
Designing Neurogames to Support Patients under Psychotherapy
Treatment: Opportunities and Challenges of the MUSE Headband
Michael Pantf
¨
order
1
and Andre Hellwig
2
1
Fraunhofer Institute for Software and Systems Engineering ISST, Dortmund, Germany
2
Hochschule f
¨
ur Gesundheit, Bochum, Germany
Keywords:
Serious Game, Neurofeedback, Psychotherapy, Brain Computer Interface, Electroencephalography.
Abstract:
In childhood and adolescence, mental development processes are crucial for a person’s long-term, cognitive
health. Many young people have at least one characteristic that leads to psychological impairment and must
be accompanied by therapy. Therapy success requires the constant execution of therapeutic exercises during
and after therapy sessions. However, keeping the motivation of the patients upright for continuous cooperation
is a key challenge, since the exercises are perceived as laborious. A digital, playful training application offers
the potential to support the therapy of children and adolescents. Measuring brain activity plays an impor-
tant role as it shows how good patients can push away negative thoughts affecting their mental disorder. For
this purpose the fundamentals of serious games, neurofeedback, brain computer interfaces (BCIs) and elec-
troencephalography (EEG) as well as different therapy-accompanying measures were examined. Based on the
findings and a focus group with psychotherapists (N=3), a serious game was designed as a motivational con-
centration and attention training to support psychotherapy. During the game the easy-to-use MUSE headband
measures concentration and integrates neurofeedback as a game mechanic. User tests with children (N=21)
were performed to evaluate the developed prototype and gather further information on usability, technology
acceptance and playfulness of the neurogame.
1 INTRODUCTION
Mental disorders are global public health issues. They
account for more than 10% of the global burden of
disease (Vigo et al., 2016) and no fewer than 800,000
people die each year as a result of suicide (World
Health Organization, 2018). The number of people
under the age of 15 who suffer from depression has in-
creased significantly in recent years and has increased
more than tenfold compared to the year 2000. Ac-
cording to Naab et al. (Naab et al., 2017) a nation-
wide study in Germany of 2,863 families with chil-
dren aged 7 to 17 years showed that 14.5% of the
children had characteristics of at least one impairing
mental health problem. Same or even higher per-
centages across Europe up to 27.9% in Bulgaria were
shown by Husky et al. (Husky et al., 2018). How-
ever, less than half of the children received therapy or
the parents considered it in need of treatment. Typi-
cal disorders that occur in young children are: post-
traumatic stress disorders, depressive disorders, atten-
tion deficit / hyperactivity disorders (ADHD), anx-
iety disorders, autistic disorders, attachment disor-
ders and sleep disorders. Successful therapy can only
be achieved through careful and independent imple-
mentation of therapy-accompanying exercises. How-
ever, many patients do not perform their exercises
regularly because they find the tasks tedious or bor-
ing (Mader et al., 2016). Accompanying and sup-
porting measures, which are used in psychotherapy
to reduce symptoms, are mindfulness exercises, re-
laxation procedures as well as concentration and at-
tention training. These measures are used to treat a
wide range of mental illnesses and have been proven
through studies. However, the patient lacks motiva-
tion to carry out the exercises continuously, since ther-
apeutic success does not occur immediately. In order
to enable treatments for the large number of young
patients and to motivate them to carefully carry out
exercises accompanying therapy, motivational, tar-
get group-specific support of the therapy is required.
Here, the use of electronic devices offers the potential
to close gaps in therapy and to open up new treat-
ment options or to supplement existing ones. Chap-
ter 2 introduces background information about neu-
rofeedback, Brain Computer Interfaces and Serious
296
Pantförder, M. and Hellwig, A.
Designing Neurogames to Support Patients under Psychotherapy Treatment: Opportunities and Challenges of the MUSE Headband.
DOI: 10.5220/0010738500003123
In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2022) - Volume 5: HEALTHINF, pages 296-305
ISBN: 978-989-758-552-4; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

Game Design. Chapter 3 outlines the conducted re-
search method. Chapter 4 presents the findings, chap-
ter 5 discusses results and chapter 6 summarizes re-
sults and gives ideas about future work.
2 BACKGROUND
According to Li et al. (Li et al., 2014), a lot of re-
search has been done in recent years to develop new
and inexpensive technologies that can be used to treat
mental health. Digital applications such as serious
games can be used as a therapy-accompanying mea-
sure and motivational incentive to support the therapy
of children and adolescents with different mental ill-
nesses. Thereby therapeutic effects can be achieved
by training certain skills as well as conveying psy-
chotherapeutic content. Such games have been used
successfully in psychotherapy to treat various mental
disorders. The success of serious games in the context
of therapy lies primarily in their ability to increase
therapy compliance and motivate patients to indepen-
dently carry out therapy-supporting exercises at home
(Brezinka and Hovestadt, 2007; Fernandez-Cervantes
et al., 2015). In addition, they offer the potential to
convey psychotherapeutic content in a playful way
and thus increase the learning success in exercises
accompanying therapy. When performing such exer-
cises, various physiological effects occur, which can
be recorded with the help of neurofeedback devices
(Goldbeck and Schmid, 2003; Forsner et al., 2014).
2.1 Neurofeedback
Today, neurofeedback is considered a scientifically
recognized method for optimizing brain activity by
minimizing or maximizing certain activities. Stud-
ies have shown that patients with various mental dis-
orders have brain activities that differ from healthy
people. A large number of disorders, diseases and un-
wanted behavior patterns can be attributed to incorrect
regulation of brain activity (Fiałek and Liarokapis,
2016; Sourina et al., 2011). Neurofeedback is mea-
sured with Brain Computer Interfaces (BCIs) and dis-
plays patient brain activity in real time. As part of
neurofeedback training, the patient should learn to
control his brain activity and to consciously change
it. Neurofeedback training is intended to teach the
patient how to regulate abnormalities in his brain ac-
tivity himself (Heinrich et al., 2007). The user can re-
ceive various feedback about his internal status. Ac-
cording to Hammond (Hammond, 2011),neurofeed-
back has been used in clinical and research appli-
cations for decades to treat patients with mental ill-
nesses and has already been used successfully in nu-
merous psychiatric and neurological disorders, such
as depression, concentration and memory problems,
stress disorders, ADHD and autism. In addition,
neurofeedback training can also be used to promote
health, preventive measures and improve cognitive
performance in healthy people, such as coping with
stress or training the memory. This makes neuro-
feedback training an important treatment method for
a wide range of mental disorders as an alternative to
medication. Neurofeedback training can be carried
out in various forms such as neurogames, simple vi-
sual feedback or audio feedback (Liu et al., 2016). So
far, there is no generally applicable standard for neu-
rogames. Various works, however, use this term in
a similar context as digital games, which use neuro-
feedback devices, such as brain computer interfaces,
for interaction within a game. BCIs measure brain ac-
tivity and recognize certain brain patterns that can be
interpreted and translated into commands for commu-
nication with BCI applications. Their use enables the
internal state of the user to be included in the game
and to provide feedback on physiological processes
in the body that are normally not perceptible (Hein-
rich et al., 2007). In this way, the application can be
adapted to the feelings and experiences of the user in
order to integrate them more into the game. With the
help of neurofeedback within a serious game, aware-
ness of one’s own inner state can be developed, self-
reflection can be facilitated and mindfulness can be
promoted (Sliwinski et al., 2017).
2.2 Brain Computer Interfaces and
MUSE Headband
A Brain-Computer-Interface (BCI), also called
Brain-Machine-Interface (BMI), is with respect to
Graimann, Allison and Pfurtscheller (Graimann
et al., 2009), an artificial system that measures the
user’s brain activity, interprets it and translates it into
control signals for BCI applications. Since the mea-
sured activity comes directly from the brain without
requiring physical movement, it is referred to as the
brain-computer interface. A BCI can, according to
Graimann et al. not read minds, but classify special
activity patterns in brain signals that are associated
with certain tasks or events. Brain-computer in-
terfaces represent a sub-category of the so-called
“prostheses”. These are devices that not only receive
output from nervous systems, but can also offer input
and thus interact with the peripheral and central
nervous system. Brain computer interfaces enable
the use of interactive applications by interpreting
and translating various brain patterns into control
Designing Neurogames to Support Patients under Psychotherapy Treatment: Opportunities and Challenges of the MUSE Headband
297

commands (Wolpaw et al., 2002). They enable a
new human-computer interaction as an alternative to
conventional input devices such as a mouse, keyboard
and touch displays and can thus be used by people
with serious physical disabilities as a non-muscular
means of communication (Graimann et al., 2009;
Perales and Amengual, 2017; Sourina et al., 2011).
BCIs can also be used as neurofeedback training as
a treatment alternative for various cognitive disor-
ders. However, brain-computer interfaces are not
suitable for controlling complex applications because
their information transfer rate is not sufficient for
this. Complex tasks like controlling a robot arm,
reaching for a bottle or chatting quickly require more
information per second than can be provided by a
BCI (Graimann et al., 2009). In addition, so-called
artifacts can occur during signal acquisition, which
arise as interference in the signal due to other activ-
ities and must be removed (Fiałek and Liarokapis,
2016; Graimann et al., 2009). Non-invasive elec-
troencephalography (EEG) is the most widespread
technology. It is used to record the electrical activity
of the scalp using electrodes. Compared to other
BCI technologies, EEGs are inexpensive, portable
and offer a reasonable compromise between spatial
and temporal resolution (Graimann et al., 2009;
Scherer et al., 2017; Vourvopoulos et al., 2017).
With the help of an EEG, the electrical potential of
the scalp can be measured using surface electrodes.
According to Sourina et.al. (Sourina et al., 2011), this
potential arises from cerebral cortex activity in the
brain and reflects the state of the brain. This makes
it possible to recognize emotions, mental states
and movement ideas of the user in a non-invasive
manner in real time (Sourina and Liu, 2015). The use
of EEG technology in various research disciplines
has increased in recent years since more and more
inexpensive, easily transportable and user-friendly
devices have been commercially available which
provide sufficient measurement quality (Krigolson
et al., 2017; Przegalinska et al., 2018; Scherer et al.,
2017). This research focuses on the MUSE headband,
as it is an easy to use EEG headband. Studies show
that it is also a reliable source for measuring gamma
waves as the source of concentration (Krigolson
et al., 2017; Przegalinska et al., 2018). Compared
to the Mindwave, which is often used as a BCI for
neurogames and offers only 1 EEG, MUSE measures
brain activity with 7 EEG sensors.
2.3 Neurogames in Psychotherapy
”Harvest Challenge” is a neurogame intended to serve
as intention training for children with attention deficit
and hyperactivity disorder between the ages of 8 and
13 years. Munoz et al. (Mu
˜
noz et al., 2015) de-
cided to use the MindWave neurofeedback headset as
part of this application, since it is comfortable for the
user to use and requires little configuration time. Har-
vest Challenge was designed for use in various edu-
cational institutions and for neuropsychological care,
but should also be usable by children at home. The
digital game was developed in an interdisciplinary
team of designers, developers, neuropsychologists
and psychiatrists and incorporates the internal state of
the user into the application with the help of an EEG.
The goal of the game is to improve certain skills of
the child. This includes patience, planning skills as
well as the ability to follow instructions and achieve
goals. The improvement of these skills should also
lead to an increased learning process as well as an
improved control of attention. Within the application,
the player controls a boy who lives in a Colombian
coffee region and has to perform various tasks in the
form of mini-games. The relaxation and concentra-
tion level of the user is integrated in different ways
for interaction within the game. As part of a mini-
game, the player has to select predetermined objects
that rotate in a circle. In order to select an object,
he must stop the rotation by increasing his attention
level when the object is at a predetermined position.
Another mini-game is that the player has to collect
vegetables. However, this is only possible if the user
reaches a certain concentration level and should train
him to keep his concentration. At the end, the course
of the user’s mental activity during the game is visual-
ized by a diagram. So far, no studies on the effective-
ness of Harvest Challenge have been published. This
application shows how a neurogame for children with
ADHD can involve the player’s level of concentration
in different ways to actively influence the game in or-
der to train the ability to concentrate, while improv-
ing other relevant skills. Schoneveld et al. (Schon-
eveld et al., 2018) as well as Jacob and Teuteberg (Ja-
cob and Teuteberg, 2017) present the game ”Mind-
Light” in their work developed by the PlayNice Insti-
tute, which also uses the MindWave from Neurosky
to include neurofeedback. This is a neurogame for the
therapy of children with increased anxiety symptoms.
Various techniques such as neurofeedback, confronta-
tion training, and attention modification training are
included within the game to train children to deal
with their anxiety. In the context of the application,
the player takes on the role of a child who wants to
save his grandmother from evil forces. Various re-
laxation techniques are taught to the user within the
game. He should also learn that he can overcome his
fears by adjusting his state of mind. The relaxation
HEALTHINF 2022 - 15th International Conference on Health Informatics
298

level of the player is included in the application and
represented by a shining light, which helps the player
to navigate through the game world and defeat oppo-
nents. The user must remain as relaxed as possible in
order to use light to transform threatening objects and
shapes into harmless ones. Schoneveld et al. exam-
ined in a study with 174 children between the ages of
7 and 12 whether MindLight is just as effective for the
therapy of children with anxiety symptoms as cogni-
tive behavior therapy. Half of the children played the
game, while the other half received conventional ther-
apy. Both treatments showed a significant decrease in
anxiety symptoms, with MindLight having the same
effectiveness as cognitive behavior therapy. Mind-
Light thus proved to be an effective measure for the
prevention of anxiety for children within the scope of
the study. This neurogame demonstrates how differ-
ent coping strategies can be conveyed as a therapeutic
measure in a child-friendly manner within an appli-
cation and how the player’s internal state can be inte-
grated in order to influence the game environment and
atmosphere and thereby achieve a therapeutic effect.
The MindWave headset however used in both projects
utilizes only one EEG sensor which could lead to in-
accurate measurements. No neurogame has currently
evaluated the MUSE headband, which might lead to
better results.
3 METHODS
The general research method used as a guiding frame-
work follows the user-centered development princi-
ples described by Abeele et al. (Abeele et al., 2011).
Firstly, a review of related work and current BCI
and EEG technologies for a focus group with psy-
chotherapists was prepared to identify requirements
and potentials of neurogames. Secondly, a neurogame
prototype using the MUSE headband was developed.
Thirdly, a gameplay test with healthy children was
conducted to evaluate game design of the developed
prototype and used technology.
3.1 Requirements Analysis: Focus
Group
As part of the preparation for this work, a prelim-
inary semi-structured focus group with psychother-
apists working in a clinic (N=3) was carried out to
identify needs and potentials for neurogames. In this
clinic, children and adolescents between the ages of 6
and 19 are treated with mental illnesses such as anx-
iety disorders, depression, eating disorders, ADHD
and disorders of social behavior. In preparation for
the focus group, an initial research was carried out
on the use of mindfulness exercises, relaxation pro-
cedures as well as attention and concentration train-
ing to accompany and support psychotherapy in or-
der to gain a basic understanding. Questions and first
ideas concerning the development of a neurogame
(for instance interaction, gameplay, learning) with the
MUSE headband have been prepared for the focus
group as well. Goal of the focus group was the iden-
tification of requirements for a neurogame supporting
psychotherapy.
3.2 Neurogame Development
Following the findings of the focus group, a neu-
rogame prototype was developed in constant interac-
tion with the psychotherapists (N=3). The different
states of the prototype were shown to the therapists re-
motely. The test subjects were advised to think aloud
while watching the game being played live. Within
the application, two players control their characters
through different levels of a pyramid with the aim
of getting to the lowest level to find the Pharaoh’s
treasure. Each level consists of a dark, randomly
generated labyrinth. Level design and scripting was
done using the Unity game engine. A script gener-
ates a random map using depth-first search for given
x and y dimensions and then places a given num-
ber of stone tablets, treasures as well as the exit at
random positions within the labyrinth. The integra-
tion of a labyrinth as a puzzle element was chosen
because labyrinth tasks are used as part of therapies
for children as a measure to promote concentration.
Both players have a special light source, the radius
of which is determined by the concentration level of
the respective player. For this purpose, the users wear
the MUSE headband, which measures the concentra-
tion of the users using gamma waves and incorporates
them into the game. To include the EEG data in the
application, both headsets must be connected to the
MUSE Direct application via Bluetooth and the data
must be transferred via Open Sound Control (OSC)
using ports 7000 and 7001. UDP is used as the trans-
port protocol. The data retrieval within the Unity ap-
plication is realized with the help of the extOSC Unity
asset. The higher the concentration level, the larger
the radius of the light and the faster the players can
move. In order to find their way around the labyrinth,
the players have to train to control their concentration
and receive direct feedback based on the light. The
concentration level is required to increase the light ra-
dius. To exit a level, the players have to find and re-
member symbols that open the door to the next, more
difficult level. Every level has a time limit. Play-
Designing Neurogames to Support Patients under Psychotherapy Treatment: Opportunities and Challenges of the MUSE Headband
299

ers have to proceed carefully through the labyrinth,
to find and remember all necessary symbols to open
the exit gate. Each level has a time limit to add dif-
ficulty. In addition, the game aims to improve social
skills and teamwork, as the players have to cooper-
ate in order to advance to the next level. Working
together and pursuing a common goal can also have a
motivating effect on the players. Here, the users are
dependent on the performance of the other. They have
to agree on how they want to search through the lev-
els, tell each other when they have found certain ob-
jects within the labyrinth and help each other to find
the way. According to Wiemeyer et al. (Wiemeyer
et al., 2016), a common goal as well as mutual de-
pendency are required for cooperation and teamwork
to take place. By taking these aspects into account,
players should be encouraged to communicate and co-
operate with one another in the context of the serious
game. The control of the characters and interaction
with objects within the labyrinth is done by controller.
3.3 Technology Acceptance and Game
Experience
A total of N=21 healthy children were recruited to
participate in the first user test in a high school, in-
cluding n=13 male and n=8 female subjects. The age
of the test participants was 10 or 11 years. Subjects
had to play the game cooperatively for about 10 min-
utes and should think aloud. Afterwards they have
been given a questionnaire consisting of 30 items in-
cluding (1) general game preferences, (2) gameplay
and movement controls of the prototype (UTAUT -
Unified theory of acceptance and technology use), (3)
fun and replayability (GEQ-core - Game experience
questionnaire) and the (4) integration of concentration
measurement and influences on the gameplay (GEQ-
ig and GEQ-sp).
4 FINDINGS
4.1 Focus Group
Therapists (N=3) confirmed the need for digital ap-
plications to support the therapy of children and ado-
lescents against the background of the large number
of young patients and showed a largely positive at-
titude towards the use of digital media as a therapy-
accompanying measure. They stated that exercises
to promote mindfulness, relaxation, attention or con-
centration are often used as part of a therapy and
suggested that a therapy-accompanying serious game
could aim to promote one of these states of conscious-
ness. The results of the focus group were divided into
three therapeutic and learning objectives that a seri-
ous game supporting psychotherapy has to offer: (1)
Training of attention and concentration skills, (2) Pro-
motion of social and team skills and (3) Distraction
from counterproductive thoughts and support for psy-
chotherapy.
1. Training of attention and concentration skills:
The digital game has to be designed to train the
players’ attention and concentration skills in order to
teach children with a lack of concentration or atten-
tion deficit, to control their concentration in a targeted
manner and to maintain their attention over a longer
period of time. It should also help them to get into
a concentrated state (n=2). Furthermore, the mem-
ory skills of the players can be promoted in this con-
text (n=1). The digital prototype is also intended to
motivate users to deal with the increasingly complex
tasks within the game over a certain period of time
and thereby improve problem-solving skills (n=1).
2. Promotion of social and team skills: Since chil-
dren and adolescents with an attention disorder often
lack social relationships due to the symptoms of their
disorder and therefore have poor social skills and,
in some cases, suffer from social exclusion (n=3).
The digital prototype has to improve social skills
and teamwork among users promote to improve their
social behavior and meet social needs. Two sub-
jects (n=2) suggested to add a multiplayer mode in
which player can play together cooperatively (n=2)
and competitively (n=1).
3. Distraction from counterproductive thoughts
and support for psychotherapy: The game is also
intended to distract users from counterproductive
thoughts, praise them for successfully completing the
levels and thereby give them a sense of achieve-
ment, since children with ADHD often cannot com-
plete tasks successfully and suffer from emotional
problems (n=2). Furthermore, the digital application
should support the psychotherapy of the children and
motivate them to deal with therapeutic content, as
well as to carry out therapy-supporting exercises on
their own responsibility (n=2).
4.2 Prototype Gameplay Test
The gameplay questionnaire consisted of items in the
following categories: (1) general game preferences,
(2) gameplay and movement control of the prototype,
(3) fun and replayability, and (4) integration of con-
centration measurement and influences on the game-
play. The test took place in the regular school envi-
ronment of the subjects.
HEALTHINF 2022 - 15th International Conference on Health Informatics
300

Figure 1: Players must navigate through a dark labyrinth to find the exit to the next level. Depending on the concentration of
the player, areas surrounding the player are better illuminated.
4.2.1 General Game Preferences
It was found that the male participants (n=9) play
video games more often on average than the female
participants (n=3). Each of the male respondents said
they played a video game before. The majority of
them play one or more times a week (n=8). The ma-
jority of female respondents, on the other hand, play
video games less frequently, n=2 of the female par-
ticipants stated that they never played video games
before. The subjects cited spending time, fun and en-
tertainment as well as the opportunity to play with
others as motivations for playing. Approx. 81% of
those surveyed also stated that they preferred to play
together with others rather than alone. As part of the
evaluation, the data of the male and female subjects
as well as the experienced and inexperienced play-
ers were compared. All subjects who stated that they
used video games at least once a week were classi-
fied as experienced players. Subjects who rarely or
never play video games were classified as inexperi-
enced players.
4.2.2 Gameplay and Movement Controls
All subjects stated in the questionnaire that they un-
derstood the rules of the game quickly and well. 90%
of the children also said that they mostly or always
knew what to do. It showed that especially subjects
who play video games more often always knew what
to do. This can be attributed to the fact that these
subjects are already familiar with various game prin-
ciples and mechanics. Within the questionnaire, all of
the respondents also stated that they found nothing in
the rules of the game to be confusing. The control of
the characters and interaction by controller was rated
by all children as pleasant and easy as well as quick
to learn. Even players who said they had never used a
controller could quickly learn how to use it. The ma-
jority of respondents also believed that no improve-
ment in control was necessary. However, some of the
children said they preferred a narrower or a PlaySta-
tion controller.
4.2.3 Fun and Replayability
As part of the questionnaire, n=18 stated that they
liked the topic of the Egyptian treasure hunt very
much. All study participants also stated that they en-
joyed the game and would like to try again. When
asked what was the most fun and what they liked
best, n=8 answered with ”everything”, n=6 of the re-
spondents stated that they liked the search for objects
most within the labyrinth. During the performance of
the game tests, it was also observed that the subjects
were very happy when they found a stone tablet or
a treasure. Furthermore, n=4 stated that they found
the inclusion of concentration particularly good in the
game. Other favorite game aspects of the children
were memorizing the symbols, completing the levels
within a given time, playing together and communi-
cating with a teammate, the tension, uncertainty and
darkness, the graphics as well as the leaderboard as
feedback on their own performance. It was also ob-
served that the players were strongly motivated by the
score and the desire to score more points than another
team.
4.2.4 Integration of Concentration via the EEG
Within the questionnaire, the subjects were asked to
rate the comfort of the MUSE-EEG. The average of
those questioned stated that the EEG was “rather com-
fortable”. The experienced players rated the comfort
of the device on average as somewhat more pleasant
than the inexperienced players. This could be due to
the fact that experienced players are used to using dif-
ferent devices when playing video games and there-
fore have greater technology acceptance or are bet-
Designing Neurogames to Support Patients under Psychotherapy Treatment: Opportunities and Challenges of the MUSE Headband
301
ter able to put themselves in the game and thereby
hide the EEG. However, the game tests showed that
in some cases the EEG was too large for the chil-
dren’s head and therefore did not sit well or even
slip. 86% of the children stated that they were able
to concentrate mostly to very well while playing. It
turned out that the female test subjects were able to
concentrate better than the male ones in the question-
naire. The female test participants indicated on aver-
age that they were able to concentrate very well while
playing. The male participants were able to concen-
trate “mostly well” on average. This could be due to
girls’ penchant for riddle and puzzle games as well as
their innate abilities that give them an edge in such
games. However, there is the question of whether it is
a false self-assessment or whether the female partic-
ipants were actually able to concentrate better. This
cannot be checked on the basis of the recorded EEG
data either, since the recordings cannot be assigned to
the questionnaires.
5 DISCUSSION
The results show unique possibilities for designing
neurogames to support psychotherapy. The majority
of the children appeared very concentrated and im-
mersed in the game while the game tests were be-
ing carried out. It could be observed that the players
looked very carefully in the labyrinth and rarely over-
looked objects. In addition, the concentration level
of the test subjects was never permanently low. In-
dividual players were even able to maintain a consis-
tently high concentration. Some children were also
very proud when they were able to reach a high level
of concentration and communicated this to their team-
mate. The children judged the targeted control of the
light by the concentration in very different ways. Two
subjects found this to be difficult to very difficult, n=9
players rated the targeted control as simple to very
easy and n=10 children said ”it works”. Although
the female participants reported that they were able
to concentrate better than the male participants, the
evaluation of the targeted control of light through con-
centration showed no difference between female and
male test subjects. Instead, control by concentration
was judged by the experienced players on average to
be easier than by the inexperienced. This could be
attributed to the fact that the inexperienced players
also rated the game difficulty as more difficult and
that various actions in the game were more difficult
due to their less experience with game principles and
mechanics. However, a negative assessment of the
targeted control of the light by the concentration can
also be related to the fact that in some cases the EEG
slipped during the game or received no or only insuf-
ficient data for a short time, which represented a low
concentration level in the game. The average of the
respondents nevertheless stated that the control of the
light by the concentration was perceived as “rather not
frustrating” and also in the long term as “rather not
exhausting”. The female participants rated the per-
manent concentration as less strenuous than the male
participants and also stated that they felt less frustra-
tion. This could be due to a different frustration tol-
erance of the female and male subjects or related to
the fact that the female players felt they could con-
centrate better. The children were also asked within
the questionnaire whether they felt more concentrated
after playing than before. Here, n=18 of the respon-
dents stated that they had been more concentrated af-
ter playing. There were no differences between male
and female as well as experienced and inexperienced
players. Over the course of the game tests, it was
also observed that some children behaved loudly and
restlessly before playing, but appeared calm, concen-
trated and immersed in the game during play. To an-
alyze the concentration curve of the test subjects, the
gamma value shares of the players were saved dur-
ing the game sessions. An increased gamma value
indicates better concentration. It was found that the
gamma waves of the children were individually very
differently pronounced.
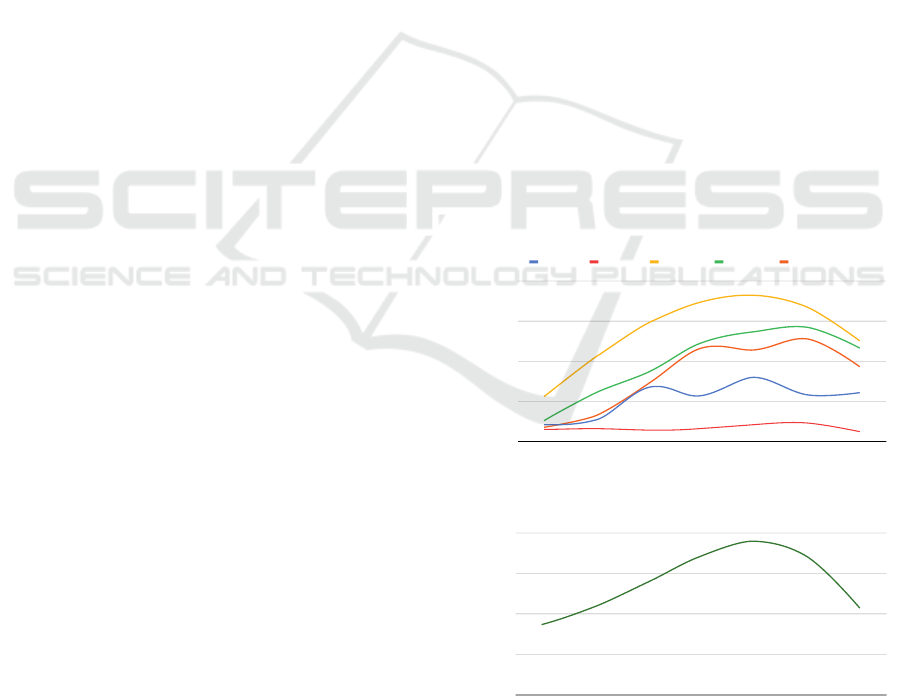
0
5
10
15
20
Start Intro Level 0 Level 1 Level 2 Level 3 Outro
Player 8 Player 9 Player 12 Player 18 Player 20
gamma value
Figure 2: Progression of the gamma value during the game
sessions by various players.
0
2
4
6
8
Start Intro Level 0 Level 1 Level 2 Level 3 Outro
gamma value
Figure 3: Average progression of the gamma value over all
players.
The average gamma value increase of the child
with the lowest values was approx. 1.7%, that of the
HEALTHINF 2022 - 15th International Conference on Health Informatics
302

child with the highest values was 13.7%. It was also
shown that the test subjects’ values fluctuated dur-
ing play. Overall, the gamma value percentage of all
players increased during the course of the game ses-
sion compared to the start of the game, indicating that
all children were able to increase their concentration.
However, this increase was different for each individ-
ual. Figure 2 shows a comparison of the gamma val-
ues of five different players during the game sessions.
For the average of the subjects, the gamma value pro-
portion increased continuously from the start of the
application up to level 2, where the values reached
their peak. Here the gamma values were on average
more than twice as high as at the beginning of the
game test, so the average of the children was most
concentrated in level 2. In level 3 as well as in the
outro, the gamma value decreases again on average.
The course of the average gamma value share of the
subjects is shown in figure 3.
While testing the game some problems with
MUSE were discovered. Due to the variation in head
sizes, a few subjects had problems tracking their EEG
data. The MUSE headband did not always fit the head
of a test person well. In addition, there were some dis-
connections of the MUSE headband during the game-
play tests, so the test subjects had to start from the
beginning.
6 CONCLUSION AND FUTURE
WORK
Through the implementation and evaluation of a pro-
totypical serious game, it is possible to show that a
playful, digital application offers the potential to sup-
port the psychotherapeutic treatment of children and
adolescents by motivating the users to independently
carry out exercises accompanying therapy. In addi-
tion, it was shown that the inclusion of measuring
neurofeedback in this context can help to support ex-
ercises in a self-effective way. Player are able to un-
derstand what concentration is all about and how this
can support therapy. As part of the evaluation, a suffi-
ciently large number of children were interviewed to
receive extensive feedback and clear results regard-
ing the prototype developed. Male and female test
subjects with different gaming experience and pref-
erences could be interviewed in order to capture the
opinion of different groups of people. Here, however,
the number of female participants was significantly
lower than the number of male participants. In addi-
tion, there were only two subjects who had no experi-
ence with video games and three test participants who
stated that they used video games on a daily basis.
In the context of the evaluation, it would have been
interesting to test a higher number of subjects with
no or extensive gaming experience in order to better
compare these groups of people with one another and
to be able to make generally valid statements about
these groups. In addition, subjects aged 10 or 11 only
were tested, which is why no statements can be made
about children in a different audience age. The goals
of the digital prototype were to train the players’ abil-
ity to pay attention and concentrate, to promote social
and team skills as well as to distract from counter-
productive thoughts and support psychotherapy. As
part of the user tests carried out, it was observed that
subjects who were initially restless and excited be-
came calmer during the session and concentrated on
the game. In addition, the recording of the gamma
values showed that the concentration of each subject
increased during the game, albeit to different degrees.
In order to be able to make further statements about
the course of concentration of the users while playing,
it would make sense to measure the brain activity of
the test subjects while performing other activities and
then to compare them with the brain activity while
playing the prototype. Some children found it diffi-
cult to concentrate and to control their concentration
in a targeted manner. Here the players need more in-
dividual support from the digital mentor, for example
through exercises or techniques to increase concen-
tration, which are taught during the game. The tests
also showed that the gamma values of the test partic-
ipants were very different. It is therefore important
that the game is based on the individual concentra-
tion values of the users and not on general values. As
part of the game tests, the prototype showed the po-
tential to promote the social skills and competences
of the children by playing together. Here it could
be observed that some children were calm and re-
served at the beginning of the game, but increasingly
communicated with each other during the game and
helped each other to find their way in the labyrinth.
All of the children surveyed stated that they enjoyed
playing with a teammate and enjoyed the cooperative
elements. It also confirmed that children can learn
from each other and motivate each other when play-
ing together. Consequently, it makes sense to let chil-
dren play a serious game together. The prototype is
intended to distract players from counterproductive
thoughts and motivate them to deal with therapeutic
content. All of the subjects stated that they had a lot
of fun with the game and wanted to play it repeatedly
during the game tests. Various game elements, such
as the use of the resources of time and points, con-
tribute to the motivation of the players and the ran-
dom generation of the labyrinths ensures the replay
Designing Neurogames to Support Patients under Psychotherapy Treatment: Opportunities and Challenges of the MUSE Headband
303

value. Consequently, a digital serious game offers
the potential to support the psychotherapy of children
and adolescents and to motivate them to deal with
therapeutic content, as well as to carry out therapy-
supporting exercises on their own responsibility. The
tests carried out also showed that feedback about their
performance was important to the children. It was
observed that they were motivated by the feedback
about their concentration and were proud when they
reached a high level of concentration. In addition,
the test subjects showed strong interest in the leader-
board, through which they were able to classify their
performance. As a result, there were positive effects
from the EEG-based feedback on the internal con-
dition of the children. A representation of the con-
centration curve could also be included in order to
give users more detailed and individual feedback. Al-
though different sources show that boys and girls have
different game preferences (Kinzie and Joseph, 2008;
Scharkow et al., 2015; Procci et al., 2011), the game
developed in this work was enjoyed by both male and
female testers. It was found here that by combining
action and puzzle elements, an application could be
developed that appeals to both genders. This confirms
the Procci et al. (Procci et al., 2011) that by mixing
game elements that correspond to the preferences of
boys and girls, a game can be developed that triggers
the interests of both genders. It also emerged that the
topic of Egyptian treasure hunt and the role of the ex-
plorer were welcomed by both boys and girls. As part
of the intro, it was observed that the children’s abil-
ity to read was at different levels and some of the test
subjects had problems reading the dialogue. Here it
would make sense to speak the text of the mentor to
relieve the children and avoid frustration. Animations
from the mentor can also be included to make them
appear more alive and to increase immersion. Fur-
thermore, the game tests revealed that some of the
children found aspects of the application to be too
difficult or too easy. This requires an adaptive level
of difficulty, which adapts individually to the skills
and performance of the children in order to maintain
a flow state and to neither bore nor overwhelm the
players. The testing of the prototype was carried out
with mentally healthy subjects. The next step is to
check whether people with a mental disorder still ben-
efit from the positive effects of the game. It is also
uncertain how long-lasting the motivation is to play
the prototype, and this should be tested in a long-term
study.
REFERENCES
Abeele, V. V., De Schutter, B., Geurts, L., Desmet, S.,
Wauters, J., Husson, J., Van den Audenaeren, L.,
Van Broeckhoven, F., Annema, J.-H., and Geerts, D.
(2011). P-iii: A player-centered, iterative, interdis-
ciplinary and integrated framework for serious game
design and development. In Joint Conference on Seri-
ous Games, pages 82–86. Springer.
Brezinka, V. and Hovestadt, L. (2007). Serious games can
support psychotherapy of children and adolescents. In
Symposium of the Austrian HCI and Usability Engi-
neering Group, pages 357–364. Springer.
Fernandez-Cervantes, V., Stroulia, E., Oliva, L. E., Gonza-
lez, F., and Castillo, C. (2015). Serious games: Re-
habilitation fuzzy grammar for exercise and therapy
compliance. In 2015 IEEE Games Entertainment Me-
dia Conference (GEM), pages 1–8. IEEE.
Fiałek, S. and Liarokapis, F. (2016). Comparing two com-
mercial brain computer interfaces for serious games
and virtual environments. In Emotion in Games, pages
103–117. Springer.
Forsner, M., Norstr
¨
om, F., Nordyke, K., Ivarsson, A., and
Lindh, V. (2014). Relaxation and guided imagery used
with 12-year-olds during venipuncture in a school-
based screening study. Journal of Child Health Care,
18(3):241–252.
Goldbeck, L. and Schmid, K. (2003). Effectiveness of auto-
genic relaxation training on children and adolescents
with behavioral and emotional problems. Journal of
the American Academy of Child & Adolescent Psychi-
atry, 42(9):1046–1054.
Graimann, B., Allison, B., and Pfurtscheller, G. (2009).
Brain–computer interfaces: A gentle introduction. In
Brain-computer interfaces, pages 1–27. Springer.
Hammond, D. C. (2011). What is neurofeedback: An up-
date. Journal of Neurotherapy, 15(4):305–336.
Heinrich, H., Gevensleben, H., and Strehl, U. (2007). An-
notation: neurofeedback–train your brain to train be-
haviour. Journal of Child Psychology and Psychiatry,
48(1):3–16.
Husky, M. M., Boyd, A., Bitfoi, A., Carta, M. G., Chan-
Chee, C., Goelitz, D., Koc¸, C., Lesinskiene, S., Mi-
hova, Z., Otten, R., et al. (2018). Self-reported mental
health in children ages 6–12 years across eight euro-
pean countries. European child & adolescent psychi-
atry, 27(6):785–795.
Jacob, A. and Teuteberg, F. (2017). Game-based learning,
serious games, business games und gamification–
lernf
¨
orderliche anwendungsszenarien, gewonnene
erkenntnisse und handlungsempfehlungen. In
Gamification und Serious Games, pages 97–112.
Springer.
Kinzie, M. B. and Joseph, D. R. (2008). Gender differ-
ences in game activity preferences of middle school
children: implications for educational game design.
Educational Technology Research and Development,
56(5-6):643–663.
Krigolson, O. E., Williams, C. C., and Colino, F. L. (2017).
Using portable eeg to assess human visual attention.
HEALTHINF 2022 - 15th International Conference on Health Informatics
304

In International Conference on Augmented Cognition,
pages 56–65. Springer.
Li, J., Theng, Y.-L., and Foo, S. (2014). Game-based digital
interventions for depression therapy: a systematic re-
view and meta-analysis. Cyberpsychology, Behavior,
and Social Networking, 17(8):519–527.
Liu, Y., Hou, X., Sourina, O., and Bazanova, O. (2016).
Individual theta/beta based algorithm for neurofeed-
back games to improve cognitive abilities. In Transac-
tions on Computational Science XXVI, pages 57–73.
Springer.
Mader, S., Levieux, G., and Natkin, S. (2016). A game de-
sign method for therapeutic games. In 2016 8th Inter-
national Conference on Games and Virtual Worlds for
Serious Applications (VS-GAMES), pages 1–8. IEEE.
Mu
˜
noz, J. E., Lopez, D. S., Lopez, J. F., and Lopez, A.
(2015). Design and creation of a bci videogame to
train sustained attention in children with adhd. In 2015
10th Computing Colombian Conference (10CCC),
pages 194–199. IEEE.
Naab, S., Kunkel, J., Fumi, M., and Voderholzer, U.
(2017). Psychosoziale risikofaktoren f
¨
ur psychische
st
¨
orungen im jugendalter. P
¨
adiatrie, 29(5):24–32.
Perales, F. and Amengual, E. (2017). Combining eeg and
serious games for attention assessment of children
with cerebral palsy. In Converging Clinical and En-
gineering Research on Neurorehabilitation II, pages
395–399. Springer.
Procci, K., Bohnsack, J., and Bowers, C. (2011). Patterns
of gaming preferences and serious game effectiveness.
In International Conference on Virtual and Mixed Re-
ality, pages 37–43. Springer.
Przegalinska, A., Ciechanowski, L., Magnuski, M., and
Gloor, P. (2018). Muse headband: Measuring tool or
a collaborative gadget? In Collaborative Innovation
Networks, pages 93–101. Springer.
Scharkow, M., Festl, R., Vogelgesang, J., and Quandt, T.
(2015). Beyond the “core-gamer”: Genre preferences
and gratifications in computer games. Computers in
Human Behavior, 44:293–298.
Scherer, R., M
¨
uller-Putz, G., Friedrich, E. V. C., Pammer-
Schindler, V., Wilding, K., Keller, S., and Pirker, J.
(2017). Games for bci skill learning. In Nakatsu,
R., Rauterberg, M., and Ciancarini, P., editors, Hand-
book of Digital Games and Entertainment Technolo-
gies, pages 173–196. Springer Singapore, Singapore.
Schoneveld, E. A., Lichtwarck-Aschoff, A., and Granic, I.
(2018). Preventing childhood anxiety disorders: Is
an applied game as effective as a cognitive behav-
ioral therapy-based program? Prevention Science,
19(2):220–232.
Sliwinski, J., Katsikitis, M., and Jones, C. M. (2017). A
review of interactive technologies as support tools
for the cultivation of mindfulness. Mindfulness,
8(5):1150–1159.
Sourina, O. and Liu, Y. (2015). Eeg-based serious games. In
Subconscious Learning via Games and Social Media,
pages 135–152. Springer.
Sourina, O., Liu, Y., Wang, Q., and Nguyen, M. K. (2011).
Eeg-based personalized digital experience. In Inter-
national Conference on Universal Access in Human-
Computer Interaction, pages 591–599. Springer.
Vigo, D., Thornicroft, G., and Atun, R. (2016). Estimating
the true global burden of mental illness. The Lancet
Psychiatry, 3(2):171–178.
Vourvopoulos, A., i Badia, S. B., and Liarokapis, F. (2017).
Eeg correlates of video game experience and user pro-
file in motor-imagery-based brain–computer interac-
tion. The Visual Computer, 33(4):533–546.
Wiemeyer, J., Nacke, L., Moser, C., et al. (2016). Player ex-
perience. In Serious Games, pages 243–271. Springer.
Wolpaw, J. R., Birbaumer, N., McFarland, D. J.,
Pfurtscheller, G., and Vaughan, T. M. (2002). Brain–
computer interfaces for communication and control.
Clinical neurophysiology, 113(6):767–791.
World Health Organization (2018). Mental health atlas
2017. World Health Organization.
Designing Neurogames to Support Patients under Psychotherapy Treatment: Opportunities and Challenges of the MUSE Headband
305
