
Sulfasalazine as an Alternative Therapy for
Generalized Pustular Psoriasis:
Case Series and Review of Literature
Jhauharina Rizki Fadhilla
1*
, Eyleny Meisyah Fitri
1
, Windy Keumala Budianti
1
, Endi Novianto
1
1
Department of Dermatology and Venereology Faculty of Medicine Universitas Indonesia/
Dr. CiptoMangunkusumo National Central General Hospital, Indonesia
Keywords: Acitretin, methotrexate, psoriasis, sulfasalazine
Abstract: Generalized pustular psoriasis (GPP), psoriasis of von Zumbusch, is infrequent and notoriously intractable
skin disease, so as the treatments remain challenging. One of the treatments of choice for GPP is acitretin
currently used by most countries. Unfortunately, our national health regulation prohibits acitretin and also
other systemic retinoids. Thus, sulfasalazine has been given to our patients due topoor responseof
cyclosporine and methotrexate (MTX) in previous treatment. We aimed to evaluate the efficacy of
sulfasalazine in GPP. Three patients affected by GPP and unresponsive to previous treatment, received
sulfasalazine started at the dosages of 1 gram/day. The dose was increased related to the response. We
observed one patient with good result after 4 months administration. The other two stopped the treatment
due to lack of response and severe digestive side effect. There were varied results of sulfasalazine therapy in
GPP. It is known to acts against molecular mechanism by inducing neutrophil apoptosis which is abundant
in GPP pathogenesis. Sulfasalazine has warranty of its availability so far, affordable, and shares efficacy as
well.
1 INTRODUCTION
Pustular psoriasis is a type of psoriasis clinically
described by small to large pustules on erythematous
skin. It is subtyped into generalized, localized
variants, and drug-induced pustular psoriasis.
Generalized pustular psoriasis consists of acute GPP,
also known as von Zumbusch type, pustular
psoriasis of pregnancy, and infantile and juvenile
pustular psoriasis. Localized pustular psoriasis
comprises palmoplantarpustular psoriasis and
acrodermatitis continua of Hallopeau. Pustular
psoriasis related drug-induced cases have been
linked with various medications.(Gudjonsson JE et
al, 2012; Sheu JS et al, 2016)
Based on histopathological analysis, pustular
psoriasis lesions express neutrophil-dominant
infiltrate. Large accumulations of neutrophils seen in
the stratum corneum and surrounded by
parakeratosis, culminate in abundant spongiform
pustules of Kogoj and microabscesses of Munro.
These histologic hints of “active” psoriasis are
discerned in pustular psoriasis.( Gudjonsson JE et al,
2012; Kerkhof PC et al,2018; Mansouri B et al
2016
)
Therapy of GPP remains challenging as its rarity
and heterogeneous nature of the disease. The clinical
practice guidelines for psoriasis are based on a
systematic review measuring skin symptoms as
progression mostly(Fujita H et al, 2018; Twelves S
et al, 2019). Fujita et al announced Japanese
guidelines for GPP at 2018. They stressed on
consideration that GPP is systemic inflammatory
response syndrome (SIRS). Consequently, primary
care, systemic maintenance, therapy of cutaneous
lesions, and complications should be highlighted.
(
Twelves S et al, 2019). Both topical and sistemic
agents are regulated as GPP treatments, the latter
including cyclosporine, MTX, acitretin, TNFα
inhibitor, other biologics,(
Fujita H et al, 2018; Twelves
S et al, 2019)
and granulocyte/monocyte adsorption
apheresis (GMA).Despite its controversy, systemic
corticosteroid is recommended in acute phase and as
second-line therapy.,(
Fujita H et al, 2018; Twelves S et
al, 2019)
According to clinical practice guidelines
released by Indonesian Society of Dermatology And
316
Fadhilla, J., Fitri, E., Budianti, W. and Novianto, E.
Sulfasalazine as an Alternative Therapy for Generalized Pustular Psoriasis: Case Series and Review of Literature.
DOI: 10.5220/0009987703160319
In Proceedings of the 2nd International Conference on Tropical Medicine and Infectious Disease (ICTROMI 2019), pages 316-319
ISBN: 978-989-758-469-5
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
Venereology (INSDV), oral acitretin is
recommended as monotherapyfor pustular psoriasis
and erythroderma psoriasis. (Kelompok Studi
Psoriasis Indonesia Perhimpunan Dokter Spesialis
Kulit dan Kelamin Indonesia, 2014).
Sulfasalazine is extensively used in treatments of
inflammatory bowel diseasesand rheumatoid
arthritis;however it israrely as systemic agent for
treatment of GPP.(Gudjonsson JE et al,
2012;Niknahad H et al, 2017; Bertolotto M et al
2009). It is used in therapy-resistant disease or if the
previous systemic agents are not well tolerated.
Therefore, we reportthe consideration of
sulfasalazine therapy as an alternative treatment in
three cases of recalcitrant GPP.
2 CASE
2.1 Case 1
A56 years old female presented with a history of
GPP for 30 years visitedour DermatoAllergo-
Immunology clinic.She came from Wonogiri,
Central Java, and worked as a farmer. She came with
chief complaint extensive scaly erythema and
multiple pustules that form “lake of pus” on her
trunk and extremities accompanied with systemic
symptoms of fever and malaise. She had been
treated with MTX (7,5-10 mg/week), topical and
systemic steroidsin 6 months.Methotrexate was
stopped because the drug had not been available for
weeks. The medication switched to azathioprine for
a month. Regrettably, patient encountered anemia
(hemoglobin level is 10,2 gr/dL). Because of that
reason, we gave sulfasalazine with starting dose
from 1000 mg per day combined with topical
corticosteroid. After two weeks administration,
patient revealed a new erythema with sterile pustules
on her cheeks, and buttocks. We increased the
doseto 1500 mg per day. After one month, the
patient showed no more erythema and sterile pustule
arised. She had taken sulfasalazine for 4 months.
During last two months, she occasionally
experienced a small number of sterile pustules which
vanished after application of topical steroid for
several times. We also evaluated factors that could
trigger flares, include infection, smoking, and drugs.
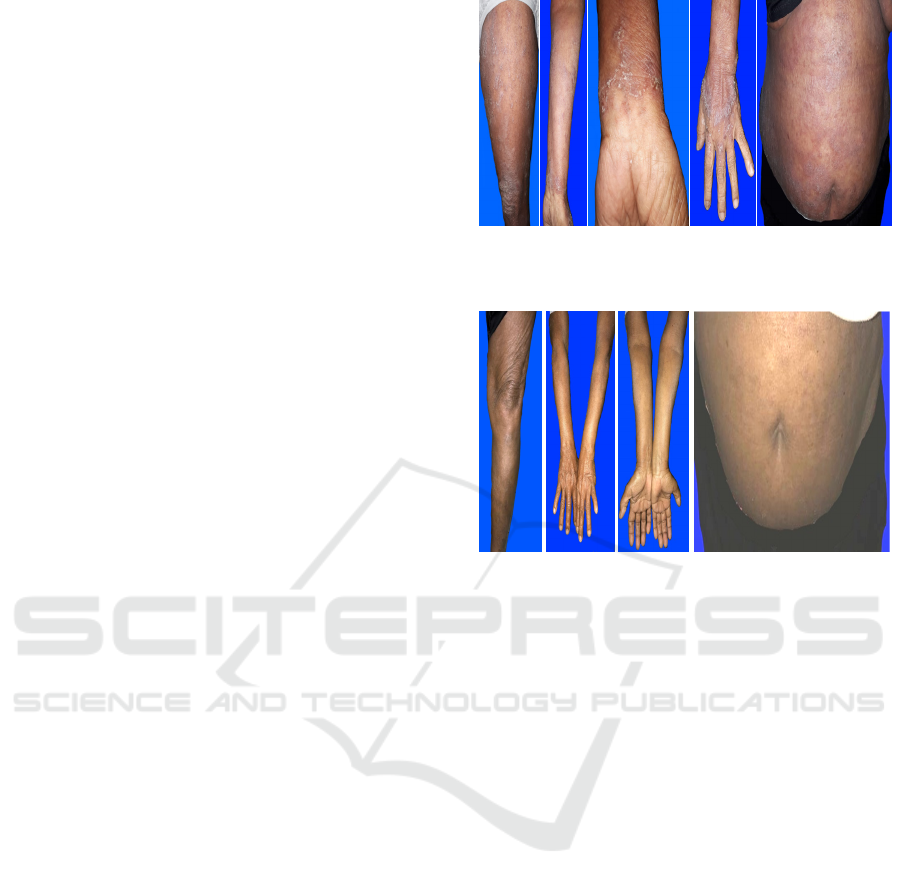
Figure 1.Erythematous plaques with sterile pustules and
scale on left upper leg, lower left arm, left wrist, hand, and
abdomen.
Figure 2. Evaluation after four months therapy of
sulfasalazine revealed marked improvement.
2.2 Case 2
A 23-year-old female, had psoriasis vulgaris since
she was 11 years old.At the age of 13 years,she
experienced GPP with no symptoms of psoriasis
arthritis. She also had -traits thalassemia as other
comorbid. For years the disease was treated with
acitretin, MTX, varying topical and systemic steroid
with poor compliance because of economic burden.
She also had been treated with cyclosporine for 8
months and had a temporary improvement. The GPP
severity measured by body surface area, reduced up
to 1.2%. But, grievously it relapsed again and
cyclosporine did not help anymore. Then, MTX
treatment replaced cyclosporine. It was started at the
third month of oral anti-tuberculosis drug, with
approval internal medicine specialist related to her
pulmonary lung tuberculosis. She was still
experienced recurrent exacerbations of GPP for six
months. We decided to replace MTX with
sulfasalazine (1-2 gram/day) subsequently,
combined with high doses until a maintenance
dosage of oral methylprednisolone (4-20 mg/day).
The severity was moderately improved while in
addition with high dose systemic steroid. A year
after, we terminated sulfasalazine and substituted by
cyclosporine again.
Sulfasalazine as an Alternative Therapy for Generalized Pustular Psoriasis: Case Series and Review of Literature
317

2.3 Case 3
A 27-year-old female came to DermatoAllergo-
Immunology clinic presenting with multiple pustules
and extensive erythematous skin. She is a private
school teacher whose planning to get married and
and refused to take any contraception. She had GPP
for ten years and had been treated with multiple
systemic agents. According to her history,
combination of acitretin and antibiotic was very
effective opposed to MTX and cyclosporine. She
did not want to delay pregnancy after married, so we
discussed about sulfalasazine as a therapeutic choice
with the patient and family. She was agreed to be
given 1000 mg sulfasalazine per day, but after one
month, she experienced severe complaints related to
her digestive tract, such as nausea, vomiting, loss of
appetite, headache, and fatigue. On her own, she
stopped treatment and treated herself by taking
methylprednisolone 1x4 mg per day irregularly.
Three months later, patient entered our emergency
room with erythematous skin accompanied by sterile
pustules that affect almost the entire body. Lastly,
patient and her family are considering treatment with
a biologic agent. While waiting, cyclosporine,
topical and systemic steroid have been administered.
3 DISCUSSION
Acute GPP ishazardoussevere form of psoriasisthat
life threatening. The typical findings are sterile
pustules on erythematous base, and followed by
constitutional symptoms. Varied triggering factors
have been notified, including pregnancy (also named
impetigo herpetiformis), consumption and
withdrawal of corticosteroid, upper respiratory tract
infections, emotional stress, and medicines.
Systemic corticosteroid usage and withdrawal is
notable factor that cause exacerbation of GPP by
inducinginhibition of the inflammatory system.
5
All
of our cases have been taking systemic
corticosteroid, however we tapered the dose down
slowly and with the addition of other systemic
agents. However, it does not rule out the possibility
of using steroids that trigger flares.
To preclude the infection, we consulted our
patients to ears, nose and throat specialist, dentist,
and sexually transmitted infections division.
Infection can also cause to an acute activation of
neutrophils which may affect as a trigger for the
acute GPP. (Gudjonson et al, 2012; James WD,
2016;Fujita H et al, 2018)
Sulfasalazine acts as an anti-inflammatory
agent.(Bertolotto et al, 2009;Wright HL et al, 2010)
.
Sulfasalazine has long been used in treatment of
ulcerative colitis and Crohn's disease, also
rheumatoid arthritis.(Akahoshi et al, 1997; Wright
HL et al, 2010).
.
The drug is composed of both
sulfapyridine and 5-aminosalicylic acid (5-ASA).
Sulfasalazine has a various kinds of effects on
leukocyte functions, namely inhibition on
degranulation, chemotaxis, superoxide generation of
neutrophils,proliferation and production interleukin-
2, and also cytokine produced by
monocytes.(Niknahad et al, 2017; Bertolotto et al,
2009). These mechanism suggests that sulfasalazine
play a role in neutrophil-mediated diseases.
A case of acrodermatitis continua of Hallopeau
(ACH), as one of subtype of pustular psoriasis, was
reported successfully treated with sulfasalazine in
Department of Dermatology, the Hospital of Jiangsu
University, Zhenjiang, China. The improvement
reached after2 weeks and total remission of skin
lesions occurred after one-month therapy.(Li M et
al., 2018). The first case we reported also showed
good efficacy of sulfasalazine administration
without being accompanied by other systemic agents
for 4 months. The patient only received topical
steroids.
The side effect profile of sulfasalazine includes
headache, nausea, and vomiting, which occur in
more or less one-third of patients. Hemolytic anemia
can occur associated with glucose-6-phosphate
dehydrogenase (G6PD) deficiency. Thus, it is
important to work up baseline data of complete
blood cell count (CBC), comprehensive
metabolic panel (CMP), and G6PD. Repeat CBC
and CMP weekly for 1 month, then every 2 weeks
for 1 month, then monthly for3 months, and then
every 3 months.
1
In this case report, we found one of
three patients,the third caseexperienced
gastrointestinal side effects such as nausea,
vomiting, loss of appetite with headache and fatigue.
Adherence to medication appears to also play a role
in its success. The third case had a history of steroid
use that does not comply with the recommendation
of administration increases the risk of recurrent of
GPP. The other treatment that can be done is the
biologic agent.
4 CONCLUSION
The three cases demonstrate both clinical benefit and
failure that were received administration of
sulfasalazine for GPP. The mechanism of
sulfasalazineas an anti-inflammationin skin diseases
ICTROMI 2019 - The 2nd International Conference on Tropical Medicine and Infectious Disease
318

is intricate; however, its efficacy in treating these
clinically distinct cases of GPP suggests a different
underlying pathophysiological mechanism. Based on
this case series and a previous case report,
sulfasalazine can be conceived as optional treatment
choice for patients with GPP.
REFERENCES
Gudjonsson JE, Elder JT. Psoriasis. In: Goldsmith LA,
Katz SI, Gilchrest BA, Paller AS, Leffell DJ, Wolff K,
editors. Fitzpatrick's Dermatology in General
Medicine. 8th edition. New York: McGraw-Hill; 2012.
p. 197-231
Kerkhof PC, Nestle FO. Psoriasis. In: Bolognia JL,
Schaffer JV, Cerroni L, editors. Dermatology 4th
edition. New York: Elsevier; 2018. p. 138-60
James WD, Berger TG, Elston DM, Neuhaus IM.
Andrew’s diseases of the skin. 11th edition.
Philadelphia: Elsevier; 2016. p. 185-98.
Sheu JS, Divito SJ, Enamandram M, Merola JF. Dapsone
Therapy for Pustular Psoriasis: Case Series and
Review of the Literature. Dermatology.
2016;232(1):97–101.
Mansouri B, Benjegerdes K, Hyde K, Kivelevitch D.
Pustular psoriasis: pathophysiology and current
treatment perspectives. Psoriasis: Targets and
Therapy. 2016 Sep;Volume 6:131–44.
Fujita H, Terui T, Hayama K, Akiyama M, Ikeda S,
Mabuchi T, et al. Japanese guidelines for the
management and treatment of generalized pustular
psoriasis: The new pathogenesis and treatment of
GPP. The Journal of Dermatology. 2018
Nov;45(11):1235–70.
Twelves S, Mostafa A, Dand N, Burri E, Farkas K, Wilson
R, et al. Clinical and genetic differences between
pustular psoriasis subtypes. Journal of Allergy and
Clinical Immunology. 2019 Mar;143(3):1021–6.
Kelompok Studi Psoriasis Indonesia Perhimpunan Dokter
Spesialis Kulit dan Kelamin Indonesia. Pedoman
tatalaksana psoriasis dan informed consent; 2014. p.
16.
Niknahad H, Heidari R, Mohammadzadeh R, Ommati
MM, Khodaei F, Azarpira N, et al. Sulfasalazine
induces mitochondrial dysfunction and renal injury.
Renal Failure. 2017 Jan;39(1):745–53.
Bertolotto M, Dallegri F, Dapino P, Quercioli A, Pende A,
Ottonello L, et al. Sulphasalazine accelerates apoptosis
in neutrophils exposed to immune complex: Role of
caspase pathway. Clinical and Experimental
Pharmacology and Physiology. 2009
Nov;36(11):1132–5.
Akahoshi T, Namai R, Sekiyama N, Tanaka S, Hosaka S,
Kondo H. Rapid induction of neutrophil apoptosis by
sulfasalazine: implications of reactive oxygen species
in the apoptotic process. Journal of Leukocyte
Biology. 1997 Dec;62(6):817–26.
Wright HL, Moots RJ, Bucknall RC, Edwards SW.
Neutrophil function in inflammation and inflammatory
diseases.Rheumatology. 2010 Sep 1;49(9):1618–31.
Li M, Zhang Y, Xu H, Chen Z-Q, Li Y-M. A case of
acrodermatitis continua of Hallopeau (ACH)
successfully treated with sulfasalazine. Dermatologic
Therapy. 2018 May;31(3):e12595.
Sulfasalazine as an Alternative Therapy for Generalized Pustular Psoriasis: Case Series and Review of Literature
319
