
Personalising Exergames for the Physical Rehabilitation of Children
Affected by Spine Pain
Cristian G
´
omez-Portes
a
, Carmen Lacave
b
, Ana I. Molina
c
, David Vallejo
d
and Santiago S
´
anchez-Sobrino
e
School of Computer Science, University of Castilla-La Mancha, Paseo de la Universidad 4, 13071 Ciudad Real, Spain
Keywords:
Rehabilitation, Exergames, Spine Pain, e-Health.
Abstract:
Injuries or illnesses related to the lumbar spine need great clinical care as they are one of the most prevalent
medical conditions worldwide. The use of exergames has been widespread in recent years and they have been
put forward as a possible solution for motivating patients to perform rehabilitation exercises. However, both
customizing and creating them is still a task that requires considerable investment both in time and effort. In
this project we present a language with which we have designed a system based on the physical rehabilitation
of patients suffering from bone-marrow injuries, which enables customization and generation of exergames.
To assess the system, we have designed an experiment with an exergame based on the physical rehabilitation
of the lumbar spine. The purpose of this was to assess its understanding and suitability, whose result reveals
that the tool is fun, interesting and easy to use. It is hoped that this approach can be used to considerably
reduce the complexity of creating new exergames, as well as supporting the physical rehabilitation process of
patients with lower back pain.
1 INTRODUCTION
In a systematic analysis (Murray et al., 2012) of the
research, called, The Global Burden of Disease 2010,
it was estimated that lower back pain is one of the
10 most frequent injuries and illnesses worldwide. It
has been calculated that every year between 6.3% and
15.4% of people suffer from lower back pain, while
any type of this complaint varies between 1.5% and
36% per year (Hoy et al., 2010). Moreover, in mon-
etary terms, treating lower back pain complaints is
an enormous burden on industries and governments,
which is even more acute for patients and families
dealing with them (Duthey, 2013).
Unfortunately, this type of condition is rather
frequent in children and teenagers between 10 and
16 (Jones et al., 2004), who need to perform rehabil-
itation exercises, which have been recommended by
a physiotherapist, at home, and that are essential for
reducing the area of pain.
Today, there are some relatively new treat-
a
https://orcid.org/0000-0002-9603-9481
b
https://orcid.org/0000-0003-2770-8482
c
https://orcid.org/0000-0002-3449-2539
d
https://orcid.org/0000-0002-6001-7192
e
https://orcid.org/0000-0001-6620-1719
ments for physical rehabilitation, the main aim of
which are to improve the quality of life of the pa-
tients (O’Sullivan et al., 2019). Among these are
tele-medicine-based solutions, aimed at making these
types of tasks accessible and providing patients with
a greater degree of independence (Palacios-Navarro
et al., 2015; Lai et al., 2015). There is even a line of
research in which gamification-based techniques and
serious games are used, in order to create technolog-
ical solutions which have motivational value to en-
courage patients to perform more rehabilitation tasks
or to enjoy them whilst reducing their pain (Deterding
et al., 2011; McCallum, 2012).
However, these approaches are not enough in
themselves to tackle two challenges: i) motivating pa-
tients to continuously carry out the programme of ex-
ercises assigned to them and ii) assessing whether the
exercises have been performed correctly. Generally, a
child or teenager will perform the exercises at home,
but without the necessary motivation, the routine re-
quired to do them will fade, and thus the desired thera-
peutic effect will be lost. Moreover, from the point of
view of the physiotherapist, it is advisable to, firstly,
have an application or game which encourages the pa-
tient to perform the exercises so that he or she can be
automatically guided, and to ensure the exercises are
carried out correctly. In other words, to provide cus-
Gómez-Portes, C., Lacave, C., Molina, A., Vallejo, D. and Sánchez-Sobrino, S.
Personalising Exergames for the Physical Rehabilitation of Children Affected by Spine Pain.
DOI: 10.5220/0009574005330543
In Proceedings of the 22nd International Conference on Enterprise Information Systems (ICEIS 2020) - Volume 2, pages 533-543
ISBN: 978-989-758-423-7
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
533

tomized activities according to the patients and their
type of illnesses so as to obtain a therapy that is both
safe and effective (Pirovano et al., 2016).
In this research, the design, developing and val-
idating a system focused on rehabilitating children
and teenagers suffering from some sort of lower back
pain, is set out, making use of development kits
with advanced artificial intelligence sensors, such as
Azure Kinect DK
TM
device, so as to accurately track
skeletons. In this way, the patient naturally inter-
acts with the system, simulating rehabilitation exer-
cises by means of motivating games. The rehabili-
tation tasks are customized with a language we have
defined as Personalised Exergames Language (PEL)
which, on the basis of the GL Transmission Format
specification (glTF) (Robinet et al., 2014), keep both
information about the exergame mechanics, gamifica-
tion elements and metrics for measuring how the pa-
tients are progressing. This information is defined by
therapists based on the patient’s condition, which is
converted into PEL sentences for automatically gen-
erating exergames. Therefore, a co-creative approach
is established between therapists, patients and devel-
opers.
By way of validation, the system has been as-
sessed by 23 potential users, being the main objective
to obtain feedback about its understanding and suit-
ability.
The remainder of the article is structured as fol-
lows: The section 2 positions our research within the
context of other works in the field. Then, the sec-
tion 3 sets out the system architecture. Subsequently,
the section 4 describes the experiment carried out and
the results obtained. Finally, in the section 5, the con-
clusions drawn are described as well as future lines of
research.
2 RELATED WORK
At present, there are tools for rehabilitation whose ex-
ercises are automatically analysed by machines which
use precise skeleton tracking or computer vision tech-
niques. The latter have traditionally been based on
using the Kinect device (Webster and Celik, 2014;
Da Gama et al., 2015), a low cost hardware solution
whose effectiveness has been seen in the field of phys-
ical rehabilitation (Clark et al., 2012; Mobini et al.,
2014; Mousavi Hondori and Khademi, 2014). Simi-
larly, there are solutions on the market which are ori-
entated at training and fitness, whose aim is to attract
specific targets, apart from providing remote rehabili-
tation from home (Deutsch et al., 2009; Esculier et al.,
2012). However, some authors shows scepticism to-
wards this approach, claiming that the lack of cus-
tomization of these games may make injuries more
likely (Sparks et al., 2011).
In light of this issue, various authors have set out a
series of considerations to ensure that exergames are
both efficient and safe. In (McCallum, 2012), one of
the most outstanding proposals is to control the game
experience, given that, depending on whether the tar-
get user is a child or adult, the original concept of
the game may be misinterpreted. A similar approach
is presented in (Wiemeyer et al., 2015), which pro-
vides recommendations for the optimal design of ex-
ergames. To take an example, it identifies postures
which ensure patient safety when in rehabilitation,
or adapts the game design to the patient characteris-
tics. A slightly different approach, which is presented
in (Pirovano et al., 2016), provides a methodology
split into four phases for creating and designing ef-
ficient and safe therapeutic exergames.
The use of exergames and gamification techniques
has also been studied in the literature to assess their
effectiveness in the rehabilitation process. A system-
atic review, shown in (Matallaoui et al., 2017), an-
alyzes different types of systems and their context,
the game elements used and the results yielded from
them, providing positive outcomes both in patient
conduct and their well-being. In a similar vein, the
research presented in (Gonz
´
alez et al., 2018) explores
studies on games and gamification applied to physical
exercise, which finds positive effects in a reduction
in body weight and in encouraging physical exercise.
Similarly, the paper (Katajapuu et al., 2017) shows a
set of exergames evaluated by a group of thirty partic-
ipants, which concludes that video games are useful
in the physical training of elderly people.
There is also a state of the art angle in which
technological solutions orientated at facilitating or au-
tomating the generation of exergames is envisaged.
For example, the TANGO:H (Tangible Goals:Health)
platform (Gonz
´
alez et al., 2013), has a range of func-
tions and contains a graphics editor to help experts
create exercises adapted to patient needs. In this
case, it refers to hospitalized children. Similarly,
in (Hardy et al., 2015), the StoryTec tool has been
envisaged. This was designed to support experts in
the field, such as doctors or therapists, so that they
can adapt and customize games-based training pro-
grammes for elderly and disabled people. In a sim-
ilar vein, the VirtualGym environment is also worth
mentioning (Fernandez-Cervantes et al., 2018), which
has been set out as a cooperative framework in which
medical professionals design exercise routines which
later become games in which an avatar guides the pa-
tient during his or her rehabilitation process.
ICEIS 2020 - 22nd International Conference on Enterprise Information Systems
534
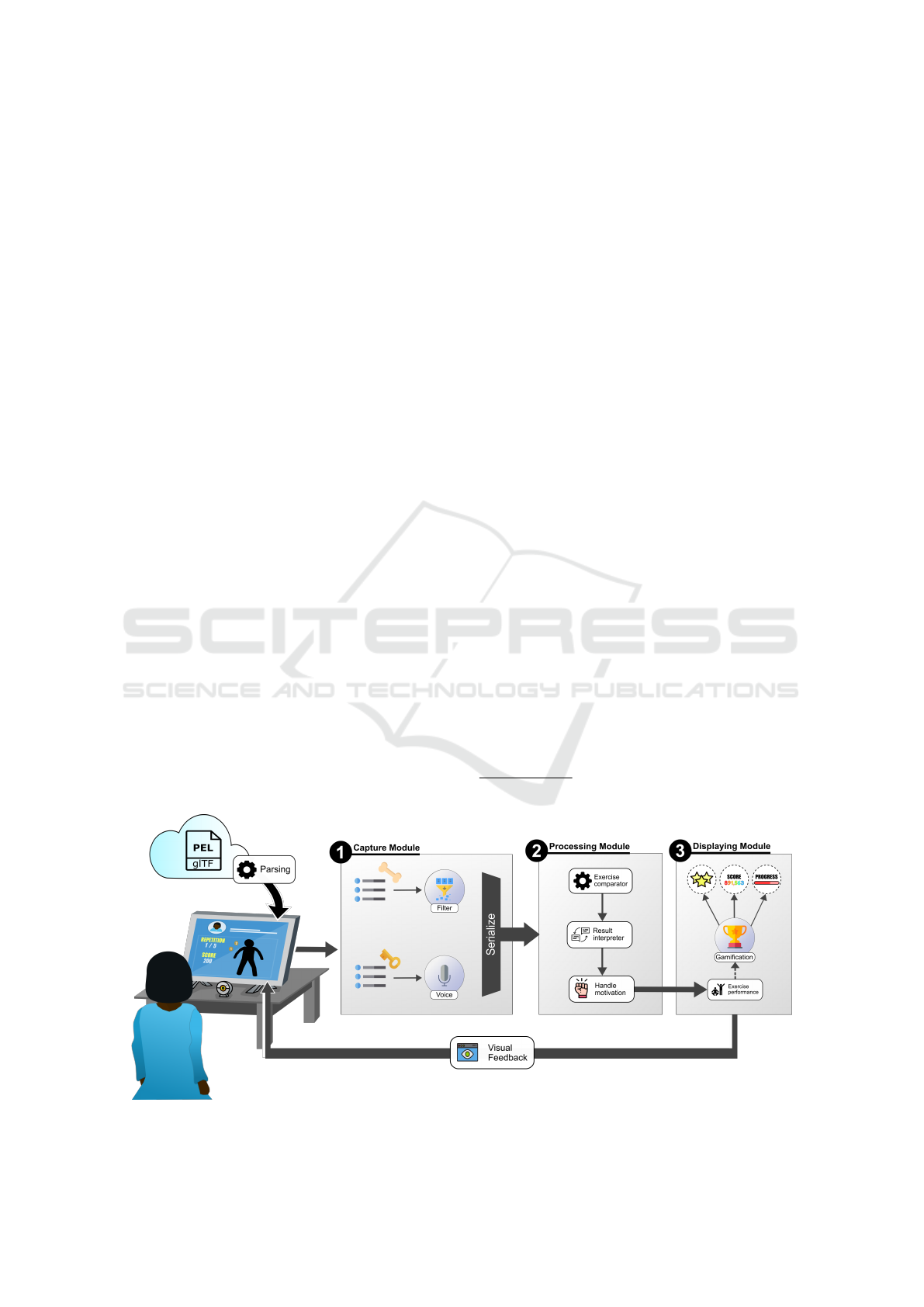
3 ARCHITECTURE
Figure 1 graphically shows the architecture designed
for the rehabilitation process for bone-marrow in-
juries. This approach mainly requires an expert in the
field to participate, namely, a therapist, entrusted with
assigning an exercises routine to the patient. As can
be seen in the figure, the exercises routine is defined
by means of data modelling in .gltf format extended
with our PEL language, which stores all information
relating to the exergame. That is, the game dynam-
ics, graphics, gamification elements, and the different
metrics by which patient participation can be evalu-
ated. In the subsection 3.1, there is an in-depth expla-
nation on the structure of the language we have de-
fined, so as to provide details in the subsection 3.2
on the translation process for this model in order to
automatically generate exergames.
Additionally, this architecture is based on a hard-
ware component for precise skeleton tracking, here
we use Azure Kinect DK
TM
, a device developed by
Microsoft which includes a RGB (Red, Green and
Blue) camera, a depth sensor and several micro-
phones, apart from the software necessary for cap-
turing movements and recognizing voice commands.
The capture module is that which interacts with the
hardware device in order to obtain the information as-
sociated with the position and orientation of the bones
that make up the patient skeleton. This module is re-
sponsible for filtering the data provided by the device,
excluding any information that is not related to the
bones in the rehabilitation exercise. For example, if
patients have to lie down to exercise their backs, and
raise the upper part of their torsos, data related to the
lower part of the hip is omitted. Apart from that, the
capture module also manages voice recognition, as it
enables the voice of the patient to be analysed in order
to perform certain tasks, namely, starting a rehabilita-
tion routine or indicating that the activity has finished.
The processing module carries out two specific
tasks: i) it evaluates the exercise performed by the
patient and ii) it monitors motivation according to
the activity. A games scenario by definition in our
system is made up of an avatar and a sequence of
nodes, called actors, which make up the path a spe-
cific part of the patient’s body must take. To evaluate
the exercise, the module analyses the set of bones that
have interacted with the sequence of actors and the
order in which this interaction has taken place. In this
way, patients are aware of whether they are perform-
ing the exercise correctly, as the module shows scores
as the activity progresses. Furthermore, it helps to
keep them motivated, whether the exercise is being
performed correctly or not, since a high score may
help maintain the rhythm, or even a low score may
help incentivize them to improve.
Finally, the visualization mode is responsible for
showing on the screen how the patient is progressing
in respect to the task performed. This module is in-
terconnected with the processing module, which pro-
vides information in numerical format (score the pa-
tient has, percentage of progress for the activity or
achievements, amongst other items) in a visually at-
tractive format which can easily be interpreted by the
patient in order to capture and maintain their motiva-
tion and attention.
3.1 PEL Structure
PEL comes from a higher level specification, pop-
ularly known as glTF
1
, a relatively new, open for-
1
https://www.khronos.org/gltf/
Figure 1: General overview of the proposed architecture for rehabilitation of patient suffering from bone-marrow injuries.
Personalising Exergames for the Physical Rehabilitation of Children Affected by Spine Pain
535
mat, based on the JSON standard, for distributing 3D
scenes in an efficient and interoperable way. It was
chosen because i) it is an open project, which means
certain parts of the product can be freely changed to
customize it; ii) it is an efficient and interoperable for-
mat; and iii) the extensibility of its data modelling
by which new properties can be added which provide
new opportunities for improving and building on the
specification.
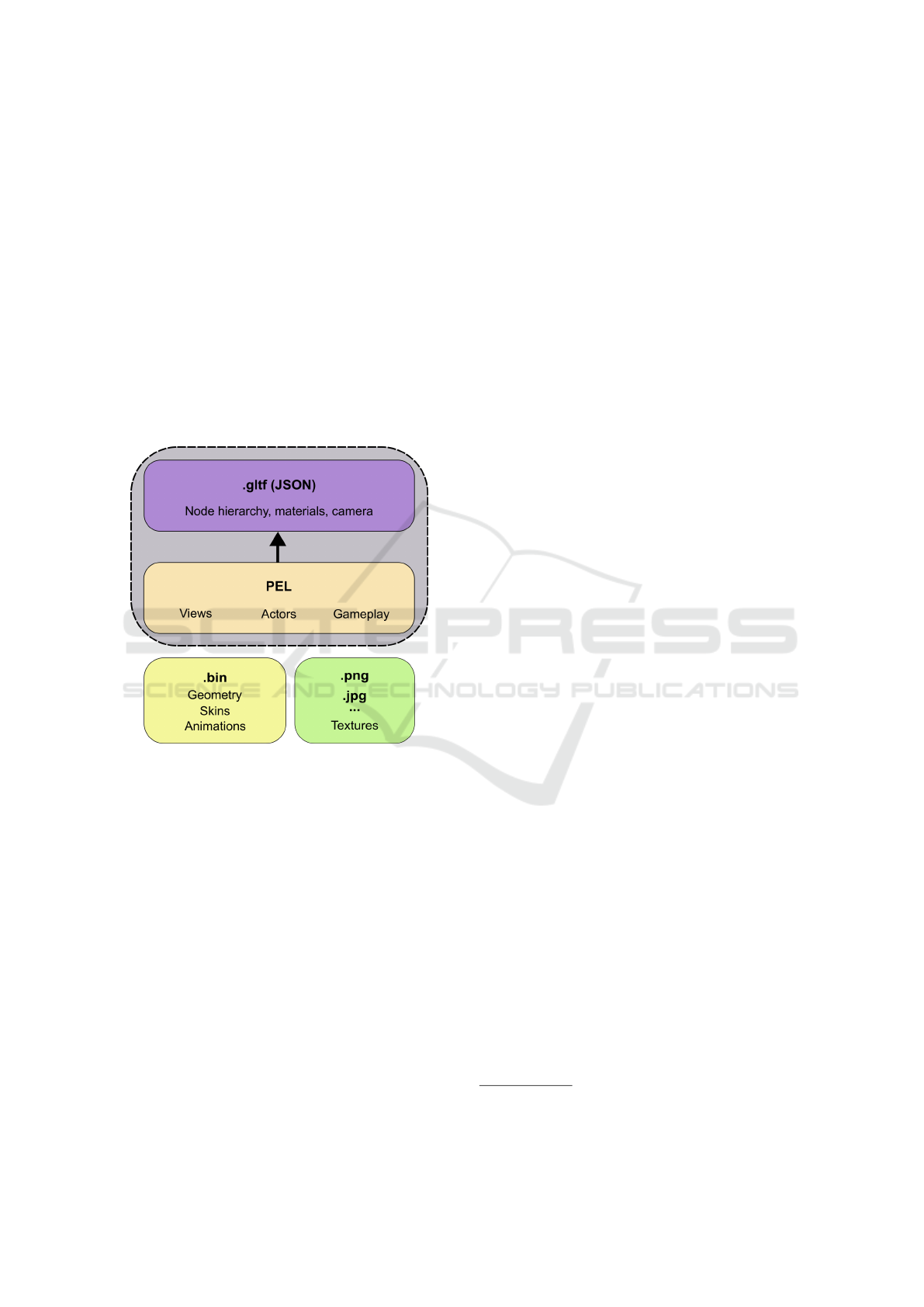
Fundamentally, our language is made up of a se-
ries of components that potentially enable tools to be
developed, which through parsing, automatically gen-
erate games-based exercises focused on rehabilitating
patients. The following points briefly summarize the
elements which define the nature of an exergame with
PEL (see Figure 2):
Figure 2: Representation of an exergame structure using
glTF extended with PEL language.
• Views. Contains three different views which the
game is split into. That is, the language envisages
a tutorial view, where an avatar, using animation,
shows the patient the activity to be carried out; a
scene in which the patient performs the activity
that has been visualized previously, with move-
ments replicated by the avatar; and finally a view
where the results are shown as a result of the ac-
tions carried out by the patient.
• Actors. They represent the elements of the game
that the avatar must interact with. These objects
essentially make up a sequence of the activity the
patient must perform, with behaviour that may be
either static or dynamic. That is, elements that
move in a 3D space through animation, or which
are just fixed elements suspended over a certain
point in the 3D scene. Moreover, these elements
provide visual feedback, which in itself, indicates
that the node must be or has interacted with the
target joint.
• Gameplay. Defines the set of actions the user
must take to complete a repetition of the ex-
ergame. In other words, it specifies the sequence
of the actors and the user interaction mode with
them. Correct execution of the game mechan-
ics deploys gamification elements to capture, in-
terest and motivate the user, which results in in-
creases the score the patient achieves for each rep-
etition, the progress of the activity or on unblock-
ing achievements, for example.
3.2 Automatic Generation of Exergames
An exergame is automatically generated from a hier-
archical analysis of a file with a gltf extension, whose
structure is defined by means of the JSON syntax.
This system has been implemented as an appli-
cation developed with Unity 3D
2
game engine, de-
ployed for Windows and Linux, both of them duly
supported by Azure Kinect DK
3
. This application re-
ceives the contents of a 3D scenario in the way of
a URI (Uniform Resource Identifier), which is sub-
sequently analysed by means of parsing technique in
order to build the game.
The mechanism for adding gITF extensions by
means of the “extras” field have made it possible to
create these type of scenarios. All the elements which
a 3D scenario is made up of (scene, node, camera, ma-
terial, animation, etc.) are added in order to provide
new functions for highly specific cases.
The process for analysing the “extras” field is inte-
grated into the parsing module, which takes the form
of a syntax analyser, based on the gITF implementa-
tion, in order to effectively deserialize the elements
included in the JSON file. In this field the attributes,
which form part of the PEL language, are included to
add specific behaviour so as to support the physical
rehabilitation process for patients.
To each of the “extras” field, we have added an
identifier as a primary property, whose purpose is to
help determine the type of behaviour which should be
assigned to a node (e.g., { "type" : "actor" }).
Therefore, once the object which implements an ex-
tensible field is detected, our parsing module identi-
fies the information to be deserialized so that it be-
haves appropriately when the exergame is running.
2
https://unity.com/es
3
https://azure.microsoft.com/es-es/services/kinect-dk/
ICEIS 2020 - 22nd International Conference on Enterprise Information Systems
536

4 VALIDATION
In order to evaluate the designed system, a quasi-
experiment with potential patients has been carried
out. The purpose of this was to validate the system
in terms of understanding and suitability. The results
of such experiment are described and discussed in this
section.
4.1 Exergame to Evaluate
The architectural design defined in this paper supports
the integration of a wide range of exergames orien-
tated towards different types of injuries, ranging from
lower limbs to upper ones.
Taking advantage of this architecture, an ex-
ergame was developed to motivate potential patients
to perform exercises aimed at the physical rehabili-
tation of the lumbar spine. The exergame was cus-
tomized by a therapist, who defined the therapeutic
objetive, the trajectory of the rehabilitation movement
and the metrics to measure the progress of the patient,
being this information translated into PEL sentences
to automatically generate the game.
This exercise consists in facing up from a lying
down position, raising the upper part of the torso
by about 25 cm with knees bent and feet resting on
the ground. Patients must maintain this position for
2 seconds and then return to their original position.
In essence, the exercise is repeated 5 times, where
the satisfactory realization of each one increases their
score by 200 points.
Figure 3 shows the different views which make up
the exergame designed for the physical rehabilitation
of bone-marrow injuries. In (1) there is a screenshot
of the tutorial view, where the avatar is seen carry-
ing out the movement, which the patient must repli-
cate later on. The participant view (2) reflects how
the patients repeats the movement shown in the pre-
vious view, increasing his or her score each time the
repetition is performed correctly. Note the spherical
blue object (actor), which is used both as a guide for
performing the exercise and as a mechanism for de-
termining the stopping conditions in a repetition. Pa-
tients can interact with the exergame as PEL is highly
flexible and the language is versatile enough to de-
fine these situations. In this case, once the head of the
avatar collides and remains on the sphere for 2 sec-
onds, the repetition finishes and the score increases.
Finally, the results view (3) reflects the indicators en-
tered in PEL language for measuring the exercise per-
formed by the patient.
4.2 Participants and Method
The experiment was carried out by two instructors and
some girls from a rhythmic gymnastics club. Twenty-
three girls were randomly selected, of whom 20, aged
between 11 and 19, agreed to participate in the expe-
rience. Of these, 8 suffered from some type of injury,
mainly related to the spine, which requires rehabil-
itation exercises at home. In order to avoid biasing
the results (McCambridge et al., 2014) and to mo-
tivate their participation (Shull et al., 2007), we ex-
plicitly stated at the beginning of the experience the
information collected would be treated confidentially
and used exclusively for this research. After being in-
formed, girls and their parents gave their consent to
Figure 3: Rehabilitation system in action. (1) tutorial view. (2) Participation view. (3) Result view. (4) Features of the Azure
Kinect DK
TM
device. (5) User using the system.
Personalising Exergames for the Physical Rehabilitation of Children Affected by Spine Pain
537

use their data.
The quasi-experiment was divided into two
phases, conducted in one session of 120 minutes:
• Phase 1 (Preparation Phase). One instructor
presented the system to all participants for ten
minutes. An example of using the system was
projected onto the wall so that the girls may un-
derstand the explanation.
• Phase 2 (Development Phase). Each girl par-
ticipating individually engaged in two activities:
First, they completed the prepared exergame,
which required about 2 minutes; then, they filled
in a questionnaire, which was provided to them
through One Drive Forms. These concerned their
perception of the activity developed, their under-
standing and how suitable they thought the tool
was.
The exergame, used as an exercise for rehabilitat-
ing the spine, was projected onto the wall so that the
girls may better visualize their avatar, as well as the
gamification elements provided by the system.
The questionnaire consisted in 21 items, shown in
Table 1, rated on a five-point Likert scale (1: totally
disagree; 5: totally agree) grouped into five blocks
or dimensions: performance subjective ratings, cog-
nitive load and effort, system utility, usefulness of the
user interface components and TAM-based question-
naire (abbreviated by TAM). (1) The first dimension
(performance subjective ratings), composed of four
items, allowed us to measure the subjective percep-
tion of the users regarding their performance during
the activity, assessing aspects such as their interest
during its execution, their commitment to doing it
correctly, as well as the user-friendliness of the sys-
tem. (2) The next block (cognitive load) was formed
by four items, inspired by the Cognitive Load The-
ory (CLT) (Sweller et al., 1998), which allowed us
to measure two of the types of cognitive load about
the use of a software system: the complexity im-
posed by the task to be performed (intrinsic load)
and the complexity imposed by the use of the soft-
ware and the interaction devices used during the per-
formance of the task (extraneous load). In addition,
two questions were included related to the effort the
users had to make to complete the task. (3) The
third block consisted in four questions related to cer-
tain users’ views: preference for the use of this type
of systems over face-to-face assistance in rehabilita-
tion centres, the system’s game format and finally,
whether they considered that its use might improve
their motivation and constancy in rehabilitation tasks.
(4) In the following block, five items were included
in which users had to assess the degree of usefulness
of each of the main elements of the application’s user
interface (virtual representation of the user, number
of repetitions, score, etc.). (5) Finally, users com-
pleted a questionnaire based on the Technology Ac-
ceptance Method (TAM) framework (Davis, 1993),
which included four items to measure the perceived
user-friendliness, usefulness and intended uses for the
system being evaluated.
To speed up the process of filling in the question-
naire, we used three laptops so that girls may do it in
parallel once they finished the exergame. There was
no time limit for this but, on average, each girl used
about 6 minutes to complete the questionnaire. In ad-
dition, another instructor was in charge of explaining
the meaning of some questions to the youngest girls
who requested them.
4.3 Results and Discussion
The results obtained from the data collected, illus-
trated in Table 1, show that the tool has been very
well received in all dimensions. It should be stressed
that the activity was more fun (item 1) and interest-
ing (item 2) for those girls who had some injury and,
therefore, needed rehabilitation, which seems logical.
Moreover, all participants thought they had tried to do
the activity well (item 3), they had found the system
useful and it had been user-friendly (item 18).
All participants considered that the cognitive load
of the activity was not very high (items 5, 8). Fur-
thermore, most of them tried to concentrate on the
activity (item 6). However, item 7 received a very
high score. This may be because the question was
posed in the opposite way to the others. Therefore, the
results show inconsistencies; probably because some
girls were confused when interpreting the values of
the answers.
On the other hand, the injured girls valued the
system more useful (items 9, 10) because they were
aware of what it meant for them to perform exercises
at home (without going to rehab centre). One highly
important point to consider is that the system can be
motivating (item 11), since one of the disadvantages
to rehabilitation for young people is the lack of mo-
tivation to do the exercises at home. Perhaps moti-
vation is key to understanding the greater enthusiasm
of the injured girls to using the system at home (item
20), as well as to recommending to friends (item 21).
As for, the usefulness of the interface elements
(items 13-17), they received positive appraisal with
the “score” being the best-rated one (item 15). Apart
from this, it is needed to bear in mind that gamifica-
tion has a crucial role in motivating a patient, espe-
cially children.
ICEIS 2020 - 22nd International Conference on Enterprise Information Systems
538

Table 1: Descriptive statistics of the dimensions evaluated. *Mean and standard deviation are shown (in parentheses).
Dimension Item Mean Mode
Injured Not Injured Injured Not Injured
Activity Perception
1. This activity has been fun for
me.
5.00 (0.00)* 4.33 (0.65)* 5 4
2. I found this activity interesting.
4.88 (0.35)* 4.75 (0.62)* 5 5
3. I have worked to do it well.
4.88 (0.35)* 4.92 (0.29)* 5 5
4. It’s been easy for me to learn
how to use this system.
4.88 (0.35)* 4.83 (0.39)* 5 5
Cognitive Load
5. The activity required a lot of
concentration.
3.00 (0.76)* 3.00 (1.48)* 3 3
6. I’ve been very concentrated
during the activity.
3.75 (0.89)* 4.17 (1.03)* 3 3
7. I’ve had to work pretty hard to
get the activity done.
3.13 (1.36)* 2.17 (1.27)* 4 1
8. I have found difficult to per-
form the rehabilitation exercise
using this system.
1.25 (0.53)* 1.50 (0.45)* 2 1
Utility
9. I’d rather use this system at
home than have to go to a rehab
centre.
4.13 (1.13)* 4.00 (1.54)* 5 5
10. This system would make me
more consistent in performing the
exercises at home.
4.75 (0.46)* 4.25 (1.06)* 5 5
11. I believe that using this sys-
tem to do rehabilitation exercises
can be motivating.
5.00 (0.00)* 4.67 (0.49)* 5 5
12. I like the application has the
format of a game.
4.50 (1.41)* 5.00 (0.00)* 5 5
Interface Elements
13. The design of the avatar is ap-
propriate.
4.88 (0.35)* 4.42 (1.24)* 5 5
14. The information about the
repetitions is useful.
4.50 (1.41)* 4.58 (1.00)* 5 5
15. I like to get score every time I
perform a good exercise.
5.00 (0.00)* 4.58 (0.79)* 5 5
16. The route composed of
spheres helps to perform the ex-
ercises.
4.88 (0.35)* 4.58 (1.16)* 5 5
17. The gym has immersed me in
a rehabilitation environment.
4.88 (0.35)* 4.75 (0.45)* 5 5
TAM
18. This system is easy to use. 4.88 (0.35)* 4.92 (0.29)* 5 5
19. Using this system could help
me in performing the rehabilita-
tion exercises.
5.00 (0.00)* 4.83 (0.39)* 5 5
20. If I could borrow this system,
I would use it at home.
5.00 (0.00)* 5.00 (0.00)* 5 5
21. I’d recommend my friends to
use this system to do the exercises
at home.
5.00 (0.00)* 4.83 (0.39)* 5 5
Personalising Exergames for the Physical Rehabilitation of Children Affected by Spine Pain
539
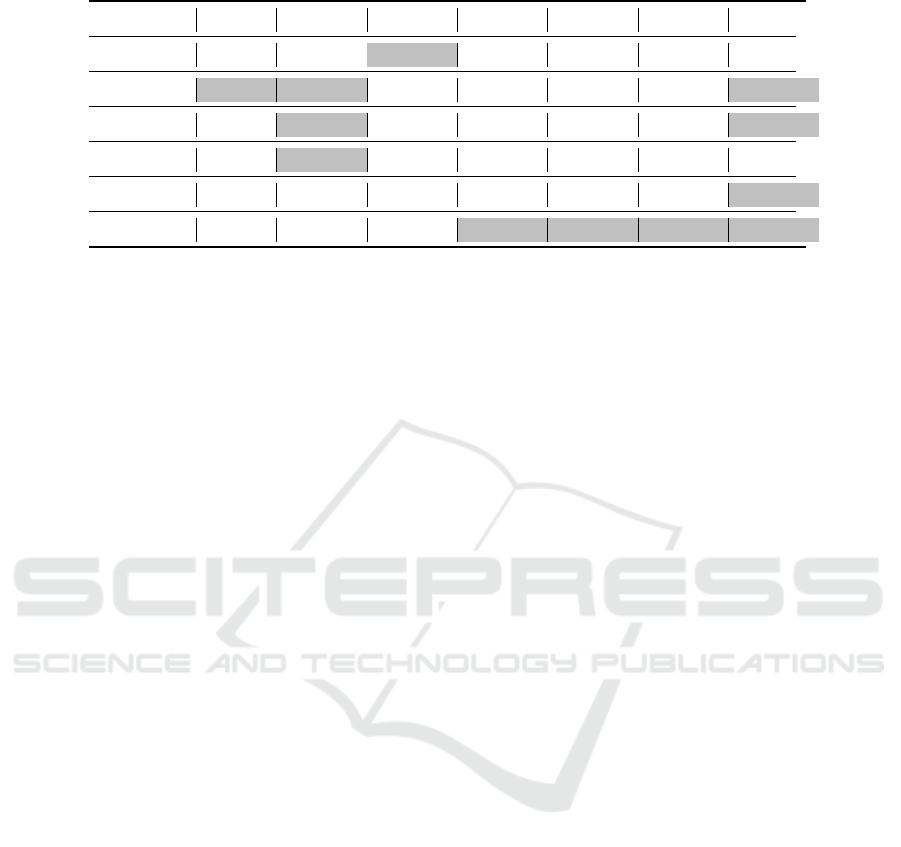
Table 2: Significant correlations among items (*:p<0.05; **:p<0.01).
Item 5 Item 10 Item 11
Item 14 Item 15
Item 16 Item 17
Item 1
.457*
Item 2
.468* .509* .498*
Item 6
.584** .427*
Item 9
.520*
Item 10
.634**
Item 11
.442* .824** .498* .688**
We also have studied the existence of correlations
among items using the Kendall tau-b correlation co-
efficient, a non-parametric measure association as the
variables do not follow a normal distribution. We
have obtained some interesting findings, shown in Ta-
ble 2. The positive correlations between item 1 and
item 11 reflect that fun and motivation are closely re-
lated factors. The correlation between item 2 and item
5 shows that the greater the interest in the activity,
the greater the concentration of girls on their perfor-
mance. Correlations between item 10 and items 2,
6 and 9 indicate that the idea of having this system
at home makes them be more motivated to carry out
rehabilitation activities. On the other hand, the posi-
tive correlations among item 11 and items 14, 15, 16
and 17, indicate that interface elements contribute to
motivate the girls to do their rehabilitation exercises.
The absence of correlation with the item related to the
avatar (item 13) can give us some extra information in
the sense that its appearance should be adapted to the
user. Finally, the positive correlations among item 17
and items 2, 6, 10 and 11 seem to indicate that the in-
terface contributes to capture the user’s interest. All
of these correlations can be observed graphically in
Figure 4, grouped into three categories: activity per-
ception, usefulness, interface.
4.4 Limitations
This pilot experience presents several threats to inter-
nal and external validity (Shadish et al., 2002) that
might have influenced our results.
• Construct Validity. Some items (5, 7, and 8) were
presented in a negative way respecting the others,
what has led to a confusion in the answers. This
should be taken into account in future experiments
to avoid erroneous answers.
• Statistical Conclusion Validity. Given the limited
power of the sample because of its size and its
domain, our data exploration has consisted in a
statistical description and a basic correlation anal-
ysis among items. A deeper study should be per-
formed in future experiments in order to contrast
answers provided by different groups of partici-
pants.
• Internal Validity. Although quasi-experiments
avoid most of the threats to internal validity that
arise in other kind of experiments (B
¨
arnighausen
et al., 2017), one limitation is related to the in-
terpretation of the results, since it is necessary to
consider the possibility that they can be influenced
by other factors not taken into account (Cook and
Campbell, 1986). For example, the 5 value has
been the most frequent one assigned in the ques-
tionnaire, which seems to indicate that girls, espe-
cially the youngest, were not very clear about the
difference between the range of values. Further-
more, since rhythmic gymnastics is a sport that
demands a high level of perfection, girls may be
influenced, unconsciously, by this level and have
thought that the only value which reflects a posi-
tive evaluation was the highest. This factor should
be taken into account in subsequent research ex-
periments.
• External Validity. The sample is not representa-
tive for the general population. Besides, data col-
lected in a gymnastics class may not be general-
ized to other educational scenarios as they are in-
evitably subjected to bias and non-bias systematic
experimental measurement errors. Moreover, al-
though we have considered a generic research hy-
pothesis, its empirical approach has forced us to
focus on a concrete context and with a specific
tool. Therefore, the replication of this study in
other contexts and with other users remains open
as an important future working line.
ICEIS 2020 - 22nd International Conference on Enterprise Information Systems
540
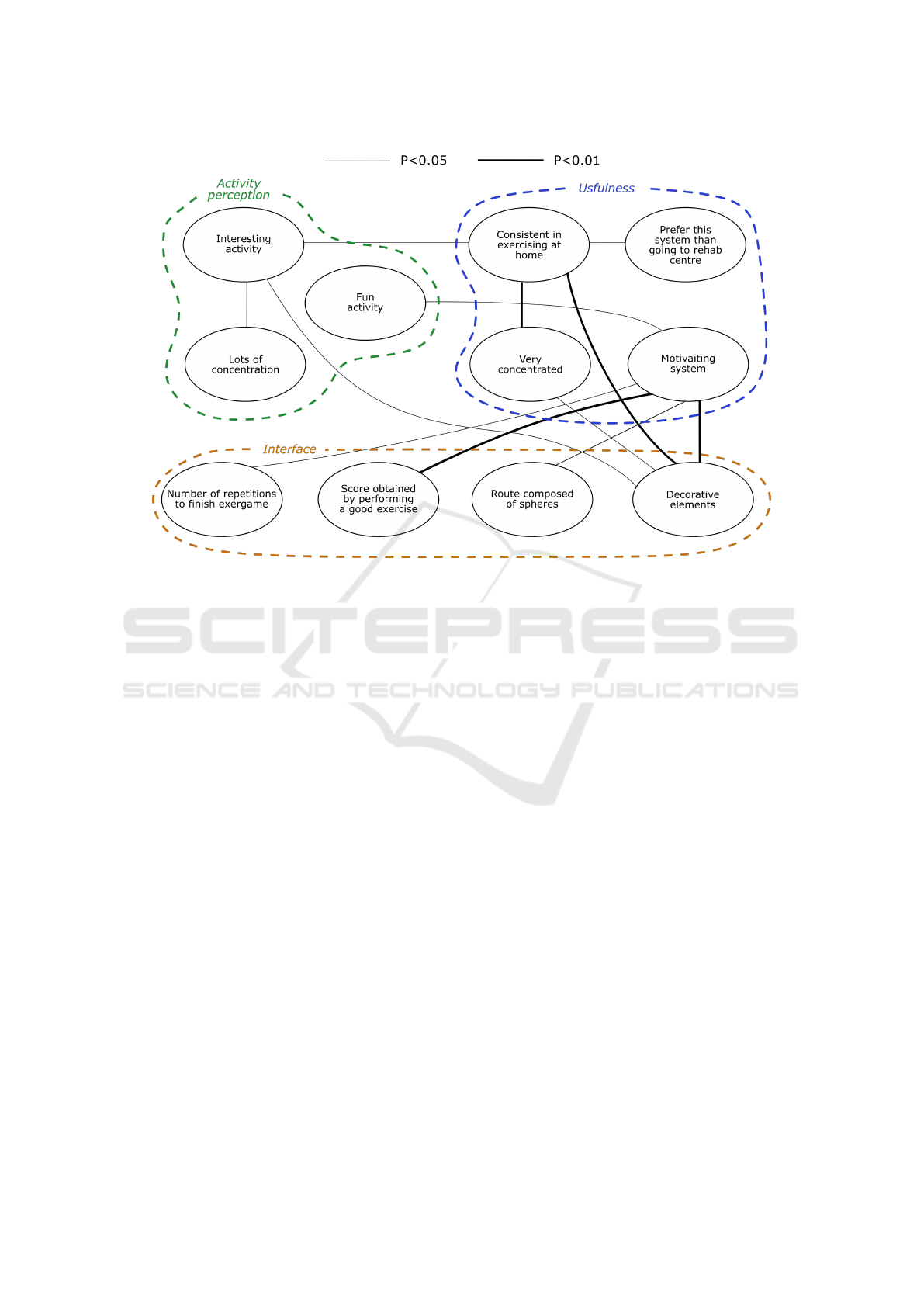
Figure 4: Correlation between variables grouped into activity perception, usefulness and interface.
5 CONCLUSIONS
In this article a system is designed to rehabilitate chil-
dren and teenagers suffering from lower back pain.
The rehabilitation tasks are customized by a high level
language called PEL, based on JSON standard, that
extends in the glTF specification. The objective of
the language in this research is aimed at rehabilitat-
ing patients with bone-marrow injuries, although the
nature of the language makes it possible be extrapo-
lated to other rehabilitation contexts. The exergames
are first designed by therapists, who define the ther-
apeutic objective, the trajectory of the rehabilitation
movement and the metrics to measure the patient’s
progress, all based on his or her conditions. Then, de-
velopers translate this information into PEL sentences
for automatically generating the exergames by means
of parsing process.
This article also includes a preliminary experi-
ment with potential patients to evaluate the system in
terms of understanding and suitability. To do this, an
exergame was developed to motivate the potential pa-
tients to perform exercises aimed at the physical reha-
bilitation of the lumbar spine. From a general point
of view, most participants perceived the tool as an ex-
cellent starting point to facilitate the process of patient
rehabilitation, considering it fun, interesting, and easy
to use.
As future lines of research, we can stress the need
to work on two core topics: (1) developing a system
or module that is capable of informing the therapist,
by way of notifications, on how children or teenagers
are progressing, and (2) constructing a visual tool to
help therapists graphically set the parameters, which
define the dynamics of an exergame, translating the
visual definition into PEL sentences.
ACKNOWLEDGEMENTS
This research was partially funded by Instituto
de Salud Carlos III, grant number DTS18/00122,
co-funded by the European Regional Development
Fund/European Social Fund “Investing in your fu-
ture”, by the Department of Technologies and Infor-
mation Systems (grant number 00421372), and by
the University of Castilla-La Mancha (AIR Research
Group, grant number 01110G9180).
REFERENCES
B
¨
arnighausen, T., Tugwell, P., Røttingen, J.-A., Shemilt,
I., Rockers, P., Geldsetzer, P., Lavis, J., Grimshaw,
J., Daniels, K., Brown, A., et al. (2017). Quasi-
Personalising Exergames for the Physical Rehabilitation of Children Affected by Spine Pain
541

experimental study designs series—paper 4: uses and
value. Journal of clinical epidemiology, 89:21–29.
Clark, R. A., Pua, Y.-H., Fortin, K., Ritchie, C., Webster,
K. E., Denehy, L., and Bryant, A. L. (2012). Valid-
ity of the microsoft kinect for assessment of postural
control. Gait & posture, 36(3):372–377.
Cook, T. D. and Campbell, D. T. (1986). The causal as-
sumptions of quasi-experimental practice: The origins
of quasi-experimental practice. Synthese, pages 141–
180.
Da Gama, A., Fallavollita, P., Teichrieb, V., and Navab, N.
(2015). Motor rehabilitation using kinect: a system-
atic review. Games for health journal, 4(2):123–135.
Davis, F. D. (1993). User acceptance of information tech-
nology: system characteristics, user perceptions and
behavioral impacts. International journal of man-
machine studies, 38(3):475–487.
Deterding, S., Khaled, R., Nacke, L. E., and Dixon, D.
(2011). Gamification: Toward a definition. In CHI
2011 gamification workshop proceedings, volume 12.
Vancouver BC, Canada.
Deutsch, J. E., Robbins, D., Morrison, J., and Bowlby, P. G.
(2009). Wii-based compared to standard of care bal-
ance and mobility rehabilitation for two individuals
post-stroke. In 2009 virtual rehabilitation interna-
tional conference, pages 117–120. Ieee.
Duthey, B. (2013). Background paper 6.24 low back pain.
Priority medicines for Europe and the world. Global
Burden of Disease (2010),(March), pages 1–29.
Esculier, J.-F., Vaudrin, J., Beriault, P., Gagnon, K., and
Tremblay, L. E. (2012). Home-based balance train-
ing programme using wii fit with balance board for
parkinson’s disease: a pilot study. Journal of Rehabil-
itation Medicine, 44(2):144–150.
Fernandez-Cervantes, V., Neubauer, N., Hunter, B., Strou-
lia, E., and Liu, L. (2018). Virtualgym: A kinect-
based system for seniors exercising at home. Enter-
tainment Computing, 27:60–72.
Gonz
´
alez, C. S., Toledo, P., Padr
´
on, M., Santos, E., and
Cairos, M. (2013). Tango: H: creating active educa-
tional games for hospitalized children. In Manage-
ment Intelligent Systems, pages 135–142. Springer.
Gonz
´
alez, C. S. G., del R
´
ıo, N. G., and Adelantado, V. N.
(2018). Exploring the benefits of using gamification
and videogames for physical exercise: a review of
state of art. IJIMAI, 5(2):46–52.
Hardy, S., Dutz, T., Wiemeyer, J., G
¨
obel, S., and Steinmetz,
R. (2015). Framework for personalized and adaptive
game-based training programs in health sport. Multi-
media Tools and Applications, 74(14):5289–5311.
Hoy, D., Brooks, P., Blyth, F., and Buchbinder, R. (2010).
The epidemiology of low back pain. Best practice &
research Clinical rheumatology, 24(6):769–781.
Jones, M., Stratton, G., Reilly, T., and Unnithan, V. (2004).
A school-based survey of recurrent non-specific low-
back pain prevalence and consequences in children.
Health education research, 19(3):284–289.
Katajapuu, N., Luimula, M., Theng, Y. L., Pham, T. P.,
Li, J., Pyae, A., and Sato, K. (2017). Benefits of
exergame exercise on physical functioning of elderly
people. In 2017 8th IEEE International Conference on
Cognitive Infocommunications (CogInfoCom), pages
000085–000090. IEEE.
Lai, C.-L., Huang, Y.-L., Liao, T.-K., Tseng, C.-M., Chen,
Y.-F., and Erdenetsogt, D. (2015). A microsoft kinect-
based virtual rehabilitation system to train balance
ability for stroke patients. In 2015 International Con-
ference on Cyberworlds (CW), pages 54–60. IEEE.
Matallaoui, A., Koivisto, J., Hamari, J., and Zarnekow, R.
(2017). How effective is “exergamification”? a sys-
tematic review on the effectiveness of gamification
features in exergames. In Proceedings of the 50th
Hawaii International Conference on System Sciences.
McCallum, S. (2012). Gamification and serious games for
personalized health. In pHealth, pages 85–96. IOS
Press.
McCambridge, J., Witton, J., and Elbourne, D. R. (2014).
Systematic review of the hawthorne effect: new con-
cepts are needed to study research participation ef-
fects. Journal of clinical epidemiology, 67(3):267–
277.
Mobini, A., Behzadipour, S., and Saadat Foumani, M.
(2014). Accuracy of kinect’s skeleton tracking for up-
per body rehabilitation applications. Disability and
Rehabilitation: Assistive Technology, 9(4):344–352.
Mousavi Hondori, H. and Khademi, M. (2014). A review
on technical and clinical impact of microsoft kinect on
physical therapy and rehabilitation. Journal of medi-
cal engineering, 2014.
Murray, C. J., Vos, T., Lozano, R., Naghavi, M., Flax-
man, A. D., Michaud, C., Ezzati, M., Shibuya, K.,
Salomon, J. A., Abdalla, S., et al. (2012). Disability-
adjusted life years (dalys) for 291 diseases and injuries
in 21 regions, 1990–2010: a systematic analysis for
the global burden of disease study 2010. The lancet,
380(9859):2197–2223.
O’Sullivan, S. B., Schmitz, T. J., and Fulk, G. (2019). Phys-
ical rehabilitation. FA Davis.
Palacios-Navarro, G., Garc
´
ıa-Magari
˜
no, I., and Ramos-
Lorente, P. (2015). A kinect-based system for lower
limb rehabilitation in parkinson’s disease patients: a
pilot study. Journal of medical systems, 39(9):103.
Pirovano, M., Surer, E., Mainetti, R., Lanzi, P. L., and
Borghese, N. A. (2016). Exergaming and rehabilita-
tion: A methodology for the design of effective and
safe therapeutic exergames. Entertainment Comput-
ing, 14:55–65.
Robinet, F., Arnaud, R., Parisi, T., and Cozzi, P. (2014).
gltf: Designing an open-standard runtime asset for-
mat. GPU Pro, 5:375–392.
Shadish, W. R., Cook, T. D., Campbell, D. T., et al. (2002).
Experimental and quasi-experimental designs for gen-
eralized causal inference/William R. Shedish, Thomas
D. Cook, Donald T. Campbell. Boston: Houghton
Mifflin,.
Shull, F., Singer, J., and Sjøberg, D. I. (2007). Guide to
advanced empirical software engineering. Springer.
Sparks, D., Coughlin, L., and Chase, D. (2011). Did too
much wii cause your patient’s injury? The Journal of
family PracTice, 60(7).
ICEIS 2020 - 22nd International Conference on Enterprise Information Systems
542

Sweller, J., Van Merrienboer, J. J., and Paas, F. G. (1998).
Cognitive architecture and instructional design. Edu-
cational psychology review, 10(3):251–296.
Webster, D. and Celik, O. (2014). Systematic review of
kinect applications in elderly care and stroke rehabil-
itation. Journal of neuroengineering and rehabilita-
tion, 11(1):108.
Wiemeyer, J., Deutsch, J., Malone, L. A., Rowland, J. L.,
Swartz, M. C., Xiong, J., and Zhang, F. F. (2015). Rec-
ommendations for the optimal design of exergame in-
terventions for persons with disabilities: Challenges,
best practices, and future research. Games for health
journal, 4(1):58–62.
Personalising Exergames for the Physical Rehabilitation of Children Affected by Spine Pain
543
