
The Influence of Religiosity Dimensions on Health Protocols
Compliance of Muslim Netizen
Sitti Raodhah, Muhammad Fais Satrianegara, Surahmawati, Muhammad Rusmin, Yessy Kurniati,
Yudhi Adnan, Zilfadhilah Arranuri
Study Program of Public Health, Faculty of Medicine and Health Sciences, Universitas Islam Negeri Alauddin Makassar,
Makassar, Indonesia
alauddin.ac.id, yessy.kurniati@uin-alauddin.ac.id, yudiadnan1987@gmail.com, iylhamec@gmail.com
Keywords: Compliance, Health, Muslim, Religiosity.
Abstract: Religion is one of the social determinants that affect health behaviour. This study aims to examine the effect
of the religious dimension on health protocols compliance on Muslim netizens in Makassar city. The study
was conducted with a cross-sectional design using purposive sampling. The number of research samples is
215 people. The dimensions of religiosity and adherence to health protocols were measured by instruments
that had been tested for validity and reliability. Data analysis was performed by linear regression test with a
significance value of p<0.05. The results showed that the dimensions of religiosity that affected adherence to
the health protocol were the ritual dimension (p=0.011), intellectual (p=0.028), and the consequence
dimension (p=0.000). While the dimension that has no effect on health protocol compliance is the ideological
dimension (p=0.061). The final model shows that Y=22.927+0.235X1+0.631X2+2.071X3. Ritual,
intellectual and consequence dimensions affect adherence to the health protocol of Muslim netizens in
Makassar City by 41%, while the rest are influenced by other factors. The dimension of religiosity is important
to pay attention for Covid 19 prevention.
1 INTRODUCTION
Coronavirus Disease 2019 (Covid-19) is a new type
of virus caused by SARS-CoV-2 (Severe Acute
Respiratory Syndrome Coronavirus 2) which is
currently shaking the world community (Mona,
2020). Since January 2020, this virus has managed to
infect hundreds of millions of people globally, with
104,370,550 confirmed cases and 2,271,180 deaths
(WHO, 2021). Even someone who does not show
symptoms of being infected with this virus can also
spread or become a carrier to others (Kumar &
Dwivedi, 2020). The public is encouraged to
implement a new healthy lifestyle according to health
protocols during this corona virus pandemic to
prevent an increase in the spread and number of
infections (Pinasti, 2020).
Health protocols are a series of activities aimed at
preventing the spread of covid 19 infection. The
forms are routinely maintaining hand hygiene,
maintaining distance, staying at home and going out
only for urgent needs, using masks when outside the
house, covering nose and mouth when sneezing,
keeping food intake, physical activity and managing
stress
Since it was implemented, public compliance
with health protocols has been quite good, but some
is still low. Research that shows that community
compliance is quite good is a study conducted in Deli
Serdang, the study shows that community compliance
is in a very positive area (Putra, 2020). Likewise, the
results of a survey conducted in the city of
Yogyakarta, the compliance of the community to
wear masks when leaving the house reached 93.3%,
80.44% always washed their hands with soap and
66.33% always kept their distance (Dinkes, 2020).
Similar results were found in the city of Jakarta,
showing that 68.96% of people comply with health
protocols in places of worship, 50.6% in traditional
markets and 80.71% in malls/shopping centres
(Simanjuntak, 2020)
However, there are also research results that show
community compliance is still low. As the results of
a survey conducted in Surabaya showed that 70% of
the people did not wear masks in places of worship
136
Raodhah, S., Satrianegara, M., Surahmawati, ., Rusmin, M., Kurniati, Y., Adnan, Y. and Arranuri, Z.
The Influence of Religiosity Dimensions on Health Protocols Compliance of Muslim Netizen.
DOI: 10.5220/0010757100003235
In Proceedings of the 3rd International Conference on Social Determinants of Health (ICSDH 2021), pages 136-142
ISBN: 978-989-758-542-5
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

and 84% did not keep their distance. While in
traditional markets, there are 81.6% of people who do
not wear masks and 85.9% who do not keep their
distance (Persakmi, 2020) Many factors affect
people's adherence to health protocols. These factors
include perception, age, education level, gender,
knowledge, marital status and health status (Larasati,
2020). Factors that cause public disobedience to
health protocols are due to lack of understanding/lack
of knowledge, economic motives, indifferent attitude
and feeling of low potential for the transmission of
covid 19 and distrust of the government (Wiranti,
2020).
One aspect that is often associated with health
behaviour is religiosity. Related to adherence to
health protocols, religiosity is an interesting aspect
that needs to be studied. Because religious gatherings
have been one of the points of spread of Covid 19
(Aschwanden, 2020). Research conducted in secular
countries, such as America, found that adherence to
health protocols tended to be lower in areas with high
levels of religiosity (Hill TD, Gonzales K, Burdette
AM, 2020). Community movement is higher in more
religious areas (Hill, 2020). Religious communities
find it more difficult to obey orders to stay at home in
an effort to prevent the spread of disease.
Indonesia is a country with the largest Muslim
population in the world. In Islam there are guidelines
on health protocols contained in the Qur'an and
Sunnah. In the Qur'an, Muslims are commanded to
stay away from things that can destroy themselves.
The Sunnah provides so many guidelines related to
this health protocol, such as the order not to cause
harm to others, the order to stay away from infectious
diseases, the quarantine order, the order to maintain
cleanliness, the order to cover the face when sneezing
to prevent the spread of droplets and the order to
consume food. healthy ones. All of these things
should be the basis for Muslims to comply with health
protocols.
This study wants to see whether religiosity has an
influence on compliance with health protocols. Do
Muslims with a high level of religiosity have a better
level of compliance?
2 METHODS
This research is a survey research with a cross-
sectional design. Measuring the level of religiosity
and compliance with implementing health protocols
at the same time. This research was conducted in
March-April 2021 in Makassar City. The population
of this research is the community of internet users in
Makassar City. Because the population is very large
and the exact number is not known, the research
sample is calculated by the formula n=Z²/4 (Moe)², so
the minimum sample size in this study is 171
respondents. The sample selection was carried out
purposively with the following criteria: Muslim,
living in Makassar City, Age > 15 years and Willing
to participate in the study. While the exclusion criteria
were not filling out the questionnaire completely and
resigning as a respondent. The data in this study were
collected using a questionnaire created on a google
form, then distributed on the researcher's social
media, such as Facebook and WhatsApp. The
questionnaire has passed the reliability test and
validity test. The test results have been used to
improve the questionnaire, so that the final
questionnaire is a questionnaire that has good
reliability and validity values. Data analysis in this
study was carried out in three stages. First, univariate
analysis to describe the characteristics of the
dependent variable and the independent variable.
Second, perform prerequisite test for multiple linear
regression test. Third, multivariate analysis with
multiple linear regression. The significance value
used is p<0.05.
This research was conducted in accordance with
applicable ethical standards by applying for an ethical
license to the Health Research Ethics Committee,
Faculty of Medicine and Health Sciences, Alauddin
State Islamic University, Makassar with license
number B.065/KEPK/FKIK/III/2021
3 RESULT AND DISCUSSION
This research was conducted in February-May 2021
with a total sample of 215 people. It can be seen that
most of the samples are women, aged < 30 years,
work as civil servants and are married. (Table 1).
Based on the characteristics, it can be seen that the
religiosity score is higher in men, but the adherence
score is higher in women. Based on age, religiosity
scores and adherence scores were highest in the >40
years age group. Based on occupation, teachers and
lecturers have the highest scores of religiosities and
obedience. Similarly, respondents who were married
had the highest scores of religiosities and obedience
(Table 2).
The Influence of Religiosity Dimensions on Health Protocols Compliance of Muslim Netizen
137
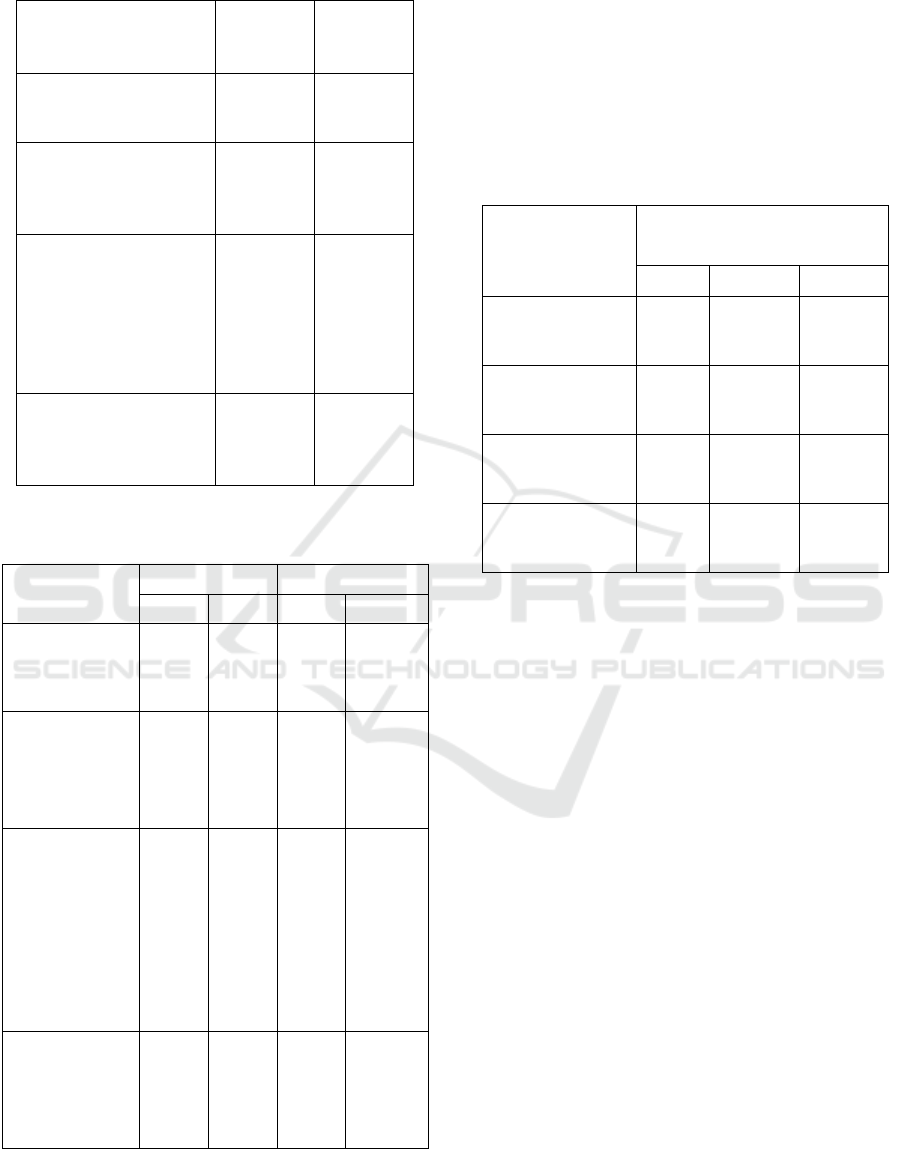
Table 1: Respondents’ characteristics
Respondent
Characteristic (n=215)
n %
Gender
Male 76 35.3
Female 139 64.7
Age
18-30 years 113 52.6
30-40 years 61 28.4
>40 years 41 19.1
Profession
Civil Servant 88 40.9
Housewife 15 7.0
Teacher/Lecturer 9 4.2
Student 80 37.2
Entrepreneurs 17 7.9
Jobless 6 2.8
Marital Status
Married 108 50.2
Not Married 103 47.9
Widow/widower 4 1.9
Table 2: Level of religiosity and adherence to health
protocols based on respondent characteristics
Characteristics
(n=215)
Religiosity Adherence
mean Sd Mean Sd
Gender
Male 58.73 ±6.85 54.35 ±1.00
Female 58.33 ±7.07 54.9 ±5.54
Age
18-30 years 57.48 ±7.03 53.65 ±5.63
30-40 years 58.57 ±6.96 55.16 ±6.48
>40 years 61.07 ±6.34 56.61 ±4.32
Profession
Civil Servant 58.93 ±6.82 55.09 ±5.79
Housewife 59 ±7.22 53.53 ±4.78
Teacher/Lecturer 63.11 ±6.85 58.44 ±5.5
Student 56.56 ±6.57 53.15 ±5.63
Entrepreneurs 60.82 ±7.68 57.29 ±4.82
Jobless 62.33 ±6.95 57.5 ±6.59
Marital Status
Married 59.49 ±6.77 55.59 ±5.86
Not Married 57.39 ±7.2 53.67 ±5.60
Widow/widower 59 ±1.82 53.75 ±2.63
There is a difference in the score of adherences to
the health protocol based on ritual, intellectual and
consequence dimensions (p<0.05), where
respondents who have a high score on the religiosity
dimension tend to have a high compliance score as
well. However, on the ideological dimension,
although there was a difference between obedience
scores based on
the level of religiosity, the difference
was not significant (p=0.061, p>0.05) (Table 3).
Table 3: Differences in adherence to health protocols based
on the level of religiosity dimensions
Religiosity
Dimension
Adherence to health
protocol
Mean Sd P*
Ritual
Medium 51.69 ±5.55 0.000
High 56.89 ±4.83
Ideology
Medium 52.35 ±7.15 0.061
High 54.88 ±5.57
Intellectual
Medium 49.78 ±5.78 0.000
High 55.93 ±5.03
Consequences
Medium 48.14 ±5.10 0.000
High 55.35 ±5.38
Based on the results of the variable prerequisite
test, it appears that the variables that meet the ritual,
intellectual and consequence dimensions (Table 4).
If the other independent variables are fixed, then
every 1% increase in the ritual dimension score, it
will increase the adherence score by 0.253. If the
other independent variables are fixed, then every 1%
increase in the intellectual dimension score, it will
increase the compliance score by 0.631. And if the
other independent variables are fixed, then every 1%
increase in the consequence dimension score, it will
increase 2,071 compliance scores. Because the value
of R square is 0.410, then the ritual, intellectual and
consequence dimension variables affect adherence to
the health protocol by 41% while the rest is
influenced by other factors. Because the R value is
0.64, it can be concluded that there is a strong
relationship between the variables of ritual,
intellectual and consequence dimensions on health
protocol compliance (Table 5).
Social capital has become one of the key determinants
of health according to WHO (Solar, 2010). This
concept includes, among others, social organization,
such as participation in social activities and voluntary
activities, mutual help and mutual trust in society
(Rouxel et al, 2015).
ICSDH 2021 - International Conference on Social Determinants of Health
138
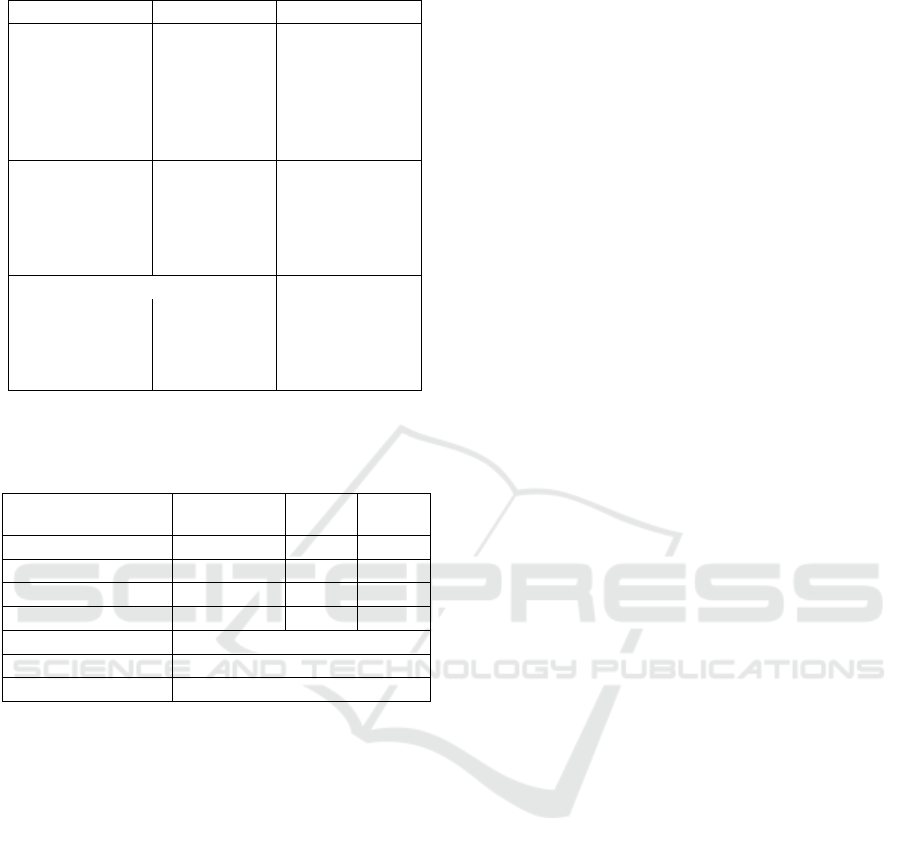
Table 4: Summary of variable prerequisite test results
Prerequisite Test p Interpretation
Normality* 0.455 Qualify
Linearity
Ritual 0.843 Qualify
Ideology 0.003 Unqualify
Intelectual 0.454 Qualify
Consequences 0.795 Qualify
Multicollinearity
Ritual 0.587 Qualify
Ideology 0.794 Qualify
Intelectual 0.473 Qualify
Consequences 1.535 Qualify
Heteroscedasticity**
Ritual 0.127 Qualify
Ideology 0.786 Qualify
Intelectual 0.612 Qualify
Consequences 0.137 Qualify
*Kolsmogorof-Smirnov
**Glejser
Table 5. Summary of multiple linear test results
Variable
Regression
Coefficient
t Sig
Constant 22.927
X1 (Ritual) 0.235 2.552 0.011
X2 (Intellectual) 0.631 2.211 0.028
X3 (Consequences) 2.071 5.405 0.000
F 30.457
R Square 0.410
R 0.640
Compliance with health protocols (Y)
Y=22.927+ 0.235X1+0.631X2+2.071X3 (1)
Social interactions without structural ties lead to
discussion of issues in the community and help
community members move together towards unseen
goals and benefits. (Pattusi MP, Marcenes W,
Croucher R, Sheiham A, 2001) Participation in
religious groups can be one of the social capitals that
provides support among participants
Religiosity can be defined as an organizational
system of beliefs, practices, rituals and symbols
designed to facilitate closeness to the sacred or
transcendent (God, a higher power or supreme
truth/reality) and to promote understanding of one's
relationships and responsibilities with others. in
living together in a society (Koenig HG, ing D and
Carvon VB, 2012)
Religiosity is associated with protection against
chronic disease and death in children and adolescents.
Data from NHANES III shows this (Bruce et al,
2017). Religiosity also has an inverse relationship
with risky behaviours such as smoking and alcohol
consumption in adolescents (Pitel et al, 2012).
Adherence to religious practice is also associated with
psychological well-being and life satisfaction in
young people (Souza, et al, 2012) and is associated
with better health status in older people (Reinal,
2004). However, there are some negative
relationships between religiosity and health.
Religiosity has been reported to be associated with
poor health (Kodzi et al, 2011) and obesity risk
(Feinsterb et al, 2011)
Religiosity is one of the factors that influence
behaviour. There are various variations of religious
dimensions that are positively related to emotional
health behaviour in adolescents. A positive
correlation was found between individual and family
factors with emotional and behavioural health in
adolescents. Religiosity directly affects emotional
health and behaviour in adolescents (Rafi MA, Avval
MH, Yazdami AA, 2020). A study found all
dimensions of religiosity to be significant predictors
of Islamic work behaviour ethics (Aminuddin, 2019).
Family religiosity is related to dental health
related to quality of life in school children
(Menegazzo, 2018). Religiosity in adolescents is a
factor that mediates the influence of parental
religiosity on health behaviour in adolescents, such as
alcohol and drug use and depression (Barton Al,
Snider JB, Vazsonyi AT, Cox JL, 2014). Workers'
religiosity has a strong influence on the
organizational behaviour of workers in the workplace
(Awani M and Zaiden M, 2019)
During a pandemic, people become more
religious (Wilson S, Bourstein M, Hernandez A,
Rozsul). More than half of Americans are praying for
the end of Covid 19 and 24% report feeling an
increase in their faith during the pandemic
(Gecewicz). Although in many countries, religious
gatherings such as the Tablighi Jamaat (India), Oneji
Shincheonji (South Korea) and Kyev Parchersh
Lavira (Ukraine) have become places for the spread
of the COVID-19 virus (Aschwanden, 2020).
Religiosity and spirituality have an important role in
healing pain, impacting health status and minimizing
the consequences of social isolation (Lucchetti G,
Goesl G, Amatul SG, et al, 2020). A study found that
most of the respondents had high levels of religiosity
and mild anxiety levels. There is a significant
relationship between religiosity and anxiety levels in
students (Wahyuni I, Suharno, Andika R, 2020)
Regions that are more religious show higher
population movements. The stay-at-home order had a
weak effect on more religious areas (Hill TD,
The Influence of Religiosity Dimensions on Health Protocols Compliance of Muslim Netizen
139

Gonzales K, Burdette AM, 2020). The high level of
religiosity in society triggers an increase in barriers to
policies imposed by the government and reduces
adherence to Covid 19 mitigation guidelines
(DeFranza D, Lindow M, Harrison K, Mishra A,
Mishra H, 2020). More religious populations report
less trust in science as a social institution and have
anti-science (science) behaviour (Evens, 2013). More
religious areas report more frequent population
movements (Hill TD, Gonzales KE, Upanieli L,
2020)
This study found that men's religiosity was higher
than women's. The results of this study are similar to
studies conducted on the effect of religiosity on
compliance with paying zakat. The study shows that
women are less religious than men (Abdulah M,
Sapeei NS, 2020). On the other hand, other studies
have found that, among Christians, women are more
religious than men, both in the United States and in
other Christian-majority countries. The study also
found that women with higher education were less
religious than men. On the other hand, men who were
more educated looked more religious (Schnabel,
2017).
The results of this study are similar to previous
findings, which found that married women and
individuals were more compliant with health
protocols (Indrayathi PA, Januraga PP, Pradayani PE,
Gesesesw HA. Ward PE, 2021). Another study found
that compared to men, women wash their hands more
often. Men wash their hands less often for various
reasons, such as feeling they don't need to do it, don't
like to wash their hands or don't have time to do it
(Bavel JJV., Baicker, K., Boggio, P.S. et al, 2020).
Women are also 12% more likely to use masks and
wash their hands than men (Rundle CW, Presley CI,
Militello M, et al, 2020). Based on these results, it
appears that women are more concerned about
maintaining their health than men (Amodan BO,
Bulage I, Katana E, et al, 2020). (Cobey KD, Laan F,
Stulp G, Bunk AP and Pollet TUJEP, 2013). While
men do have high risk behaviour
This study found that the highest adherence was
in the group of women, highly educated, married and
aged > 40 years. This finding is similar to the results
of a study in Italy, that women, most educated, middle
age (50-59 years), married/divorced have the highest
level of adherence to health protocols. And similar to
the results of the study, in this study, the young age
group, unmarried and student status, had the lowest
level of adherence (Carlucci L, D'Ambrosiox I,
Balsamo M, 2020). Studies in America, also found
that women and older age have better adherence.
(Park CL, Russell BS, Fendrich M, et al, 2020). Older
people will try to comply with health protocols
because they are a group that is more at risk of fatality
due to Covid 19 (Chen CN, Zhou M, Dong X, Qu J,
et al, 2020)
Religiosity does not directly predict an
individual's intention to worship at home during a
pandemic. However, religiosity has a role in raising
the intention to change the habit of worshiping at
home. Other factors that predict an individual's
adaptive behaviour to worship at home are intention,
social influence, and trust in the government
(Rostiani R, Toyib JS, Khoiriyyah S, 2021)
Research in Aceh found that there were
differences in the behaviour patterns of respondents
when going to public places and when going to
mosques. This study found that 68% of respondents
rarely visit public places, but they always pray in
congregation at the mosque. In addition, it was found
that 44% of respondents always use masks when
going to public places, but 55.3% of respondents
never wear masks when praying in mosques.
Respondents tend to adhere more to ethical health
protocols going to public places when compared to
mosques. This is caused by 3 things. First, the
religiosity of respondents has influenced the
perception of risk or fear of being infected with Covid
19. They believe that ablution and prayer can prevent
someone from being exposed to Covid 19. Second,
religiosity has made them feel uncomfortable when
leaving worship at the mosque, so they tend to
disobey the recommendations for worship at home.
Third, they believe that praying in congregation at the
mosque is useful for preventing Covid 19. (Nurrahmi
F, Masykur T, Harapan H, Masykin T, 2021)
Religiosity in Islam should make a person more
obedient in carrying out health protocols. Because
Islam teaches to protect others and yourself from
harm. In addition, many sources of Islamic teachings
are in line with the principles of health protocols. So
that a good Muslim should have a good level of
compliance with health protocols. Worshiping in the
mosque can still be done, but of course when the
disease case can still be controlled. Worship at the
mosque must still be carried out in accordance with
the health protocol, so that the mosque as a place of
worship does not become a source of transmission of
the Covid 19 outbreak.
4 CONCLUSIONS
Based on the results of the study, it can be concluded
that religiosity has an influence on compliance with
ICSDH 2021 - International Conference on Social Determinants of Health
140

health protocols and Muslims with a high level of
religiosity have a better level of compliance.
ACKNOWLEDGEMENTS
The researcher would like to thank the respondents
who are willing to be involved in this research
REFERENCES
Abdulah M., Sapeei, N, S., 2020. Do Religiosity, gender
and Educational Background Influence Zakat
Compliance? The Case of Malaysia. International
Journal of Social Economics.
Aminuddin, N, A., 2019. Demographic factors and
religiosity dimensions as preditors of Islamic Ethical
work behaviour in Brunei. Psychological Thought, 12
(2), 185-201.
Amodan, B,O., Bulage, I., Katana, E., et al, 2020. Level and
determinants of adherence to covid 19 preventive
measures in the first stage of the outbreak in Uganda.
International Journal Environment Res Public Health,
17, 1-14.
Aschwanden., 2020. How :Superspread" events drive most
covid 19 spread. Retrieved from Scientific America:
https://www.scientificamerican.com
Awani, M., and Zaiden, M., 2019. Organizational
Citizenship Behaviour and Religiosity at The
Workplace. International Journal of Contempory
Research and Review, 10 (5), 21501-21514.
Barton, A,l., Snider, J,B., Vazsonyi, A,T., Cox, J,L., 2014.
Adolescent religiosity as a mediator of the relationship
between parental religiosity and adolescent helath
outcome. Journal religious and health, 53, 86-94.
Bavel, J,J,V., Baicker, K., Boggio, P, S., et al, 2020. Using
social and behavioural science to support COVID-19
pandemic response. Nature Human Behaviour, 4, 460-
471.
Bruce, M, A., Martins, D., Duru., Beech, B,M., Sims, M.,
Herawa, N., 2017. Church attendance, allostatic load
and mortalilty in middle aged adults, 12. Plos One, e
0172618.
Carlucci, L., D'Ambrosiox, I., Balsamo, M., 2020.
Demographic and Attitudinal Factor of Adherence to
Quarantine Guidelines During Covid 19 : the Italian
Model. Frontier in Psychology.
Chen, C, N., Zhou, M., Dong, X., Qu, J., et al, 2020.
Epidemiological and Clinical Characteristics of 99
cases of 2019 novel coronavirus pneumonia in Wuhan,
China. Lancet, 395, 507-513.
Cobey K, D., Laan, F., Stulp, G., Bunk, A, P, and Pollet, T,
U, J, E, P., 2013. Sex Difference in Risk Taking
Behaviour among Dutch Cyclrst. Evol. Psychol, 11,
350-64.
DeFranza, D., Lindow, M., Harrison, K., Mishra, A.,
Mishra, H.. 2020. Religion and Reactance to Covid-19
Mitigation Guidelines. American Psychologist, 10, 1-
11.
Dinkes Yogyakarta. 2020. Respon masyarakat terhadap
Covid 19 di DIY.
Evens., 2013. The growing social and moral conflict
between conservative protetanism and science. Journal
for the scientific study of religion, 52, 368-385.
Feinsterb, M., Liu, K., Ning, H., Fitchett, G., Lioyd-Jones,
D, M., 2011. Burden of Cardiovasculer Risk Factors,
Subclinical atheroschlerosis and dimensions of
religiosity : the multy-etnic study of atheroschlerosis.
Circulation, 121, 659-666.
Gecewicz. (n.d.). Few Americans Say their house of
worship is open, but quarter say their faith has grown
among pandemic. Retrieved from
https://www.pewreserach.org
Hill, T,D., Gonzales, K., Burdette, A, M. 2020. The Blood
of Crist Compels Them : State Religiosity and state
population mobility during the coronavirus (Covid 19)
pandemic. Journal of Religion and Health, 59, 2229-
2224.
Hill, T,D., Gonzales, K,E., Upanieli, L., 2020. Love thy
Aged? A State level analysis of religiosity and mobility
in aging population during the novel coronavirus (covid
19) pandemic. Journal of aging and health, 1-10.
Indrayathi, P,A., Januraga, P,P., Pradayani, P,E., Gesesesw,
H,A., Ward, P,E., 2021. Perceived Social Norms as
Determinants of Adherene to Public Health Measures
Related to covid-19 in Bali Indonesia. Frontier in
Public Health, 9, 1-8.
Kodzi, I,A., Obeng, Gyimah, S., Emina, J., Chika, E,A.,
2011. Religious Involvement, Social Engagement and
subjective health status of older residents of informal
neighborhoods of Nairobi. J Urban Health, 88 (suppl
2), s 370-80.
Koenig, H,G., Ing, D., and Carvon, V,B., 2012. Handboo of
Religion and Health. USA: OUP.
Larasati., 2020. Faktor yang berpengaruh terhadap
kepatuhan masyarakat pada protokol kesehatan dalam
mencegah penyebaran covid 19. Seminar Nasional
official statistik dalam mendukung implementasi
SDG's.
Lucchetti, G., Goesl, G., Amatul, S.G., et al. 2020.
Spirituality, religiosity and the mental helath
consequences of social isolation during covid 19
pandemic. International Journal of Social Psychiatry,
1-8.
Menegazzo, G,R., Sfreddo, C,S., Marquesan, P,K.,
Ramadan, Y,H., Ardenghi, T,M., 2018. Family
Religiosity and Oral Health Related Quality of Life : A
Multilevel Analysis in Brazilian School children.
Brazilian Dental Journal, 29(4), 381-387.
Nurrahmi, F., Masykur, T., Harapan, H., Masykin, T., 2021.
Paradox of Protective Behaviour Among Muslim Men
During the Early Stage of The Covid 19 Pandemic in
Aceh, Indonesia. Disaster Medicine and Public Health
Preparedness.
Park, C,L., Russel, B,S., Fendrich, M, et al., 2020.
American's Covid 19 Stress, Coping and Adherence to
The Influence of Religiosity Dimensions on Health Protocols Compliance of Muslim Netizen
141

CDC Guidelines. Journal of General Internal
Medicine, 35, 2296-2303.
Pattusi, M,P., Marcenes, W., Croucher, R., Sheiham, A.,
2001. Social deprivation, income inequality, social
cohesion and dental caries in Brazilian School children.
Soc Sci Med, 53, 915-925.
Persakmi. 2020. Protokol Kesehatan Pasar Tradisional
Surabaya. Surabaya.
Pitel, L, Madarasova, G, A., et al, 2012. Gender Difference
in The Relationship between religiosity and health-
related behaviour among adolescent. J Epidemiol
Community Health, 66, 1122-1128.
Putra, I. M., 2020. Determinant Analysis of Public
Compliance with the implementation of corona virus
disease 2019 (Covid 19) health protocol in Parcut Deli
Serdang Regency. Medan: Fakultas Dakwah dan
Komunikasi Universitas Islam Negeri Sumatera Utara.
Rafi, M,A., Avval, M,H., Yazdami, A,A., 2020. The
Influence of Religiosity on the emotional-behavioural
health of adolescent. Journal of religion and health, 59,
1870-1888.
Reinal, B,M., Brown, C., 2004. Religion and Preventive
health care utilization among the elderly. Soc Scimed,
58, 109-118.
Rostiani, R., Toyib, J,S., Khoiriyyah, S., 2021. Why do
Muslim Engage in Adaptive Worship Behaviour
During the Pandemic? The Role of Protetion Motives
and Religiosity. Journal of Islamic Mareting, 12 (3),
518-542.
Rouxel, P,L., Heilmann, A., Aida, J., Tsako, G., Watt, R,G.,
2015. Social Capital : theory, evidence and implications
for oral health. Community Dent Oral Epidemiol, 43,
97-105.
Rundle, C,W., Presley, C,I., Militello, M., et al. 2020. Hand
hygiene during covid-19 : recommendation from the
American Contact Panemyc Dermatitis Society.
Journal of American Academic Dermatology, 83, 1730-
7.
Schnabel., 2017. Gendered Religiosity. Review of Religious
Research, 59, 547-556.
Simanjuntak, D,R., Napitupulu, T,M., Wele, A,M., dan
Yanie, R., 2020. Gambaran kepatuhan masyarakat
menerapkan protokol kesehatan covid 19 di tempat
umum periode September 2020 di DKI Jakarta.
Solar, O., Irwan, A., 2010. A Conceptual Framework for
Action on The Social Determinant of Health Discussion
Paper 2 (Policy and Practice). Geneva: WHO
Document Production Service.
Souza, L, D, M., Maragalhoni, T,C., Quincoses, M,T., et
al., 2012. Psychological wellbeing of young people 18
to 24 years of age and assocrated factors. Cad Saude
Publica, 28, 1167-1174.
Wahyuni, I., Suharno., Andika, R., 2020. Relation Between
Religiosity Levels With Anxiety Levels on College
Student During Pandemi Covid 19. Al Irsyad Health
Journal, 13(2), 131-144.
Wilson, S., Bourstein, M., Hernandez, A., Rozsul.. (n.d.).
Coronavirus Creates Conflict for churches, where
gathering can be dangerous but also provide solace.
Retrieved from Washington Post: https//
www.washingtonpost.com
Wiranti, Sriatni, Kusumastuti., 202). Determinan
kepatuhan masyarakat Kota Depok terhadap kebijakan
pembatasan sosial berskala besar dalam pencegahan
covid 19 . Jurnal kebijakan kesehatan Indonesia, 9(3),
117-124.
ICSDH 2021 - International Conference on Social Determinants of Health
142
