
Uptake of Pedometer-based Physical Activity: Success and Challenges
of a Church based Physical Activity Promotion Programme among
Overweight and Obese Adults in Kenya
Jane Wanjiku Kamau
1
, Peter Wanderi Mwangi
2
and Lucy-Joy Wachira
1
1
Department of Physical Education, Exercise and Sports Science, Kenyatta University, Nairobi, Kenya
2
Directorate of Corporate Services, Mount Kenya University, Thika, Kenya
Keywords: Uptake, Pedometer-based, Physical Activity, Overweight, Obesity, Church-based.
Abstract: Physical inactivity is among the modifiable risk factors to overweight and obesity. Targeting community units
in promoting active lifestyles is beneficial in offering social support. Technological devices such as
pedometers can promote physical activity at individual level by providing feedback. This paper presents the
success and challenges in implementing an on-going longitudinal pedometer- based PA programme in a
selected church in Kenya. Baseline results of 100 participants indicated that 20% were overweight and 26%
were obese with BMI scores being higher in those aged 30 years and above. There was significant correlation
between BMI and WHR (r=0.67 for females, r=0.88 in males). Physical inactivity among 46 participants in
the PA programme was at 52.4%. Most of them work in offices (81%) and use private (71.4%) or public
(19%) motorized transport. Majority of them (75%) do not use pedometers to track PA and do not follow
guidelines of the programme. Cost, time and competing priorities were cited to hinder participation. The 25%
of pedometer users acknowledge their importance and influence to their participation in PA. This paper
recommends that the church device strategies to navigate the challenges of physical inactivity while tapping
into the resources available within the church settings.
1 INTRODUCTION
Obesity has over the years become a global pandemic
with 650 million adults aged 18 years and above and
41 million children being obese in the year
2016(World Health Organization [WHO], 2020).
Although there is no conclusive and current
population-wide data on prevalence of obesity in
Kenya, the Stepwise Survey for Non-Communicable
Diseases (NCDs) Risk Factors (2015) showed that
28% of Kenyans aged 18-69 years are either
overweight or obese with women recording a higher
percentage (38.5%) than men (17.5%), while 4.1% of
children under the age of five are either overweight or
obese (Ministry of Health [MOH], 2015a).
Obesity has been associated with cardiovascular
diseases, diabetes, musculoskeletal disorders and
some forms of cancer (WHO, 2018).
These NCDs have reached pandemic levels in
Kenya accounting for more than 50% of total hospital
admissions and over 55% of hospital deaths (MOH,
2015a).They are indeed a major public health concern
with significant social and economic implications in
terms of health care needs, lost productivity and
premature death thus presenting serious setback to the
attainment of desired social, health and economic
targets outlined in the United Nations (UN) 2015
Sustainable Development goals Number 3, Kenya’s
Vision 2030 and the Kenyan Government 2017 Big
Four Agenda.
Energy imbalance between calories consumed
and calories expended are the fundamental causes of
obesity and overweight (WHO, 2020).
One proven way of increasing energy expenditure
is participation in regular physical activity (PA) that
leads to accumulation of at least 150 minutes of
moderate-intensity aerobic physical activity
throughout the week for adults and
60minutesperdayforchildren (MOH, 2017). Physical
activity is recommended to reduce excess body
weight, prevent body weight regain and decrease
subsequent risks in developing metabolic and
orthopedic conditions (Natel, Mathieu & Prince,
2011).
126
Kamau, J., Mwangi, P. and Wachira, L.
Uptake of Pedometer-based Physical Activity: Success and Challenges of a Church based Physical Activity Promotion Programme among Overweight and Obese Adults in Kenya.
DOI: 10.5220/0010026001260132
In Proceedings of the 8th International Conference on Sport Sciences Research and Technology Support (icSPORTS 2020), pages 126-132
ISBN: 978-989-758-481-7
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

Despite the health benefits of PA, there is reduced
participation world over with a resultant increase in
overweight and obesity. In Kenya, the rate of PA is
estimatedtobeonly10%inmalesand14% in females
(WHO 2014) with uneven distribution among rural
and urban populations where levels of physical
activity among rural populations are higher (Muthuri,
et al, 2014).
Some of the barriers to PA in Kenya include rapid
urbanization; wherein access to fields needed to play
such games as soccer are not available due to dense
populations and their subsequent demand for land,
poor built environment, lack of safe environment in
which to walk or cycle to work or to school or for
physical play at home, inadequate information by the
public on PA, increased use of motorized transport
and social cultural factors (WHO, 2018).A
combination of all these factors has lead Kenya to get
into the fourth pattern of the nutritional and physical
activity transition characterized by nutrition and
physical inactivity related obesity and NCDs as
identified by Popkin in2015.
1.1 Problem Statement
Although there is a lot of good information
concerning prevention and management of obesity
and associated NCDs in Kenya, including
development of important documents outlining the
strategies to be adopted at individual, community and
society level, there seems not to be a commensurate
change in occurrence of the pandemic.
If anything, the rise is on a positive incline. For
instance, Strategic objective number three (3) in the
Kenya National strategy for prevention and control of
non- communicable diseases (2015-2020) is aimed at
promoting healthy lifestyles and implementing
interventions to reduce the modifiable risk factors for
NCDs (MOH, 2015b).
There seem to be a general lack of action on the
available information with an estimated PA of only
10% in males and 14% in females (WHO 2014)
which is unevenly distributed among rural and urban
populations. Children are also showing transition
towards sedentary behavior especially those in urban
settings with only 12.6% of school children in Nairobi
City meeting the recommended levels of daily
physical activity (Muthuri et al, 2014). Onywera et al
(2012) adds that about 50% of children in urban areas
spend over 2 hours per week viewing television
compared to<10% of rural children.
With this kind of lifestyle, there is compromised
health, high cost to manage disease, loss of
productivity due to absence from work and the lack
of capacity to work as the health conditions
deteriorate. The immediate effects are felt at family
level as domestic expenditure on health increases, at
institutional level as institutions commit big parts of
their budget for health management of their
employees, and at the community level as people
come together in aid of health care expenses of the
affected individuals. This consequently thwarts
economic development of the nation.
Voluntary exercise is the most important
component of total daily energy expenditure by
individuals. This can be achieved at community level
by provision of supportive environments within the
communities where they come from. This will
collectively challenge individuals to follow
recommendations for physical activity that promotes
and or maintain health.
Such a model is outlined in the midstream
approach suggested in the Kenya National Strategy
for prevention and control of NCDs (2015-2020)
which has interventions targeting groups of people,
institutions and communities.
Churches play an important role in communities
especially in Africa; serving as primary
organizational units and sources of social support and
leadership. As such, they are potentially effective
settings for implementing community health
intervention programmes. In Kenya, the most
predominant religion is Christianity with an
adherence of 84.8% of the total population (World
Factbook, 2020). Thus, targeting churches as the
platform for the community-based lifestyle
interventions ensures that majority of the population
in terms of age group, gender and social economic
class are included.
In addition to community-based approaches,
technology has been used to promote PA and change
exercise behavior (Heyward & Gibson, 2018). For
instance, electronic pedometers are increasingly
being used to measure PA among all populations
because of their ability to count and monitor steps
taken throughout the day during ambulatory activities
such as walking, jogging and running. A study by
Bravata (2007) indicated that participation in PA
increased by 27% over baseline levels among
pedometer users. According to Masi, Peterman and
Kaminsky (2019), when adults accumulate 10,000
steps per day, this translates to an equivalent of
walking roughly 8.045kilometers. These researchers
recommend 10,000 to 12,500 steps per day for health
and wellbeing.
This paper aims at highlighting the success and
challenges of a community (church) based
programme designed to promote PA among church
Uptake of Pedometer-based Physical Activity: Success and Challenges of a Church based Physical Activity Promotion Programme among
Overweight and Obese Adults in Kenya
127

congregants using pedometers as the motivator that
provides feedback necessary to help individuals track
their levels of physical activity by tracking their step
counts, sending reminders and real time alerts
concerning their activity levels.
The paper highlights the overweight and obesity
status of the congregants, the PA levels of the
congregants as well as the success and challenges
recorded during the implementation of the programme.
2 METHODOLOGY
2.1 Study Design
This paper is developed from an on-going programme
that is longitudinal in overall design with an end point
focusing on behavior change of the congregants from
sedentary to active living. The programme is being
carried out in two phases comprising of a baseline
survey phase and intervention phase.
The baseline survey phase adopted a cross-
sectional analytical design to conduct a Health Risk
Appraisal (HRA) on overweight and obesity among
the church members. Participation in PA was
determined among other modifiable risk factors
associated with overweight and obesity. This was
followed by physical measurement of height, weight,
waist circumference and waist to hip ratio for risk to
CVD determination.
The intervention phase involved among other
interventions use of pedometers to track daily PA
levels of the participants.
2.2 Target Population
The baseline survey targeted all members of the
selected church while the intervention phase targeted
the overweight and obese adults identified during the
health risk appraisal. Parents and guardians as well as
the youth were to act as champions of wellbeing at
family level serving as models to their children and
siblings.
2.2.1 Inclusion and Exclusion Criteria
The programme included all congregants who
consented. The programme excluded pregnant
women because of the natural weight gain that
accompanies pregnancy thus affecting the body mass
index as well as the change in body morphology that
may not allow objective assessment of waist
circumference and determination of waist to hip ratio
(WHR).
2.3 Sampling and Sample Size
Census sampling was used to include all the
congregants (100) who took part in the first phase of
the baseline study. Purposive sampling was used to
target all the (46) youth and adult congregants within
the overweight and obese category following the
results of the baseline health risk appraisal.
Convenience sampling was used to enroll willing and
motivated congregants into the health promotion
programme.
2.4 Data Collection Instruments
The baseline data on PA was obtained using a
questionnaire where respondents self-reported on PA
among other modifiable risk factors to obesity and
NCDs. Physical activity related questions assessed
the nature of occupation/work (either office or
manual work), the means of transport to work
(walking, motorized transport; either private or
public) and involvement in other forms of physical
activity apart from work (either at the gymnasium,
jogging or other sports).
Anthropometric measurements of body weight,
height and waist circumference were taken using
portable digital Seca Robusta 813 weighing scales
(Hamburg Germany), Seca 214 portable stadiometer
(Hamburg, Germany) and anthropometric tapes
respectively. Overweight and obesity was determined
using BMI.
Classification for risk category was followed by
measuring waist and hip circumferences using
anthropometric tapes. These measurements were then
used to determine the WHR.
Given the different financial abilities of the
participants, they were advised to purchase
pedometers of their choice, so long as they would take
step counts and provide distance covered per day in
kilometers. The pedometers were also required to be
able to give alerts on sedentarism when participants
were seated for too long without walking. The
pedometers were also supposed to have the ability to
synchronize with mobile phone applications that
would allow data interpretation and sharing on the
WhatsApp platform.
2.5 Study Procedure
Permission was sought from the church leadership to
conduct a church-wide one day health risk appraisal
camp for the congregants at the church premises in
August, 2019. During this camp, the participants were
presented with a talk on obesity and its associated risk
icSPORTS 2020 - 8th International Conference on Sport Sciences Research and Technology Support
128
factors and NCDs. The camp was a diagnostic and not
curative forum with the aim of collecting baseline
information that would inform development of the
pedometer-based PA promotion programme. General
feedback on the health risk appraisal was presented
on another day to the church after analysis. It is during
this feedback meeting that congregants were recruited
to the PA promotion programme. During the launch
of the programme, participants signed the informed
consent for the intervention and guided on the basic
specifications of the pedometers and how to acquire
them. The participants were allowed to purchase
pedometers of their choice so long as they could take
step counts, distance in kilometers, give real time
alerts on sedentarism and could be synchronized with
mobile phone applications to allow data sharing and
report their engagement in PA on a daily basis. A
WhatsApp account was created and all the consenting
participants registered.
The participants were to engage in self- directed
PA throughout the week from their homes or work,
and were to take screenshots of their workouts as
recorded by their pedometers and post them on the
WhatsApp forum. They were encouraged to share
their experiences in the forum. They were also
provided with an opportunity to ask questions or
discuss topics related to PA and obesity in the forum.
Once every week on Saturday morning from 7.00am,
they were taken through a one hour aerobic dance
session by a qualified fitness instructor. This allowed
for a face to face interaction with one another.
2.6 Data Analysis
Anthropometric data was analyzed in Microsoft excel
programme. Frequencies were used to summarize the
raw data. Pearson product moment correlation
coefficient was used to relate BMI scores with the
WHR scores. Self-report data on participation in PA
was analyzed using Google forms to accord the study
real time responses from the participants. Data on
uptake of pedometer-based PA at community level
(church) were analyzed under two main themes
namely; success and challenges. The results are
presented in tables, charts and bar-graphs.
2.7 Logistical and Ethical
Considerations
Permission to recruit the congregants was sought
from the Vicar In-charge of the selected church.
Members were provided with information concerning
the program and given opportunity to give written
informed consent. For sustainability, it is hoped that,
promotion of self-directed active lifestyle will ensure
that congregants are in control of their weight and
health in general. The church will play the role of
social support structure offering the desired social
environment for continued engagement of its
members on healthy active practices beyond the
programme. The documented success of the
intervention will act as evidence for scaling up to
other community settings countrywide.
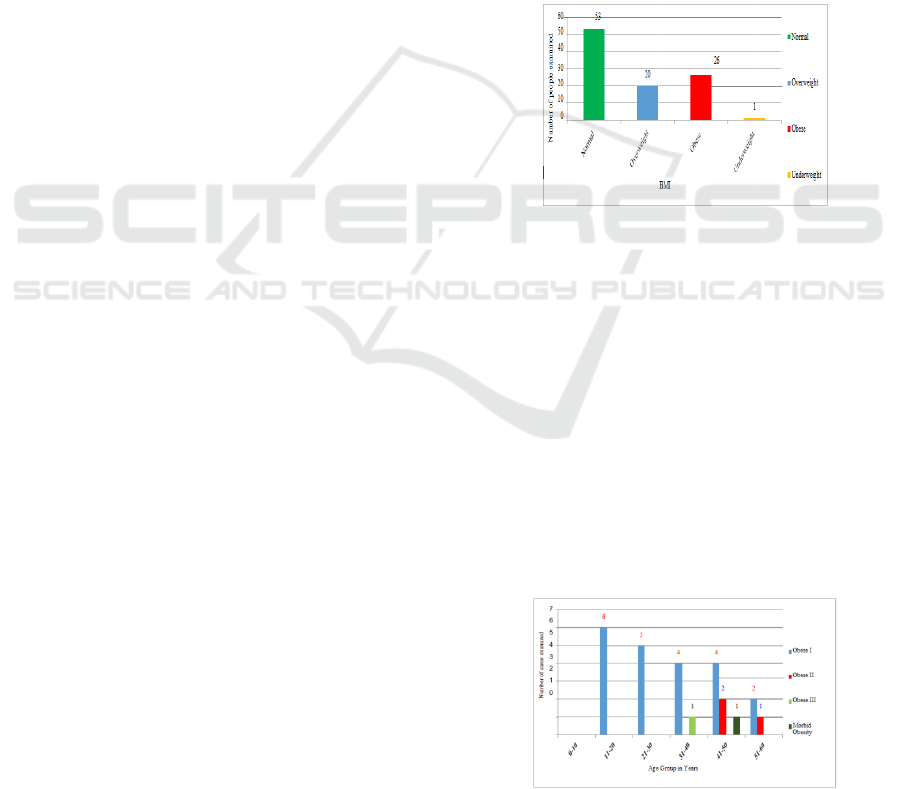
3 RESULTS
Figure 1 indicates that a total of 100 congregants were
assessed of their weight status, out of which 20 were
overweight with a BMI=25˂30 while 26 were obese
with their BMI ≥30.00.
Figure 1: Overweight and Obesity Status of the
congregants.
BMI scores for the participants in the obese
category were distributed against age and the results
presented in figure2.
The results in figure 2 indicate that out of the 26
obese participants, 6 participants (11-20years), 5
participants (21-30 years), 4 participants (31-40
years) and 2 participants (51-60 years) were in the
class 1 of obesity (BMI=30˂35). Two participants (41-
50years) and 1 participant (51-60 years) were in class
II of obesity (BMI=35˂40. One participant (31-40
years) was in category III of obesity (BMI=40) while
1 participant (41-50years) was in the category for
morbid obesity (BMI˃40.
Figure 2: Overweight and Obesity Status by Age and
Gender.
Uptake of Pedometer-based Physical Activity: Success and Challenges of a Church based Physical Activity Promotion Programme among
Overweight and Obese Adults in Kenya
129
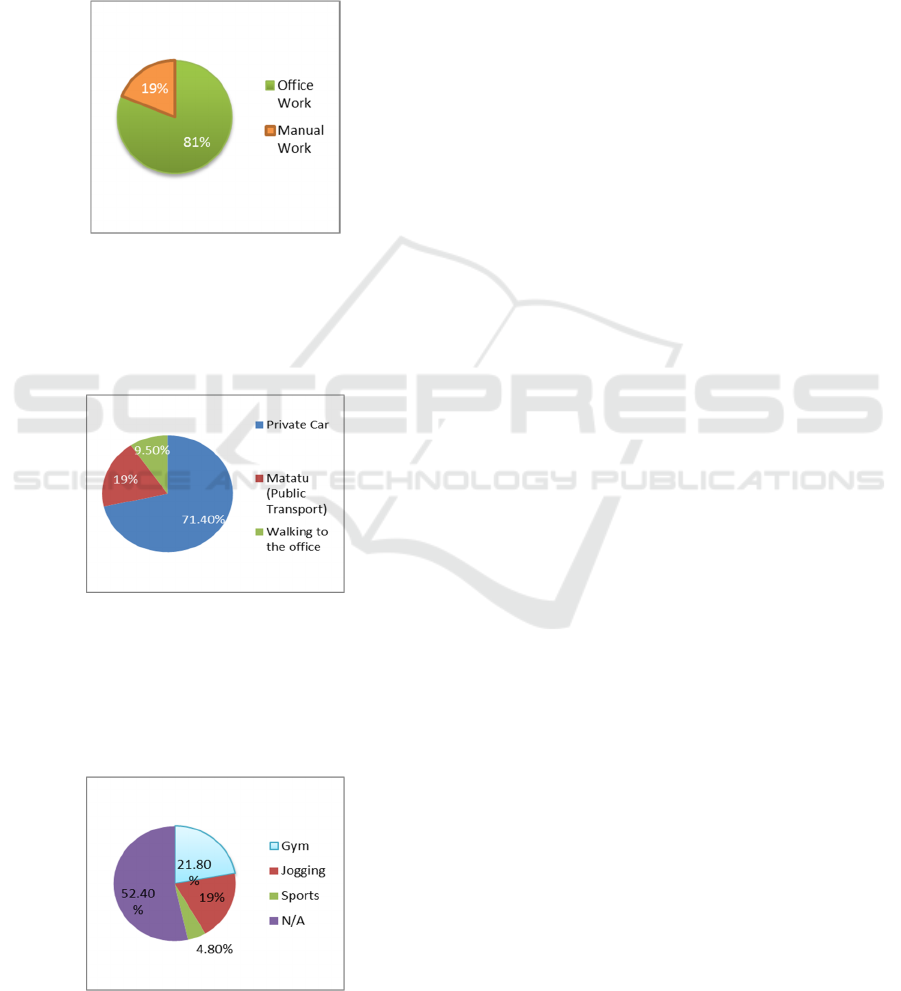
3.1 Self-report on PA
Out of the 46 congregants who consented to take part
in the health promotion programme, 21 completed the
self-report questionnaire on participation in PA and
their results are presented in figures 3, 4 and 5. Figure
3 indicates that out of the 21 respondents, 19% are
involved in manual work while 81% work in the
offices.
Figure 3: Type of Work/Occupation.
Figure 4 indicates that out of the 81% respondents
who work in the office, 9.5% walk to the office, 19%
use public means while 71.4% use private vehicles to
travel to work.
Figure 4: Means of travel to work.
Figure 5 shows that other than work 19% engage
in jogging activity, 21.8% are engaged in activities at
the gymnasium, 4.8% are engaged in other sports
while 52.4% are not involved in any other physical
activity.
Figure 5: Activities other than work.
To determine the risk status of the recruited
congregants to disease, waist to hip ratios were
measured against their BMI by gender.
Out of the 16 female participants, 9 were under
the high-risk category, 3 were in the low risk while 4
were in the very low risk. On the other hand, out of
the 6 male participants, 2 were in the high-risk
category, 2 in the low while 2 were in the very low
risk category.
In addition, a relationship between BMI and waist
to hip ratio was determined using the Pearson product
moment correlation coefficient for each gender. The
analysis indicated a significant relationship between
BMI scores and WHR scores for females(r=0.67) and
males (r=0.88).
3.2 Uptake of Pedometer-based PA at
the Church
Although all the participants were sufficiently
sensitized on the role of wearable technology devices
such as pedometers and their importance in
monitoring an individual’s PA level and volume, it
was solely based on voluntary acquisition and self-
motivated daily use of the gadget. This was important
for a sustainable self-driven approach that can be
carried forward even after the intervention period
lapses. However, this study shows a poor uptake of
the recommended pedometer based PA monitoring
approach with 75% opting not to acquire or use the
device. They cited conflicting demands of resources
(money and time) while directing their focus on other
non-health and wellness needs.
There was however a positive adoption by a
quarter (25%) of the sample who found pedometers
valuable and a positive influence in PA participation.
This included 2 males and 2 female participants aged
between 25 and 35 years. It is interesting to note that
all the 25% of the pedometer users were in the
overweight category and all were in the very low risk
to development of CVDs as categorized by their waist
to hip ratios. One would expect to see the obese
individuals being enthusiastic about taking PA as a
weight remedy and using pedometers for motivation,
however is was not the case so far in this study.
Additionally, all the pedometer users were among the
youth category aged 25 to 35 years who may find
technology use easy and friendly in offering
solutions. Probably the older congregants, besides the
financial challenge, found the use of pedometers to be
technically challenging.
icSPORTS 2020 - 8th International Conference on Sport Sciences Research and Technology Support
130

3.2.1 Success
The following successes emanated from an interview
conducted among the 21 participants of the
pedometer-based PA promotion programme. They
opined that:
i. The programme has been useful in creating
awareness about overweight and obesity
status of the congregants
ii. It has been useful in helping the congregants
understand the role of exercise among other
interventions in management of overweight
and obesity
iii. It has brought people together to work
towards a common goal of leading healthy
active lives.
3.2.2 Challenges
The participants cited the following as challenges that
are possibly slowing down the program.
i. There is lack of capacity at institutional level
to support frequent mass activities.
ii. The uptake of the PA has not been felt at the
health club level.
iii. Conflicting demand for resources (time and
money) whereby investing in pedometers,
PA support equipment and facilities are
considered as opportunity cost over other
priorities.
4 DISCUSSION
4.1 Overweight and Obesity Status of
the Congregants
Twenty percent of the congregants are overweight
while 26% are obese indicating that the pandemic is
increasing in Kenyan communities. Although there
are cases of obesity among younger populations (6 in
11-20years) the serious cases of obesity (categories,
II, III and morbid obesity) are more prevalent in later
years especially 30- 60 years. This finding agrees with
that of Mkuu et al, (2018) who observed high
prevalence of overweight (20.5%) and obesity (9.1%)
among Kenyan women aged 35-44years.
4.2 Physical Activity Status
From the self-report on participation in PA, most
congregants are inactive with majority working in
offices (81%) where they probably sit all day long.
They also use motorized transport (90%) to and from
work with majority of them using private vehicles
(71%) offering them less or no opportunity to be
active. Worse still, majority of the congregants
(52.4%) do not engage in PA other than office work
further compromising their activity levels leaving no
avenue for energy expenditure.
This provides good ground for overweight and
obesity to develop and blossom. These results agree
with the observations by King and Jacobson (2017)
who in their review observed that though fast and
convenient, automobiles are replacing PA involved in
walking or cycling with sedentary activity of driving
thus increasing obesity by reducing energy
expenditure.
4.3 Uptake of Pedometer-based PA at
the Church
On use of objective monitoring of PA using wearable
devices such as pedometers proposed in this project,
it is noteworthy that although this represents a
valuable mode of monitoring volumes and
influencing participation, its uptake at community
level may be low and poor at the beginning due to
other competing priorities (costs and time). This may
be addressed through continuous sensitization,
encouragement and follow-up by peers until lasting
habits and appreciation of the initiatives are
established. The 25% of the participants who used
pedometers were mainly youth aged 25-35 years.
This pointed to the fact that younger generation may
embrace technology faster and better than the older
ones. The use of pedometers was equal among gender
on a ratio of 1:1 and therefore the use of pedometer
may not be influenced by gender. However, those that
used pedometers were the young and were all in the
overweight category with none from the obese
category. This indicates the need to continuously
target the older congregants in promoting the PA
programme while encouraging them to use the
pedometers for they are likely to sustain the
motivation for self-directed PA. Another area of
focus in this study would be to encourage the obese
congregants to engage in PA and offer personalized
support to them towards developing a self-directed
PA routine. The 25% who used pedometers referred
to them as useful and had significant influence on
their daily participation in PA. This finding is similar
to that of Baker et al., (2008) who observed
significant increases in step counts among the
intervention group as well as the time spent in leisure
walking and a reduction in sitting time among
pedometer users.
Uptake of Pedometer-based Physical Activity: Success and Challenges of a Church based Physical Activity Promotion Programme among
Overweight and Obese Adults in Kenya
131

5 CONCLUSIONS
The uptake of pedometer-based PA promotion
programme is slow at the community-church level even
though cases of overweight and obesity are
increasing. The few congregants that have embraced
pedometer use to monitor their PA levels are among
the youth age category and are mainly in the overweight
category. This leaves out a key population of the church;
the older where majority of obesity cases lie. There is a
noticeable percentage of physical inactivity among
the congregants a reason that can be associated with
the high levels of overweight and obesity. The
increase in overweight and obesity is likely to
predispose most of the congregants to developing one
or more of NCDs whose risk factors include among
others physical inactivity.
6 RECOMMENDATIONS
This paper recommends that the church by virtue of
being an organized and well- structured social unit in
the society should promote and device strategies to
help the congregants navigate the challenges of
physical inactivity while at the same time tapping into
the resources available to it including facilities and
health experts within its reach to address the rising
cases of obesity and related comorbidities in the
society. Among the proposed recommendations is
continued sensitization on use of pedometers by the
congregants and the importance of acquiring
pedometers for PA promotion. One of the main
limitations of this programme is lack of provision of
pedometers to the participants. May be if this was
achieved, there would be a higher level of uptake
which would enable the researcher to track the step
counts attained by the participants against the
recommended number of 10,000 steps per day. This
would help address issues of adherence and allow
further analysis of the uptake of pedometer-based PA
promotion on health outcomes especially on
overweight and obesity status of the congregants.
REFERENCES
Baker, G., Gray, S. R., Wright, A., Fitzsimons, C., Ninimo,
M., Lowry, R, Mutrie, N & Scottish Physical Activity
Research Collaboration [SPARColl] (2008). The Effect
of a Pedometer-based Community Walking
intervention “walking for wellbeing in the west” on
physical activity levels and health outcomes: a 12 week
randomized control trial. International Journal of
Behavioral Nutrition and Physical Activity. Vol 5 no.44
Bravata, D. M., Smith-Spangler, C., Sundaram, V.,
Gienger, A. L., Lin, N., Lewis, R., & Sirard, J. R.
(2007). Using pedometers to increase physical activity
and improve health: a systematic review. Jama,
298(19), 2296-2304.
Heyward, V. H. & Gibson A. L. (2020). Advanced Fitness
Assessment and Exercise Prescription: Technology can
Boost Physical Activity Promotion. Human Kinetics.
US. Humankinetics.com
King, D. M., & Jacobson, S. H. (2017). What is driving
obesity? A review on the connections between obesity
and motorized transportation. Current obesity reports,
6(1), 3-9.
Masi, E., Peterman, J. E. & Kaminsky, L. A. (2019). The
Health Benefits of a Pedometer- Based 100,000 Steps
per week Physical Activity Program. Journal of Science
in Sports and Exercise, Vol 1pg176-183
Ministry of Health (2018) National Physical Activity
Action Plan 2018-2023.World Health Organization
Ministry of Health (2017). National Guidelines for Healthy
Diets and Physical Activity. Government of Kenya.
Nairobi.
Ministry of Health (2015a). Kenya Stepwise Survey for
Non- Communicable Diseases Risk Factors 2015
Report. Division of NCDs, Afya House, Cathedral
Road, Nairobi, Kenya.
Ministry of Health (2015b) Kenya National Strategy for the
Prevention and Control of Non- Communicable
Diseases, 2015- 2020. International Institute of
Legislative Affairs.
Mkuu, R. S., Epnere, K., & Chowdhury, M. A. B. (2018).
Peer reviewed: prevalence and predictors of overweight
and obesity among Kenyan women. Preventing chronic
disease, 15.
Muthuri, S. K., Wachira, L. J. M., Leblanc, A. G., Francis,
C. E., Sampson, M., Onywera, V. O., & Tremblay, M.
S. (2014). Temporal trends and correlates of physical
activity, sedentary behaviour, and physical fitness
among school-aged children in Sub-Saharan Africa: a
systematic review. International Journal of
environmental research and public health, 11(3), 3327-
3359.
Onywera, V. O., Adamo, K. B., Sheel, A. W., Waudo, J. N.,
Boit, M. K., & Tremblay, M. S. (2012). Emerging
evidence of the physical activity transition in Kenya.
Journal of physical activity and health, 9(4), 554-562.
Popkin, B. M. (2015). Nutrition transition and the global
diabetes epidemic. Current diabetes reports, 15(9), 64.
World Health Organization (2020). Obesity and Overweight
Fact sheet. https://www.who.int/news-room/fact-sheets/
detail/obesity-and-overweight
World Factbook (2020) -Central Intelligence Agency:
Kenya People. https://Theodora.com
icSPORTS 2020 - 8th International Conference on Sport Sciences Research and Technology Support
132
