we
deal with the situations where the agent takes control
of the dialogue.
4.1 How Dialogflow Is Used
Dialogflow CX has a visual builder in its console,
where conversation paths are graphed as a state ma-
chine model, making it easier to design, enhance, and
maintain. Conversation states and state transitions
are first-class types that provide explicit and powerful
control over conversation paths. We can clearly de-
fine a series of steps that we want the end-user to go
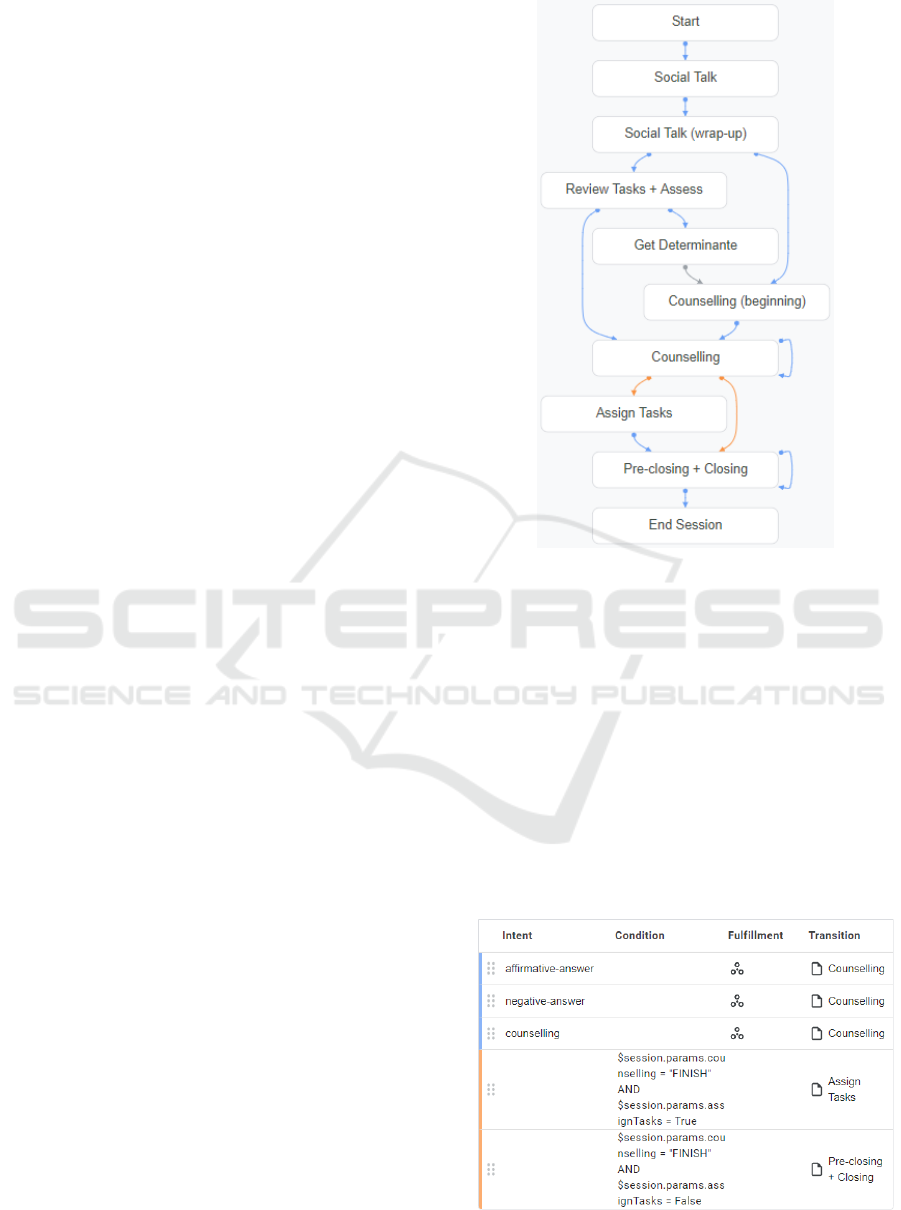
through. Following the work of Bickmore’s relational
agents group (Bickmore et al., 2005), dialogues are
organized in eight steps: opening, social talk, review
tasks, assess, counseling, assign tasks, pre-closing
and closing. The visual state machine created for our
agent is represented in Figure 4.
Each state is represented by a page, that can be
configured to collect information from the end-user
that is relevant for the conversational state represented
by the page. For simpler dialogue steps, such as
opening, social talk, assess, pre-closing and closing,
we configured the respective pages to give static text
responses, since there are no parameters or external
conditions that they depend on. For more complex
dialogue steps, such as review tasks, counseling and
assign tasks, we configured their respective pages to
enable webhook, in order to provide a dynamic re-
sponse based on external conditions.
To each page can be added state handlers, that
are used to control the conversation by creating re-
sponses for the end-users and/or by transitioning the
current page. There are two types of state handlers:
routes and event handlers. Routes are called when
an end-user input matches an intent (categorizes an
Figure 4: Conversation path of the Dialogflow agent.
end-user’s intention for one conversation turn) and/or
some condition.
Figure 5 shows the routes in our Counselling page.
The first three routes (with the blue left border) are
intent routes, which means that either one of those
routes are called when the user input matches one of
those intents. The last two routes (with the orange
left border) are condition routes, that are called if the
respective condition is satisfied. At the end of a route,
there’s a Transition field, which defines the next page
in the conversation.
In other resources, and in Dialogflow ES, an intent
usually contains a field with the training phrases and
Figure 5: Counselling page.
ICAART 2022 - 14th International Conference on Agents and Artificial Intelligence
220

a field with the agent response, that is sent back to the
user if their input matches the training phrases for that
intent. During an interaction, a user can say “yes” or
“no” multiple times, which means that, with this type
of intent, every time the user can say “yes” or “no”
during the conversation, there would have to be an in-
tent with the same training phrases but different agent
response, depending on the context. In Dialogflow
CX, an intent only contains the logic to detect what
the user says (the training phrases), which means an
intent can be reused in multiple places of a conversa-
tion.
4.2 Training Process
When an agent is trained, Dialogflow uses the train-
ing data to build machine learning models specifically
for that agent. This training data primarily consists of
intents, intent training phrases, and entities referenced
in a flow, which are effectively used as machine learn-
ing data labels. However, agent models are built using
parameter prompt responses, state handlers, agent set-
tings, and many other pieces of data associated with
the agent.
In the agent settings, it can be chosen to train
the agent automatically or manually. By default, the
training is executed automatically, showing a popup
dialogue in the console every time there’s an update
of the flow.
4.3 Leading the Dialogue
Technologies like Dialogflow are generally used in
virtual agents meant to handle questions from the
user. In our case, it is important that the agent is
the one taking control of the conversation, asking the
questions, and delivering the content in a “doctor-
patient” type of way, i.e. with the doctor leading the
interaction.
On previous work, after the agent’s response, the
user interface had buttons for the user to choose their
answer, and during longer explanations or a change
in the dialogue phase, it would present a “Continue”
button (Balsa et al., 2020). When the user has total
control over the input, we can not expect them to ca-
sually answer that. The agent must seek the user’s
attention and interest, keeping the user engaged in the
conversation.
In Dialogflow CX, all the agent responses are han-
dled in page, and a page can have an entry fulfillment,
and a static response for each route. The entry fulfill-
ment is optional, and it is what the agent will respond
to the end-user when a page initially becomes active.
For each route added to a page, there is a fulfillment
field, where it is possible to add several types of re-
sponse messages, although, in this work we only used
text response messages.
The entry fulfillment feature is a great advantage
since it makes it possible for the agent to say some-
thing to the user without the need to have a previous
input. This gives the agent more initiative and con-
trol over the conversation, being extremely useful be-
tween dialogue phases.
5 AGENT ARCHITECTURE
The architecture of our agent has comprises three
main components: the Core, the Dialogflow Engine,
and the Ontology (Figure 6). The Core controls the
interface and, along with the Dialogflow Engine, con-
trols the flow of execution and the speech of the agent.
The Ontology holds external data that can be queried
by the Core whenever necessary.
Figure 6 shows the steps that take place for one
conversational turn of a session:
1. The end-user types something, known as user in-
put.
2. The user interface (UI), responsible for the view
provided to the user, receives the input and for-
wards it to the Dialogflow API in a detect intent
request (handled by the Application Controller).
3. The Dialogflow API receives the detect intent re-
quest. It matches the user input to an intent or
form parameter, sets parameters as needed, and
updates the session state. In case it needs to call
a webhook-enabled fulfillment, it sends a web-
hook request to the Webhook Service, otherwise
it jumps straight to step 6.
4. The Webhook Service receives the webhook re-
quest and it takes any actions necessary, such as
querying the ontology and/or fetching dialogue
from external sources (JSON files).
5. The Webhook Service builds a response and sends
a webhook response back to Dialogflow.
6. Dialogflow creates a detect intent response. If
a webhook was called, it uses the response pro-
vided in the webhook response. If no webhook
was called, it uses the static response defined in
the Dialogflow Agent. The detect intent response
is send to the user interface.
7. The user interface receives the detect intent re-
sponse and forwards the text response to the end-
user.
8. The end-user sees the response.
Operationalizing Behavior Change Techniques in Conversational Agents
221
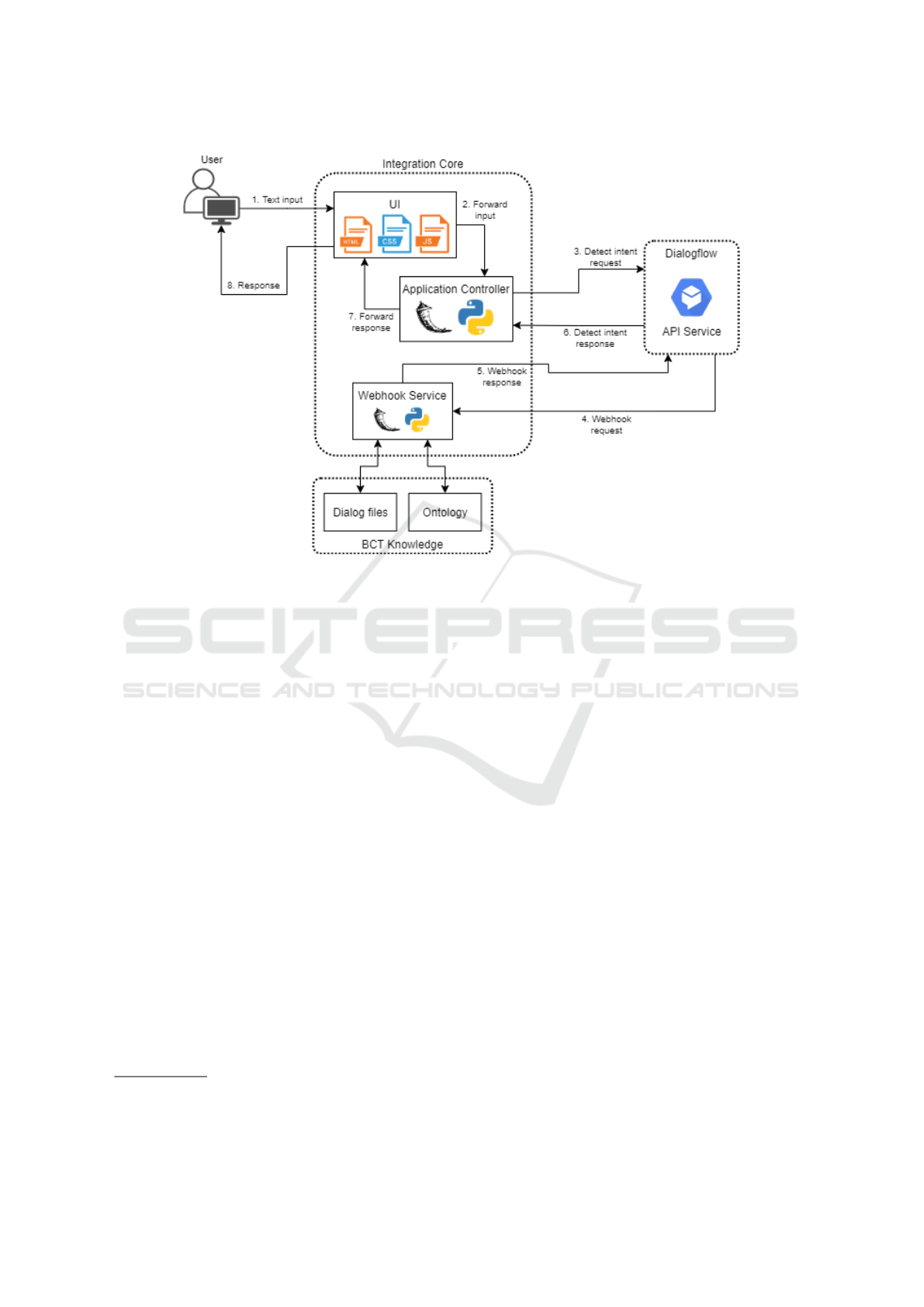
Figure 6: Agent architecture.
In short, when a user submits a message, it is sent
to Dialogflow to detect the intent of the user. Di-
alogflow will process the text, then send back a ful-
fillment response (either static, or dynamic, by means
of the Webhook Service).
6 DEMO
During a few dialogue steps, there are specific BCTs
that are always operationalized in the same way,
therefore being simpler to execute. For example, dur-
ing Review Tasks, the BCT Self-monitoring of behav-
ior (2.3)
7
is always executed and delivered in the same
way: by collecting data on the user’s behavior. To
do that, our system takes advantage of the following
ontology classes: User and Behavior Goal. Linking
those classes is an object property, labeled has active
goals, that connects one or more behavior goals to a
specific user. That way, the system can easily get ac-
cess to the goal that the user agreed on, and through
its label, ask if they completed it or not.
During Assess and Counseling, the procedure is
a bit more complex, since the BCTs operationalized
on those dialogue steps are executed in several differ-
ent ways, depending on more than just one condition.
7
The numbers next to the names of the BCTs refer to the
codes used in the taxonomy (Michie et al., 2013).
Following the case mentioned in the previous para-
graph, after Review Tasks, comes Assess, and during
that step, the system takes advantage of the follow-
ing classes: Operationalization, User, Behavior Goal,
Behavior Determinant and Behavior Change Tech-
nique. As was mentioned in Section 3.1, when the
system gets the non-adherence determinant, it queries
the ontology in order to find which operationalization,
related to the active goal, is triggered by that given de-
terminant. After that, the system accesses the object
property triggers, to see which BCTs are triggered in
that operationalization. In case the operationalization
is of the Sequential type (a complex operationaliza-
tion where the BCTs are delivered in sequential or-
der), the system accesses the data property BCT order,
to be able to deliver the BCTs in the suitable order.
Figure 7 illustrates an output demonstration of the
examples given in the previous paragraphs. The agent
asks the user if they completed the agreed goal ( “have
at least three main meals”, highlighted in green on the
first chat message on the left upper corner), to which
the user answers negatively. After that, there is the
operationalization of another simpler BCT, Feedback
on behavior (2.2), statically delivered by Dialogflow
since it only depends on the intent (“Yes” or “No”).
The user answers saying “I don’t have motivation”, to
which the system catches the “motivation” behavior
determinant. The operationalization related to the ac-
tive goal, and triggered by motivation, is the individ-
ICAART 2022 - 14th International Conference on Agents and Artificial Intelligence
222

Figure 7: An example dialogue.
ual OP Alim Det1 2, which triggers the BCTs Prob-
lem solving (1.2) and Information of health conse-
quences (5.1), having “1.2, 5.1” as BCT order. Given
those conditions, the system accesses the dialogue file
and extracts the dialogue parts related to those BCTs,
ordering them accordingly and sending them to the
user. In the last chat message on the lower left corner
of Figure 7, highlighted in dark blue is the dialogue
delivering Problem solving (1.2), and higlighted in
purple is the dialogue part that delivers Information
of health consequences (5.1).
7 CONCLUSIONS
The main goal of this work was achieved with the de-
sign and implementation of a novel architecture for
the development of conversational agents for behav-
ior change interventions. This architecture allows the
combination of an advanced dialogue engine with a
learning ability (DialogFlow) with the representation
of knowledge on the operationalization of behavior
change techniques, by means of defining an ontology
of behavior change intervention concepts.
The design was explained and the functioning of
the agent illustrated.
Regarding future work, two immediate steps fol-
low: the incorporation of additional knowledge so
that the agent capacity can be enlarged; the additional
training of the system with a set of dialogues that were
developed in a previous work.
Additionally, we intend to incorporate in the de-
sign mechanisms that will allow the consideration of
an ethical dimension in this type of agents. As rec-
ognized by Zhang and her colleagues (Zhang et al.,
2020), the ethical dimensions regarding conversa-
tional agents development has been completely ab-
sent. But, in contexts where the goal is to induce be-
havior change in humans, the incorporation of ethical
principles and the insurance of responsibility in the
systems’ designers is of paramount importance.
ACKNOWLEDGEMENTS
This work was supported by FCT through the
LASIGE Research Unit, ref. UIDB/00408/2020 and
ref. UIDP/00408/2020.
REFERENCES
Balsa, J., F
´
elix, I., Cl
´
audio, A. P., Carmo, M. B., Silva, I.
C. e., Guerreiro, A., Guedes, M., Henriques, A., and
Guerreiro, M. P. (2020). Usability of an Intelligent
Virtual Assistant for Promoting Behavior Change and
Self-Care in Older People with Type 2 Diabetes. Jour-
nal of Medical Systems, 44(7):130.
Baptista, S., Wadley, G., Bird, D., Oldenburg, B., Speight,
J., and Group, T. M. D. C. R. (2020). Acceptabil-
ity of an Embodied Conversational Agent for Type
2 Diabetes Self-Management Education and Support
via a Smartphone App: Mixed Methods Study. JMIR
mHealth and uHealth, 8(7):e17038.
Bhuyan, S. S., Lu, N., Chandak, A., Kim, H., Wyant, D.,
Bhatt, J., Kedia, S., and Chang, C. F. (2016). Use of
Mobile Health Applications for Health-Seeking Be-
havior Among US Adults. Journal of Medical Sys-
tems, 40(6):153.
Bickmore, T. W., Caruso, L., Clough-Gorr, K., and Heeren,
T. (2005). ‘It’s just like you talk to a friend’ relational
agents for older adults. Interacting with Computers,
17(6):711–735.
Buinhas, S., Cl
´
audio, A. P., Carmo, M. B., Balsa, J.,
Cavaco, A., Mendes, A., F
´
elix, I., Pimenta, N., and
Guerreiro, M. P. (2019). Virtual Assistant to Improve
Self-care of Older People with Type 2 Diabetes: First
Prototype. In Garc
´
ıa-Alonso, J. and Fonseca, C., edi-
tors, Gerontechnology, Communications in Computer
and Information Science, pages 236–248. Springer In-
ternational Publishing.
Cane, J., Richardson, M., Johnston, M., Ladha, R., and
Michie, S. (2015). From lists of behaviour change
techniques (BCTs) to structured hierarchies: Com-
parison of two methods of developing a hierarchy
of BCTs. British Journal of Health Psychology,
20(1):130–150.
F
´
elix, I. B., Guerreiro, M. P., Cavaco, A., Cl
´
audio, A. P.,
Mendes, A., Balsa, J., Carmo, M. B., Pimenta, N.,
and Henriques, A. (2019). Development of a Com-
plex Intervention to Improve Adherence to Antidia-
betic Medication in Older People Using an Anthro-
pomorphic Virtual Assistant Software. Frontiers in
Pharmacology, 10:680.
Operationalizing Behavior Change Techniques in Conversational Agents
223

Gong, E., Baptista, S., Russell, A., Scuffham, P., Riddell,
M., Speight, J., Bird, D., Williams, E., Lotfaliany, M.,
and Oldenburg, B. (2020). My Diabetes Coach, a Mo-
bile App–Based Interactive Conversational Agent to
Support Type 2 Diabetes Self-Management: Random-
ized Effectiveness-Implementation Trial. Journal of
Medical Internet Research, 22(11):e20322.
Guerreiro, M. P., Angelini, L., Rafael Henriques, H., El Ka-
mali, M., Baixinho, C., Balsa, J., F
´
elix, I. B., Khaled,
O. A., Carmo, M. B., Cl
´
audio, A. P., Caon, M., Da-
her, K., Alexandre, B., Padinha, M., and Mugellini, E.
(2021). Conversational Agents for Health and Well-
being Across the Life Course: Protocol for an Evi-
dence Map. JMIR Research Protocols, 10(9):e26680.
Kramer, L. L., ter Stal, S., Mulder, B. C., de Vet, E., and
van Velsen, L. (2020). Developing Embodied Con-
versational Agents for Coaching People in a Healthy
Lifestyle: Scoping Review. Journal of Medical Inter-
net Research, 22(2):e14058.
Michie, S., Atkins, L., and West, R. (2014). The behaviour
change wheel : a guide to designing interventions. Sil-
verback.
Michie, S., Richardson, M., Johnston, M., Abraham, C.,
Francis, J., Hardeman, W., Eccles, M. P., Cane, J., and
Wood, C. E. (2013). The Behavior Change Technique
Taxonomy (v1) of 93 Hierarchically Clustered Tech-
niques: Building an International Consensus for the
Reporting of Behavior Change Interventions. Annals
of Behavioral Medicine, 46(1):81–95.
Michie, S., Thomas, J., Johnston, M., Aonghusa, P. M.,
Shawe-Taylor, J., Kelly, M. P., Deleris, L. A.,
Finnerty, A. N., Marques, M. M., Norris, E., O’Mara-
Eves, A., and West, R. (2017). The Human Behaviour-
Change Project: harnessing the power of artificial
intelligence and machine learning for evidence syn-
thesis and interpretation. Implementation Science,
12(1):121.
Michie, S., West, R., Finnerty, A., Norris, E., Wright, A.,
Marques, M., Johnston, M., Kelly, M., Thomas, J.,
and Hastings, J. (2021). Representation of behaviour
change interventions and their evaluation: Develop-
ment of the Upper Level of the Behaviour Change
Intervention Ontology. Wellcome Open Research,
5(123).
Morrissey, E. C., Corbett, T. K., Walsh, J. C., and Molloy,
G. J. (2016). Behavior Change Techniques in Apps
for Medication Adherence. American Journal of Pre-
ventive Medicine, 50(5):e143–e146.
Schachner, T., Keller, R., and v Wangenheim, F. (2020). Ar-
tificial Intelligence-Based Conversational Agents for
Chronic Conditions: Systematic Literature Review.
Journal of Medical Internet Research, 22(9):e20701.
Teixeira, M. S., Maran, V., and Dragoni, M. (2021). The in-
terplay of a conversational ontology and AI planning
for health dialogue management. In Proceedings of
the 36th Annual ACM Symposium on Applied Comput-
ing, pages 611–619, Virtual Event Republic of Korea.
ACM.
Wattanapisit, A., Teo, C. H., Wattanapisit, S., Teoh, E.,
Woo, W. J., and Ng, C. J. (2020). Can mobile health
apps replace GPs? A scoping review of comparisons
between mobile apps and GP tasks. BMC Medical In-
formatics and Decision Making, 20(1):5.
Weizenbaum, J. (1966). ELIZA—a computer program for
the study of natural language communication between
man and machine. Communications of the ACM,
9(1):36–45.
World Health Organization (2011). mHealth : new horizons
for health through mobile technologies. World Health
Organization, Geneva.
World Health Organization (2021). Noncom-
municable diseases: Mortality. [online].
https://www.who.int/data/gho/data/themes/topics/
topic-details/GHO/ncd-mortality [accessed 2021-09-
28].
Zapata, B. C., Fern
´
andez-Alem
´
an, J. L., Idri, A., and Toval,
A. (2015). Empirical Studies on Usability of mHealth
Apps: A Systematic Literature Review. Journal of
Medical Systems, 39(2):1.
Zhang, J., Oh, Y. J., Lange, P., Yu, Z., and Fukuoka,
Y. (2020). Artificial Intelligence Chatbot Behavior
Change Model for Designing Artificial Intelligence
Chatbots to Promote Physical Activity and a Healthy
Diet: Viewpoint. Journal of Medical Internet Re-
search, 22(9):e22845.
ICAART 2022 - 14th International Conference on Agents and Artificial Intelligence
224
