
Pediatric Psoriasis in Patient with Obesity
Elin Herlina
1*
, Eunice Gunawan
1
, Retno Indar Widayati
1
, Widyawati
1
, Indra Wijaya
1
1
Departement of Dermatovenereology,
5
Departement of Anatomic Pathology Faculty of MedicineDiponegoro University /
Dr. Karyadi General Hospital Semarang
*Corresponding author
Keywords: Childhood psoriasis, psoriasis vulgaris, pediatric psoriasis.
Abstract: Psoriasis is an immunologically mediated chronic inflammatory skin disease, characterized by well-defined
salmon-pink plaques bearing large adherent silvery centrally attached scales. The prevalence in children
aged 10-19 years is about 1.37%. Pediatric psoriasis has been associated with specific comorbidities, such
as obesity, hypertension, hyperlipidemia, diabetes mellitus, and rheumatoid arthritis, making early diagnosis
and management essential.A 12-year-old boywhose have body weight was 120 kilograms presented with
erythematous patches and plaques covered by thick silvery scales on his face, trunk, belly, elbows, lower
limbs, and knees. Patient felt itchy onthose lesions. The diagnosis was made based on clinical history,
clinical examination, and histopathology examination. Histopathological examination showed tissue
covered by keratinized stratified squamous epithelium, hyperkeratotic, parakeratotic, acanthosis, regular rete
ridges, the dermis consisted of skin adnexa and fibro collagenous stroma connective tissue with perivascular
lymphocytes. The patient was treated with Methotrexate 5mg per 12 hours given on the first and second day
of every week, folic acid 1 mg per day is given on the third to seventh day every week, 0.25%
desoximetasone cream and 10% urea cream twice daily. Information, education, communication, and
psychological support were provided to the patient and his parents.A good response was observed after two
months of treatment.
1 INTRODUCTION
Psoriasis is a chronic inflammatory
hyperproliferative disease of the skin, scalp, nails,
and joints. Psoriasis is an inherited papulosquamous
skin disorder with a variety of clinical presentations,
most of which eventuate into well-defined
erythematous lesions with typical silvery scales
(Bronkers et al, 2015). The prevalence of psoriasis
in childhood is about 0.55 % in children aged 0–9
years and 1.37 % in children aged 10–19 years
(Bronkers et al, 2015).
Psoriasis in children can have a significant
impact on the quality of life by interfering with self-
esteem, family and social relationship and school.
Children suffering from psoriasis also have a higher
prevalence of comorbidities, including obesity,
diabetes mellitus, hypertension, rheumatoid arthritis,
Crohn’s disease, and psychiatric disorder (Bronkers
et al, 2015)..
Psoriasis flares can be provoked by non-specific
triggers. A higher frequency of stress (associated
with the start of the school year, the birth of
brother/sister, etc.), mild trauma (Koebner
phenomenon), and infection (streptococcal, viral)
were reported. Systemic drugs (beta-blockers,
lithium, antimalarial, etc.) or HIV infection, are less
frequently implicated in children than in an adult
(Mahe, 2016).
Plaque psoriasis is the most common form of
pediatric psoriasis. The presentation in children
resembles psoriasis in adults. However, initial
lesions are less prominent, with mild scaling and
induration. In later stages, the clinical presentation is
dominated by scaly plaques accompanied by itching.
Psoriasis frequently affects elbows, knees, scalp,
umbilicus,and face (Mahe, 2016; Madiraca er al,
2016).
Treatment of psoriasis in the pediatric patient is
challenging because lack of clinical trial and
guidelines. There are currently no international
standardized guidelines for medical treatment of
pediatric psoriasis.Treatment options include topical
agents, systemic agents, biologic agents, and
phototherapy. Treatment success depended mainly
380
Herlina, E., Gunawan, E., Widayati, R., Widyawati, . and Wijaya, I.
Pediatric Psoriasis in Patient with Obesity.
DOI: 10.5220/0009989503800383
In Proceedings of the 2nd International Conference on Tropical Medicine and Infectious Disease (ICTROMI 2019), pages 380-383
ISBN: 978-989-758-469-5
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
on parental involvement and education.
Psychosocial support is another critical component
of therapy for children with psoriasis (Bronkers et al,
2015; Madiraca et al, 2016).
2 CASE
A 12-year-old boy, Javanese, Indonesian, cameto
Dermatovenereology Department Kariadi General
Hospital Semarang on23 August 2018 with itchy
erythematous plaquesand thick silvery scaling all
over his body for several years. The plaque first
appeared on the face, trunk, belly, elbows, and
knees.
The mother said since he was 5-year-old,
erythematous spots and scales had started to appear
on her son's body and get worse, the patient had
never been treated.
The patient is the second child, the father works
as a trader in the market, and the mother is
unemployed.Medical expenses are covered by the
Social Insurance Administration
Organization/Badan Penyelenggara Jaminan
Sosial(BPJS). The socioeconomic impression is
sufficient.
The patient whose body weight was 120
kilogramswith BMI 43belonged to the obese
category, and the health conditions, in general, were
perfect.Physical examination on the face, trunk,
belly, elbows, lower limbs and knees found several
lesions presented as well-defined erythematous
plaques that were partially covered by thick silvery
scales. Auspitz test was positive (+). Laboratory
examination found hemoglobin level of 15.7 g/dL,
SGOT 22 U/L, SGPT 60 U/L, Urea 22 mg/dL,
Creatinine 0.79 mg/dL, blood sugar 81 mg/dL,
which were all within the normal limit.
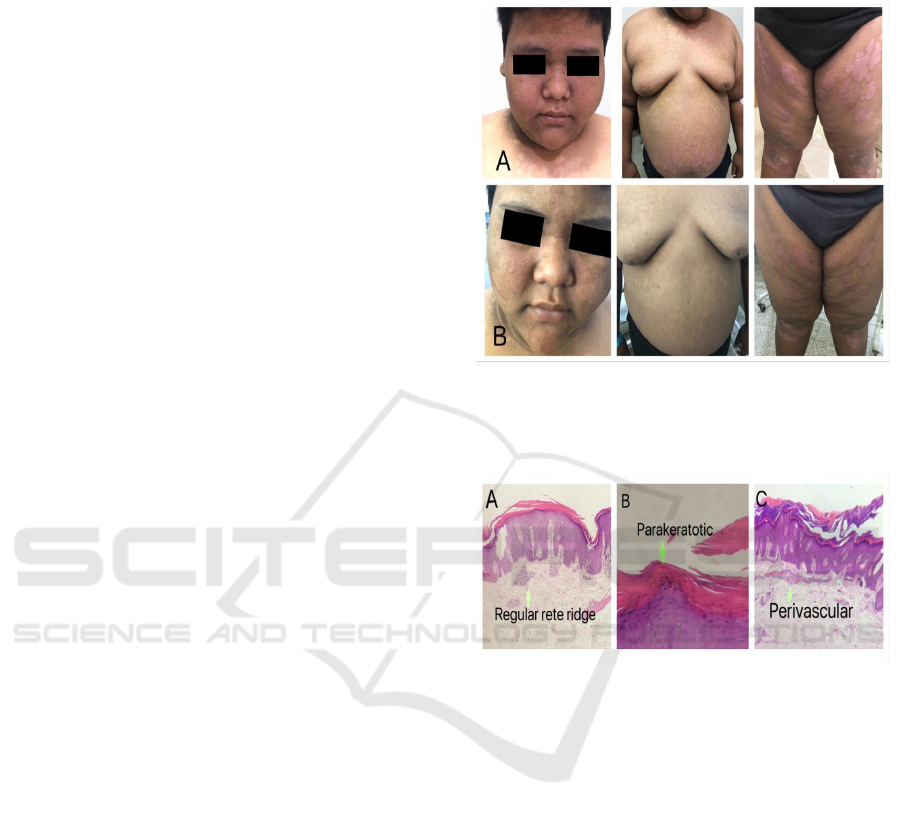
Histopathology examination showed tissue
covered by keratinized stratified squamous
epithelium, hyperkeratotic, parakeratotic, acanthosis,
regular rete ridges, the dermis consisted of skin
adnexa and fibro collagenous stroma connective
tissue with perivascular lymphocytes. No signs of
malignancy. The 10%Potassium hydroxidetestdid
not find any hypha or spores.
The diagnosis of this patient was psoriasis
Vulgaris with a PASI score of 19.9. The patient was
treated with Methotrexate 5mg per 12 hours given
on the first and second day of every week, folic acid
1 mg per day is given on the third to seventh day
every week,0.25%desoximetasone creamapplied to
the lesion twice a dayand 10% urea cream was
applied twice a day as a moisturizer. Therapy was
done for two months, a significant improvement was
found.
Figure 1. (A)First observation there were erythematous
plaques and silvery scales(B)Second observation after two
months therapy
Figure 2. Histopathologic Findings
3 DISCUSSION
A 12-year-old boy withwell-defined erythematous
plaques, partially covered by thick silvery scales on
the face, trunk, belly, elbows, lower limbs and
knees. According to the references, the disorder may
present in1.37 % children aged 10–19 yearswith
solitary lesions or countless plaques in a generalized
distribution. (Bronkers et al, 2015;De Waard-van der
Spek FB et al,2011).
There was no history of psoriasis in his family. A
child with one affected parent has a 14% chance of
developing psoriasis disease, and this rises to 41% if
both parents are affected.(Fortina et al,2017)
The
prevalence of psoriasis patients with an affected
family member is observed to be higher in early-
onset psoriasis (before age 16) than in adult-onset
psoriasis (after age 16). (Bronkers et al, 2015).
Pediatric Psoriasis in Patient with Obesity
381

The patient whose body weight was 120
kilograms with BMI 43 belonged to the obese
category, but this patient had an excellent metabolic
condition. In the literature, obesity as a comorbidity
of psoriasis has been the focus of much
investigation, and the large international cross-
sectional study has demonstrated the increased risk
of being overweight or obese in pediatric psoriasis in
5- to 17-year-old children with psoriasis. (Bronkers
et al, 2015).
Dermatological examination showed erythematous
plaques, partially covered by thick silvery scaleson
face, trunk, belly, elbows, lower limbs, and knees.
Positive auspitz sign.According to the references
psoriasis in children if often similar to that seen in
adult patients. The lesions are well-defined,
erythematous, and papulosquamous, with silvery
scales. The successive removal of psoriatic scales
produces small bleeding points where the thin
suprapapillary epitheliums are torn off (Auspitz
Sign). (De Waard-van der Spek FB et al,2011).
Although the diagnosis of psoriasis is primarily
based on clinical features, a biopsy can help to
confirm the diagnosis in children. Analysis of a skin
biopsy specimen from the patient showed tissue
covered by keratinized stratified squamous
epithelium, hyperkeratotic, parakeratotic, acanthosis,
regular rete ridges, the dermis consisted of skin
adnexa and fibro collagenous stroma connective
tissue with perivascular lymphocytes.Histological
features of psoriasis include parakeratosis, loss of
granular cell layer, elongation of the rete ridges,
neutrophilic aggregates within the epidermis
(microabscesses of Munro) especially common in
early lesions, dilated blood vessel in the dermis, and
perivascular lymphocytic infiltrates. These
characteristics may vary depending on site of
biopsy, psoriasis subtype, and whether children have
been treated with topical and or systemic treatment.
(De Waard-van der Spek FB et al, 2011;
Rapini,2005).
The differential diagnosis oftinea corporis could
be excluded because the lesion in tinea corporis
showed enlarging raised red rings with a central area
of clearing, mycological examination (+).(Fortina et
al,2017)
Patient’s 10% potassium hydroxide test
result did not find any hypha or spores.
The patient was treated with Methotrexate 5mg
per 12 hours three times per week and folic acid
1mg per day given except on the day of
methotrexate therapy. From the results of this
patient's laboratory, there were no contraindications
for methotrexate therapy. Methotrexate is considered
the systemic treatment of choice for children with
moderate-to-severe plaque psoriasis. However, its
use in childhood is also appropriate for PsA,
extensive, recalcitrant, severe or disabling psoriasis,
and erythrodermic or generalized pustular disease
resistant to topical and phototherapy. In children,
methotrexate advantages include the efficacy and
weekly oral dose (0.2–0.7 mg/kg/week). Dose
escalations of 1.25–5 mg/week until the achievement
of clinical benefits, followed by a slow taper to a
maintenance dosage, are advised. Based on a study,
acitretin, MTX and CsA may be considered as first-
line therapy for childhood psoriasis with acceptable
efficacy and few adverse effects, with acitretin
seeming efficient on a plaque, pustular and
palmoplantar psoriasis, methotrexate on plaque and
guttate psoriasis, and CsA on erythrodermic and
palmoplantar psoriasis. Folic acid is routinely
administered to improve tolerability and decrease
the appearance of nausea, macrocytic anemia,
pancytopenia, and hypertransaminasemia. Some
authors prescribe folic acid two days after every
methotrexate dose, while others recommend daily
except on the day of methotrexate therapy
(Napolitano et al,2016).
Topical 0.25% Desoxymethason cream was
given twice aday. Topical corticosteroids have a
vital role in treatment due to antiproliferative, anti-
inflammatory, immunosuppressive, and
vasoconstrictive properties. Desoxymethason is a
potent corticosteroid that can be used on thick
psoriatic plaques (Madiraca et al,2016). Emollients
are used as adjunctive agents to decrease the
associated scaling and dryness but should not
replace medications when inflammation is
present.(Paller et al,2011)
.
4 CONCLUSION
A 12-year-old patient with psoriasis vulgaris and
obesity. The diagnosis was based on the anamnesis
and the clinical features, as well as on
histopathological examinations of our patient's tissue
specimens.The combination treatment
ofMethotrexate and topical corticosteroid
successfullyreduced the PASI Score to 9.9. The
prognosis was quo ad vitam ad bonam, ad sanam
dubia ad bonam, ad cosmeticam ad bonam.
ICTROMI 2019 - The 2nd International Conference on Tropical Medicine and Infectious Disease
382

REFERENCES
Bronkers IMGJ, Paller AS, Van Geel MJ, Van De Kerkhof
PCM, Seyger MMB. 2015. Psoriasis in Children and
Adolescents: Diagnosis, Management and
Comorbidities. June; 17: p. 373-384.
Callen J. P. 2008. Immunosuppressive and
Immunomodulatory Drugs. In: Goldsmith L. A, Katz
S.I, Gilchrest B.A, Paller A. S, Leffell D. J, Wolff K,
editor. Fitzpatrick’s Dermatology in General
Medicine, 8
th
edition. New York: McGraw Hill. p.
2807-2814
De Waard-van der Spek FB, Oranje AP. 2011. Psoriasis.
In: Irvine A, Hoeger P and, Yan A, editor. Harper’s
Textbook of Pediatric Dermatology, 3
rd
edition. West
Sussex: Blackwell Publishing Ltd. p. 80.1-80.7
Dogra S, Bishnoi A. 2018. Childhood psoriasis: what is
new and what is news. Volume 19. October-Desember
: p. 308-314
Fortina A.B, Bardazzi F, Berti S, Carnevale C, Lernia VD
et al. 2017. Treatment of Severe Psoriasis in Children:
Recommendations of an Italian Expert Group. August
MadiracaD, Situm M, Prkacin I, Bulic SO. 2016.
Treatment Options for Pediatric Psoriasis. February;
24(3): p. 175-180
Mahe E. 2016. Childhood Psoriasis. November. 26(6): p.
537-48
Napolitano, Megna M, Balato A. 2016. Systemic
Treatment of Pediatric Psoriasis: A Review. April; 6:
p. 125-142
Paller A.S, Mancini A.J. 2011. Hurwitz Clinical Pediatric
Dermatology. 4
th
edition. New York: Elsevier
Saunders. p. 71-91.
Rapini R.P. 2005. Practical Dermatopathology. Elsevier
Mosby. p.51-52
Weller R.B, Hunter H.J.A, Mann M.W. 2015. Psoriasis.
In. Clinical Dermatology,5
th
edition. West Sussex:
John Wiley & Sons Ltd. p. 52-67
Pediatric Psoriasis in Patient with Obesity
383
