
Determinants of Oral Health Behavior in Preschoolers: Application
of the Theory of Health Belief Model
Pahrur Razi
1a
, Muhammad Rusdi
2b
, Asni Johari
2c
, Syahrial
2d
, Asrial
2e
and Sukmal Fahri
1f
1
Department of Health Promotion, Ministry of Health Health Polytechnic Jambi, Jl. H. Agus Salim, Jambi, Indonesia
2
PMIPA Doctoral Program, Jambi University, Jambi, Indonesia
1
Department of Health Environment, Health Polytechnic, Ministry of Health Jambi, Jl. H. Agus Salim, Jambi, Indonesia
Keywords: Oral Health Behavior, health belief model, pre-schoolers.
Abstract: Oral and dental health behavior greatly influences the occurrence of dental disease, where children aged five
years have the highest incidence of dental disease, which is 93%. Regarding the use of healthy behavior
factors, people are still not aware that oral and dental health behavior is only 2.8% in the five-year age group.
This study aims to determine the predictive factors of oral health behavior in pre-school children based on the
theory of health belief model, Theory of Planned Behavior and Social Cognitive Theory. The cross-sectional
study method involved 200 mothers and children in the city of Jambi with a sampling technique using
purposive sampling. The results showed that the mean standard deviation of the children's age was 5.6 ± 1.1
years (range 5-6), and 52% were girls. The mean (SD) score for oral health behavior was 4, 8 (±1.9) out of
10. Regression analysis showed a positive relationship between all HBM, TPB and SCT structures on oral
health behavior. Conclude that Health Belief Model was an important predictor of children's oral health
behavior (p < 0.001). Effective promotional interventions can be designed based on these predictors to help
improve children's oral hygiene behavior.
1 INTRODUCTION
Dental and oral health is one of the basic components
of pre-school children's health. Young children are
completely dependent on their parents, especially
their mothers, to have proper oral health (Baghiani,
2015). The proportion of tooth brushing behavior
based on the age group of 5-9 years brushing their
teeth every day is 93.2%, but the correct brushing
time is only 1.4%. While in Jambi Province, it was
found that 96.4% brushed their teeth every day, only
1% of them brushed their teeth according to the
recommendation. Nationally, tooth brushing behavior
in Jambi province is the lowest in Indonesia
(Kemenkes RI, 2018).
Regarding the use of healthy behavior factors,
people are still not aware that oral and dental health
a
https://orcid.org/0000-0003-2835-1710
b
https://orcid.org/0000-0003-1075-6023
c
https://orcid.org/0000-0002-9776-0617
d
https://orcid.org/0000-0002-0919-146X
e
https://orcid.org/0000-0001-6257-0285
f
https://orcid.org/0000-0001-6352-087X
behavior is only 2.8% in the five-year age group. Oral
and dental health behavior greatly influences the
occurrence of dental disease, where children aged
five years have the highest incidence of dental
disease, which is 93%. Therefore, it is highly
recommended to improve oral and dental health
behavior as an effort to prevent dental and oral
diseases in children (Publishery, 2013). Behaviors
related to oral health include eating habits, oral
hygiene habits, dental care (Branden, et al., 2014).
Several research results on oral behavior in pre-
school children, a significant predictor of individual
behavior today is attitude. The theory of planned
behavior (TPB) and the health action process
approach (HAPA) were the best predictors of
intention to engage in both behaviors (Dumitrescu Al,
et al. 2014). The Health Belief Model shows the
relationship between several structures related to
Razi, P., Rusdi, M., Johari, A., Syahrial, ., Asrial, . and Fahri, S.
Determinants of Oral Health Behaviour in Pre-schoolers: Application of the Theory of Health Belief Model.
DOI: 10.5220/0010757400003235
In Proceedings of the 3rd International Conference on Social Determinants of Health (ICSDH 2021), pages 147-150
ISBN: 978-989-758-542-5
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
147

personal perceptions, perceived barriers and self-
efficiency, and behavior (Baghiani, 2015). The theory
of Planned Behavior is also proven to be an important
predictor of children's oral health behavior. These
findings are useful in the formation to promote dental
and oral health behaviors of children. An effective
dental and oral health education intervention can be
designed based on this predictor (TPB component) to
increase the mother's perspective on oral health and
dental and oral health behavior of her child. Health
professionals in health care settings can provide
mothers with accurate practical information and
training on oral self-care behaviors. However, further
research is needed to confirm the results of this study
(Soltani, 2018).
Research by Makuch et al (2011) stated that the
use of games, exercises, performances/theatre and
puppets aimed at children's development is more than
just presenting didactic information. From the model
given above, it can be stated that the development of
oral health skills is carried out using an exclusive
approach and a program that aims to improve the oral
health abilities of pre-school children. An
unsupportive approach was taken by Garbin, et al
(2009), where pre-school children were involved in
programs using role-play programs, painting using
numbers, audiovisual, music, and playing programs.
As a result, pre-schoolers can pass on the knowledge
gained at school to their parents who change their
family members' dental health routines.
In addition to the approach mentioned above,
changes in oral health behavior are mostly carried out
through the application of program models as
researched by Yevlahova, et al (2009) that the
transtheoretical model, has been found to be the most
effective approach to updating health behavior.
From a preliminary study of pre-school-aged
children in Jambi City, it was shown that the oral
health behavior of pre-school children in TK/PAUD
was not optimal, ie 2.2 criteria were lacking. The oral
health behavior of pre-school children in Jambi City
still needs to be improved. These data are supported
by facts found when interviewing pre-school
children, kindergarten teachers and parents, such as:
(1) Pre-school children's oral health behavior is not
optimal, (2) Unable to maintain oral health at home,
(3) Does not know the function and shape of teeth, (4)
likes to eat foods that can damage teeth, (5) only gets
oral health information from television, and (6) tends
to receive oral health information obtained by the
teacher without being followed by understanding the
material obtained so that it is less able to maintain oral
health.
Based on the analysis presented above, the
problems faced are the low oral health behavior of
pre-school children and understanding of oral health
materials. So the authors feel it is necessary to know
the determinants of oral health behavior in pre-school
children in developing an intervention model for
changing oral and dental health behavior for pre-
school children according to the characteristics of the
intervention material.
2 MATERIALS AND METHODS
Cross-sectional study This study was conducted on
200 mothers and children with children aged 4-6
years in Kindergarten in Jambi City, Indonesia with
the sampling technique in this study is non-
probability sampling, which in this study was chosen
purposive sampling, the reason for choosing this
sampling technique is considering the sample of this
study, namely parents of kindergarten children who
are willing to have specific information on children's
oral health behavior. Inclusion criteria were
willingness to participate in the study, mothers with
children aged 4-6 years actively enrolled in
Kindergarten school year 2020/2021, and not
suffering from any physical or mental illness.
Data were collected through a questionnaire that
was filled out by the mother herself. They were
informed of the purpose of the study and
subsequently, they signed a written informed consent.
Filling out the questionnaire takes approximately 25
minutes. The participants were awarded several
prizes (such as toothpaste and toothbrush) for their
voluntary participation in the study.
2.1 Measurement
The implementation of data collection techniques is
adjusted to the Covid-19 health protocol, carried out
through the google form. The link (link) of the
questionnaire will be distributed to all parents of
kindergarten children via WhatsApp. The
questionnaire consisted of three parts: demographic
characteristics, children's oral health behaviors, and
the construction of HBM (perceived benefits, barriers
to action, and self-efficacy). However, because the
Covid-19 pandemic is still collecting data on the
perceived severity component, the signal for action
cannot be taken. Demographic characteristics include
age of mother and child, gender of child, age of
mother's occupation and education (illiteracy,
elementary, junior high, high school, diploma, and
ICSDH 2021 - International Conference on Social Determinants of Health
148
academic) and economic status (weak, moderate,
good).
2.2 Children's Dental and Oral Health
Behavior
Children's oral health behavior was evaluated through
10 questions about oral health. Scores may range
from 0–10, with higher scores indicating better oral
health behaviors.
2.3 TPB Arrange Items
The HBM construct related to children's oral health
behavior was assessed through 18 items derived from
the available literature in accordance with HBM
procedures and guidelines. The HBM-based
questions address perceived vulnerabilities,
perceived benefits, perceived barriers and self-
efficacy. Responses to all items were scored on a 5-
point scale ranging from 1 (strongly disagree) to 5
(strongly agree).
dapatkah Anda menjelaskan berapa banyak item
sebelum dan sesudah uji validitas dan reliabilitas?
2.4 Reliability and Validity
When tested for the validity of the contents of all the
questionnaires confirmed to be valid. The mean was
0.81 (p>0.6) and the total reliability (Cronbach's
alpha) was 0.89, indicating good internal consistency.
Tes statistik seperti apa?
Statistic analysis
All data were analyzed using SPSS version 16
software. The analysis was carried out using
univariate and bivariate analysis (linear regression)
with a level of <0.05.
3 RESULTS AND DISCUSSION
Table 1 displays the demographic characteristics of
the participants. The mean ± SD children's age was
5.24 ± 0.61 years; and 52% were women. The mean
age ± SD of the mother was 31.25 ± 1.27. About 28%
of mothers have a bachelor's degree; 92 mothers
(46%) worked; and 66% good economic status and
24% mother's knowledge about oral health is good.
Then the average oral health behavior is 4.23,
susceptibility is 2.24, benefit is 2.27, barrier is 2.28
and efficacy is 2.29.
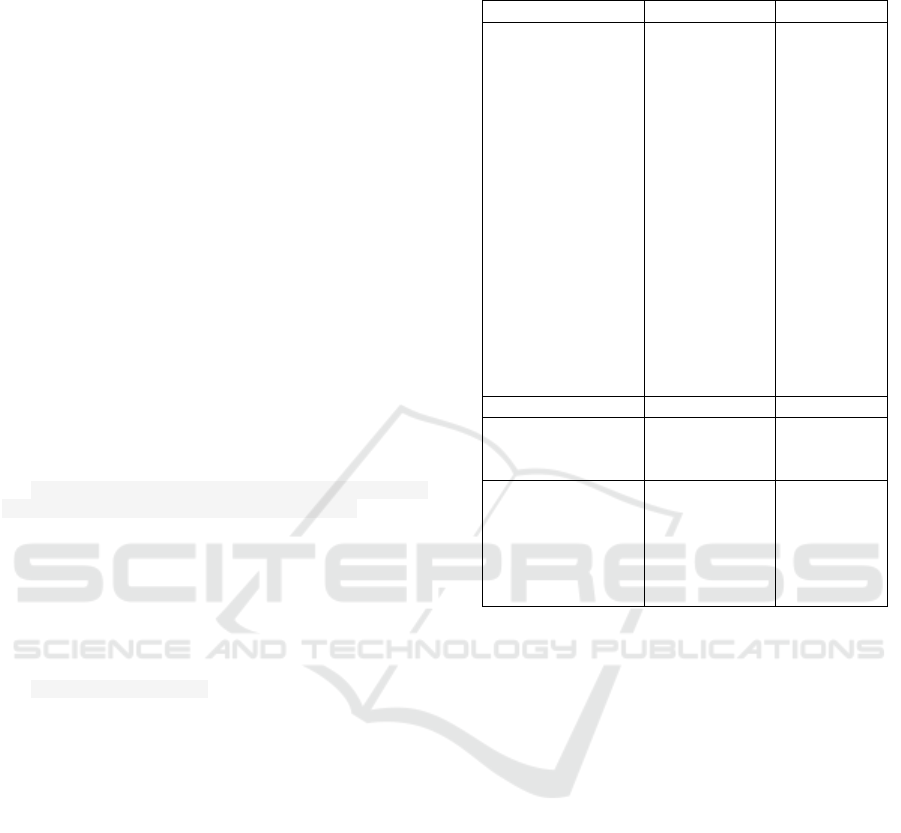
Table 1: Distribution of socio-demographic characteristics,
oral health behaviors and the construct of HBM (n = 200)
Variable Total (N) (%)
Child Gender
- Man
- girl
Mother's Education
- high school
- Diploma
- University
Mother's
Employment Status
- Work
- Unemployment
Economic Status
- Weak
- Good
Mother's
Knowledge
- Not good
- Goo
d
96
104
96
76
28
92
108
68
132
152
48
48
52
48
38
14
46
54
34
66
76
24
Variable Average SD
Mother's Age
(years)
Child's Age (years)
31.25
5.24
1.27
0.61
Oral health
behavior
Vulnerability
Benefits
Resistance
Self efficac
y
4.23
2.24
2.27
2.28
2.29
0.86
0.73
0.69
0.68
0.66
Table 2 of the relationship between perceived
vulnerability, benefits, barriers and self-efficacy
shows a positive correlation with low
strength/closeness of the relationship on perceived
vulnerability (r = 0.236), perceived benefits (r =
0.458), perceived barriers (r = 0.351) and self-
efficacy (r = 0.499). This means that the higher the
vulnerability, benefits, barriers and self-efficacy, the
higher the child's oral health behavior. However, the
perceived susceptibility variable can only explain
5.6%, and 5.5% (perceived benefits and barriers), and
4.4% (self-efficacy) variations in children's oral
health behavior variables. Although this relationship
was statistically significant (p < 0.05). All
components of the HBM are the main predictors of
oral health behavior in pre-school children.
Determinants of Oral Health Behaviour in Pre-schoolers: Application of the Theory of Health Belief Model
149
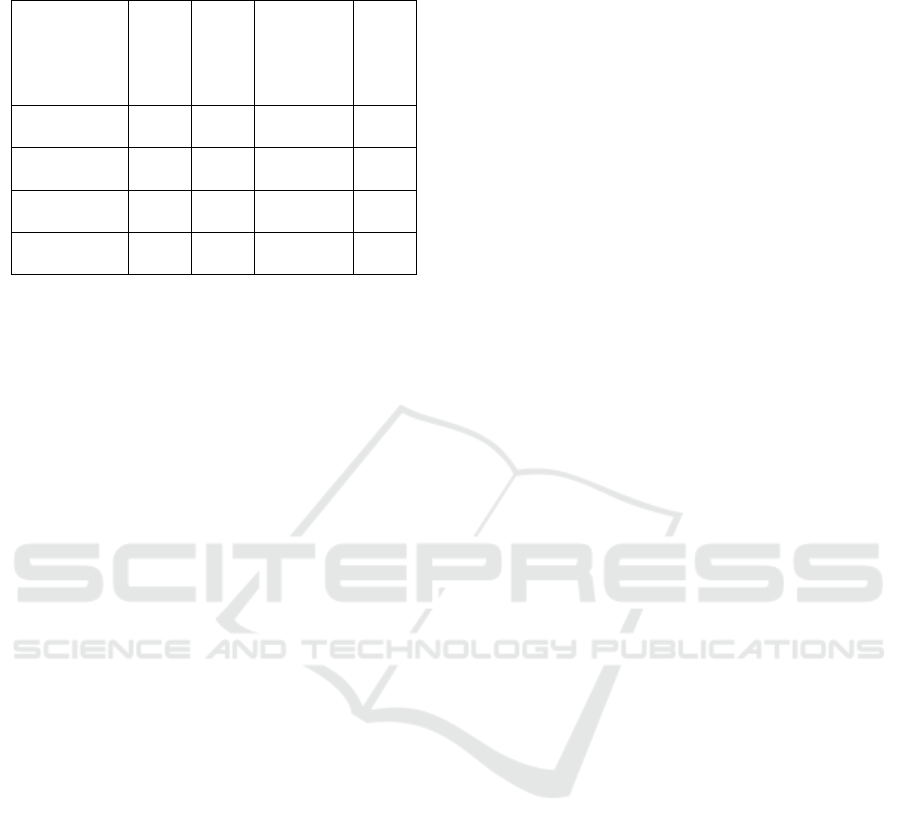
Table 2. Analysis of Correlation and Linear Regression
Oral health behavior and components of HBM
Variable R R2
Line
Equation
(Oral
Health
Behavior)
p-
value
V
ulnerabilit
y
0.236 0.056
3.599 +
0.279
0.001
Benefits 0.235 0.055
3.562 +
0.292
0.001
Resistance 0.235 0.055
3.548 +
0.297
0.001
Self efficac
y
0.209 0.044
3.603 +
0.271
0.003
4 CONCLUSIONS
Health Belief Modelproven to be an important
predictor of oral health behavior in pre-school
children. These findings are useful in designing a
conceptual framework for promoting oral health
behaviors in pre-school children. Effective oral health
promotion interventions can be designed based on
this predictor (HBM component) to improve oral
health behaviors in pre-school children. However,
further research is needed to confirm these results
especially in the development of a health promotion
model to improve oral health behavior in pre-school
children.
ACKNOWLEDGEMENTS
The authors would like to thank the Director of
Poltekkes, Ministry of Health, Jambi, for their
support. We also appreciate all the promoters who
have taken the time to complete this research.
REFERENCES
Baghiani Moghadam MH, Mozaffarian Azad M, Biria M,
Sabour S. Evaluation of oral hygiene care of less than 4
years old children by their mothers based on the Health
Belief Model. J Dent Sch. 2015; 33:9-18.
Dumitrescu AL, Dogaru BC, Duta C, Manolescu BN.
Testing five social-cognitive models to explain
predictors of personal oral health behaviors and
intention to improve them. Oral Prev Dent.
2014;12(4)345-355.
Garbin C, Garbin A, Santos K, Lima D. Oral health
education in schools: promoting health agents. int. J
Dent Hyang 2009;7:212-6.
Makuch A, Rescke K, Rupf S. (2011). Effective Teaching
of Tooth Brushing to Pre-schoolchildren. J Dent Child
(Chic), 2011. 78(1):9-12.
Ministry of Health of the Republic of Indonesia. 2018.
Basic Health Research (RISKESDAS) 2018. The
Indonesian Ministry of Health Research and
Development Agency for 2018.
Pullishery F, Panchmal GS, Shenoy. (2013). Parental
attitudes and tooth brushing habits in pre-school
children in Mangalore, Karnataka: A cross-sectional
study. International Journal of Clinical Pediatric
Dentistry, 6(3), 156-160.
Rusdi, 2018. Research on Educational Design and
Development. New Knowledge Concepts, Procedures
and Synthesis. 1st printing, July 2018. Publisher PT.
RajagrafindoPersada. Rajawali Press: Depok.
Rusdi, 2020. Research on Educational Treatment. 1st
printing, August 2020. Publisher PT.
RajagrafindoPersada. Rajawali Press: Depok.
Soltani R., Sharifirad G., Mahaki B., Eslami AA.,
Determinants of Oral Health Behavior among Pre-
school Children: Application of the Theory of Planned
Behavior. J Dent (Shiraz). 2018 Dec; 19(4): 273-279.
Souza IPMA, Jacobina RR. Educaçãoemsaúde e
suasversõesnahistóriabrasileira. Rev
BaianaSaúdePública2009;33:618-27.
Tolvanen M, Lahti S, Poutanen R, Sepp L, Pohjola V,
Hausen H. Changes in children's oral health-related
behavior, knowledge and attitudes during a 3.4-yr
randomized clinical trial and oral health-promotion
program. Eur J Oral Sci 2009;117:390-7.
Van den Branden S, Van den Broucke S, Leroy R, Declerck
D, Hoppenbrouwers K. Predicting oral health-related
behavior in the parents of pre-school children:
Application of the Theory of Planned Behavior. Health
Educational Journal. 2014; 74: 221-230.
Yevlahova D., Satur J., 2009. Models for individual oral
health promotion and their effectiveness: a systematic
review.
ICSDH 2021 - International Conference on Social Determinants of Health
150
