
The Gammarana Intervention Succeeded in Restraining the Increase
in Stunting during the COVID 19 Pandemic in Enrekang, South
Sulawesi
Sirajuddin
1,2
, Saifuddin Sirajuddin
3
, Abdul Razak Thaha
3
, Amran Razak
4
, Ansariadi
5
,
Ridwan M. Thaha
6
, Purnawan Junadi
7
, Pungkas Bahjuri Ali
8
1
Doctoral Study Program, Faculty Public Health, Hasanuddin University, Indonesia
2
Department of Nutrition and Dietetic Health Polytechnic of Makassar, Indonesia
3
Department of Nutrition, Faculty Public Health Hasanuddin University, Indonesia
4
Department of Health Policy, Faculty Public Health Hasanuddin University, Indonesia
5
Department of Health Environment, Faculty Public Health Hasanuddin University, Indonesia
6
Department of Health Promotion, Faculty Public Health Hasanuddin University, Indonesia
7
Department of Hospital Administration, Faculty Public Health Indonesia University, Jakarta, Indonesia
8
The National Development Planning Agency, Jakarta Indonesia
Keywords: Stunting, COVID-19, Nutrition Intervention.
Abstract: Enrekang is the district with the highest prevalence of stunting in South Sulawesi. The Indonesian
government designated pilots for a stunting prevention convergence intervention project, called Gammarana.
The purpose of this study is to evaluate the impact of the program on stunting prevention during the COVID19
pandemic. The method is quasi-experimental. The intervention group was given macronutrient supplements,
micronutrient supplements, child feeding education and natural interventions. The control group was given
natural intervention (IFA-S, Antenatal Care and Growth Monitoring). The intervention group was located in
30 villages and the control group was 30 villages with similar socio-demography. Intervention for 6 months.
Results, stunting in the intervention group increased from 18.7% to 20.1% or 1.4%, while stunting in the
comparison group increased from 16.4% to 19.51% or 3.1%. Overall stunting increased from 17.7% to 19.9%
or 2.1%. The results of the Wilcoxon test showed that there was no change in stunting in the intervention
group (p=0.293) while in the comparison group it increased significantly (p=0.048) as well as overall
(p=0.016). Conclusion, The Gammarana intervention was able to restrain the rate of increase in the
prevalence of stunting during the COVID-19 Pandemic.
1 INTRODUCTION
Stunting has become a serious public health problem
in Indonesia. This is addressed on a regional basis,
especially in areas with a stunting prevalence of
>20%. The Indonesian government, especially South
Sulawesi, has established a focus area for stunting
prevention, one of which is the Enrekang District.
This district had a stunting prevalence of 48% in
2019, before the COVID-19 pandemic spread
(Kemenkes, 2018).
The problem at present is that there are no results
of an extensive, population-scale impact evaluation of
the intervention. This is required, because the track
record of sustainable interventions, is very useful to
be refined. The experience of a broad community-
based intervention is one of the potential lessons
learned from the experience that is very well imitated
(Haselow, Stormer și Pries, 2016),(Hossain et al.,
2017a)
The absence of efficacy studies of stunting
prevention interventions in Indonesia is due to the
absence of specific and sensitive nutrition
intervention packages designed in the perspective of
evaluation studies but generally designed and
implemented in the perspective of program
orientation alone. Several programs are implemented
as routine activities and their impact on stunting
reduction has not been specifically measured. Routine
program packages such as folic acid supplementation
for pregnant women and adolescent girls,
Sirajuddin, ., Sirajuddin, S., Thaha, A., Razak, A., Ansariadi, ., Thaha, R., Junadi, P. and Ali, P.
The Gammarana Intervention Succeeded in Restraining the Increase in Stunting during the COVID 19 Pandemic in Enrekang, South Sulawesi.
DOI: 10.5220/0010760000003235
In Proceedings of the 3rd International Conference on Social Determinants of Health (ICSDH 2021), pages 195-203
ISBN: 978-989-758-542-5
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
195

supplementary food supplementation for chronically
deficient pregnant women, high-dose vitamin A
supplementation for children aged five years, salt
iodization in endemic goitre areas, regulation of
mother's milk, surveillance for monitoring the growth
of children under five, and basic immunization
packages for children under five and pregnant
women. On the other hand, sensitive intervention
packages for both the agricultural and environmental
sectors have also been carried out throughout
Indonesia. (Beal et al., 2018),(Aryastami et al.,
2017), (Prawirohartono, Nurdiati și Hakimi, 2016).
Although the intervention package has been
carried out on a massive scale, there are very few
study reports that examine its impact on stunting
reduction. This fact needs to be explained as a result
through the evaluation of a large-scale stunting
prevention intervention program. The Government of
Enrekang Regency, South Sulawesi, has made a pilot
project of a comprehensive stunting prevention
approach involving a sensitive and specific approach
at the village level. Thirty villages were targeted for
intervention with an estimated stunting number of
2230 children and 120 pregnant women in 2020,
(Jeon et al., 2019),(Haselow, Stormer și Pries, 2016).
Based on the evidence base of other studies on the
impact of micronutrient supplementation,
macronutrients and nutritional literacy that are
aligned with improvements in environmental
sanitation, theoretically stunting will decrease by
around 4% per year. All of the above studies were
carried out under normal conditions(S. et
al.,2016),(Olney et al., 2018),(Gelli et al., 2018). The
results of the above study were then adopted as the
basis for implementing stunting prevention
interventions in Enrekang Regency, which is called
the local term Gammarana.
Gammarana, is a unique innovation in the stunting
prevention program, because it is based on evidence
from previous randomized studies, but also when the
new normal system was implemented in Indonesia.
Can this intervention package provide an alternative
to stunting prevention, when pressure from external
environmental factors due to the COVID-19
pandemic is increasing (Pérez-Escamilla,
Cunningham și Moran, 2020)? Access and services
were stopped in a direct form, but eventually,
adaptation was carried out so that stunting did not
increase further. (Akseer et al., 2020). This
evaluation study aims to analyze the impact of
Gammarana on stunting prevention in Enrekang
district when the COVID-19 pandemic has not ended.
2
METHODS
This study is quasi-experimental, investigating the
impact of Gammarna on stunting
2.1 Study Design
This study was conducted in 60 villages, 30 villages
as the intervention group and 30 villages as the
comparison group. The comparison villages had the
same characteristics (7 indicators) in aspects of food
security (p=0.111), agricultural land area ratio
(p=0.317), access to clean water (p=0.154), latrine
status, family planning (p=0.545), basic
immunization (p= 0.999), exclusive breastfeeding
(p=0.999), and growth monitoring (p=0.317) and
health insurance (p=0.999), these are presented in
other study reports (1). The duration of this study was
180 days, baseline and endline measured stunting
status, while the comparison of confounding variables
was controlled by selecting similar villages.
(Sirajuddin et al., 2021)
The intervention village was selected based on the
consideration of high stunting prevalence and has
been designated by the Enrekang district government
as a stunting focus village, while the comparison
village was chosen intentionally by the researchers
with the criteria, geographically being in one sub-
district, having similarities in 7 indicators to control
for confounding variables.
Another similarity between the two groups is
natural intervention, namely folic acid
supplementation for pregnant women, adolescent
girls, basic immunization for children under five,
supplementary feeding for pregnant women, chronic
lack of energy, and growth monitoring. The
difference with the intervention group is the
Gammarana intervention component.
ICSDH 2021 - International Conference on Social Determinants of Health
196
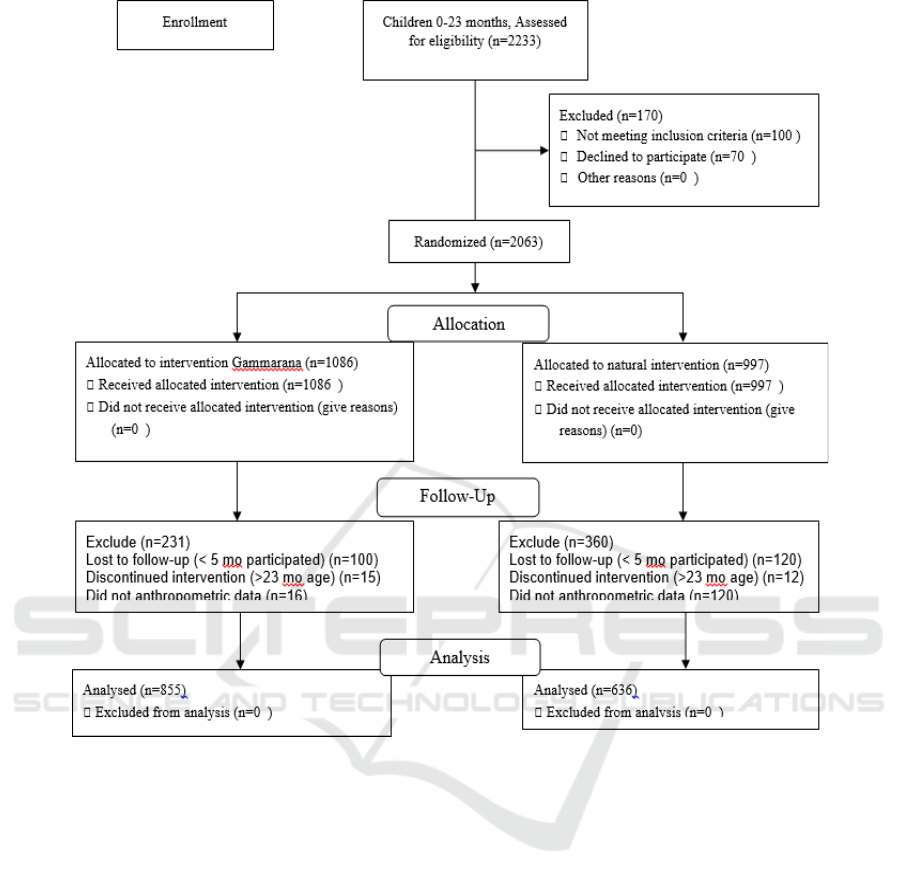
Figure 1. The Sample enrolled and finally analysed
2.2 Participants
2.2.1 Pregnant
Pregnant participants as targets who were given
protein supplementation, and Moringa capsules.
Pregnant is known based on the results of amenorrhea
history followed by a urine test. If it is declared
positive for pregnancy, then deregister as a subject.
This is done by the Midwife of the Health Center. The
total number of pregnant was 200 in the intervention
village and 100 in the comparison village. Of this
number who gave birth in the period August 2020 to
February 2021, 30 in the Intervention Village and 30
in the Comparison Village. This pregnant participant
was registered because the pregnancy outcome in the
form of birth height was the primary outcome
variable in this study.
2.2.2 Child 0-23 Months
Children aged 0-23 months were enrolled as subjects
in this study. An 855 out of 1086 in the intervention
village and 636 out of 997 in the comparison village.
Excluded children with birth defects, adopted
children from outside the region, down syndrome,
caregivers who did not participate in Gammarana, did
not record anthropometry (weight and height) at the
beginning and end of the program. Determination of
age based on birth certificate documents, calculated
in the full month method.
The Gammarana Intervention Succeeded in Restraining the Increase in Stunting during the COVID 19 Pandemic in Enrekang, South
Sulawesi
197

Table 1: Characteristic of the Subject Intervention and Control
Mean SD Mean SD Mean SD
Food security composite scores
3.83 1.34 4.20 1.27 4.02 1.31
0.111
The ratio of land for agriculture
0.16 0.32 0.08 0.06 0.12 0.23
0.317
The ratio of foo
d
p
roduction
0.07 0.03 0.08 0.04 0.07 0.04
0.393
The ratio of poverty quantile 1
0.06 0.03 0.05 0.02 0.06 0.03
0.034
Foo
d
Securit
y
Index
57.9611.04 61.129.33 59.5410.26
0.531
Access latrine (%)
91.369.20 89.2010.54 90.289.87
0.321
Access wate
r
treated (%)
94.785.79 92.9812.74 93.889.85
0.154
Famil
y
Plannin
g
(%)
18.3416.53 26.5223.76 22.4320.71
0.545
Delivery in health facilities (%)
80.1921.71 81.6330.16 80.9126.06
0.691
Basic immunization (%)
96.875.62 97.685.19 97.285.38
0.999
Exclusive
b
reastfeedin
g
(%)
93.2010.16 93.407.66 93.308.92
0.999
Growth monitorin
g
(%)
94.518.67 96.973.21 95.746.60
0.317
Health insurance Access (%)
47.6510.64 50.9811.15 49.3210.93
0.999
2.3 The Component of Gammarana
Their Component of intervention was Taburia
supplementation, Moringa extract capsule
supplementation, protein supplementation and
nutrition education. This was only given to the
Taburia is given to all children aged 6-23 months, the
response dose is 1 sachet / 2 days/child. How to give,
prepare children's food, separate 1/3 part, shake the
taburia, tear the package and sprinkle it on 1/3 of the
preparing the Taburia, continue to be breastfed for
those who are still breastfed. The total number of
sachets for each child is 90 sachets for 180 days, One
sachet = 1 g.
Provision Taburia to children is carried out by
skilled caregivers, through demonstrations and
simulations, guided by nutritionists, carried out by
skilled caregivers. Each village has 1 nutritionist
specifically for the Intervention village, while the
comparison village has no nutritionists in the village.
The nutritional contribution of each sachet (1 g) to
the Recommended Daily Allowance (RDA) (%) for
pregnant, age of 19-30 years, trimester 2, vitamins and
minerals is vitamin A (13.90), Bi1 (35,71), B2
(31.25), B3 (34.72), B6 (26.32), B12 (22.22), folic
acid (25.00), vitamin C (35.29), pantothenic acid
(50.00), Vitamin D3 (33.33), Vitamin E (400),
Vitamin K (36,36), Iodine (227,27), Iron (74,07), and
Zn (41,67) and selenium (68,97). Taburia has been
registered at the Center for Drug and Food Control No
SD 171250351, and LPPOM MUI: 01251097470214.
Intervention village, while the natural intervention
was not only given to the comparison village group
but also the intervention village.
2.3.1 Taburia Suplementation
separated food, mix well, try to consume this mixture
for <30 minutes, should not be mixed with soupy
foods and drinks, wash hands before and after.
2.3.2 Moringa Extract Capsule
Moringa extract capsules (MEC) were taken every
pregnancy, the response dose is 1 capsule per day
during pregnancy. The contribution of RDA (%)
Vitamin A (0.19), Vitamin E (2.93), Vitamin C
(2,55), Iron (2,00), Zinc (0,01) and selenium (0.24).
The MEC has been registered at the Center for Drug
and Food Control No TR203339021.
2.3.3 Proten Supplementation
Proten supplementation (PR) is given to all pregnant.
The response doses are one sachet every 2 days. The
method of preparation is to dissolve the PR powder in
warm or cold water according to the tastes of pregnant
women, 200 ml of water. Drink immediately < 30
minutes after preparation. The entire contents of one
sachet are made for one serving, cannot be divided
into two or more. Leftovers that are not used should
not be saved for the next gift but must open a new
bag. a sachet 52 g.
ICSDH 2021 - International Conference on Social Determinants of Health
198

Table 2: The impact of nutrition intervention on reducing stunting
Group
N
utritional Status
a
seline n(%)
E
ndline n(%)
D
elta n(%) Wilcoxon Test
P
-Value
Intervention Stunting 160 (18,7) 172 (20.1) 1.4 0.293
N
ormal 695 (81,3) 683 (79.9)
Total 855 (100) 855 (100)
Control Stuntin
g
104(16.4) 124(19.5) 3.1 0.048*
N
ormal 532(83.6) 512(80.5)
Total 636 (100) 636(100)
Total Stuntin
g
264 (17.7) 296 (19.9) 2.1 0.036*
N
ormal 1227 (82.3) 1195(80.1)
Total 1491 (100) 1491 (100)
Mann-Whitne
y
P-Value 0,238 0,767
*=significant <0,05, differences before –after for control (natural intervention) and across group
The provision of PR is carried out by pregnant
after skillfully preparing, guided by nutritionists in
each village. Nutritional contributions to the RDA
(%) of pregnant are energy (17.50), fat (14.86),
protein (27.4), carbohydrates (17), sodium (23.33),
calcium (24.89), vitamin A (1.90) B1 (117.14), B2
(29.38), B3 (19,19), B5 (43.33), B6 (120.53),
B7(2.6), Vitamin C (38.82), Selenium (75.86). and
Iron (22.22.) and Zinc (16.67). It is also given to
children aged 12-23 months who have not gained
weight. The response doses is sachet/day (25 g)
dissolved in 100 ml of cold or warm water. Giving is
carried out by skilled caregivers, guided by
nutritionists. Nutritional contributions to the RDA of
pregnant are energy (32,59), fat (22.22), protein
(33.33), carbohydrates (31.63), sodium (23.33),
vitamin A (4,28), B1 (328), B2 (156) , B3 (31.67),
B5 (130), B6 (458), B7(3.31), Vitamin C (82.50),
Selenium (122). and Iron (85,71). PR has been
registered with BPOM No: 862513022005.
2.3.4 Biscuits for Children
Biscuits for children (BFC) were given to children
aged 6-23 months in both groups. The duration of
administration was divided into two, namely wasting
toddlers <-2SD median WHO Anthro 2006 was given
for 1 month. Meanwhile, if wasting <-3SD is given
indefinitely until the nutritional status of the WHZ
score is at least -2SD. The response dose for each
administration is the age of 6-11 months given 8
pieces (80 g) per day, 12-23 months of age given 12
pieces (120 g) per day. Energy 160 kcal, 3.2-4.8 g
protein, 4-7.2 g fat. Enriched with 11 vitamins (A, D,
E, K, B1, B2, B5, B3, B16, B12) and 7 kinds of
minerals (Iron, Iodine, Zn, Calcium, Sodium and
Phosphorus. The provision of BFC is accompanied by
nutrition education by nutrition workers at the Public
Health Centres in the comparison villages and by
volunteer nutritionists in the intervention villages.
2.3.5 Biscuits for Pregnant
The Biscuit for Pregnant (BFP), given to pregnant. in
both groups. The dose of administration is 2
pieces/day for the first trimester, and 3 pieces daily @
20 g or 60 g / day for the second and third trimesters.
Energy 270 kcal, 6 g protein, 12 g fat. Enriched with
10 vitamins (A, D, E, K, B1, B2, B3, B16, B12) and
7 kinds of minerals (Iron, Iodine, Zn, Calcium,
Sodium and Phosphorus.
The duration of administration of BFP without
chronic energy deficiency (upper arm circumference
> 23.5 cm) is for 1 month, while for pregnant women,
upper arm circumference < 23.5 cm, is given during
pregnancy until it reaches >= 23.5 cm. Another
provision for the provision of biscuits to pregnant
women is that the provision of complete food remains
the main reference, while this package is only a
supplement.
2.3.6 Growth Monitoring
Growth monitoring (GM) is carried out once a month.
Measurement of body weight using an accuracy of 0.1
kg. Measurement of height using length board to the
nearest 0.1 cm. Measurements were taken at the
beginning and end of the intervention in both groups.
Enumerators who carry out measurements have been
trained in anthropometric techniques and are declared
eligible to carry out according to their competencies.
The measurement results are inputted into the Big
of Nutrition Surveillance Indonesia Data at each
location, according to the month of measurement. The
z-score was calculated using the WHO Anthro 2006
application. Extreme values + 6 SD were excluded
from the analysis. The index used is BAZ, HAZ and
WHZ.
The Gammarana Intervention Succeeded in Restraining the Increase in Stunting during the COVID 19 Pandemic in Enrekang, South
Sulawesi
199

2.3.7 Iron Folic Acid Supplementation
Iron Folic Acid supplement (IFA-S), given to
pregnant. Dosage response for prevention 90 tablets
during pregnancy. The contribution of folic acid and
iron respectively 60 mg (10%) and 0.25 mg (1%) to
Recommended Daily Allowance (RDA) of Indonesia.
2.3.8 Basic Immunization
Basic immunization (BI) provision for infants
younger than 24 hours. It giving hepatitis B
immunization (HB-0). 1 month age giving Bacille
Calmette Guerin
(BCG) and Poliomyelitis 1. Infants
aged 2 months giving of vaccine Diphtheria-Tetanus-
Pertussis (DPT) Haemophilus influenzae type b
(Hib1), poliomyelitis
-2, and Rotavirus. Infants aged
3 months: DPT-HB-Hib 2 and poliomyelitis 3. Infants
aged 4 months: DPT-HB-Hib 3, poliomyelitis
4.
2.3.9 Nutrition Education
Nutrition education (NE) is given to the caregivers,
by nutritionists in each village. The material given is
related to breast milk and complementary foods for
breastfeeding. Education is carried out twice a month
for 6 months, through home visits. Educational guide,
compiled and provided to every nutritionist.
2.4 Outcomes
Primary outcomes are the number and percentage of
stunting before and after the intervention, in
Gammarana and Comparative villages. Stunting is
known from the Z value of the 2006 WHO Reference
LAZ score. Values <-2 SD are called stunting. This
calculation uses the WHO Anthro 2005 software
version 3.2.2. Biologically implausible values LAZ -
6<LAZ>+5 and were excluded from the analysis.
The prevalence of stunting in this study was
calculated before and after the intervention for the
same subject (dependent). If the subject did not
complete the data at the beginning and at the end, then
he was excluded from the analysis. Analysis of
stunting changes using a paired test approach.
2.5 Sample Size
A total of 2333 children were enrolled, 170 were
excluded because their height was not measured at the
beginning of the screening so that the remaining 2063
were. These were then divided into two groups,
namely intervention 1086 and control 997. In the
intervention group, 231 were excluded because the
age was more than 23 months at the end of the
program. did the final measurement, because they did
not undergo the intervention for 5 months. In the
control group, 362 were excluded due to incomplete
anthropometry and out of the area. The final sample
size in the intervention group was 855 and in the
control group was 636.
2.6 Randomisation
Randomization, carried out at the level of selection of
the comparison village, after being selected, all
children in the village are registered as subjects and
then screened for age and willingness to participate.
In the intervention village, no randomization was
carried out because this village was selected from all
villages with the highest prevalence of stunting in the
Enrekang District of 30 so that there were 30
intervention villages and 30 comparison villages.
Allocation concealment mechanism was not done,
because controlling the mobility of subjects between
villages was not feasible.
2.7 Statistical Method
Stunting efficacy was tested from ordinal data on
stunting status before and after the intervention in
both groups. Test the normality of the data with the
Kolmogorov Test p = 0.000, so the Wilcoxon test was
used. Conversion from LAZ values to categorical
data follows, the following criteria: Stunting if the
LAZ value is <-2 SD, and Normal if >=-2 SD. There
are only 2 categories, namely stunting and normal.
Data analysis with SPSS 16.0. This study was
recognized by the Hasanuddin University Ethics
Committee
and registered with The Registry for
International Development Impact Evaluations
(5.24.2021).
3
RESULTS
During this 6-month study, the number of children
under five who intervened was 1086 in locus villages,
997 in non-locus villages. The coverage of children
changes every month, duo to the number of births and
leave over the age of 23 months do not compare.
Investigate of stunting efficacy interventions only
took place on children who were intervened for 6
months, excluded children who did not reach the 6-
month intervention. Does not reach because the age is
past 23 months and or the age has not reached 6
months. The number of eligible children is 855 in
Gammarana village and 636 in Non-Gammarana
ICSDH 2021 - International Conference on Social Determinants of Health
200

village (Figure:1)
The findings of this study show that in the
intervention group there was no change in stunting
proportion although increased by 1.4%. On the other
hand, in the control group, it was found that there was
a significant increase in stunting at (p=0.048) is 3.1%.
Due to this high increase, overall it is known that the
increase is 2.1% (p=0.036) (Table 2). Of course, this
finding proves that if there is an intervention, the
increase in stunting can be prevented, although the
reduction is still difficult to achieve because this study
used a two-paired sample, not an independent sample.
If the phenomenon is like this, then the
effectiveness of prevention in newborns is required.
If children were born from mothers who covered in
the Gammarana were able to reduce stunting, the
stunting population will decrease significantly. The
decline in this intervention is a decrease that is
triggered by the absence of new cases and vice versa,
newborns tend to have good nutritional status or are
not stunted.
4
DISCUSSION
The result of this study is that the Gammarana
intervention succeeded in restraining the rate of
stunting increase in the intervention village because it
only increased by 2.1% while in the comparison
village is increased by 3%. Unable to reduce stunting,
due to various factors that are thought to be indirectly
related to the condition of the COVID-19 pandemic,
in which access to basic health services was delayed
for several months before finally reopening at the end
of 2020 on a limited basis.
There are two approaches used in many studies,
namely independent samples and paired samples. If
the change in stunting is calculated based on the free
sample, then the design is cross-sectional twice at the
beginning and end. This has the advantage that
changes in the percentage of stunting are very
dynamic, especially in a small population. The
population will change according to the distribution
of birth age and stunting prevention efficacy. If the
efficacy is good and the birth rate is high, a real
reduction in stunting occurs even in a very short time.
The study in this study uses a paired sample model
so that the direction of change in stunting will focus
more on delaying new cases due to interventions in
subjects who have not been stunted effectively or not.
In stunted subjects, the ability to get out of this zone
is very difficult. This is related to the line of height
growth in children does not apply throughout the
year.
The experience of various studies in testing the
efficacy of stunting prevention through RCT studies
shows that if the intervention goes well, the reduction
is estimated to be >4% per year. Of course, the
intervention runs in a period of between 4-6 years.
This is a child's life cycle as a period of growth and
development. The difference with this study is that
here, it is a pilot program that continues to be
developed (Hossain et al., 2017b).
Similar studies to this study in Burkina Faso
(Lanou et al., 2019), (Fadnes et al., 2016) and
(Muhoozi et al., 2018), where there was no decrease
in stunting after the intervention, but also no increase
in stunting. On the one hand, this provides an
advantage because there is no increase in stunting
cases. This phenomenon is interesting to discuss
because various possibilities are unique to be
discussed. The first is that stunting rehabilitation is
very difficult, due to the accumulation of nutritional
deficiencies that have an impact on the ability to
absorb nutrients in the digestive tract. This is
associated with stunting as an indication of chronic,
not an acute deficiency. On the other hand,
inflammation increases demand but decreases
appetite. Recovery must be gradual and requires
patience on the part of the caregiver.
In addition, the studies reported by (Olney et al.,
2018), (Gelli et al., 2017), succeeded in reducing
stunting, because they not only managed to prevent
new cases but managed to rehabilitate stunting to
normal. This is especially found in cases of stunting,
the threshold difference between normal and mild
stunting, and the majority of the age is < 12 months.
This age still can increase in height between 10-23 cm
for one year, if nutritional intake meets the RDA. A
micronutrient enrichment base intervention with
maximal adherence control and coverage will find
results like this.
The limitation is that the coverage and adherence
to the intervention package are not optimal due to the
irregular supply of materials, which is caused by the
refocusing of the budget due to the pandemic.
However, this does not reduce the quantity and
quality of interventions at the end of the program,
because coverage can be maximized. This causes
some intervention packages to be given after the
program ends and after the follow-up program which
was not reported in this study.
The generalizability of this study is that
Gammarana can be replicated with noted
improvements in the timely mechanism of micro and
macronutrient packet administration. One way is that
Gammarana is continued in the second year in the
Enrekang districts and others in South Sulawesi. The
The Gammarana Intervention Succeeded in Restraining the Increase in Stunting during the COVID 19 Pandemic in Enrekang, South
Sulawesi
201

interpretation of the results of this study is that
stunting prevention must be evidence-based and
Gammarana provides a way out for the use of
macronutrient, micronutrient supplementation and
nutrition education intervention packages controlled
by nutritionists through home visits as educators.
The evidence in this study is consistent with the
results of studies in Burundi (Leroy, Olney și Ruel,
2018), Bangladesh (Mridha et al., 2016), Tanzania
(Locks et al., 2016), Burkina Faso (Lanou et al.,
2019), Mali (Adubra et al., 2019), Uganda (Carroll et
al., 2017). Although these studies are known to differ
from those of studies in Guatemala (Olney et al.,
2018), Bangladesh (Shafique et al., 2016), Malawi
(Gelli et al., 2018), Phipipina (Kandpal et al., 2016)
and Ghana (Kandpal et al., 2016), these differences
are not the main substance that renders the results of
these studies inapplicable. Each community group
has different determinants, so that modifications are
only needed on the context and mechanism side, but
do not differ on the underline side of the intervention
package. The strategy to overcome the differences in
context mechanism side, but do not differ on the
underline side of the intervention package. The
strategy to overcome the differences in context and
mechanism in each social unit of society is by
analyzing the right situation when the initial design of
the intervention control the implementation process
with an up to date approach. (Mirzoev et al., 2016),
(Jeon et al., 2019), (Lacouture et al., 2015). It takes
consistency and focuses from program
implementation. This can be done with the
cooperation of stakeholders as practitioners and
academics as independent reviewers who are free of
conflicts of interest.
5 CONCLUSIONS
Gammarana can suppress the rate of stunting increase
during the COVID-19 pandemic so that it can be
replicated in new areas.
ACKNOWLEDGEMENTS
Thank you, to the government of Enrekang District,
Faculty of Public Health Hasanuddin University and
Health Polytechnic of Makassar.
REFERENCES
Adubra, L. et al. (2019) „Conditional cash transfer and/or
lipid-based nutrient supplement targeting the first 1000
d of life increased attendance at preventive care services
but did not improve linear growth in young children in
rural Mali: Results of a cluster-randomized control",
American Journal of Clinical Nutrition, 110(6), pp.
1476-1490. DOI: 10.1093/ajcn/nqz238.
Akseer, N. et al. (2020) „COVID-19 pandemic and
mitigation strategies: implications for maternal and
child health and nutrition", The American journal of
clinical nutrition, 112(2), pp. 251-256. DOI:
10.1093/ajcn/nqaa171.
Aryastami, N. K. et al. (2017) „Low birth weight was the
most dominant predictor associated with stunting
among children aged 12–23 months in Indonesia",
BMC Nutrition, 3(1), pp. 1-6. DOI: 10.1186/s40795-
017-0130-x.
Beal, T. et al. (2018) „A review of child stunting
determinants in Indonesia", Maternal and Child
Nutrition, 14(4), pp. 1-10. DOI: 10.1111/mcn.12617.
Carroll, G. J. et al. (2017) „Evaluation of nutrition
interventions in children in conflict zones: A narrative
review", Advances in Nutrition, 8(5), pp. 770-779.
DOI: 10.3945/an.117.016121.
Fadnes, L. T. et al. (2016) „Effects of an exclusive
breastfeeding intervention for six months on growth
patterns of 4-5-year-old children in Uganda: The
cluster-randomised PROMISE EBF trial", BMC Public
Health, 16(1), pp. 1-10. DOI: 10.1186/s12889-016-
3234-3.
Gelli, A. et al. (2017) „Improving diets and nutrition
through an integrated poultry value chain and nutrition
intervention (SELEVER) in Burkina Faso: Study
protocol for a randomized trial", Trials, 18(1), pp. 1-16.
DOI: 10.1186/s13063-017-2156-4.
Gelli, A. et al. (2018) „Using a Community-Based Early
Childhood Development Center as a Platform to
Promote Production and Consumption Diversity
Increases Children's Dietary Intake and Reduces
Stunting in Malawi: A Cluster-Randomized Trial",
Journal of Nutrition, 148(10), pp. 1587-1597.
DOI:10.1093/jn/nxy148.
Haselow, N. J., Stormer, A. și Pries, A. (2016) „Evidence-
based evolution of an integrated nutrition-focused
agriculture approach to address the underlying
determinants of stunting”, Maternal and Child
Nutrition, 12, pp. 155-168. doi: 10.1111/mcn.12260.
Hossain, M. et al. (2017a) „Evidence-based approaches to
childhood stunting in low and middle-income countries:
A systematic review", Archives of Disease in
Childhood, 102(10), pp. 903-909. DOI:
10.1136/archdischild-2016-311050.
Hossain, M. et al. (2017b) „Evidence-based approaches to
childhood stunting in low and middle income countries:
A systematic review", Archives of Disease in
Childhood, 102(10), pp. 903-909. DOI:
10.1136/archdischild-2016-311050.
ICSDH 2021 - International Conference on Social Determinants of Health
202

Jeon, Y.-H. et al. (2019) „A pragmatic randomised
controlled trial (RCT) and realist evaluation of the
interdisciplinary home-based Reablement program (I-
HARP) for improving functional independence of
community-dwelling older people with dementia: an
effectiveness-implementation ", BMC Geriatrics, 19(1),
pp. 1-14. DOI: 10.1186/s12877-019-1216-x.
Kandpal, E. et al. (2016) „A Conditional Cash Transfer
Program in the Philippines Reduces Severe Stunting",
The Journal of Nutrition, 146(9), pp. 1793-1800. DOI:
10.3945/jn.116.233684.
Kemenkes (2018) „Basic Health Research Report of
Indonesia Year 2018”, Riskesdas 2018, pp. 182-183.
Lacouture, A. et al. (2015) „The concept of mechanism
from a realist approach: A scoping review to facilitate
its operationalization in public health program
evaluation", Implementation Science, 10(1), pp. 1-10.
DOI: 10.1186/s13012-015-0345-7.
Lanou, H. B. et al. (2019) „Micronutrient powder
supplements combined with nutrition education
marginally improve growth amongst children aged 6–
23 months in rural Burkina Faso: A cluster randomized
controlled trial", Maternal and Child Nutrition, 15(4),
pp. 1-13. DOI: 10.1111/mcn.12820.
Leroy, J. L., Olney, D. și Ruel, M. (2018) „Tubaramure, a
food-assisted integrated health and nutrition program,
reduce child stunting in Burundi: A cluster-randomized
controlled intervention trial", Journal of Nutrition,
148(3), pp. 445-452. DOI: 10.1093/jn/nxx063.
Locks, L. M. et al. (2016) „Effect of zinc and multivitamin
supplementation on the growth of Tanzanian children
aged 6-84 wk: A randomized, placebo-controlled,
double-blind trial", American Journal of Clinical
Nutrition, 103(3), pp. 910-918. DOI:
10.3945/ajcn.115.120055.
Mirzoev, T. et al. (2016) „Study protocol: Realist
evaluation of effectiveness and sustainability of a
community health workers programme in improving
maternal and child health in Nigeria", Implementation
Science, 11(1), pp. 1-11. DOI: 10.1186/S13012-016-
0443-1.
Mridha, M. K. et al. (2016) „Lipid-based nutrient
supplements for pregnant women reduce newborn
stunting in a cluster-randomized controlled
effectiveness trial in Bangladesh", American Journal of
Clinical Nutrition, 103(1), pp. 236-249. DOI:
10.3945/ajcn.115.111336.
Muhoozi, G. K. M. et al. (2018) „Effects of nutrition and
hygiene education on oral health and growth among
toddlers in rural Uganda: follow-up of a cluster-
randomised controlled trial", Tropical Medicine and
International Health, 23(4), pp. 391-404. DOI:
10.1111/tmi.13036.
Olney, D. K. et al. (2018) „PROCOMIDA, a food-assisted
maternal and child health and nutrition program,
reduces child stunting in Guatemala: A cluster-
randomized controlled intervention trial", Journal of
Nutrition, 148(9), pp. 1493-1505. DOI:
10.1093/jn/nxy138.
Pérez-Escamilla, R., Cunningham, K. și Moran, V. H.
(2020) „COVID-19 and maternal and child food and
nutrition insecurity: a complex syndemic", Maternal
and Child Nutrition, 16(3), pp. 8-11. DOI:
10.1111/mcn.13036.
Prawirohartono, E., Nurdiati, D. și Hakimi, M. (2016).
Prognostic factors at birth for stunting at 24 months of
age in rural Indonesia", Paediatrica Indonesiana, 56(1),
p. 48. DOI: 10.14238/pi56.1.2016.48-56.
S., S. et al. (2016) „Mineral- and vitamin-enhanced
micronutrient powder reduces stunting in full-term low-
birth-weight infants receiving nutrition, health, and
hygiene education: A 2 3 2 factorial, cluster-
randomized trial in Bangladesh", American Journal of
Clinical Nutrition, 103(5), pp. 1357-1369. DOI:
10.3945/ajcn.115.117770.
Shafique, S. et al. (2016) „Mineral- and vitamin-enhanced
micronutrient powder reduces stunting in full-term low-
birth-weight infants receiving nutrition, health, and
hygiene education: A 2 3 2 factorial, cluster-
randomized trial in Bangladesh", American Journal of
Clinical Nutrition, 103(5), pp. 1357-1369. DOI:
10.3945/ajcn.115.117770.
Sirajuddin, S. et al. (2021) „It has no impact but is useful as
a lesson learned from the Gammarana Enrekang
stunting prevention project during the COVID-19
pandemic”, Annals Romanian Society Biology Cell,
25(6), pp. 4723-4728.
The Gammarana Intervention Succeeded in Restraining the Increase in Stunting during the COVID 19 Pandemic in Enrekang, South
Sulawesi
203
