
The Role of Social Determinants and Nutrient Intake on Nutritional
Status of Pregnant Women in Malaria Endemic Areas, Pesawaran
District
Dian Isti Angraini
1
, Reni Zuraida
1
, Efriyan Imantika
2
, Merry Indah Sari
3
1
Department of Community Medicine and Public Health, Faculty of Medicine, Lampung University, Lampung, Indonesia
2
Department of Obstetrics and Gynecology, Faculty of Medicine, Lampung University, Lampung, Indonesia
3
Department of Medical Education, Faculty of Medicine, Lampung University, Lampung, Indonesia
Keywords: Endemic of malaria, Nutrient intakes, Nutritional status, Pregnant women, Social determinants.
Abstract: The nutritional status of pregnant women is influenced by food consumption, infectious diseases (malaria),
and social determinants. Pesawaran district is one of the malaria-endemic areas in Lampung Province. The
study aims to determine the role of social determinants and nutrient intake in pregnant women in Pesawaran.
This study is a cross-sectional design, in Hanura and Gedongtaan community health centers Pesawaran, from
May to December 2019. The sample was 70 pregnant women, taken by purposive sampling technique.
Nutritional status was measured by examining mid-upper arm circumference, data on educational age, family
income, race, and parity were obtained from interviews, maternal knowledge ang food intake were obtained
from interviews using questionnaires. Data were analyzed using univariate, bivariate, and multivariate. The
results showed that malnutrition in pregnancy was 22.9%. Most of the pregnant women are highly educated
(55.7%), sufficient knowledge (58.6%), high family income (58.6%), multiparous (57.1%), non-Lampung
race (60%), adequate energy intake (55.7%), and protein intake (68.6%). The results showed education
(p=0.11), knowledge (p=0.025), income (p=0.005), parity (p=0.036), race (p=0.017), energy intake (p=0.011),
and protein intake (p = 0.033) have a role in the nutritional status of pregnant women. The factors that must
play a role are education, knowledge, income, and parity.
1 INTRODUCTION
Efforts to improve the nutritional status of the
community, including reducing the prevalence of
stunted toddlers, are one of the national development
priorities listed in the main targets of the 2020 – 2024
National Medium-Term Development Plan (Ministry
of Health, 2020). Improving the nutritional status and
health of pregnant women is the best way to
overcome stunting. Fetal nutrition depends entirely
on the mother's nutrition so that pregnant women
must receive adequate nutrition. Insufficient energy
and protein intake in pregnant women can cause
malnutrition/chronic energy deficiency (CED).
Chronic Energy Deficiency is a condition in which
women experience long-lasting or chronic
malnutrition (calories and protein), which describes a
"steady state" of a person's body being in an energy
imbalance between energy intake and expenditure
and causes low body weight and low body energy
supply (Wiyono et al., 2020).
Factors that play a role in the nutritional status of
a woman of childbearing age, both pregnant and non-
pregnant, consist of many factors, namely food
intake, illness (infectious diseases such as malaria,
anemia, protein deficiency), food availability,
environment (family, environmental hygiene,
culture), history of illness/health, health services,
education and maternal knowledge (UNICEF, 2015;
Ministry of Health, 2015).
The results of the 2018 Basic Health Research
(Riskesdas) showed that in Indonesia, the prevalence
of CED in pregnant women reached 17.3% and in
Lampung province, it was 13.6%. The prevalence of
CED in pregnant women aged 15-19 years is 33.5%
and at the age of 20-24 years is 23.3%; this figure is
still high so further intervention is needed (Ministry
of Health, 2018). One indicator of efforts to improve
nutrition in Indonesia is a decrease in the prevalence
of chronic energy deficiency in women of
childbearing age, both pregnant and non-pregnant
(Ministry of Health, 2017).
10
Angraini, D., Zuraida, R., Imantika, E. and Sari, M.
The Role of Social Determinants and Nutrient Intake on Nutritional Status of Pregnant Women in Malar ia Endemic Areas, Pesawaran District.
DOI: 10.5220/0010756900003235
In Proceedings of the 3rd International Conference on Social Determinants of Health (ICSDH 2021), pages 10-17
ISBN: 978-989-758-542-5
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
In Pesawaran district, Lampung province, the
number of pregnant women suffering from SEZ in
2018 was 485 people and pregnant women suffering
from malaria were 1,922 people (Dinas Kesehatan
Pesawaran, 2019). The nutritional status of pregnant
women is influenced by food consumption and
infectious diseases. Malaria suffered by a person can
cause malnutrition and anemia (Gulo, 2008).
Pesawaran Regency is one of the malaria-endemic
areas. Based on data on the health profile of
Pesawaran district in 2016, malaria cases were 1.915,
with the highest distribution being in the working area
of the Hanura community health center, followed by
Padang Cermin, Pedada, and Gedongtataan
community health centers (Dinas Kesehatan
Pesawaran, 2017).In malaria-endemic areas, parasitic
infections and malnutrition, especially in pregnant
women, are problems that arise simultaneously. The
state of malaria infection can cause anemia and other
micronutrient deficiencies. Micronutrient deficiency
can also lead to an increased risk of infection and this
will harm the unborn baby (Steketee et al., 2001).
2 SUBJECT AND METHOD
This research is an observational analytic study with
a cross-sectional research design. The study was
conducted at the Hanura and Gedongtaan community
health centers in Pesawaran district from May to
December 2019. The population in this study were
pregnant women in Pesawaran district. Based on the
results of the sample calculation, the minimum
number of samples that must be met is 70 people. The
sample size calculation uses the sample size formula
for unpaired categorical comparative analytics with a
95% confidence value, the power of the test is 80%.
Sampling was done by the purposive sampling
method. The inclusion criteria for this research
sample were pregnant women aged 18-35 years and
willing to participate in the research process. The
exclusion criteria for this study were pregnant women
with malignancy, diabetes mellitus, and tuberculosis.
The independent variables in this study were
social determinants (education, knowledge, income,
parity, ethnicity/race) and nutrients intake (energy
and protein intake). The dependent variable in this
study is nutritional status. Nutritional status data was
measured by examining the upper arm circumference,
data on educational age, family income,
race/ethnicity, and parity were obtained from
interviews, mother's knowledge data was obtained
from interviews using a questionnaire, and nutrients
intake data was measured using a 24h food recall
questionnaire, to assess consumption of energy and
protein in grams/day, then compared with the
recommended nutritional adequacy rate (RDA) so
that the nutritional adequacy level is obtained. Data
collection was carried out by researchers with the
help of 2 enumerators who had been given previous
guidance and training. The data was analyzed with a
significant degree of 95% (p<0.05) univariate,
bivariate with chi-square test, and multivariate
logistic regression. This research was carried out after
obtaining a research ethical clearance letter from the
Ethics Committee of the Faculty of Medicine, the
University of Lampung with number
3138/UN26.18/PP.05.02.00/2019.
3 RESULTS
The results showed that malnutrition status in
pregnant women was 16 people (22,9%) and good
nutritional status was 54 people (77,1%), low
education was 31 people (44.3) and high education
was 39 people (55,7%), family income is low (less
than the provincial minimum wage) as many as 29
people (41,4%) and family income is high (more than
the provincial minimum wage) as many as 41 people
(58,6%), knowledge of pregnant women is poor 29
people (41,4%) with sufficient knowledge as many as
41 people (58,6%), parity nulli/ primipara as many as
30 people (42,9%) and multi para as many as 40
people (57,1%), Lampung ethnicity as many as 28
people (40%) and non-Lampung was 42 people
(60%), have an inadequate energy intake as many as
31 people (44,3%) and adequate energy intake as
many as 39 people (55,7%) and have an inadequate
protein intake as many as 22 people (31,4%) and
adequate protein intake as many as 48 people (68,6%).
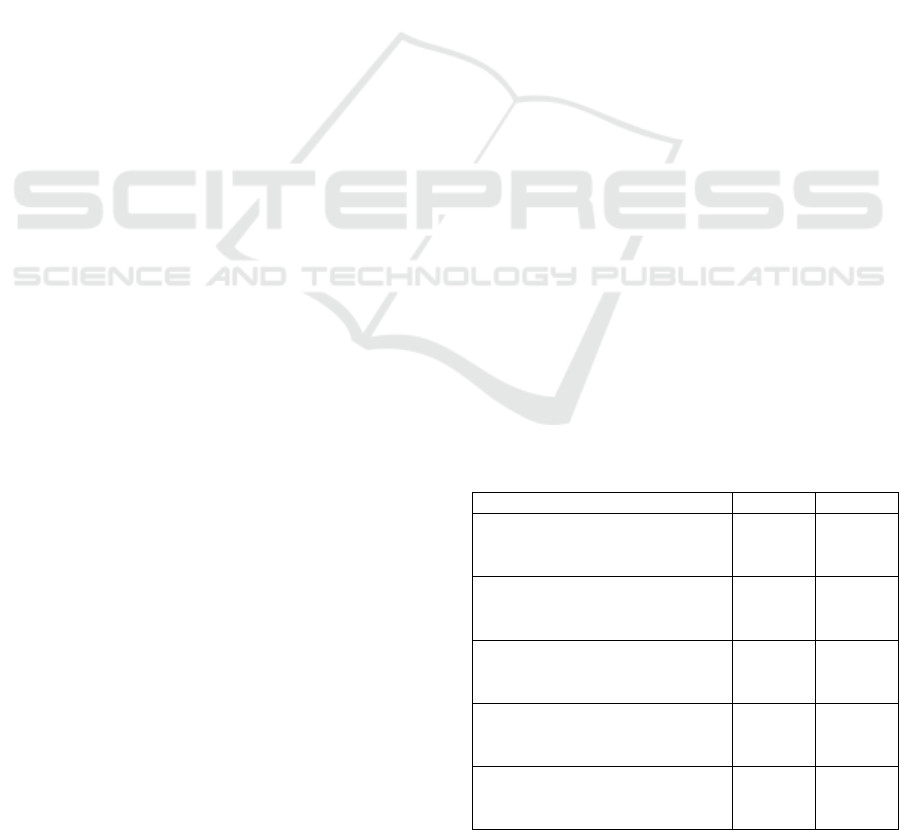
Table 1: Characteristic of study subject
Variable n %
Nutritional Status
a. Malnutrition
b
. Goo
d
nutrition status
16
54
22,9
77,1
Education
a. Low
b
. High
31
39
44,3
55,7
Family income
a. Low
b
. Hi
g
h
29
41
41,4
58,6
Knowledge
a. Poor
b
. Sufficient
29
41
41,4
58,6
Parity
a. Nulli/primiparity
b
. Multipa
r
it
y
30
40
42,9
57,1
The Role of Social Determinants and Nutrient Intake on Nutritional Status of Pregnant Women in Malaria Endemic Areas, Pesawaran
District
11
Race/ethnicity
a. Lampung
b
. Non-Lampung
28
42
40
60
Energy intake
a. Inadequate
b
. Adequate
31
39
44,3
55,7
Protein intake
a. Inadequate
b
. Adequate
22
48
31,4
68,6
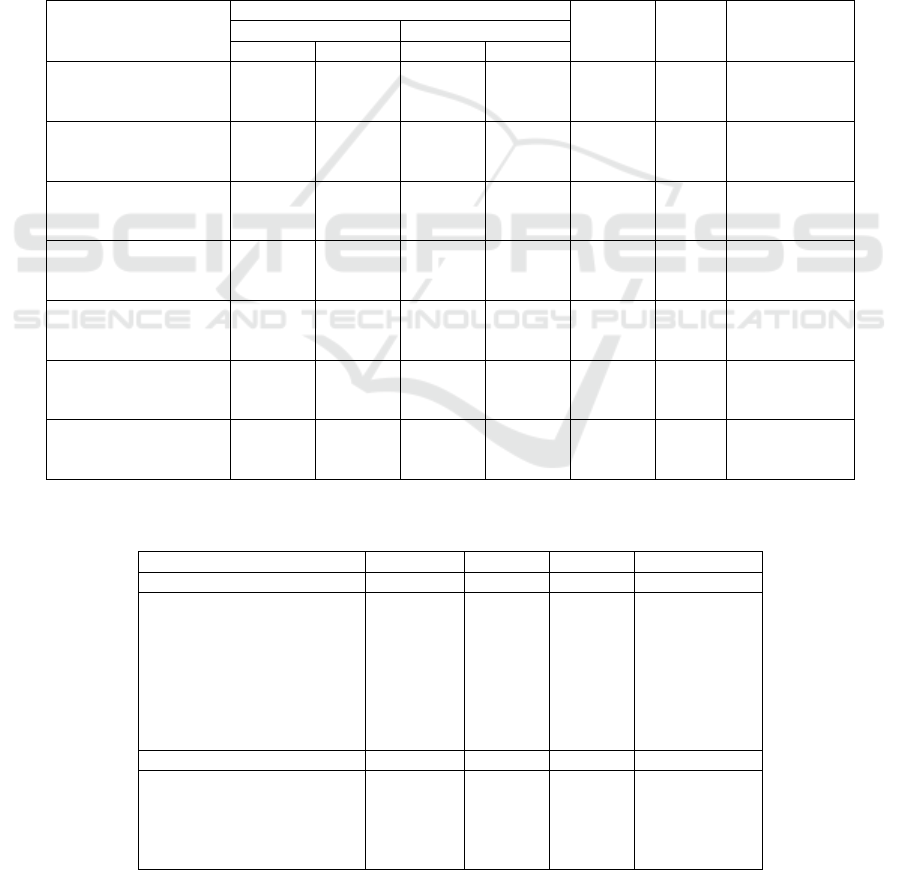
The results of cross-tabulation as shown in Table
2, of pregnant women with low education and
malnutrition, were 38,7% higher than those with high
education and malnutrition status, which was 10,3%.
The results showed that education had a role in the
nutritional status of pregnant women (p = 0,011) and
low education was a risk factor for malnutrition in
pregnant women with OR = 5,5 (95% CI; 1,56-19,52),
which means the pregnant women with low education
are 5,5 times more likely to suffer from malnutrition
than those with high education.
The results of cross-tabulation as shown in table 2,
of pregnant women with family incomes low (less
than the provincial minimum wage) and malnutrition,
were 41,4% greater than family incomes high (more
than the provincial minimum wage) and malnutrition,
which was 9,8%. The results showed that family
income had a role in the nutritional status of pregnant
women (p = 0,005) and low family income (less than
the provincial minimum wage) was a risk factor for
malnutrition in pregnant women with OR = 6,5 (95%
CI; 1,83-23,22), which means that pregnant women
whose family income is low (less than the provincial
minimum wage) will be 6,5 times greater risk of
suffering from malnutrition than those whose family
income is high (more than the provincial minimum
wage).
The results of cross-tabulation as shown in table
2, of pregnant women with poor knowledge and
malnutrition, are 37,9% greater than those with
sufficient knowledge malnutrition, which is 12,2%.
The results showed that knowledge played a role in
the nutritional status of pregnant women (p = 0,025)
and poor knowledge of mothers was a risk factor for
malnutrition in pregnant women with OR = 4,4 (95%
CI; 1,32-14,59), which meaning that pregnant women
with poor knowledge will be at risk of 4,4 times
greater to suffer from malnutrition than those with
sufficient knowledge.
The results of cross-tabulation as shown in table
2, of pregnant women with nulli/primiparity and
malnutrition status, were 36,7% higher than those
with multiparity and malnutrition, which was 12,5%.
The results showed that parity played a role in the
nutritional status of pregnant women (p = 0,036) and
nulli/primiparity was a risk factor for malnutrition in
pregnant women with OR = 4 (95% CI; 1,22-13,39),
which means the mother pregnant with
nulli/multiparity will be at risk of 4 times greater to
suffer from malnutrition than multiparity.
The results of cross-tabulation as shown in table
2, of pregnant women with Lampung race/ethnicity
and malnutrition, were 39,3% greater than those of
non-Lampung ethnicity/race and malnutrition, which
was 11,9%. The results showed that race/ethnicity
had a role in the nutritional status of pregnant women
(p = 0,017) and Lampung race/ethnicity was a risk
factor for malnutrition in pregnant women with OR =
4,7 (95% CI; 1,43-15,94), which means that pregnant
women with Lampung race/ethnicity will have a 4,7
times greater risk of suffering from malnutrition than
those of non-Lampung ethnicity/race.
The results of cross-tabulation as shown in table
2, of pregnant women who have inadequate energy
intake and malnutrition, are 38,7% greater than those
who have sufficient energy intake and malnutrition,
which is 10,3%. The results showed that energy
intake played a role in the nutritional status of
pregnant women (p = 0,011) and inadequate energy
intake was a risk factor for malnutrition in pregnant
women with OR = 5,5 (95% CI; 1,56-19,52), which
means that pregnant women who have inadequate
energy intake will have a 5,5 times greater risk of
suffering from malnutrition than those who have
adequate energy intake.
The results of cross-tabulation as shown in table 2,
of pregnant women who have inadequate protein
intake and malnutrition, are 40,9% greater than those
who have adequate protein intake and malnutrition,
which is 14,6%. The results showed that protein intake
had a role in the nutritional status of pregnant women
(p = 0,033) and inadequate protein intake was a risk
factor for malnutrition in pregnant women with OR =
4 (95% CI; 1,26-13,04), which means the pregnant
women who have inadequate protein intake will have
a 4 times greater risk of suffering from malnutrition
than those who have adequate protein intake.
Based on the results of the bivariate analysis using
the chi-square test, the independent variables were
determined as candidates in the multivariate analysis;
is the variable with p-value <0,25. The candidate
variables included in the multivariate analysis were
education, family income, knowledge, parity,
race/ethnicity, energy intake, and protein intake. The
results of the multivariate analysis using binary
logistic regression with the backward stepwise
method as shown in table 3 found that the factors that
most contributed to the nutritional status of pregnant
women were education, income, knowledge, and
ICSDH 2021 - International Conference on Social Determinants of Health
12
parity. The null hypothesis in the Hosmer and
Lemeshow test has a p-value of 0.998 so that the null
hypothesis is accepted. This means that there is no
difference between the observed value and the
expected value/expectation so that it can be
concluded that the obtained equation is well-
calibrated (Dahlan, 2012).
4 DISCUSSIONS
This study shows that pregnant women in malaria-
endemic areas, Pesawaran District, Lampung
Province, have malnutrition as many as 16 people
(22.9%). The results of this study are lower than the
prevalence of malnutrition in pregnant women in the
vivax malaria-endemic area of Bengkulu city, which
is 40% (Aguscik & Ridwan, 2019) and in the district
of Allada the economic capital of Benin, West Africa,
which is 44,2% (Ouedraogo et al., 2012). Malnutrition
in pregnant women illustrates that pregnant women do
not have adequate reserves of nutrients to provide the
physiological needs of pregnancy, namely hormonal
changes and increase blood volume for fetal growth,
so the supply of nutrients to the fetus is reduced. As a
result, the growth and development of the fetus are
harms and is born with a low weight (SACN, 2011;
Sgarbieri & Pacheco, 2017).
Table 2: The role of social determinants and nutrients intake on nutritional status in pregnant woman
Variable
Nutritional Status
p OR 95% CI Malnutrition Goo
d
n % n %
Education
a. Low
b
. Hig
h
12
4
38,7
10,3
19
35
61,3
89,3
0,011 5,5 1,56- 19,52
Family income
a. Low
b
. Hig
h
12
4
41,4
9,8
17
37
58,6
90,2
0,005 6,5 1,83- 23,22
Knowledge
a. Poor
b
. Sufficien
t
11
5
37,9
12,2
18
36
62,1
87,8
0,025 4,4 1,32- 14,59
Parity
a. Nulli/primiparity
b
. Multipa
r
ity
11
5
36,7
12,5
19
35
63,3
87,5
0,036 4 1,22- 13,39
Race/Etnic
a. Lampung
b
. No
n
lampung
11
5
39,3
11,9
17
37
60,7
88,1
0,017 4,7 1,43- 15,94
Energy intake
a. Inadequate
b
. Adequate
12
4
38,7
10,3
19
35
61,3
89,7
0,011 5,5 1,56- 19,52
Protein intake
a. Inadequate
b
. Adequate
9
7
40,9
14,6
13
41
59,1
85,4
0,033 4 1,26- 13,04
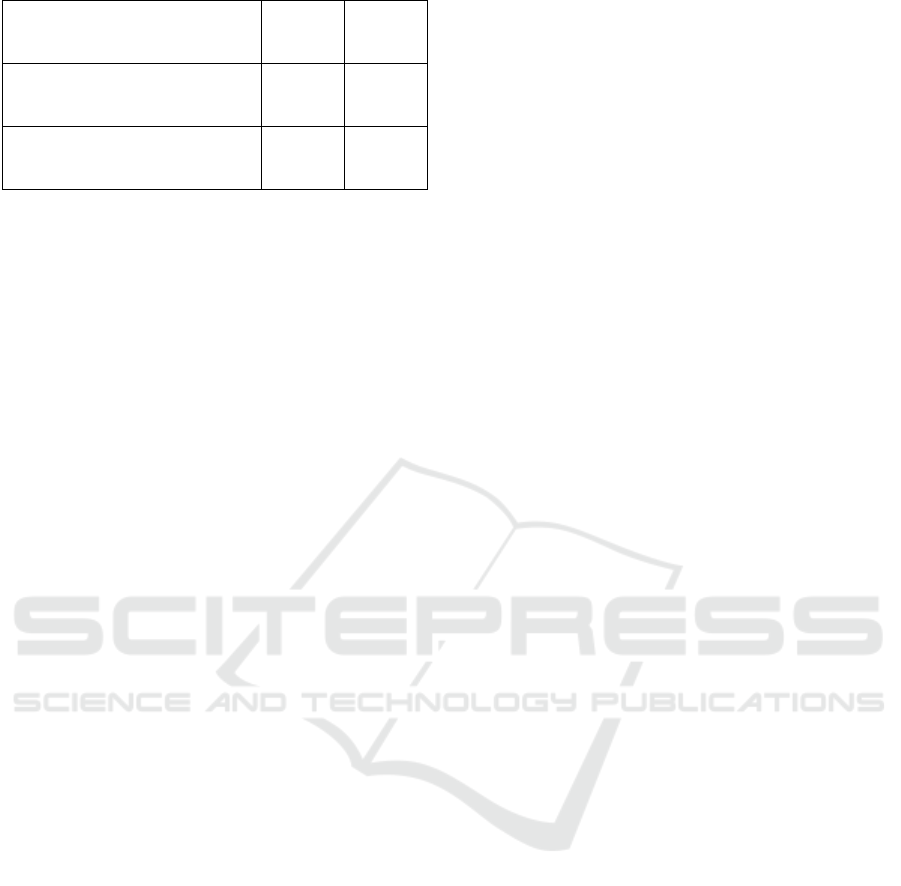
Table 3: Initial model and final model of binary logistic regression analysis of factors contribute to the nutritional status of
pregnant women
B
p
OR 95% CI
Initial Model
a. Education
b. Family income
c. Knowledge
d. Parity
e. Race/Ethnic
f. Energy intake
g. Protein intake
Constan
t
2,014
2,152
1,804
1,865
1,005
0,072
0,330
-12,374
0,03
0,017
0,036
0,060
0,229
0,938
0,691
7,4
8,6
6
6,4
2,7
1
1,3
1,21-46,31
1,47-50,21
1,12-32,75
0,92-44,98
0,53-14,04
0,17-6,5
0,27-7,06
Final Model
a. Education
b. Family income
c. Knowledge
d. Parity
Constan
t
2,377
2,435
1,773
2,136
-11,490
0,008
0,004
0,028
0,012
10,7
11,4
5,8
8,4
1,86-62,05
2,14-60,86
1,21-28,52
1,61-44,48
The Role of Social Determinants and Nutrient Intake on Nutritional Status of Pregnant Women in Malaria Endemic Areas, Pesawaran
District
13

Based on the results of the analysis obtained the following equation:
Malnutrition in pregnant women= -11.49 + (2,377*low education) + (2,435*low family income) +
(1,773*poo
r
knowled
g
e) + (2,136*nulli/multiparit
y
)
(1)
Pregnant women are more at risk of contracting
malaria and suffer more severe consequences if they
get malaria compared to women who are not pregnant
(Schantz-Dunn & Nour, 2009). In addition, malaria
also harms the fetus it contains. Malaria in pregnant
women contributes to mother, infant, and neonatal
mortality because it can cause complications in
pregnant women such as anemia, fever,
hypoglycemia, cerebral malaria, pulmonary edema,
and sepsis (Saba, Sultana & Mahsud, 2008). The fetus
it contains causes low birth weight, premature birth,
stillbirth, congenital malaria, and others (Guyatt &
Snow, 2004). Research in India shows that the
prevalence of malaria in pregnant women is higher
than in women who are not pregnant (Singh, Shukla
& Sharma, 1999).
The results of this study stated that education
plays a role in the nutritional status of pregnant
women in malaria-endemic areas. Low education is a
risk factor for malnutrition in pregnant women,
pregnant women with basic education have a 5,5
times greater risk of experiencing malnutrition than
higher education. Educational factors affect the diet
of pregnant women, higher education levels are
expected to have better knowledge and information
about nutrition so that they can meet their nutritional
intake (Goodarzi-Khoigani et al., 2018). Low
education will cause nutritional knowledge by
pregnant women to be also low, thus affecting food
intake. Food intake plays a direct role in the
nutritional status of pregnant women
(Teweldemedhin et al., 2021).
Education also affects income. Higher education
will make a person get wider opportunities to get a
better job with a bigger income. Meanwhile, people
with low education get jobs with small incomes.
Family income is one of the factors that determine the
amount of food available in the family so that it also
determines the nutritional status of the family (Nofita
& Darmawati, 2016).
The results showed that family income played a
role in the nutritional status of pregnant women in
malaria-endemic areas. Low income (less than the
provincial minimum wage) is a risk factor for
malnutrition in pregnant women, pregnant women
with low income (less than the provincial minimum
wage) have a 6,5 times greater risk of experiencing
malnutrition than high income (more than the
provincial minimum wage). The results of this study
are in line with the research of Serbesa, Iffa & Geleto
(2019) which states that low economic status is
associated with malnutrition (p = 0.035) in pregnant
women and lactating mothers at the Miesso Health
Center, Ethiopia. Based on the Institute of Medicine
& National Research Council (2015) and Jaffee et al.
(2019), families with low economic levels will
usually spend part of their income on food.
Meanwhile, the more money, the better the food
obtained because some of the income is used to buy
food ingredients as desired. Economic status affects a
person's nutritional status. Especially if the person
concerned lives below the poverty line or in a pre-
prosperous family, it is useful to ascertain whether the
mother is capable of buying and choosing foods with
high nutritional value.
The results of the study stated that knowledge
plays a role in the nutritional status of pregnant
women in malaria-endemic areas. Poor knowledge is
a risk factor for malnutrition in pregnant women,
pregnant women with poor knowledge have a 4,4
times greater risk of experiencing malnutrition than
sufficient knowledge. The results of this study are
following the research of Manaf et al. (2014) which
states that nutritional knowledge score was positively
correlated with gestational weight gain (r = 0.166, p
< 0.05) in pregnant women from two selected private
hospitals in Klang Valley, Malaysia. Based on
Hamulka et al. (2018), the level of knowledge
determines the behavior of food consumption, one of
which is through nutrition education. Nutrition
education seeks to increase knowledge and improve
food consumption habits. Sakamaki et al. (2005) said
that nutrition knowledge has an important role in
using the right food, so that good nutritional status
and status can be achieved. Knowledge is very
important in determining whether or not in choosing
the right food consumption which will ultimately
affect their health status.
The results showed that parity had a role in the
nutritional status of pregnant women in malaria-
endemic areas. Low parity (nulli/primiparity) is a risk
factor for malnutrition in pregnant women, pregnant
women with low parity (nulli/primiparity) have a 4
times greater risk of experiencing malnutrition than
high parity (multiparity). The results of this study are
following the research of Kumera et al., (2018) which
states that parity is related to the nutritional status of
pregnant women (p = 0.04) in pregnant women
ICSDH 2021 - International Conference on Social Determinants of Health
14

attending antenatal care at the University of Gondar
Hospital, Northwest Ethiopia.
Low parity is related to low knowledge and
experience when a woman is pregnant, thus affecting
food selection, food intake, and nutritional status
(Kumera et al, 2018). The risk of the occurrence of
malnutrition in pregnant women who have never
given birth, but if the mother has good knowledge
about the nutritional status of pregnant women which
is part of efforts to optimize the mother's ability so
that pregnant women are expected in third-semester
pregnancy has a good nutritional status as well
(Hamel et al, 2015).
The results showed that race/ethnicity played a
role in the nutritional status of pregnant women in
malaria-endemic areas. Lampung race/ethnicity is a
risk factor for malnutrition in pregnant women,
pregnant women with Lampung race/ethnicity have a
4,7 times greater risk of experiencing malnutrition
than non-Lampung races/ethnicities. Lampung is one
of the tribes a patrilineal kinship system, which is a
legal society whose members draw their lineage
upward through the father's line, the father from the
father, and continues upwards so that finally a man is
found as his ancestor. The legal consequence arising
from this patrilineal system is that the wife because of
her marriage usually marriage with an honest money
payment system), is removed from her family, then
enters and becomes her husband's family. It is men
who play a role, o that even traditional positions are
controlled by men. This shows that the position of a
husband is higher than the position of his wife, the
wife is a companion in upholding the household, the
wife follows her husband's kinship after marriage and
the husband is the head of the family in the household.
It is possible if the wife (preconception woman) of the
Lampung race experiences malnutrition caused by
eating behavior by prioritizing her husband, while the
wife will eat when her husband and children have
finished eating or just finished eating the existing
food (Destryana, 2017).
The results of the study stated that energy intake
plays a role in the nutritional status of pregnant
women in malaria-endemic areas. Inadequate energy
intake is a risk factor for malnutrition in pregnant
women, pregnant women with inadequate energy
intake have a 5,5 times greater risk of experiencing
malnutrition than adequate energy intake. The results
of this study are following the research of Desyibelew
& Dadi (2019) which states that energy intake is
related to the nutritional status of pregnant women.
The lower the energy intake of pregnant women, the
lower the nutritional status. The decrease in
nutritional status is caused by the lack of food
consumed both in quality and quantity.
Food intake is very influential on a person's
nutritional status. If a person's food intake is low and
unbalanced, it can lead to malnutrition. If the food
intake (energy) is smaller than the energy expended,
there will be an energy deficit and a decrease in body
weight which in turn leads to poor nutritional status.
On the other hand, if the energy expended is greater
than the energy expended, there will be excess energy
that will be stored as body fat and can lead to obesity.
Lack of energy from food intake causes the body to
take up stored energy reserves. If this happens
continuously then a person can become
malnourished. Pregnant women need additional
energy for the growth and development of the fetus,
placenta, breast tissue, and fat reserves (National
Research Council, 1989; WHO, 2003).
The results of this study showed that protein
intake played a role in the nutritional status of
pregnant women in malaria malaria-
endemicInadequate protein intake is a risk factor for
malnutrition in pregnant women, pregnant women
with less protein intake have a 4 times greater risk of
experiencing malnutrition than adequate protein
intake. The results of this study are in following of
Kurniasari et al. (2018) which states that protein
intake is related to the nutritional status of pregnant
women in the city of Semarang (p = 0,002) with a
positive correlation (r = 0,502), which means that the
lower the protein intake of pregnant women, the
lower the nutritional status. The role of protein in
building the structure of body tissues becomes the
final part to supply energy needs when carbohydrate
and fat intake is reduced. Intake of fat and
carbohydrates as a comparison of protein intake in its
role as an alternative energy source.
Based on the results of the multivariate analysis,
it was found that the most important factors on the
nutritional status of pregnant women in malaria-
endemic districts, were social determinants, namely
education, family income, knowledge and parity.
Based on the OR value, the biggest social determinant
as a risk factor for malnutrition in pregnant women is
family income, followed by education, parity, and
knowledge of pregnant women. Family income is the
biggest risk factor, this is possible because income
will determine the amount of food that can be
purchased so that it directly plays a role in the food
intake and nutritional status of pregnant women.
5 CONCLUSIONS
The most influential factors on the nutritional status
of pregnant women in the malaria-endemic areas of
Pesawaran district are social determinants, namely
education, family income, knowledge, and parity.
However, food intake (energy and protein) is a direct
factor that plays a role in the nutritional status of
The Role of Social Determinants and Nutrient Intake on Nutritional Status of Pregnant Women in Malaria Endemic Areas, Pesawaran
District
15

pregnant women, and food intake is influenced by
social determinants.
REFERENCES
Aguscik, R. 2019. Pengaruh status gizi terhadap kejadian
anemia pada ibu hamil di daerah endemik malaria kota
bengkulu. Jurnal Kesehatan Poltekkes Palembang,
14(2), 97-100.
Destriyana, M., 2017. Hubungan Persepsi Budaya Dan Ras
Terhadap Risiko Kurang Energi Kronis (KEK) Pada
Wanita Usia Subur (WUS) Di Kecamatan Terbanggi
Besar Kabupaten Lampung Tengah. Skripsi.
Universitas Lampung: Bandar Lampung.
Desyibelew D & Dadi AF, 2019. Burden and determinants
of malnutrition among pregnant women in Africa: A
Systematic Review and Meta-Analysis. PLOS Global
Public Health, 14(9), e0221712, 1-19.
Dinas Kesehatan Kabupaten Pesawaran (Dinkes
Pesawaran). 2017. Profil Kesehatan Kabupaten
Pesawaran 2016.Dinkes Pesawaran. Pesawaran.
Dinas Kesehatan Kabupaten Pesawaran (Dinkes
Pesawaran). 2019. Profil Kesehatan Kabupaten
Pesawaran 2018.Dinkes Pesawaran, Pesawaran.
Goodarzi-Khoigani, M., Moghadam, M. H. B.,
Nadjarzadeh, A., Mardanian, F., Fallahzadeh, H., &
Mazloomy-Mahmoodabad, S. 2018. Impact of nutrition
education in improving dietary pattern during
pregnancy based on pender’s health promotion model:
A Randomized Clinical Trial. Iranian Journal of
Nursing and Midwifery Research, 23(1), 18-25.
Gulo, R, 2008. Status Kurang Energi Kronis dan Anemia
Pada Ibu Hamil di Daerah Endemis Malaria Kabupaten
Nias. Tesis. FK UGM, Yogyakarta.
Guyatt, H. L. & Snow, R. W. 2004. Impact of malaria
during pregnancy on low birth weight in Sub-Saharan
Africa. Clin Microbiol Rev, 17(4), 760–769.
Hamel, C., Enne, J., Omer, K., Ayara, N., Yarima, Y.,
Cockcroft, A., et al. 2015. Childhood malnutrition is
associated with maternal care during pregnancy and
childbirth: A Cross-sectional study in Bauchi and Cross
River States, Nigeria. Journal Of Public Health
Research 4(408), 58-64.
Hamulka, J., Wadolowska, L., Hoffmann, M.,
Kowalkowska, J., & Gutkowska, K. 2018. Effect of an
education program on nutrition knowledge, attitudes
toward nutrition, diet quality, lifestyle, and body
composition in polish teenagers. The ABC of Healthy
Eating Project: Design, Protocol, and Methodology.
Nutrients, 10 (1439), 1-23.
Institute of Medicine and National Research Council. 2015.
A Framework for Assessing Effects of the Food
System. The National Academies Press: Washington
DC.
Jaffee, S., Henson, S., Unnevehr, L., Grace, D., & Cassou,
E., 2019. World Bank Group, Washington DC.
Kumera, G., Gedle, D., Aleber, A., Feyera, F., & Eshetie,
S., 2018. Undernutrition and its association with socio-
demographic, anemia and intestinal parasitic infection
among pregnant women attending antenatal care at The
University of Gondar Hospital, Northwest Ethiopia.
Maternal Health, Neonatology, and Perinatology,
4(18), 1-10.
Kurniasari, R., Cahya, F., Widiastuti, Y., Adi, P., &
Zainudin, A. 2018. Hubungan tingkat asupan energi,
protein, dan zat besi (Fe) dengan kejadian anemia dan
risiko Kekurangan Energi kronis (KEK) pada ibu hamil
di Kota Semarang. Health Science Growth (HSG)
Journal, 3(1), 77-90.
Ministry Of Health. 2015. Pedoman Penanggulangan
Kurang Energi Kronik (KEK) Pada Ibu Hamil. Ditjen
Bina Gizi dan KIA Kemenkes RI, Jakarta.
Ministry Of Health. 2016. Situasi Balita Pendek. Pusat Data
dan Informasi, Kemenkes RI, Jakarta.
Ministry Of Health. 2017. Surveilans Gizi. Pusat
Pendidikan Sumber Daya Kesehatan Kemenkes RI,
Jakarta.
Ministry Of Health. 2018. Laporan Nasional RISKESDAS
2018. Balitbangkes Kemenkes RI, Jakarta.
Ministry Of Health. 2020. RPJMN dan RENSTRA
Kementerian Kesehatan, Kemenkes RI, Jakarta.
Manaf, Z. A., Johari, N., Mei, L. Y., Yee, N. S., Yin, C. K.,
& Teng, L. W. 2014. Nutritional status and nutritional
knowledge of Malay pregnant women in selected
private hospitals in Klang Valley. Jurnal Sains
Kesihatan Malaysia (Malaysian Journal of Health
Sciences), 12(2).
National Research Council, 1989. Diet And Health.
National Academy Press, Washington DC.
Ouédraogo, S., Koura, G. K., Accrombessi, M. M., Bodeau-
Livinec, F., Massougbodji, A., & Cot, M. 2012.
Maternal anemia at first antenatal visit: prevalence and
risk factors in a malaria-endemic area in Benin. The
American journal of tropical medicine and hygiene,
87(3), 418.
Saba, N., Sultana, A. and Mahsud, I., 2008. Outcome and
complications of malaria in pregnancy. Gomal Journal
of Medical Sciences, 6(2), 98-101.
Sakamaki, R., Toyama, K., Amamoto, R., Liu, C.J. and
Shinfuku, N., 2005. Nutritional knowledge, food habits
and health attitude of Chinese university students–a
cross sectional study–. Nutrition journal, 4(1), 1-5.
Schantz-Dunn, J. and Nour, N.M., 2009. Malaria and
pregnancy: a global health perspective. Reviews in
obstetrics and gynecology, 2(3), 186-192.
Prentice, A. and Williams, A., 2011. The influence of
maternal, fetal and child nutrition on the development
of chronic disease in later life. The Stationery Office.
Serbesa, M.L., Iffa, M.T. and Geleto, M., 2019. Factors
associated with malnutrition among pregnant women
and lactating mothers in Miesso Health Center,
Ethiopia. European Journal of Midwifery, 3, 1-5
Sgarbieri, V.C. and Pacheco, M.T.B., 2017. Human
development: from conception to maturity. Brazilian
Journal of Food Technology, 20.
Singh, N., Shukla, M.M. and Sharma, V.P., 1999.
Epidemiology of malaria in pregnancy in central India.
ICSDH 2021 - International Conference on Social Determinants of Health
16

Bulletin of the World health Organization, 77(7), 567-
572.
Steketee, R.W., Nahlen, B.L., Parise, M.E., Menendez, C.
2001. The Burden of Malaria in Pregnancy in Malaria-
endemic Area. Am J Trop Med Hyg, 64(1-2 Suppl), 28-
35.
Teweldemedhin, L.G., Amanuel, H.G., Berhe, S.A.,
Gebreyohans, G., Tsige, Z. and Habte, E., 2021. Effect
of nutrition education by health professionals on
pregnancy-specific nutrition knowledge and healthy
dietary practice among pregnant women in Asmara,
Eritrea: a quasi-experimental study. BMJ Nutrition,
Prevention & Health, 181-194.
United Nations Children’s Fund (UNICEF). 2015.
UNICEF’s approach to scaling up nutrition for mother
and their children. Nutrition Section, Programme
Division United Nations Children’s Fund (UNICEF),
New York.
Sugeng, W., Annas, B., Titus, P.H., Iskari, N., Nanang, P.,
Ratih, P.P., Dewi, E. and Farha, F., 2020. Study causes
of chronic energy deficiency of pregnant in the rural
areas. International Journal of Community Medicine
and Public Health, 7(2), 443-448.
World Health Organization (WHO), 2003. Diet, Nutrition,
and The Prevention Of Chronic Diseases. WHO
Library Cataloguing-in-Publication Data: Geneva.
The Role of Social Determinants and Nutrient Intake on Nutritional Status of Pregnant Women in Malaria Endemic Areas, Pesawaran
District
17
