
Dietary Assessment of Children under Five using Calculator of
Inadequate Micronutrient Intake (CIMI) Approach Study Case in
Pandeglang, Banten Province Indonesia
Fetriyuna
1,2
a
, May Susandy
1
and Ratna C. Purwestri
2
b
1
Department of Food Technology, Faculty of Agro-Industrial Technology, Universitas Padjadjaran, Jln. Raya Bandung-
Sumedang Km. 21 Jatinangor, Kab. Sumedang 45363, Indonesia.
2
Institute for Nutritional Science (140a), University of Hohenheim, Garbenstrasse 30, 70599 Stuttgart, Germany
Keywords: CIMI, Micronutrient Intake, Dietary Assessment, Food Groups, Daily Intake
Abstract: Calculator of Inadequate Micronutrient Intake (CIMI Apps) is software to determine the energy, protein, and
micronutrient intakes based on regional dietary patterns. CIMI apps is use to calculate the absolute intake of
energy, macronutrients, retinol, ß-carotene, retinol equivalents, iron, and zinc. CIMI represents an informative
dietary assessment tool to detect nutrient gaps concerning local eating habits based on the food group
classification. Data of 24-hours recall from food intake of 110 respondents of children under five from
Pandegelang district, Banten Province Indonesia was analyzed using CIMI. The result was the percentage of
nutrients covered through the daily diet of the Children. The dietary pattern in that region is characterized by
starchy food (72%), vegetables (12%), and fruits (7%). In addition, a considerable amount of fish and meat
were consumed and a very low portion of dairy products. Every second of children had inadequate
consumption of energy (55.2 %), iron (50%), zink (53%) and almost all the children have inadequate
consumption of vitamin A (98%). The calculation using CIMI delivered information, that on average, the
children’s needs of energy, iron, and zinc were insufficiently fulfilled through their daily intake and extreme
deficiency in the supply of proteins and vitamin A (retinol).
1 INTRODUCTION
The prevalence of undernutrition in Indonesia
remains at a very high level. Based on the report of
Basic Health Research (Badan Penelitian dan
Pengembangan Kesehatan. Kementerian Kesehatan
RI, 2007, 2013 and 2018), the prevalence of stunting
among children under five years of age in Indonesia
were in the range of 30.8% - 36.8%). The proportions
were higher than the whole of Southeast Asia (25.7%)
and even the prevalence globally (22.2%) (UNICEF,
WHO and World Bank Group, 2018) while wasting
is about 10.2% – 13.6% and underweight is at 17.7–
18.4 %. Some programs have been done to overcome
undernutrition through vitamin A supplementation
for children and pregnant women, fortification of
commonly consumed foods, and promotion of
increasing the intake of vitamin and mineral-rich
a
https://orcid.org/0000-0001-6735-0724
b
https://orcid.org/0000-0001-5892-4749
foods (ICN2, 2014; Kemenkes RI, 2018; Budiastutik
and Nugraheni, 2018; The SMERU Research
Institute, 2015). Unfortunately, they still need
innovations that can adapt to the specific situation in
Indonesia.
All age groups can be affected by malnutrition,
whereas infants, young children, and pregnant or
lactating women are the most nutritionally vulnerable
groups because of their high physiological and
nutritional requirements. Malnutrition by means of
undernutrition mostly affects children under the age
of five because of their more demanding dietary
requirements. Undernourishment in childhood could
affect the overall cognitive development, school
performance, lifetime earnings, and vulnerability to
infectious and chronic diseases in adulthood (higher
risk of death and illness) (Global Panel on Agriculture
and Food Systems for Nutrition., 2016).
64
Fetriyuna, ., Susandy, M. and Purwestri, R.
Dietary Assessment of Children under Five using Calculator of Inadequate Micronutrient Intake (CIMI) Approach Study Case in Pandeglang, Banten Province Indonesia.
DOI: 10.5220/0010758600003235
In Proceedings of the 3rd International Conference on Social Determinants of Health (ICSDH 2021), pages 64-69
ISBN: 978-989-758-542-5
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

Malnutrition (which by means undernutrition) is
usually correlated with insufficient consumption of
nutritious food especially micronutrient deficiencies
(FAO, 1992; Stewart CP, Iannotti L, Dewey KG,
2013; World Health Organization and UNICEF,
2019). Micronutrient deficiencies are believed to
cause more detrimental effects on physical and
cognitive development compared with a calorie
deficit and also creates irreversible of failure growth.
Indonesia has plenty of local food resources,
including numerous tubers, cereals, beans, fruits and
vegetables. Due to the lack of information on the
potential uses and the nutrient contents and the stigma
of being inferior foods, some of them are
underutilized. Many of the underutilized foods are
gaining popularity nowadays because they have
nutritionally rich compounds, which can be used to
combat malnutrition and food and nutrition insecurity
(Durst and Bayasgalanbat, 2014) and (Dandin and
Kumar, 2016).
Food security includes food accessibility and food
availability, was proven to correlate with the
prevalence of stunting in Indonesia ((The SMERU
Research Institute, 2015) and (BMKG, Kementan,
BNPB, LAPAN, BPS, 2017). Data about food
consumption is needed to ensure the possible driven
factors of undernutrition in Indonesia. Table 1
presents the recommendation of nutrients intake of
some of the essential macro and micronutrients for
children up to 6 years old in Indonesia.
To assess the nutritional condition and predict the
micronutrient deficiency, an express instrument is
needed. Calculator of Inadequate Micronutrient
Intake (CIMI Apps) has been used for the rapid
assessment of micronutrient deficiencies in several
countries like Ethiopia (Bosha, Lambert, Riedel,
Gola, et al., 2019; Bosha, Lambert, Riedel, Melesse,
et al., 2019), Ghana (Philipp et al., 2019) and
Indonesia (Radix et al., 2014). This method has
advantages compared to clinical testing for blood or
urine assay which takes a relatively long time and the
action cannot be carried out directly on site.
Table 1. Recommended Nutrient Intake (RNI) Children
Under Five in Indonesia.
Nutrition Unit
Recommended Nutrient Intake
(RNI)
0-6
months
7-11
months
1-3 years
4-6
years
1 Energy kcal 550 725 1125 1600
2 Protein g 12 18 26 35
3 Vitamin A mcg 375 400 400 450
4 Fe mg 2.5 7 8 9
5 Iodine mcg 90 120 120 120
6 Zink mg 2.75 3 4 5
(Ministry of Health RI, 2013)
To assess the nutritional condition and predict the
micronutrient deficiency, an express instrument is
needed. Calculator of Inadequate Micronutrient
Intake (CIMI Apps) has been used for the rapid
assessment of micronutrient deficiencies in several
countries like Ethiopia (Bosha, Lambert, Riedel,
Gola, et al., 2019; Bosha, Lambert, Riedel, Melesse,
et al., 2019), Ghana (Philipp et al., 2019) and
Indonesia (Radix et al., 2014). This method has
advantages compared to clinical testing for blood or
urine assay which takes a relatively long time and the
action cannot be carried out directly on site.
2 METHODOLOGY
Food consumption of 24-h recall was collected from
the respondent of children under five and the data was
entered into the Calculator of Inadequate
Micronutrient Intake (CIMI) program to calculated
the amount of energy intake, protein, carbohydrate,
fats, iron, zinc, pre-formed vitamin A, carotenoids,
retinol equivalents (RE) with a carotenoid conversion
factor of 1:6 or 1:12 and percent of total energy
intake. The individual data will automatically
generate. Percent of the recommended intake of
energy, protein, iron, zinc, and vitamin A intake were
calculated based on the FAO/WHO age- and sex-
specific RNI (Jati et al., 2014).
The data were analyzed using SPSS statistics 22
(IBM, Armonk, NY, USA). The general level of
significance was set at p < 0.05. The results are
expressed in percentages or means-SD/median. Tests
applied were the Kolmogorov–Smirnov test, the
student's t-test/Mann–Whitney test, and univariate
ANOVA/Kruskal–Wallis test.
In order to ascertain amongst which groups a
significant difference was found, the Duncan posthoc
test was performed, or in case of non-normal data the
Mann–Whitney test with subsequent correction of the
Dietary Assessment of Children under Five using Calculator of Inadequate Micronutrient Intake (CIMI) Approach Study Case in
Pandeglang, Banten Province Indonesia
65

alpha inflation (cumulative Type I error) according to
Bonferroni. To elucidate associations between two
continuous variables, the Pearson/Spearman
correlation was applied. Sets of categorical data were
assessed by Pearson's chi-square test or Fisher's exact
test.
2.1 Ethics Approval and Consent to
Participate
As part of the research about the nutritional condition
of children under five in Banten, the study conformed
to the provisions of the Declaration of Helsinki in
1995 (as revised in Edinburgh 2000). Eligible
children were included only on the basis of the
informed consent of their caretakers. The baseline
study is registered with the study code No:
840/UN6.C.10/PN/2017 at the Health Research
Ethics Committee Faculty of Medicine Universitas
Padjadjaran Bandung, Indonesia (July 28
th
, 2017) and
approved by the Badan Kesatuan Bangsa dan Politik
(Board of national and political unity) code No:
070/160-kesbangpol/2017 (Oct 2
nd
, 2017). Before
enrolment, a full explanation of the study purpose was
given to the communities, and informed consent was
obtained either by signature or thumbprint.
3 RESULT AND DISCUSSION
The study was conducted from 7
th
October 2017 until
13
th
October 2017 in two villages Kadomas and
Kalanganyar of Banten Province Indonesia. The data
was collected from a total of 105 children (aged 7-61
months) of 56 (53.3%) boys and 49 girls (46.7%). In
regard to the data collection of 24-h recall, 105
caretakers participated. The main caretakers were
mothers (78.2% with 14 are single parents), followed
by 18.1 % grandparents and aunty or other relatives
(3.7 %). Around 53.3% of children recruited in this
study were boys. The majority (76.2%) of the
children lived in a nuclear family.
The age of the children (n = 105) was, on average
31.6 ± 16.0 months at baseline with no significant
difference in the age distribution between both sexes.
The data about the nutritional condition of children
under five were explained in another paper.
3.1 Dietary Intake of The Children
Data of 24-h recall of children under five were
collected during the household visit and the
mother/caretakers were helped to fill the form with
the illustration to predict the total consumed foods.
Table 2 presents the percentage fulfillment of nutrient
consumption which is processed with CIMI apps
from data of 24-h recall. Every second of children
have inadequate consumption of energy (45%),
micronutrient of iron (50%), Zink (53%) and almost
all the children have inadequate consumption of
vitamin A (98%).
There were no differences in consumption
between gender except for iron (p=0.000). The
consumption of energy is not significantly different
among of age group (p=0.19), while shown to a
significant difference for micronutrient iron and zinc
(p=0.000). The inadequate consumption of Iron is
significantly increasing by the age of children, it is
shown that the drastic increase from the age group of
1-2 years to age group 2-3 year from 9% into 21%.
Similarly, with the zinc, or the same age group, the
inadequate consumption increasing from 10% up to
22% in children age 2-3 years. All the age group has
the high level of inadequate consumption of vitamin
A, with the highest of the age group 2-3 years as 28%.
Table 3 presents the fulfillment of nutrients based on
gender and age group of children under five.
The result also confirmed the Fe deficiency was
observed in 4.1–8.8% of the children, the percentage
of children with dietary intakes of energy, protein,
and vitamins A below the Indonesian RNI was high
and differed across urban and rural areas and age
groups (The SMERU Research Institute, 2015;
United Nations Children’s Fund (Unicef), 2018). The
same finding was also funded in India (Meshram et
al., 2012) the health problem among tribal children in
India are associated with food security, food intake,
socioeconomic condition, literacy of parents, and
personal hygiene.
ICSDH 2021 - International Conference on Social Determinants of Health
66
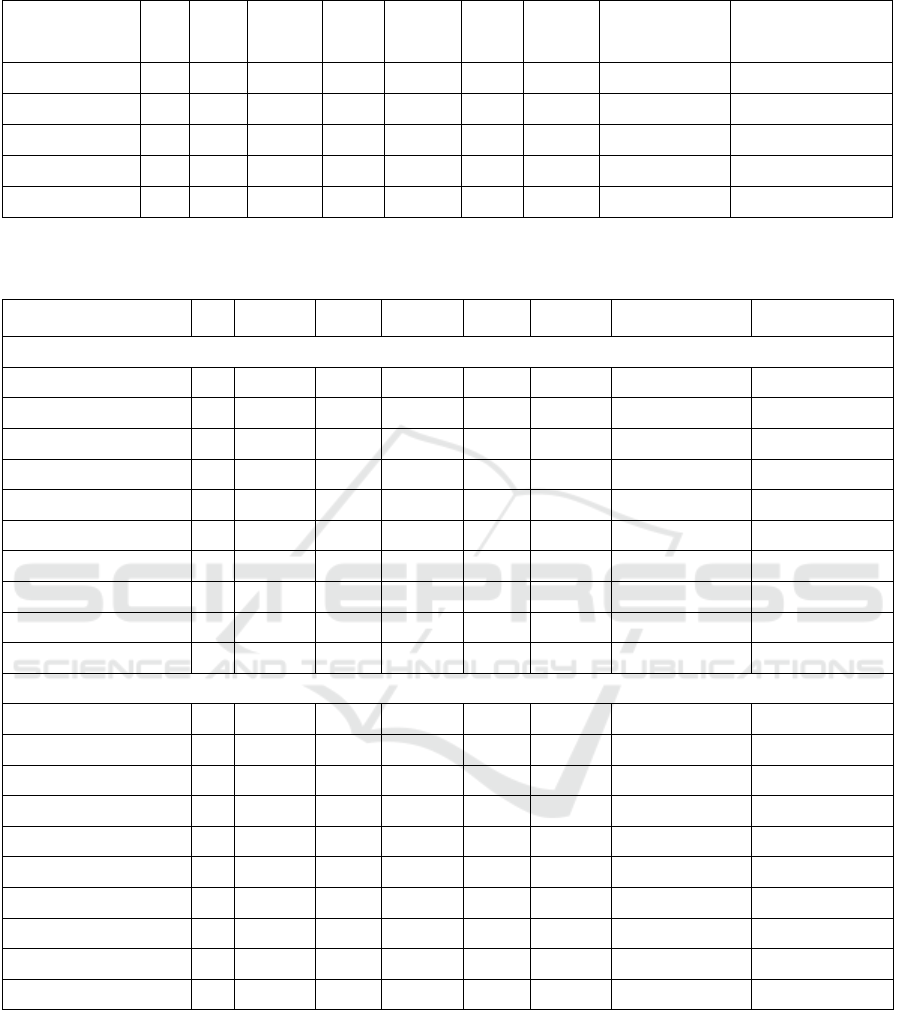
Table 2. Nutrient Intake of The Children Under Five in The Research Area.
Total n RNI
a
Mean Sd Median Min Max
Adequate* (%) Inadequate (%)
Energy (kcal) 105 1200 1,196.9 505.9 1,076.6 160.8 2,585.5 58 (55.2) 47 (44.8)
Protein (g) 105 32 33.6 13.6 33.8 4.0 68.2 102 (97.1) 3 (2.9)
Iron (mg) 105 8 4.85 2.8 4.8 0.0 13.1 52 (49.5) 53 (50.5)
Zinc (mg) 105 4 4.9 3.5 4.01 0.4 18.8 49 (46.7) 56 (53.3)
Vitamin A (mg) 105 400 167.8 86.9 164.3 0.0 448.1 2 (1.9) 103 (98.1)
a
(Ministry of Health RI, 2013)
Table 3. The Dietary Intake and Nutrition Fulfillment Based on CIMI.
Total n Mean Sd Median Min Max
Adequate* (%) Inadequate (%)
by Gender
Energy (kcal) Boys 56 1,207.1 486.4 1107.3 322.9 2,263.5 32 (57.1) 24 (42.9)
Energy (kcal) Girls 49 1,185.2 528.9 1,007.9 160.9 2,585.6 26 (53.1) 23 (46.9)
Protein (g) Boys 56 33.1 13.3 32.8 9.2 68.2 54 (96.4) 2 (3.6)
Protein (g) Girls 49 34.1 13.9 33.8 4.0 59.5 48 (98.0) 1 (2.0)
Iron (mg) Boys* 56 4.9 2.9 5.1 0.0 13.1 31 (55.4) 25 (44.6)
Iron (mg) Girls* 49 4.8 2.8 4.6 0.7 11.1 20 (40.8) 29 (59.2)
Zinc (mg) Boys 56 4.5 2.9 4.1 0.7 16.6 25 (44.6) 31 (55.4)
Zinc (mg) Girls 49 5.3 3.9 3.9 0.4 18.8 24 (49.0) 25 (51.0)
Vit. A (mg) Boys 56 161.7 82.4 157.0 0.0 401.4 1 (1.8) 55 (98.2)
Vit. A (mg) Girls 49 174.6 91.9 174.8 0.0 448.1 1 (2.0) 48 (98.0)
by Age
Energy ≤ 2 year 42 1,080.2 256.3 990.6 160.9 2,585.6 19 (18.1) 23 (21.9)
Energy > 2 year 63 1,278.8 495.8 1,187.9 467.3 2,450.5 39 (37.1) 24 (22.9)
Protein ≤ 2 year* 42 28.0 12.8 25.3 4.0 53.1 39 (37.1) 3 (2.9)
Protein > 2 year* 63 37.4 13.4 35.0 12.2 68.2 63 (60) 0 (0)
Iron ≤ 2 year* 42 3.1 2.4 2.6 0.0 7.6 11 (10.5) 31 (29.5)
Iron > 2 year* 63 6.0 2.7 5.3 0.0 13.1 41 (39.0) 22 (21.0)
Zinc ≤ 2 year* 42 2.8 1.9 2.5 0.4 6.6 8 (15.4) 34 (84.6)
Zinc > 2 year* 63 6.2 3.6 5.7 0.66 18.8 41 (64.3) 22 (35.7)
Vit. A ≤ 2 year 42 171.9 56.7 162.0 2.11 314.0 0 (0) 42 (40)
Vit. A > 2 year 63 173.8 92.5 170.6 0.0 448.1 2 (2.0) 61 (58)
*p-values are significant at p < 0.05
Dietary Assessment of Children under Five using Calculator of Inadequate Micronutrient Intake (CIMI) Approach Study Case in
Pandeglang, Banten Province Indonesia
67

3.2 Dietary Intake (Food Consumption
and Dietary Pattern)
Based on dietary intake and nutrition fulfillment in
Table 1, only half (55.2 percent) of the children have
the fulfillment of the energy, iron (50.5%) zink
(53.3%) while almost all of them (98.1%) have
insufficient consumption of vitamin A.
Monotonous food consumption which is
dominated by carbohydrate sources (rice, cassava,
and bread) and a small portion of vegetables and
animal food sources resulted from the poor nutrition
of consumption. Children require high value and
diversity of food consumption for optimal growth and
development. Poor diet always comes out with
undernutrition as a result. The study
About the potential of food carrier for
micronutrients in Indonesia also found that the low
food diversity and less animal source, fruit and
vegetables cause the undernutrition in some remote
areas in Indonesia (Melse-Boonstra et al., 2000) low
divers diet of animal source foods (ASF)
(Muslimatun and Wiradnyani, 2016) and dietary
diversity and household food security (Pipi, Nanseki
and Chomei, 2014) and (Meshram et al., 2012).
The government of Indonesia has tried to improve
the micronutrients intake with the regulation of food
fortification (Melse-Boonstra et al., 2000;
Soekirman, Atmarita and Sanjaya, N. Elhusseiny,
2003) of iron in wheat flour and instant noodle; iodine
in salt and monosodium glutamate; vitamin A in oil.
In terms of energy and protein consumption, the
majority of Indonesia population has an adequate (60
%) even more than the normative reference on 50 %
of food consumption, while the consumption of food
derived from tubers, protein from animal sources,
fruits, and vegetables are lower than the ideal or
normative recommendations (Salim and Basuno,
2010). Furthermore, the quality of food consumption
of the Indonesian people is still low due to low food
diversification, nutritionally imbalanced, and unsafe
cause by high contamination.
4 CONCLUSION
Food consumption of children under five in Banten
province Indonesia is dominated by a monotonous
diet in which rice is the main source of carbohydrates
and a low portion of animal source food, vegetables,
and fruits. The fulfillment of energy is sufficient
while deficit in micronutrients (vitamins and
minerals).
REFERENCES
BMKG, Kementan, BNPB, LAPAN, BPS, W. and F. I.
(2017) ‘Buletin Pemantauan Ketahanan Pangan di
Indonesia’, 9, p. 21.
Bosha, T., Lambert, C., Riedel, S., Melesse, A., et al. (2019)
‘Dietary Diversity and Anthropometric Status of
Mother – Child Pairs from Enset ( False Banana ) Staple
Areas : A Panel Evidence from Southern Ethiopia’.
Bosha, T., Lambert, C., Riedel, S., Gola, U., et al. (2019)
‘Validation of the CIMI-Ethiopia Program and
Seasonal Variation in Maternal Nutrient Intake in Enset
( False Banana ) Growing Areas of Southern Ethiopia’,
pp. 1–13.
Budiastutik, I. and Nugraheni, A. (2018) ‘Determinants of
Stunting in Indonesia: A Review Article’, International
Journal Of Healthcare Research, 1(1), pp. 2620–5580.
Dandin, S. B. and Kumar, N. K. K. (2016) ‘Neglected and
Underutilized Fruit Species – an Insurance Against
Global Mal and Under Nutrition’, FAO Regional
Expert Consultation on Scoping, Prioritizing and
Mapping of Neglected and Underutilized Crop Species
in Asia, pp. 1–40. Available at:
http://www.fao.org/fileadmin/templates/rap/files/meeti
ngs/2016/161203_session1_4.pdf.
Durst, P. and Bayasgalanbat, N. (2014) Promotion of
underutilized indigenous food resources for food
security and nutrition in Asia and the Pacific,
Promotion of underutilized indigenous food resources
for food security and nutrition in Asia and the Pacific.
FAO (1992) ‘World Declaration and Plan of Action for
Nutrition’, International Conference on Nutrition,
(December), pp. 1–42.
Global Panel on Agriculture and Food Systems for
Nutrition. (2016) Food systems and diets : Food
systems and diets :
ICN2 (2014) ‘National Nutrition Strategy Paper of
Indonesia’, pp. 1–52.
Jati, I. R. A. P. et al. (2014) ‘Design and validation of a
program to identify inadequate intake of iron, zinc, and
vitamin A’, Nutrition. Elsevier Inc., 30(11–12), pp.
1310–1317. doi: 10.1016/j.nut.2014.03.015.
Kemenkes RI (2018) ‘Buletin Stunting’, Kementerian
Kesehatan RI, 301(5), pp. 1163–1178.
Melse-Boonstra, A. et al. (2000) ‘The potential of various
foods to serve as a carrier for micronutrient
fortification, data from remote areas in Indonesia’,
European Journal of Clinical Nutrition, 54(11), pp.
822–827. doi: 10.1038/sj.ejcn.1601094.
Meshram, I. I. et al. (2012) ‘Trends in the prevalence of
undernutrition, nutrient & food intake and predictors of
undernutrition among under five year tribal children in
India’, Asia Pacific Journal of Clinical Nutrition, 21(4),
pp. 568–576. doi: 10.6133/apjcn.2012.21.4.12.
Ministry of Health Indonesia (2007) ‘Laporan Riskesdas
Nasional 2007’, Riskesdas. doi: 1 Desember 2013.
Ministry of Health RI (2013) ‘Angka Kecukupan Gizi
(AKG) Recommended Nutrient Intake (RNI) of
Indonesia’, Kementerian Kesehatan RI, (mL), pp. 5–10.
ICSDH 2021 - International Conference on Social Determinants of Health
68

Muslimatun, S. and Wiradnyani, L. A. A. (2016) ‘Dietary
diversity, animal source food consumption and linear
growth among children aged 1–5 years in Bandung,
Indonesia: a longitudinal observational study’, British
Journal of Nutrition, 116(May 2018), pp. 1–9. doi:
10.1017/S0007114515005395.
Philipp, J. et al. (2019) ‘Validation of a computer-based
analysis tool for real-time dietary assessment within a
Ghanaian region’, NFS Journal. Elsevier, 16(April), pp.
15–25. doi: 10.1016/j.nfs.2019.06.002.
Pipi, D., Nanseki, T. and Chomei, Y. (2014) ‘Relationship
between dietary diversity and perceived food security
status in Indonesia - A case of households in the North
Luwu of South Sulawesi Province’, Journal of the
Faculty of Agriculture, Kyushu University, 59(2).
Radix, I. et al. (2014) ‘Design and validation of a program
to identify inadequate intake of iron , zinc , and vitamin
A’, Nutrition. Elsevier Inc., 30(11–12), pp. 1310–1317.
doi: 10.1016/j.nut.2014.03.015.
Salim, H. P. and Basuno, E. (2010) ‘Diversification of Food
Consumption: Its Current Conditions, Problems and
Prospects in Indonesia’, United Nation ESCAP
(Economic Social Commision for Asia and the Pasific),
8 Number 3(ISSN 1693-4636), pp. 1–6.
Soekirman, Atmarita, J. L. O. and Sanjaya, N. Elhusseiny,
F. J. L. (2003) ‘Indonesian Micronutrient Reference
Report’, (19).
Stewart CP, Iannotti L, Dewey KG, M. K. & O. A. (2013)
‘Childhood Stunting : Context, Causes, and
Consequences’, Maternal and Child Nutrition, 9(2), pp.
27–45.
The SMERU Research Institute (2015) ‘Food and nutrition
security in Indonesia : a strategic review. Improving
food and nutrition security to reduce stunting’,
SMERU-UKP4-WFP, p. 89.
UNICEF, WHO and World Bank Group (2018) ‘Levels and
Trends in Child Malnutrition, UNICEF / WHO / World
Bank Group Joint Child Malnutrition Estimates’,
Midwifery, 12(3), pp. 154–155. doi: 10.1016/S0266-
6138(96)90067-4.
United Nations Children’s Fund (Unicef) (2018) ‘Nutrition
Capacity Assessment in Indonesia’, UNICEF, Jakarta,
August.
World Health Organization and UNICEF (2019) ‘The
extension of the 2025 Maternal, Infant and Young Child
nutrition targets to 2030’, Discussion paper, p. 12.
Available at: https://www.who.int/nutrition/global-
target-2025/discussion-paper-extension-targets-
2030.pdf?ua=1.
Dietary Assessment of Children under Five using Calculator of Inadequate Micronutrient Intake (CIMI) Approach Study Case in
Pandeglang, Banten Province Indonesia
69
