
The Problem Strategy and Emotion Focus Coping with Pain Intensity
in Post Major Surgery
Friska Ernita Sitorus
1
, Dewi Tiansa Barus
1
, Siti Marlina
1
, Fithri Handayani Lubis
2
, Yunita Syahputri
Damanik
2
, G. F. Gustina Siregar
3
1
Nursing Faculty of DELI HUSADA Deli Tua Health Institute Deli Tua, Indonesia
2
Public Health Faculty of DELI HUSADA Deli Tua Health Institute Deli Tua, Indonesia
3
Midwifery Faculty of DELI HUSADA Deli Tua Health Institute Deli Tua, Indonesia
Keywords: Problem, Emotion Focus Coping, Pain Intensity, Post Mayor Surgery.
Abstract: Adaptive individual coping strategies are needed for post-major surgery patients to minimize the patients’
pain after surgery. If the patient's coping is increasingly adaptive so the patient's pain intensity decreases.
This study used cross sectional design with 96 respondents who were post-major surgery patients in the
category of post-oncology and digestive surgery, with Spearman statistical test. The results showed that
there was relationship between problem (r = 0.445) and emotion focus coping (r = 0.449) with pain intensity
(α <0.005). After identifying the types of coping strategies that majority used by patients are emotion
problem coping with social withdrawal domains and the minority are problem focus coping domain express
emotion. Respondents followed the instructions to minimize pain, and get closer to God..
1 INTRODUCTION
Pain is an unpleasant individual experience that
can cause potential and actual tissue damage (Elahe,
2018). Pain in postoperative patients has
characteristics that involve damage starting from the
integument, muscle tissue, vascular and causing
long-lasting pain effect during recovery (Roht,
2017). Pain in postoperative patients is reported at
severe level (Lamontagne, 2017). Pain is problem
that must receive attention, not only in postoperative
patients, because pain can negatively affect the
health status of patients (Roykulcharoen, 2017).
Individuals who feel pain feel depressed or suffer
and seek efforts to relieve pain. Nurse uses various
interventions to relieve pain or restore comfort. The
nurse cannot see or feel the pain the patient feels.
Pain is subjective, there are no two individuals who
experience the same pain and nothing two similar
pain events generate response or identical feelings
for individuals. Pain is a source of frustration, both
patients and health workers (Potter and Perry, 2017)
Providing analgesics does not the main control
holder to overcome the patient's pain complaints
because it has side effects that increase the recovery
time. In addition to pharmacological therapy, there
are also non-pharmacological therapy options
available to control pain. This method can be
combined with pharmacological methods that focus
on better management in reducing pain (Tetti, 2017).
Coping strategy is the way it is done to change
the environment or the situation or solve the
problem which is being felt or faced. Effective
coping will produce persistent adaptation which is a
new habit and repair from old situations, while
coping which is not effective end up maladaptive
namely behavior the deviant from normative desires
and can hurt yourself or other people or the
environment, each individual Coping is not alone
and not only use one strategy but it can do it varies,
it depends from ability and individual conditions
(Rasmun 2017)
If pain occurs after surgery, the combination of
non-pharmacological techniques with
pharmacologists is the most effective method for
pain relief (Suza, 2017).
According to Marialaura (2017) Coping can
resolve pain in chronic patients, namely
Fibromyalgia. In this study, patients used problem
focus coping. Effective coping will produce
permanent adaptation which is a new habit and
improvement of the old situation, while ineffective
coping ends in maladaptive namely behavior that
deviates from normative desires and can harm
Sitorus, F., Barus, D., Marlina, S., Lubis, F., Damanik, Y. and Siregar, G.
The Problem Strategy and Emotion Focus Coping with Pain Intensity in Post Major Surgery.
DOI: 10.5220/0009974205210527
In Proceedings of the International Conference on Health Informatics and Medical Application Technology (ICHIMAT 2019), pages 521-527
ISBN: 978-989-758-460-2
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
521
oneself or others or the environment, each individual
in doing coping is not alone and not only use one
strategy but can do it varies, it depends on the
abilities and conditions of the individual (Rasmun
2017).
In addition to coping strategy of Benson's
relaxation in minimizing the intensity of pain in post
section patients, it is very effective to do where the
patient is able to manage his pain, so the patient's
pain intensity decreases (Sedigheh, 2017).
Distraction giving in minimizing pain in patients on
intra-spinal injections given for patients who will
undergo effective chemotherapy is done (Shirkey,
2019)
According to International Association for the
Study of Pain (IASP), there are five models used in
dealing with patient pain, including: cognitive /
behavioral models, emotional models, coping
models, fear avoidance models and acceptance
models. From the five models, the coping model is
one of the best models used to insure the pain
experienced by patients. Coping strategy is one of
the strategies used by patients in reducing,
overcoming, dealing with pain that involves the
behavior and cognitive of the patient itself. Effective
coping will produce permanent adaptation which is a
new habit and an improvement from the old
situation, while ineffective coping ends in
maladaptive i.e. behavior that deviates from
normative desires.
2 METHOD
This research was quantitative study by using an
explanatory analytic design with cross-sectional
approach. Research location was in RSUP. H Adam
Malik Medan. The population of this study were
post-major surgery patients with minimum sample
size of 96 people. Taking samples used consecutive
sampling. The selected respondents were
postoperative digestive patients, postoperative
oncology patients, postoperative patients at least 3rd
day, maximum patient pain scale of 6, patients
willing to be respondents, patients understood
instructions both verbally and writing and they were
≥ 18 years old.
The respondent coping strategy was measured by
using coping strategy inventory (CSI) instrument
consisting of 32 statement items, consist of Problem
Solving, Cognitive Restructuring, Express Emotions,
Social Support, Problem Avoidance, Wishful
Thinking, Self Criticism, Social Withdrawal whereas
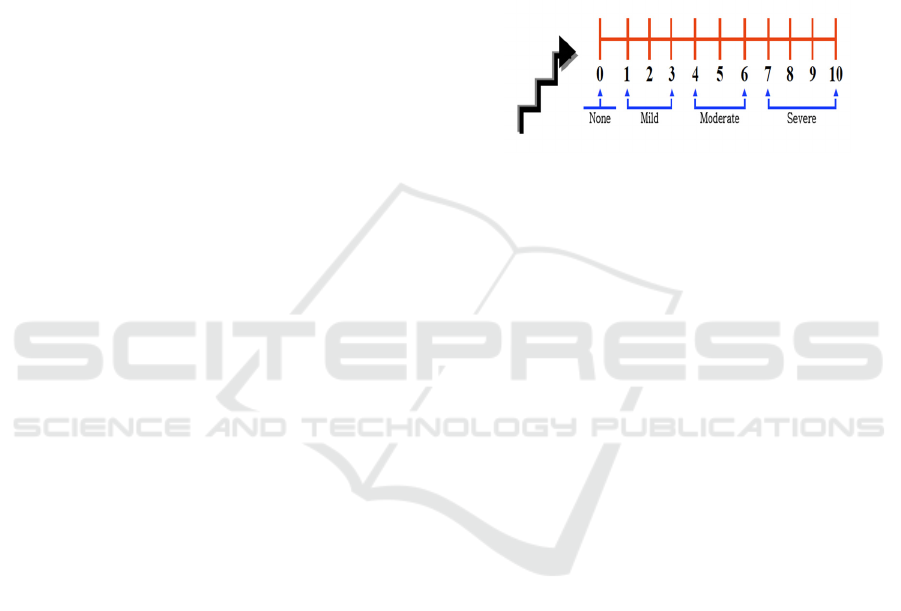
each each item consist of 4 statements. Pain intensity
was measured by using numeric rating scale (nRs)
on 1-10 scale. Before conducting research, the
instrument is tested for validity and reliability. In the
results of content validity testing given to 3 experts,
value of 0.895 was obtained. While the testing
results of construct validity from 30 respondents
obtained all items of valid statement with a
Cronbach Alpha value of 0.90.
Data were analyzed by using Pearson correlation,
where previously the data were analyzed by
normality test with Kolmogorov-Smirnov.
Figure 1 : Numeric Rating Scale
3 RESULT
3.1 Respondents Characteristics
The sample in this study amounted 96
respondents with characteristics showed the majority
of late adulthood namely 36-45 years as many as 23
people (24%), male sex as many as 35 people
(36.5%), the majority of Islamic religion as many as
72 people (77.1 %), the majority Batak tribe as many
as 34 people (35.4%), with the majority marital
status married as many as 91 people (94.8%), with
senior secondary education as many as 39 people
(40.6), the average job as many as 55 entrepreneurs
(57.3) %), with operations history that had never
been carried out before as many as 52 people (54%)
with the type of oncology surgery as many as 55
people (57%).
3.2 Respondents’ Coping Strategy
In this study coping strategies are divided into
two namely problem focus coping and emotion
focus coping. Based on problem focus coping, it is
found that the highest mean is 9.49 in sub social
support with standard deviation value of 2,294 and
the lowest mean is 9.16 and standard deviation of
2,390 in sub cognitive restructuring. Whereas based
on emotion focus coping, the highest mean is 10.55
with standard deviation of 2,280 in sub social
withdrawal and the lowest mean is 8.98 and a
standard deviation of 2,371 on sub wishful thinking.
ICHIMAT 2019 - International Conference on Health Informatics and Medical Application Technology
522

Table 1: Frequency distribution based on problem focus
coping.
Problem
Avoidance
Cognitive
Restructuring
Express
Emotion
Sosial
Support
96 96 96 96
0 0 0 0
9.89 9.16 9.44 9.49
2.401 2.390 2.214 2.294
12 11 11 11
Table 2: Frequency distribution based on emotion focus
coping.
Problem
Avoidance
Wishful
Thinking
Self
Critism
Social
Withdraw
96 96 96 96
0 0 0 0
9.89 8.98 9.43 10.55
2.401 2.371 2.051 2.280
12 12 10 12
3.3 Pain Intensity
Based on the study result, it was found that the
pain intensity with coping strategies: problem focus
coping experienced mild pain as many as 15 people
(14.4%) and moderate pain as many as 22 people
(21.12%) while in emotion focus coping experienced
mild pain as many as 36 respondents (34.56%) and
moderate pain as many as 23 respondents.
Table 3: Pain intensity
Category frequensy percent
Mild 50 52
Moderate 46 48
Total 96 100
3.4 Normally Test
The results of the study explain that data is not
normally distributed by using Kolmogorov-smirnov
with a p-value of 0,000 Where p-value <0.05 means
data is not normally distributed.
Table 4: Data normally test problem focus coping with
pain intensity
Problem focus
coping
Kolmogorov-Smirnov
a
Statistic Df Sig.
Mild .452 22 .000
Moderate .361 74 .000
Emotion focus coping normality test results with
pain intensity explain that that data is not normally
distributed by using Kolmogorov-smirnov with a p-
value of 0,000 Where p-value <0.05 means data is
not normally distributed.
Table 5: Data normally test emotion focus coping with
pain intensity
Emotion focus
coping
Kolmogorov-Smirnov
a
Statistic Df Sig.
Mild .456 19 .000
Moderate .357 77 .000
3.5 The Relationship between Coping
Strategy with Pain Intensity
The study results about the relationship between
coping strategies: problem focus coping with pain
intensity obtained results with p-value of 0.02 with
correlation value of 0.430 in the negative direction
where if the coping strategy is good then pain
decreases
Table 6: Relationship problem focus coping with pain
intensity
Problem
focus coping
Pain
intensity
Problem
focus
Coping
Correlation
Coefficient
1.000 .430
*
Sig. (2-tailed) . .027
N 96 96
Pain
intensity
Correlation
Coefficient
.430
*
1.000
Sig. (2-tailed) .027 .
N 96 96
The result between emotion focus coping with
pain intensity obtained results with p-value of 0,000
with correlation value of 0.449 means there is
relationship between coping strategies with the pain
intensity in post-major surgery patients with
negative direction where if we use the the better
coping, so the pain that feels decreases
Table 7: Relationship emotionfocus coping with pain
intensity
Problem
focus coping
Pain
intensity
Emotion
focus
Coping
Correlation
Coefficient
1.000 .449
*
Sig. (2-tailed) . .000
N 96 96
Pain
intensity
Correlation
Coefficient
.449
*
1.000
Sig. (2-tailed) .000 .
N 96 96
The Problem Strategy and Emotion Focus Coping with Pain Intensity in Post Major Surgery
523

4 DISCUSSION
4.1 Coping Strategy
Coping is a process that continually strives to
change the cognitive and behavioral efforts of both
external and internal demands where the judgment is
obtained from humans themselves (Garbee.D, 2017).
Coping strategies are ways that individuals do in
solving problems, adjusting to changes, and
responding to threatening situations (Keliat, 2016).
If an individual is under stress, he will use variety of
ways to overcome it, individuals can use one or
more available coping sources (Rasmun, 2017).
Reportedly, in general the coping strategy that is
often used by post-major surgery patients is adaptive
coping strategy (Kaczynski, 2017). These results are
reinforced by studies conducted by Kaczynski that
based on respondents' coping strategies, it shows
that coping strategies used by post-major surgery
patients are generally adaptive obtained from social
or family support, trust in God and ability in
emotional management (DeGraff, 2018). It is also
illustrated from the results of research conducted by
Wong (2017) that coping strategies used by post-
major surgery patients are generally adaptive coping
strategies where family support plays an important
role in the recovery period for pain felt by patients.
According to DeGraff the most universal coping
strategy used by respondents is emotion focus
coping which aims to minimize the perceived stress
that triggers pain in spinal injury (DeGraff, 2018).
Likewise, Borland expressed that post-oncology
patients used emotion focus coping more identical in
dealing with perceived problems (Lily M, 2018). It
is also supported by studies conducted by Lilly that
patients who experience identical collisions or
accidents use emotion focus coping, where patients
who use emotion focus coping at least more often
experience more pain symptoms (Mandl, 2017).
After being identified from the types of coping
strategies, social withdrawal is a type of coping
strategy that the majority of patients use in reducing
the intensity of pain that is felt around 88.7% which
is part of emotion focus coping. In this case the
patient is more identical to follow the instructions to
overcome the pain felt, pray to God, and try to
convince themselves with the situation experienced
by the patient. Social withdrawal is a principle of
coping strategy where the individual sees the
positive side of pain experienced in his life by
looking for the meaning or benefit of the experience.
Mandl said that patients who can see the positive
side of what is experienced are far better than
patients who are always anxious about their
conditions (Folkman, 2017). Lenti (2017) conducted
postoperative patients who do not try to see the
positive side of themselves in their recovery are
more likely to experience more serious and ongoing
pain.
The study results also found that the most
minorities of coping strategies used by patients is
79.4% express emotion. Express emotion is an
individual trying to find support and use the
assistance from others in the form of advice or
action in overcoming the problem (Gallo, 2017). The
study results are strengthened from Gallo's research
result where postoperative patients are very
commonly experiencing cognitive and emotional
function decline. When analyzed that the decline in
perception of cognitive function can cause decrease
in emotional function, which after being investigated
between cognitive declines is strongly associated
with decreased emotional function in postoperative
patients (Owen, 2016). Likewise, research
conducted by Owen in postoperative oncology
patients, where express emotion is always followed
by a change in the level of patient cognition. Even
though the results do not show strong relationship,
each patient's express emotion is always
accompanied by cognitive change in the patient
(Sharpe, 2017). Furthermore Sharpe reported that
problem solving and cognitive restructuring have a
role in reducing stress, where pain that occurs with
postoperative patients can also be caused by stress
(Aubun, 2017).
4.2 Pain Intensity
Pain intensity is description about how severe
pain is felt by individuals, measurement of pain
intensity is very subjective and individual and the
possibility of pain in the same intensity is felt very
differently by two different people. Pain
measurement with the most likely objective
approach used the body's physiological response to
pain itself. However, measurements with this
technique also cannot provide a definite picture of
the pain itself (Tamsuri, 2017).
According to Benedetti (1990), intense pain
stimulates stress reactions that adversely affect the
heart and immune systems. When pain impulses are
transmitted, muscle tension increases, as does local
vasoconstriction. Ischemia at the site of pain causes
further stimulation of pain receptors. When these
painful impulses spread centrally, sympathetic
activity is exacerbated, which increases myocardial
demand and oxygen consumption.
ICHIMAT 2019 - International Conference on Health Informatics and Medical Application Technology
524

The study results are same as Smeltzer & Bare
report which states that after undergoing surgery, the
patient feels postoperative pain stimulation because
it is caused by mechanical stimulation of the wound
which causes the body to produce pain chemical
mediators. Besides this, patients with severe pain are
absent, high pain intensity usually occurs on 2nd day
(Logan, 2017).
There are several factors that affect the pain
itself, including age, gender, ethnicity, etc. From the
study results, the majority of respondents
experienced moderate pain in late adulthood. Pain in
late adult patients can be complex because it is
related to pharmacodynamics and pharmacokinetics
which can affect the body's response to pain (Suza,
2017). From the study results also found that women
tend to experience mild pain compared to men. It is
in line with Logan & Rosen study where women
tend to show pain compared to men due to
anticipatory pressure. Whereas in ethnicity term, it is
found that Batak tribe show more pain than other
tribes (Guyton, 2017). It is supported by Suza's
research that Batak tribe responds the pain by
crying, screaming, or angry (Lamontagne, 2018).
According to gate control theory, pain impulses
can be regulated or inhibited by defense mechanisms
throughout the central nervous system. This theory
says that pain impulses are delivered when defense
is opened and an impulse is inhibited when defense
is closed. The effort for closing defense is the basis
theory of pain relief. It can be done by modifying the
patient's coping strategy (Guyton, 2018).
The study results are also almost same with
Lamontagne research that postoperative pain will
decrease on the 2nd day. An effective coping
strategy is given after 2nd day to minimize pain
[24]. Likewise, Roth research that pain decreases on
3rd day, especially if it’s adapative patient’s coping
(Aubun, 2017).
According to Elizabeth G (2012), patients often
report that pain has subsided on the 3rd day after
surgery. Pain will increase if the mood, sleep quality
and stress cannot be maintained, during this pain
period it is expected that family can provide support
to respondents in minimizing the pain experienced.
4.3 The Relationship between Coping
Strategy with Pain Intensity
Postoperative patient pain is caused by a tissue
incision in the operating area, besides that the pain
will also increase along with the patient's stress
which can disrupt sleep patterns, the patient's
appetite for anxiety. All of these things will
stimulate the amyglada which is part of the limbic
system associated with emotional components of the
brain. The neurological response of the amygdala is
transmitted and stimulated the hormonal response of
hypothalamus. The hypothalamus releases the
hormone Corticotropin-Releasing Factor (CRF)
which stimulates the pituitary to release another
hormone, adrenocorticotropic hormone (ACTH),
into blood. ACTH instead stimulates the adrenal
glands to produce cortisol, a small gland that is
above the kidney which will stimulate
vasoconstriction of blood vessels which will cause
pain (Shirkey, 2018). Coping strategy is one way
that can be used by patients in reduce and resolve
pain that involves the patient's own behavior and
cognitive. Adaptive and appropriate coping will
provide the ability for patients to adjust and be ready
to deal with stressors in the form of: pain, loss of
function or damage to body tissue and decreased
mobility, etc.
According to Mandl, it is reported that about 8%
of postoperative patients have coping strategies by
using Social withdrawal, and it was also described
that almost three times occur pain intensity decrease.
The pain intensity that occurs in patients on scale of
moderate to severe pain on postoperative at first day
and in this case the patient is more identical use
pharmacological drugs to reduce pain that is felt, and
pain will decrease on a moderate to mild scale on the
3rd day post operation. In this study Social
withdrawal appears to be more important for patients
who have recently undergone surgery, where in this
case the patient has more leverage to follow the
instructions to reduce the pain that is felt, and it has
started to accept the situation that occurs with an
approach to God [26]. It is same with Borland
research results (2018), that the intensity of pain
decreases with the adaptive coping strategies usage
in chronic patients undergoing dialysis
(Haemodialisa). In this case the patient has entered
into palliative care where the patient must be able to
make strategies in minimizing the pain that is felt.
Research conducted by Shirkey and Kezia on
Dispositional versus Episode Specific Assessment of
children's coping with pain with sample of 116
children who experience abdominal pain. The results
show that coping is higher level of all variables that
can reduce pain. Children are assisted by family or
parents in order to relieve the pain felt by the child.
Likewise, research conducted on the
effectiveness of coping usage in adolescent patients
after spinal surgery, it is obtained good results of
coping will minimize pain, coping strategies can be
used during recovery to reduce pain after surgery,
The Problem Strategy and Emotion Focus Coping with Pain Intensity in Post Major Surgery
525

and it is done on the 2nd day post surgery (Marie,
2018).
Based on the study results, from the types of
coping strategies namely problem focus coping and
emotion focus coping, it was found that emotion
focus coping has high value in minimizing pain even
though problem focus coping has another role. It is
done in post mastectomy patients. In this case in
addition to coping strategies, the patient's cognitive
regulation must also be done because in addition to
the pain that is felt there is also loss of limbs which
can increase the patient's pain (Moore, 2018).
Patient coping strategies in post-hysterectomy
surgery are emotion focus coping, for example, the
acceptance of pain that is felt, seeking support and
diversion to the pain felt by patients, the emotion
focus coping usage can not be separated from coping
strategies with problem focus coping, the results
show that patients use emotion focus coping is
always followed by problem focus coping and in this
case it is difficult to identify patient coping because
each patient has different amount of coping (Moore,
2018).
Likewise the study conducted where the research
is done on post mastectomy patients, the results
obtained that coping has strong contribution in
minimizing postoperative pain (Lamontagne, 2017).
Thus it can be clearly seen that the respondent
coping strategy has very important role to minimize
the pain intensity in post-major surgery patients.
5 CONCLUSIONS
There is relationship problem (r = 0.449) and
emotion focus coping (r = 0.445) with the pain
intensity where the increasing coping of the
individual, the intensity of pain decreases with the
direction of negative correlation. Emotion focus
coping is more used by patients to minimize the pain
felt. Emotional settings were given starting on the
2nd day after the operation.
REFERENCES
Auburn, F (2017), The elderly patient and postoperative
pain treatment. Journal Clinical Anaesthesiology, 21,
109 – 127
Borland (2018), Using information for emotion focus
coping : cancer patients use of a cancer helpline.
British journal of health psychology
DeGraff (2018), Emotion focus coping : A primary
defense against stress people living with spinal cord
surgery. Journal of rehabilitation Vol.74, Number 1
Elahe, Reza (2018). Pain Coping Strategies and Their
Relationship with Unpleasant Emotions (Anxiety,
Stress, and Depression) and Religious Coping in
Cancer Patients. Middle East Journal of Cancer; July
2018; 9(3): 208-216
Folkman &Lazarus (2017), Stress Appraisal and Coping.
New York: Springer
Garbee D.D, Judith A (2017), Coping With The Stress
Surgery. Association of Operating Room Nurses.
AORN Journal; May 2001; 73, 5; ProQuest
Gallo, C.L (2017), Perceived cognitive function and
emotional distress following coronary artery bypass
surgery. Journal of behaviour medicine, Vol.28, No.5
Guyton A.C, Hall J.E (2017) , Buku Ajar Fisiologi
Kedekteran, Edisi 11. Alih bahasa Irawati EGC,
Jakarta.
Kaczynski, J.K (2017), Anxiety, coping, and disability : A
test of mediation in a pediatric chronic pain sample.
Journal of pediatric psychology 36(8). 932-941
Keliat, B.A ( 2016), Proses Keperawatan Kesehatan Jiwa.
Jakarta : EGC
Lilly M (2018), Intimate partner violence and PTSD : The
moderating role emotion focus coping.
Lenti (2017), Social Withdrawal Worsens Pain After
Surgery
Logan, E, D., & Rose, B, J.(2017). Gender differences in
post-operative pain and patient controlled analgesia
use among adolescent surgical patients diakses pada
tanggal 10 Januari 2014 dari
http://www.sciencedirect.com/science/article/pii/S030
4395904001186
Lamontagne L, Josept T, Michele H (2018), Effect Of
Coping Instruction In Reducing Young Adolescents
Pain After Mayor Spinal Surgery. Journal Ortthopedic
Nursing
Mandl (2017), Study: People Who Are Socially
Withdrawal Experience More Pain After Hip
Replacement
Marie C (2018), Self-coherence, coping and mood in
women following hysterectomy
Moore (2018), Relationship among optisims, cognitive
appraisal, coping strategies, and psycholocial
adjustment in Thai women newly diagnosed with
mastectomy
Marialaura (2017). Coping strategies and perceived social
support in fibromyalgia syndrome: Relationship with
alexithymia. Scandinavian Journal of Psychology
Rasmun. (2017). Stres, Koping dan Adaptasi: Teori dan
Pohon Masalah Keperawatan (Edisi 1). Jakarta:
Sagung Seto.
Roth, Maya L (2017), Demografic and Psychosocial
predictors of acute perioperative Pain For Total Knee
Arthroplasty. The Journal of the Canadian Pain
Society; Autumn 2007; 12, 3; ProQuest Medical
Library
ICHIMAT 2019 - International Conference on Health Informatics and Medical Application Technology
526

Roykulcharoen, V, Good, M (2017), Systematic
Relaxation To Relieve Post operative Pain, Advanced
Nursing, Vol.48, 140-148
Suza, D.E (2017), Pain experiences between Javanese and
Bataknese patients with major surgery in Medan,
Indonesia
Sedigheh Fooladi (2019). Effect of Distraction Therapy on
Physiological Indices and Pain Intensity Caused by
Intra-Spinal Injection of Chemotherapy Drugs in
Cancerous Children: A Clinical Trial. Medical -
Surgical Nursing Journal
Shirkey C.K, Craig S.M, (2019), Dispositional Versus
Episode-Specific Assessment of Children’s Coping
with Pain. Journal of Pediatric Psychology 36(1) pp.
74–83
Sharpe, S (2017), Problem solving versus cognitive
restructuring of medically ill seniors with depression
(PROMISE-D Trial): study protocol and design.
Retrieved from :
http://www.Biomedcentral.com/1471-244X/12/207
Tamsuri, A. (2017). Konsep dan penatalaksanaan nyeri.
Jakarta : EGC.
Tetti Solehati1 and Yeni Rustina (2017). Benson
Relaxation Technique in Reducing Pain Intensity in
Women After Cesarean Section. Journal
Anesthesiology and Pain Medicine
Owen, E.J (2016), Self-report and linguistic indicators of
emotional expression in narratives as predictors of
adjustment to cancer. Journal of behaviour medicine,
Vol.29, No.4
Wong, P.T.P, Reker G.T & Peacock, E (2017), The
resorce-congruence model of coping and the
development of the coping schemas inventory.
Handbook of multicultural perspective on stress and
coping . NewYork, NY : Springer.
The Problem Strategy and Emotion Focus Coping with Pain Intensity in Post Major Surgery
527
