
The Impact of Coping Classes toward Anxiety Level, and Coping
Ability during Labor
Runjati, Marsum, Sri Rahayu, Sri Wahyuni, Ida Ariyanti, Triana Sri Harjanti and Umaroh
Poltekkes Ministry of Health Semarang, Semarang, Indonesia
Keywords: Smart Mother Classes, Anxiety, Coping Ability, Labor.
Abstract: Backgrounds: Coping efforts carried out during pregnancy are very meaningful to influence pregnancy
outcomes and better birth, by minimizing or preventing negative influences from emotional, behavioral,
cognitive, and physiological responses.
Objectives: This study aims to analyze the impact of coping classes on anxiety levels and coping abilities
during labor.
Methods: This research was a type of experimental research design that used a Pre-test post-test control group
design. The samples were chosen randomly for 60 pregnant women who were given standard classes plus
coping classes and 60 pregnant women who were given standard pregnant mother classes which were carried
out in 12 clinics. Mother was given a class of 4 meetings. Measurements were taken three times before the
intervention, 4 weeks after the intervention, and during labor. This study used repeated ANOVA Post Hoc
LSD.
Results: The results showed that the score of anxiety in the intervention group at the second measurement
was lower as much as 0.896 (p = 0.502) and the score of anxiety during labor was lower as much as 0.563
(p = 0.683) than the control. The coping ability of the intervention group after the fourth week was higher by
1.740 (p = 0.284) and the coping ability of the intervention group at birth was higher by 3.942 (p = 0.030)
than the control group and the difference was significant.
Conclusion: The mother's classes Plus Coping Skills affect the level of anxiety, and coping skills during
delivery. Providing midwifery care uses continuity of care so that it can monitor and optimize preventive and
promotive effects.
1 INTRODUCTION
Pregnancy is a process that changes both physically
and psychologically for the mother (Hikmah et al.,
2019). Pregnancy is a major event in a woman's life,
not only affecting psychological, but also biological,
familial, and social domains (Lahti et al., 2017).
During pregnancy, there are significant changes
that can contribute to increased anxiety. (Corbijn van
Willenswaard et al., 2017) The prevalence of anxiety
disorders during pregnancy in developed and
developing countries is 10-25%.(Shahhosseini et al.,
2015) Meta-analysis of 102 studies found that the
prevalence of anxiety in pregnancy was 18.2% in the
first trimester and increased to 24.6% in the third
trimester.(Willenswaard et al., 2017) The results of
research in Indonesia stated that there were 26.4% of
*
Corresponding author
pregnant women experiencing anxiety (Hanifah &
Utami, 2019).
Pregnant women with anxiety during pregnancy
were shown to be three times more at risk of postnatal
depression and harmed the child's psychological
state. Anxiety conditions can increase the hormone
cortisol in utero so it is associated with impaired
cognitive development, behavioral problems, and
long-term emotions (Shrestha & Kd, 2018). In
addition, anxiety in pregnancy can affect the outcome
of childbirth (Zijlmans et al., 2017). Symptoms of
anxiety in pregnancy are related to the increased fetal
heart, fetal emergency, congenital malformation,
premature labor, and low body weight (Gejala &
Hasanjanzadeh, 2017; Shapiro et al., 2017; Yonkers,
K Hayden, K Forray, 2017). In Indonesia alone the
prevalence of Low Birth Weight (BBLR) is 6.2%
Runjati, R., Marsum, M., Rahayu, S., Wahyuni, S., Ariyanti, I., Harjanti, T. and Umaroh, U.
The Impact of Coping Classes toward Anxiety Level, and Coping Ability during Labor.
DOI: 10.5220/0010810000003347
In Proceedings of the 2nd International Conference on Psychological Studies (ICPsyche 2021), pages 159-166
ISBN: 978-989-758-580-7
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
159

(Kesehatan, 2018). Many bad consequences result
from maternal anxiety during pregnancy. Prevalence
is high, but a new study finds treatment rates are still
low (Kingston et al., 2017).
Pregnant women with anxiety have certain
characteristics and are affected by the environment.
Pregnant women with anxiety are influenced by
cultural background, tend to have a history of
infertility, unplanned pregnancies, and have low
psychosocial resources thus increasing anxiety. This
process can affect the mother, placenta, and fetal
systems especially when it occurs early in pregnancy
which is a sensitive period. (Dunkel Schetter &
Tanner, 2012) It is widely recognized that anxiety in
pregnancy can affect the neuro-endocrine
development of the fetus which will also affect the
emotional development of the fetus. (Olanike Busari,
2018) anxiety in pregnancy is also associated with
the incidence of short gestational age and fetal nerve
development. Mothers who experience anxiety may
also experience disorders during the postpartum
period (Dunkel Schetter & Tanner, 2012).
Anxiety during pregnancy is considered one of the
risk factors for fetal development because it can harm
the fetus related to prematurity, BBLR, childbirth
outcomes, and complications such as bleeding and the
risk of abortion. Anxiety levels will increase in the III
trimester of pregnancy. The anxiety is associated with
getting closer to the time of delivery. Facts show the
time approaching childbirth as a vulnerable condition
and trigger even feelings of fear for mothers who have
been pregnant before. These feelings of fear are more
likely to develop into anxiety (Nogueira & Alfenas,
2017).
Coping efforts carried out during pregnancy are
very meaningful to influence better pregnancy and
birth outcomes, by minimizing or preventing the
negative effects of emotional, behavioral, cognitive,
and physiological responses against stress. Coping
skills serve to select and implement appropriate
measures to cope with stress and as a defense resource
for pregnant women and children from the potentially
harmful effects of exposure to prenatal stress. A study
of coping skill training done on diabetes type 1
showed that coping skill training decreases
depression, anxiety, and stress among adolescents
with type 1 diabetes.(Edraki et al., 2018) Another
study that has done coping skill training during
pregnancy and measured after 4 weeks also showed
that coping skill training can decrease stress during
pregnancy and increase self-efficacy during
pregnancy.(Runjati et al., 2017) Coping responses are
associated with more favorable indicators of
psychological well-being. Coping during pregnancy
through positive assessment with an effort to create
positive meaning focused on personal development is
associated with better outcomes for mother and baby,
fewer depressive symptoms, and fewer problems in
pregnancy (Pakenham, KI; Smith A; Rattan, 2007).
In addition, one of the efforts to prevent problems
and complications during pregnancy is to increase the
knowledge of pregnant women and prepare for
childbirth, namely through classes for pregnant
women which are carried out on an ongoing
basis.(Emiyanti et al., 2017) The antenatal classes for
pregnant women are expected to better prepare
mothers psychologically and increase their
knowledge about pregnancy and the birthing process
so that it can help reduce maternal anxiety facing
childbirth. The study showed that physical and mental
changes caused by pregnancy, causing high levels of
stress, which is associated with adverse outcomes for
the mother and fetus and pregnant women require
coping strategies during pregnancy to combat these
created challenges. Coping with stress in mothers is
very important because it affects the mental health of
the mother and baby.
Other studies, especially on pregnant women,
have integrated mother classes activities with
maternal coping skills which allow mothers not only
to benefit from aspects of pregnancy and birth care
practices as well as postpartum and infant care but
also to help mothers with emotional aspects in dealing
with stress and confidence to face delivery during
pregnancy (Runjati et al., 2017), but the study that
integrated coping skill with mother classes stress have
not yet measured the mother's condition such as
anxiety and coping ability until the delivery process
by looking at the anxiety and coping ability outcome
when at labor process. This study aims to analyze the
impact of coping classes on anxiety levels and coping
abilities during labor
2 METHODS
This research is a type of research experimental
design. The design of this study used a pre-test post-
test control group design. The population in this study
were all primiparous pregnant women in the early 3rd
trimester (28-34 weeks gestation) at the Semarang
City Health Center that meet inclusion criteria as
normal pregnancy and exclusion criteria as a single
parent. The sampling method was cluster random
sampling for 12 public health centers from 35 public
health centers and then random allocation to be
experimental group and control group. The
experimental groups were given the combination of
ICPsyche 2021 - International Conference on Psychological Studies
160

coping skills and standard antenatal education
method ( n=60 ) pregnant women in 6 clinics and each
clinic 10 mothers chosen randomly from each clinic,
while the control groups were given only standard
antenatal classes( n=60) pregnant women at 6 clinics
and each clinic there were 10 mothers also chosen
randomly.
The Experimental groups were treated using
antenatal standard classes developed by the ministry
of health as a government program during antenatal
care and combine with coping skill education
developed by the previous study. The module of
antenatal classes has been developed by the ministry
of health as standard antenatal education as part of
antenatal care. While module of coping skill
education has been developed from previous research
and revised. (Runjati et al., 2017) Education classes
and coping skill classes were done four times in four
weeks and measured three times: before the
treatment, in the fourth weeks after the last treatment,
and during the delivery process for Anxiety and
coping ability during Labour.
The intervention was done by trained midwives
using the module of antenatal classes and the module
of coping skill education. The midwives who held
intervention groups were trained not only in antenatal
classes but also in coping skill education. While the
midwives who held the control group were trained
only in antenatal classes. The duration of the
intervention for each class for only standard antenatal
classes for 45 minutes and coping skill education for
45 minutes which the whole duration was about 1.30
minutes. The classes run four times for four weeks.
While The Control groups were given only
standard antenatal Classes four times in four weeks
and measured three times: before the treatment, in the
fourth weeks after the last treatment, and during the
delivery process for Anxiety and coping ability
during Labour. Pregnant women were measured
using anxiety scale instruments developed by a
previous study that has 26 questions with aspect
psychology and physiology with the result of validity
score was 0,366 s/d 0,764 P<0,05, and reliability sore
was 0,906. While the Instrument of coping ability
scale was developed also from a previous study with
37 Questions and the result of validity score was
0,337 s/d 0,683 P<0,05 P<0,05, and reliability score
was 0,906 (Sijangga, 2010).
This study using a different test to determine the
difference before and after treatment and the
difference in the mean of each measurement on the
anxiety variable, and Coping ability was measured at
the beginning, four weeks after the intervention, and
during the delivery. The analyzed data used the
repeated measured ANOVA test with Post Hoc LSD.
Ethical Clearance obtained from the Bioethics
Commission of the Faculty of Medicine, Sultan
Agung Islamic University Semarang number 510 /
VIII / 2019 / Bioethics Commission.
3 RESULT
The results of the different tests before the
intervention on the level of anxiety, and the ability to
cope during childbirth before treatment after four
weeks and during labor to see the difference between
the groups. The result pre-intervention between-
group showed the p-value on all variables showing a
p value> 0.05 so it was concluded that there was no
difference in the initial intervention in the two groups.
3.1
Proving the Effect of Maternity
Classes and Coping Skills on the
Anxiety of Pregnant Women during
Childbirth
The results are shown in Table 1 that the experimental
group that received standard classes plus coping skills
experienced a sharper decrease in the mean of anxiety
score. The different test was carried out between the
two groups based on the average change of each
group in three measurements, namely measurement 1
before treatment, measurement 2 was carried out at
week 4 after treatment and measurement 3 was
carried out at delivery using the Repeated ANOVA
test with post hoc LSD. The results of different tests
can be concluded that the class of pregnant women
plus coping skills can reduce the anxiety score of
pregnant women. The intervention groups at the
second measurement had an anxiety score of 0.896
which was lower than pregnant women who were not
given treatment/control but the difference was not
significant (p=0.502). It can be concluded that the
class of pregnant women plus coping skills can
reduce more the anxiety score of pregnant women
than control groups. While the score of anxiety at the
third measurement during labor was lower as much as
0.563 (p = 0.683) than the control group. It also can
be concluded that antenatal classes plus coping skill
education more reduced anxiety levels during labor
than control groups that were only given antenatal
classes even not significant.
Furthermore, Figure 1 showed that the
experimental group, the different test of Anxiety
scores before and after intervention on the fourth
weeks after the intervention and the third
The Impact of Coping Classes toward Anxiety Level, and Coping Ability during Labor
161
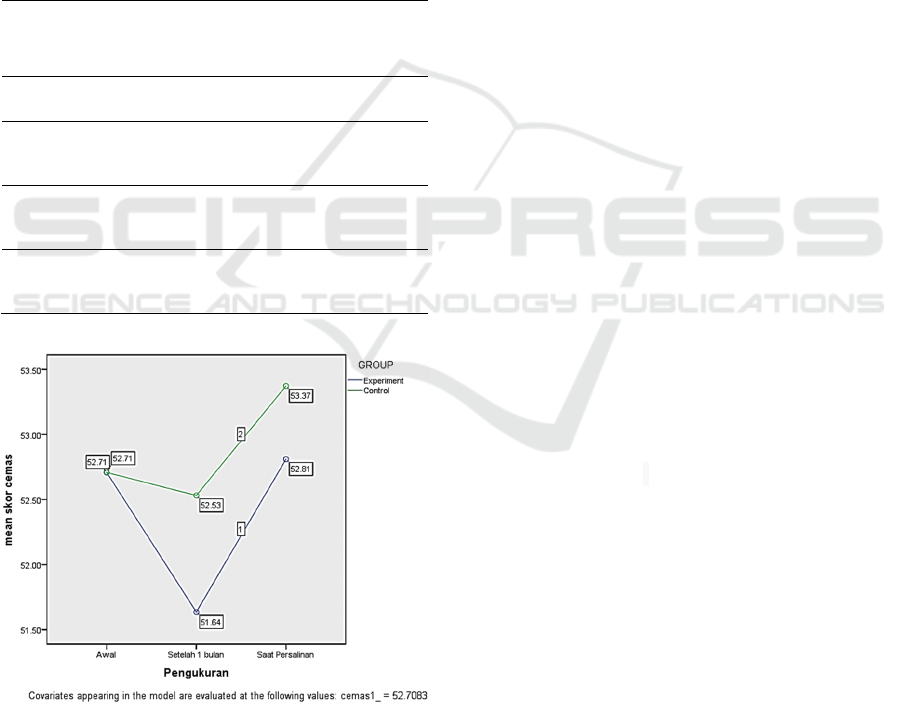
measurement at the time of delivery with the
Repeated measured Anova showed the mean score of
Anxiety before (52.71) and after the second
measurement (51.64) and the third measurement at
delivery (52.81) after the intervention. In the graphic
image, the anxiety score shows a decrease in the 2nd
measurement but at the time of delivery, it has
increased. In contrast in the control group the mean
score of Anxiety was before (52.71) and after the
second measurement (51.53) and the third
measurement at delivery (53.37). The graphic showed
that the intervention group had a trend of lower
anxiety levels at four weeks after intervention and
birth than the control groups.
Table 1: Differences in anxiety scores before and after
intervention by a group.
Group
Anxiety
Pre
Anxiety
Four weeks
P.
Anxiety
At labor
P.
mean ± SD mean ± SD
m
ean ± SD
Coping
Classes
53.23 ± 7,45 51.82 ± 7.66
52,93 ±
7,82
0,327
Standard
Classes
52.18± 9,86 52.35 ± 8.04
53,25 ±
4,62
0,630
Coping
Classes
-0.896 0.502 -0.563 0.683
pre vs post: Repeated Measured Anova, post hoc LSD
Figure 1: Anxiety score chart before and after intervention
in the experimental group (n=60) and the control group
(n=60).
3.2
Proving the Influence of Maternity
Classes and Coping Skills on the
Coping Abilities of Pregnant
Women and Childbirth
The results are shown in Table 2 that the experimental
group that received standard classes plus coping skills
experienced a sharper increase in the mean of coping
ability score. The different test was carried out
between the two groups based on the average change
of each group in three measurements, namely
measurement 1 before treatment, measurement 2 was
carried out at week 4 after treatment and measurement
3 was carried out at delivery using the Repeated
ANOVA test with post hoc LSD. The results of
different tests can be concluded that the class of
pregnant women plus coping skills can increase the
coping ability score of pregnant women. The
intervention groups at the second measurement had a
coping ability score of 1.740 which was higher than
pregnant women who were not given
treatment/control but the difference was not
significant (p=0.284). It can be concluded that the
class of pregnant women plus coping skills can
increase more the coping ability score of pregnant
women than control groups. While the score of
coping ability at the third measurement during labor
was higher as much as 3.942 (p = 0.030) than the
control group. It also can be concluded that antenatal
classes plus coping skill education more reduced
anxiety levels during labor than control groups that
were only given antenatal classes significantly during
labor. Interestingly the result of coping ability at the
third measurement of control groups during labor
showed a decrease significantly during labor while
the control group in contrast showed an increase
coping ability during labor even it was not significant.
Furthermore, The Changes in coping scores from
before the intervention in the first week to after the
intervention in the fourth week as well as changes in
the average coping scores at delivery are shown in
Figure 2. Figure 2 showed that the experimental
group, the different test of Anxiety scores before and
after intervention on the fourth weeks after the
intervention and the third measurement at the time of
delivery with the Repeated measured Anova showed
the mean score of coping ability before (117.78) and
after the second measurement (118.80) and the third
measurement at delivery (118.78) after the
intervention. It can be concluded from the graphic
image; the coping ability score shows an increase in
the 2nd measurement sharply but at the time of
delivery showed a slight decrease. In contrast in the
control group the mean score of coping ability showed
ICPsyche 2021 - International Conference on Psychological Studies
162

before antenatal education was (117.78) and after the
second measurement was decreased slightly (117.08)
and the third measurement at delivery showed the
coping ability was a decrease sharply (114.84). it can
be concluded from the graphic that the intervention
group had a trend increase of coping level at four
weeks after intervention and a slight decrease of coping
ability at birth than the control groups.
Table 2: Differences in Coping Scores before and after
intervention by a group.
Coping
ability
Pre
Coping
Ability
Four weeks
P.
Coping
Ability
At labor
P.
mean ± SD mean ± SD mean ± SD
Coping
Classes
116.17 ±
9.46
118.00 ±
9.71
118.02 ±
9.46
0.178
Standard
Classes
119.38±
10.16
117.87 ±
10.26
115.55 ±
11.62
0.045
Coping
Classes
1,740 0.284 3,942 0.030
pre vs post: Repeated Measured Anova, post hoc LSD
Figure 2: Coping score chart before and after intervention
in experimental group (n=60) and control group (n=60).
4 DISCUSSION
4.1
Proving the Effect of Maternity
Classes and Coping Skills on the
Anxiety of Pregnant Women during
Childbirth
The results of different tests can be concluded that the
class of pregnant women plus coping skills can
reduce the anxiety score of pregnant women ( 0.896
)which was lower than pregnant women who were not
given treatment/control but the difference was not
significant (p=0.502). furthermore, the score of
anxiety level during labor was lower as much as 0.563
(p = 0.683) than the control group.
Anxiety is a feeling of worry as if something bad
will happen and feeling uncomfortable as if there is a
threat. The more pregnancy the mother will feel more
anxious. Maternal anxiety is felt to increase due to
increased discomfort in pregnancy and also the
approaching labor process. A mother may feel fear of
the pain and physical danger that will arise at the time
of delivery.(H. Keliat et al., 2011) Anxiety and stress
during pregnancy are often overlooked when it is
important to pay attention. Midwives should
recognize anxiety and overcome it by providing
information and explanations about anxiety during
pregnancy and at the time of birth by providing
antenatal classes plus coping skill classes. The study
showed that anxiety during pregnancy and at birth can
influence the outcome of the health of the mother and
fetus and also the outcome of birth and after birth
during the postpartum period.(Blackmore et al., 2016)
increase anxiety during pregnancy also has a risk to
have a preterm birth.(Kartal & Oskay, 2017) It can be
also explained as a result of anxiety and fear, many
mothers experience more severe pain commonly
referred to as fear-tension-pain that influences the
outcome of birth. Fear causes anxiety so that muscles
become stiff and cause pain. (Sartika & Susilawati,
2021) So that emotional support is needed in
pregnancy and facing childbirth which can be
provided not only antenatal classes but also by
providing coping skill classes. Furthermore, health
care providers included midwives need to be sensitive
about the adaptation of active approach styles in
coping that are needed for pregnant women. The
combination of antenatal classes and coping skill
education provide more comprehensive information
and trained skilled how pregnant women overcome
the feeling of anxiety using problem-focused coping
and emotional-focused coping. The method of
problem-focused coping and emotional-focused
coping was trained in the experimental group to
provide the ability for mothers to overcome anxiety
during pregnancy and also manage feeling anxiety
facing labor and during labor. It is effectively that
manage anxiety could provide mothers cope better
with uncomforted feelings during pregnancy and at
birth.
Pregnant women express anxiety during their
pregnancy until the delivery process they will face
The Impact of Coping Classes toward Anxiety Level, and Coping Ability during Labor
163

and it causes stressors. The results showed that the
experimental group who received antenatal classes
and coping skill classes experienced a sharper
decrease in the mean anxiety score on the 2nd
measurement after 4 weeks compared with the control
group who received only standard antenatal classes.
Thus the results of the study are consistent that the
individual response to stressors in the form of anxiety
and times of anxiety is determined by coping, namely
oriented and intra-physical efforts to manage the
environment and internal needs as well as conflicts
regarding this matter. Furthermore, coping efforts can
affect birth outcomes by serving to minimize or
prevent negative emotional, behavioral, cognitive,
and physiological responses to stress. As a result, the
ability to select and implement appropriate coping
responses can serve as an endurance resource that
buffers pregnant women and their children from the
potentially harmful effects of prenatal anxiety and
stress exposure.(Guardino CM, 2015) Thus can be
concluded that coping skill education was useful to
provide pregnant women the ability to cope with
anxiety during facing labor by modification and doing
such positive behavior to minimize anxiety.
4.2
Proving the Influence of Maternity
Classes and Coping Skills on the
Coping Abilities of Pregnant
Women and Childbirth
The results showed in Table 2 that the experimental
group who received coping classes experienced a
sharper increase in the average coping ability after the
fourth week and the coping ability of the intervention
group at birth was higher than the control group and
the difference was significant.
Coping is a process in which individuals try to
find out the distance that exists between demands
(both demands that come from individuals and those
from the environment) and the resources they use in
dealing with situations that arise stress full.(Lazarus
RS, 1984; Taylor, 2015)
Coping strategy emphasizes
the effort or a process, where the individual tries to
resolve or deal with an event or events that are
considered stressful. The trick is to change his
cognition to control, tolerate, reduce, or minimize
pressure situations, to find a sense of
security.(Aldwin, 2007) the study showed that
coping skill education is more effective to train
mothers' ability to do coping during pregnancy and
labor. The coping ability is very important, based on
the study ability to cope with anxiety and stress
during pregnancy and labor was effective to
overcome the worst birth outcome(Kartal & Oskay,
2017; Sharon-David & Tenenbaum, 2017).
Furthermore, coping skill ability that was treated
during pregnancy integrated standard antenatal
classes was beneficial for mother not only has skills
pregnancy, birth and baby and postpartum care but
also ability to develop the coping ability to modified
some skill facing a delivery. The other research also
has proved that there was a high correlation between
coping ability with the stress of pregnant women. The
study also stated that better coping ability during
labor would result from a better outcome of
pregnancy and birth. (Sarani et al., 2016) It can be
concluded that mother who received antenatal classes
with coping skill classes has more skill ability to cope
better during pregnancy and facing labor and during
labor than mother only provided antenatal classes. A
previous study proved that better coping will decrease
stress during pregnancy and better outcomes of birth
and postpartum.(Goletzke et al., 2017) Coping ability
was found very useful trained during pregnancy as the
study found that women who have coping ability
better will have larger scores in self-efficacy and
carried out more coping behavior strategies during
labor. Pregnant women also had a more positive
evaluation of the childbirth experience and showed
significant gains in satisfaction after childbirth. It was
also needed assessment the level of confidence
women have in their ability to cope with the birth and
ability to have a vaginal birth. Furthermore, the study
also said that there were also need health care proved
should provide coping skill education to mothers so
that it can increase satisfaction with the childbirth
experience by helping to enhance self-efficacy and
coping in pregnant women (Report, 2017).
5 CONCLUSION
Based on the study result it can be concluded that
standard classes plus coping skills have a better
impact to decrease anxiety levels during pregnancy
and birth and improve coping ability during
pregnancy and birth.
The provision of midwifery care uses continuity
of care so that it can monitor and optimize preventive
and promotive efforts. In addition, it can provide
holistic and comprehensive care including bio,
psycho, social, and spiritual. For further researchers,
it is hoped that they can develop research on
psychological well-being in postpartum mothers and
child development.
ICPsyche 2021 - International Conference on Psychological Studies
164

ACKNOWLEDGMENTS
Thank you to pregnant women as well as midwives at
the clinic and PMB for their willingness to participate
in the research. Acknowledgments to Poltekkes
Kemenkes Semarang for providing funding for this
research.
REFERENCES
Aldwin, C. M. (2007). Stress, coping, and development: an
integrative perspective, 2nd edition (2nd editio). The
Guilford Press.
Blackmore, E. R., Gustafsson, H., Gilchrist, M., Wyman,
C., & G O’Connor, T. (2016). Pregnancy-related
anxiety: Evidence of distinct clinical significance from
a prospective longitudinal study. Journal of Affective
Disorders, 197, 251–258. https://doi.org/10.1016/
j.jad.2016.03.008
Corbijn van Willenswaard, K., Lynn, F., McNeill, J.,
McQueen, K., Dennis, C.-L., Lobel, M., & Alderdice,
F. (2017). Music interventions to reduce stress and
anxiety in pregnancy: a systematic review and meta-
analysis. BMC Psychiatry, 17(1), 271.
https://doi.org/10.1186/s12888-017-1432-x
Dunkel Schetter, C., & Tanner, L. (2012). Anxiety,
depression and stress in pregnancy: Implications for
mothers, children, research, and practice. Current
Opinion in Psychiatry, 25(2), 141–148.
https://doi.org/10.1097/YCO.0b013e3283503680
Edraki, M., Rambod, M., & Molazem, Z. (2018). The effect
of coping skills training on depression, anxiety, stress,
and self-efficacy in adolescents with diabetes: A
randomized controlled trial. International Journal of
Community Based Nursing and Midwifery, 6(4), 324–
333. https://doi.org/10.30476/ijcbnm.2018.40839
Emiyanti, Rahfiludin, M. Z., & Winarni, S. (2017). Analisis
Faktor-Faktor Yang Berhubungan Dengan
Keikutsertaan Kelas Ibu Hamil Januari-Juli Tahun
2017. Jurnal Kesehatan Masyarakat (e-Journal), 5(4),
801–811.
Gejala, D., & Hasanjanzadeh, P. (2017). Hubungan antara
ibu Umum dan Spesifik-Kehamilan Stres , Kecemasan ,
dan. 11(4), 4–7.
Goletzke, J., Kocalevent, R.-D., Hansen, G., Rose, M.,
Becher, H., Hecher, K., Arck, P. C., & Diemert, A.
(2017). Prenatal stress perception and coping strategies:
Insights from a longitudinal prospective pregnancy
cohort. Journal of Psychosomatic Research, 102, 8–14.
https://doi.org/10.1016/j.jpsychores.2017.09.002
Guardino CM, S. C. (2015). Coping during pregnancy : a
systematic review and recommendations. Health
Psychol., 8(1), 70–94. https://doi.org/10.1080/
17437199.2012.752659.Coping
H. Keliat, B. A., Wiyono, A. P., & Susanti. (2011).
Manajemen Kasus Gangguan Jiwa: CMHN
(Intermediate Course). EGC.
Hanifah, D., & Utami, S. (2019). The Associated Factors of
Antenatal Anxiety. 5, pISSN 2(01), 77–88.
Hikmah, N., Naimah, & Yuliani, I. (2019). Self Efficacy Ibu
Hamil Trimester III dengan Tingkat Kecemasan
menghadapi Persalinan. 5(2), 123–132.
Kartal, Y. A., & Oskay, U. Y. (2017). Anxiety, Depression
and Coping with Stress Styles of Pregnant Women with
Preterm Labor Risk. International Journal of Caring
Sciences, 10(2), 716–725.
Kesehatan, K. (2018). Hasil Utama Riskesdas 2018.
Kingston, D., Austin, M., & Zanten, S. V. Van. (2017).
Pregnant Women ’ s Views on the Feasibility and
Acceptability of Web-Based Mental Health E-Screening
Versus Paper-Based Screening : A Randomized
Controlled Trial Corresponding Author : 19, 1–18.
https://doi.org/10.2196/jmir.6866
Lahti, M., Braeken, M., Rooij, S. R. De, Hoyer, D.,
Roseboom, T., Katri, R., King, S., & Schwab, M.
(2017). Prenatal developmental origins of behavior and
mental health: the influence of maternal stress in
pregnancy. Neuroscience and Biobehavioral Reviews.
https://doi.org/10.1016/j.neubiorev.2017.07.003
Lazarus RS, F. S. (1984). Stress, appraisal, and coping. In
Behaviour Research and Therapy (Vol. 23, Issue 6).
spinger Publishing Company, Inc.
Nogueira, D. A., & Alfenas, U. F. De. (2017). Anxiety in
pregnancy : Prevalence and associated factors Anxiety
in pregnancy : prevalence and associated factors *.
September. https://doi.org/10.1590/s1980-220x201604
8003253
Olanike Busari, A. (2018). Multiple sclerosisPrevalence
and Associated Factors of Anxiety and Depression
Among Pregnant Women. Open Access Journal of
Neurology & Neurosurgery, 9(2).
https://doi.org/10.19080/OAJNN.2018.09.555758
Pakenham, KI; Smith A; Rattan, S. (2007). Application of
a stress and coping model to antenatal depressive
symptomatology. Psychology, Health, & Medicine,
12(3), 266–277.
Report, T. (2017). Self-efficacy , use of coping behavior
strategies and experience of childbirth in low-risk
pregnancy. June. https://doi.org/10.13140/RG.2.2.21
810.50883
Runjati, ., Susanto, H., Sawitri, D. R., & Thaufik, S. (2017).
The Effect of Antenatal Class Plus Coping Skill
Training on the Level of Stress and Childbirth Self-
Efficacy. Advanced Science Letters, 23(4), 3329–3333.
https://doi.org/10.1166/asl.2017.9125
Sarani, A., Azhari, S., Mazlom, S. R., Sherbaf, H., &
Aghamohammadian, M. (2016). The relationship
between coping strategies during pregnancy with
perceived stress level in pregnant mothers
10.22088/jbums.18.7.7. J. Babol Univ. Med. Sci, 18(7),
7–14. https://doi.org/10.22088/jbums.18.7.7.
Sartika, Y., & Susilawati, E. (2021). Pendampingan dan
Penerapan Modul Healing Touch Dalam Mengatasi
Kecemasan Pada Persalinan Oleh Bidan Klinik/Pmb
Di Kota Pekanbaru. 1(2), 1–6.
Shahhosseini, Z., Pourasghar, M., Khalilian, A., & Salehi,
F. (2015). A Review of the Effects of Anxiety During
The Impact of Coping Classes toward Anxiety Level, and Coping Ability during Labor
165

Pregnancy on Children ’ s Health. 27(April), 200–202.
https://doi.org/10.5455/msm.2015.27.200-202
Shapiro, G. D., Séguin, J. R., Muckle, G., Monnier, P.,
Fraser, D., Shapiro, G. D., Séguin, J. R., Muckle, G.,
Monnier, P., & Fraser, W. D. (2017). Sebelumnya
kehamilan hasil dan kecemasan kehamilan berikutnya
dalam kohort prospektif Quebec.
https://doi.org/10.1080/0167482X.2016.1271979
Sharon-David, H., & Tenenbaum, G. (2017). The
Effectiveness of Exercise Interventions on Coping with
Stress: Research Synthesis. Studies in Sport
Humanities, 22, 19–29. https://doi.org/10.5604/
01.3001.0012.6520
Shrestha, S., & Kd, P. (2018). Anxiety on Primigravid
Women Attending Antenatal Care : A Hospital Based
Cross-sectional Study. XX(X), 29–33.
Sijangga, W. N. (2010). Hubungan antara strategi coping
dengan kecemasan menghadapi persalinan pada ibu
hamil hipertensi.
Taylor, S. E. (2015). Health Psychology. In Journal of
Chemical Information and Modeling (Vol. 53). Mc
Graw-Hill Education.
Willenswaard, K. C. Van, Mcneill, J., Dennis, C., & Lobel,
M. (2017). intervensi musik untuk mengurangi stres
dan kecemasan dalam kehamilan : review sistematis
dan meta-analisis. 1–9.
Yonkers, K Hayden, K Forray, A. L. (2017). Association of
Panic Disorder, Generalized Anxiety Disorder, and
Benzodiazepine Treatment During Pregnancy With
Risk ofAdverse Birth Outcomes. 06510.
https://doi.org/10.1001/jamapsychiatry.2017.2733
Zijlmans, M. A. C., Beijers, R., Riksen-walraven, M. J., De,
C., Zijlmans, M. A. C., Beijers, R., Riksen-walraven,
M. J., & Weerth, C. De. (2017). Ibu akhir kecemasan
kehamilan dan stres dikaitkan dengan kesehatan anak-
anak : studi longitudinal. 3890. https://doi.org/10.1080/
10253890.2017.1348497
ICPsyche 2021 - International Conference on Psychological Studies
166
