
The Proportion of Asymptomatic Bacteriuria among Pregnant
Women in a Primary Health Centre Medan, Indonesia
Putri Wulandari
1
, Rina Yunita
2*
1
Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia
2
Department of Microbiology, Universitas Sumatera Utara, Medan, Indonesia
*Corresponding author
Keywords: Pregnant women, asymptomatic bacteriuria, UTI
Abstract: Pregnancy is a risk factor for urinary tract infection (UTI). UTI in pregnant women is generally
asymptomatic bacteriuria. Although asymptomatic, 40% of asymptomatic bacteriuria can develop into
symptomatic UTI if left untreated, this condition can increase lower weight in infants and premature labor.
Screening and treatment for asymptomatic bacteriuria reduce the risk of symptomatic UTI and
complications. The objective of this study was to determine the proportion of asymptomatic bacteriuria in
pregnant women at the Padang Bulan Health Center Medan. This study is a descriptive study with a cross-
sectional design involving 50 pregnant women who came to the Padang Bulan Health Center. Data was
obtained by taking the central portion of urine and examine them for UTI. The results of the study found
significant bacteriuria as many as in 14 pregnant women (28.0%) with Escherichia coli (28.6%) as the most
common bacteria. The highest proportion was found in women aged 16-25 (57.1%), with income
<Rp.1,000,000, had sexual activity in the last 2 weeks (64.3%), nullipara (71.4%), and with gestational age
13-26 weeks (50.0%). Meropenem, ceftazidime, and nitrofurantoin were the antimicrobials still effective
against these isolates.
1 INTRODUCTION
Urinary tract infection (UTI) is a significant public
health problem worldwide. More than 10 million
outpatient visits and nearly 1 million emergency
department visits in the United States are related to
UTI every year. Women bear the most risk of
infections, nearly half of all women will experience
at least one episode of UTI during their lifetime.
This difference is attributed to factors such as the
urethra is shorter in women, and one-third of the
lower part of the urethra continues to be
contaminated with pathogens of the vagina and
rectum, women tend not to empty their bladder
completely like a man, and the female urogenital
system is exposed to bacteria during sexual
intercourse (Pais and reinstalled, 2018).
Pregnancy itself is an independent risk factor
for UTI (Pais and reinstalled 2018). UTI in
pregnancy generally do not cause symptoms or
asymptomatic bacteriuria (Bukitwetan et al., 2004).
It is defined as positive bacteriuria if the colony
counts yielding bacterial growth of ≥ 10
5
CFU/ml of
urine midstream taken by the method of clean-catch
(Azkia, 2018). Although the incidence of bacteriuria
in pregnant women is similar to that in the
nonpregnant, the incidence of pyelonephritis in
pregnant women is significantly increased compared
with non-pregnant women (Macejko and Schaeffer,
2006). The anatomic and physiologic changes
induced by the gravid state significantly alter the
natural history of bacteriuria, these changes may
cause pregnant women to be more susceptible to
pyelonephritis and may require alteration of therapy.
About 20% to 40% of pregnant women with
untreated bacteriuria will develop pyelonephritis
(Schaeffer et al.,2016) and may lead to adverse
obstetric outcomes such as prematurity, low birth
weight, and higher fetal mortality rate (Turpin et al.,
2007). Therefore, the treatment of bacteriuria early
in pregnancy has been shown to decrease the
incidence of pyelonephritis by 90% (Macejko and
Schaeffer, 2006).
Detection asymptomatic bacteriuria in
pregnancy is important so asymptomatic UTI could
be prevented with treatment. Screening for
Wulandari, P. and Yunita, R.
The Proportion of Asymptomatic Bacteriuria among Pregnant Women in a Primary Health Centre Medan, Indonesia.
DOI: 10.5220/0009864102470252
In Proceedings of the 2nd International Conference on Tropical Medicine and Infectious Disease (ICTROMI 2019), pages 247-252
ISBN: 978-989-758-469-5
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
247

asymptomatic bacteriuria became standard obstetric
care, and most antenatal guidelines include routine
screening for asymptomatic bacteriuria (Schaeffer et
al., 2016). USPTF, IDSA, ACOG, American
Academy of Pediatrics (AAP), and the American
Academy of Family Physicians (AAFP) recommend
screening pregnant women for asymptomatic
bacteriuria. IDSA, AAP, and ACOG recommend
screening with urine culture early in pregnancy,
whereas USPTF and AAFP recommend screening at
12-16 weeks gestation, or at first prenatal visit
(Turpin et al., 2007).
The prevalence of asymptomatic bacteriuria in
America ranges from 4% to 7%, but in certain
groups can range from about 2% to 11%. In Nigeria,
the prevalence of asymptomatic bacteriuria was as
high as 86.6%. Prevalence of asymptomatic
bacteriuria in pregnancy in Indonesia itself is 7.3%,
but research in Tambora Health Center, West
Jakarta, showed a higher prevalence at 35.3%
(Bukitwetan et al., 2004).
Based on this background, researchers wanted to
evaluate the proportion of asymptomatic UTI among
pregnant women in the Padang Bulan Clinic, Medan,
Indonesia.
2 MATERIALS AND METHODS
2.1 Study Area
This study is a descriptive study with a cross-
sectional approach, was carried out in the Padang
Bulan Primary health center, Medan.
2.2 Study Population
The population in this study were all pregnant
women, while the accessible population of this study
was pregnant women attending Padang Bulan
Primary Health Center, Medan from September to
November 2018. Samples who fulfilled the inclusion
criteria selected were asked to participate in the
study by signing the consent form. Demographic
data were obtained from the questionnaire (Laily,
2017). The sampling technique in this study was
non-probability sampling with purposive sampling.
Inclusion criteria included pregnant women
attending Pada Bulang Primary Health Centre
Medan, and those who agreed to participate.
Exclusion criteria included pregnant women with the
signs and symptoms of UTI or symptomatic
(dysuria, urgency, frequency, suprapubic discomfort,
fever, and low back pain), patients who had
difficulty in collecting the urine, and patients who
took antibiotics in the previous 2 weeks.
2.3 Specimen Collection and
Processing
The proportion of asymptomatic bacteriuria is
determined based on the freshly voided midstream
urine sample, Subjects were properly educated to
collect clean-catch midstream urine with sterile
technique into wide-mouthed, sterile capped
containers. After urine was collected, urine samples
were properly labeled and placed in a cold box. The
urine specimen was processed in the Microbiology
laboratory at Universitas Sumatera Utara within 2
hours of collection. Samples were cultured on Blood
agar and McConkey agar and were incubated at
37
o
C aerobically for 24 hours. Bacterial isolate
growth was monitored on the culture media and was
identified using colony characteristics, gram-
staining, and series of biochemical test.
Antimicrobial susceptibility testing was performed
using the disk diffusion method on Mueller-Hinton
agar.
The collected data were processed using the
computer program. The results of the examination
were recorded, compiled, and analyzed by the Chi-
Square test.
3 RESULTS
Fourteen of 50 pregnant women (28%) who were
analyzed with urine culture and had significant
colony counts (≥10
5
CFU/mL) had asymptomatic
bacteriuria (table 1). The most dominant bacteria
was Escherichia coli (28,6%), followed by
Staphylococcus coagulase negative (21,4%),
Klebsiella pneumonia (14,3%), Pseudomonas
aeruginosa (14,3%), Staphylococcus aureus (7,1%),
Klebsiella oxytoca (7,1%), and Staphylococcus
epidermidis (7,1%) (table 2).
ICTROMI 2019 - The 2nd International Conference on Tropical Medicine and Infectious Disease
248
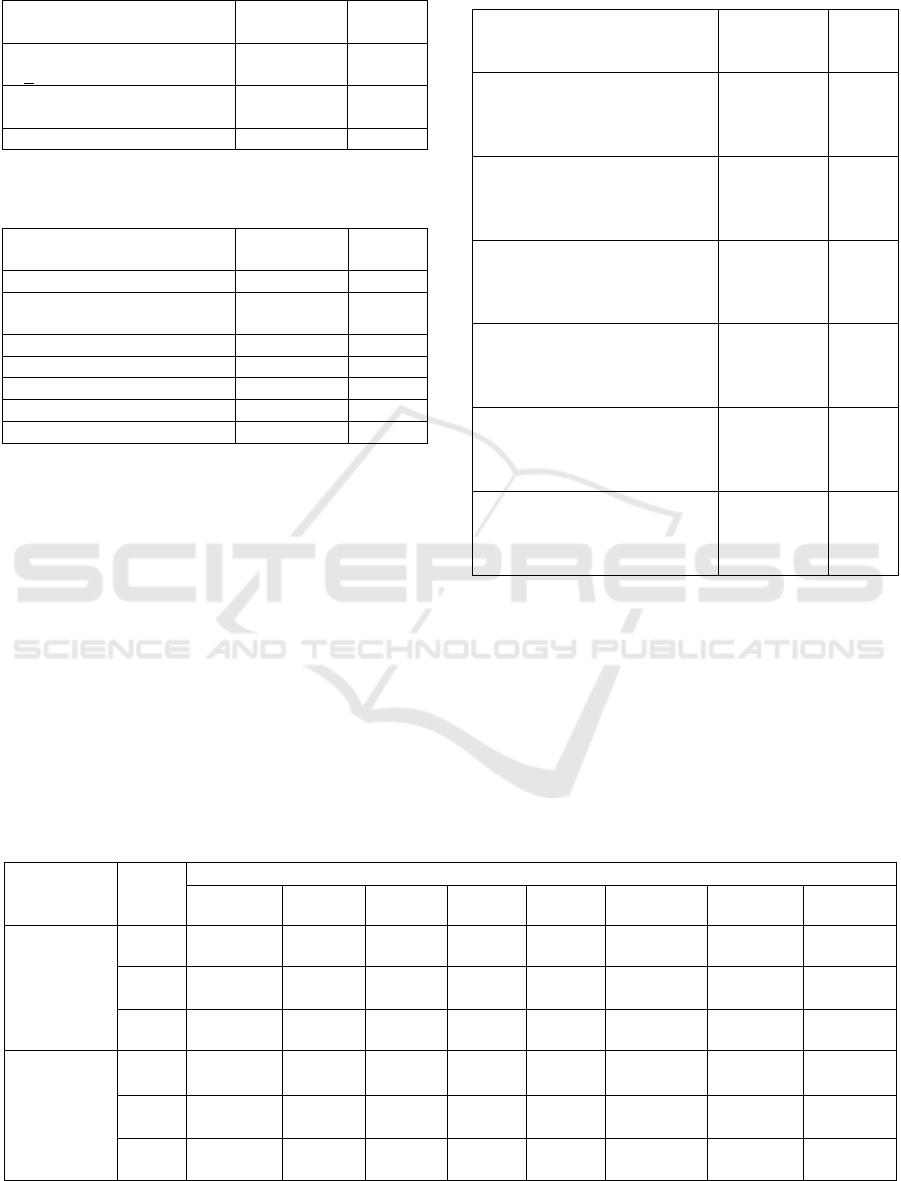
Table 1: Distribution of frequency of pregnant women
based on colony count.
Colony counts Frequency
(n=50)
%
Significant growth
(>100,000 CFU/ml)
14
28.0
No significant growth
(<100,000 CFU/ml)
17
34.0
No growth 19 28.0
Table 2: Bacterial isolates among pregnant women with
significant bacteriuria
Bacterial isolate Frequency
(n=14)
%
Escherichia coli 4 28.6
Staphylococcus coagulase
negative
3
21.4
Staphylococcus aureus 1 7.1
Staphylococcus epidermidis 1 7.1
Klebsiella pneumonia 2 14.3
Klebsiella oxtica 1 7.1
Pseudomonas aeruginosa 2 14.3
The collected data showed that pregnant
women with asymptomatic bacteriuria cases were
found mostly in pregnant women with age group 16-
25 years old (57,1%), were in high school (42,9%),
had monthly income <1.000.000 Rupiah (50,0%),
had sexual intercourse in the last 2 weeks (64,3%),
nullipara (71,4%), and were in second trimester
(50,0%).
Table 3: Distribution of frequency of pregnant women
with asymptomatic bacteriuria based on the characteristic.
Characteristics Total
number
(n=14)
%
Age group (years)
16-25
26-35
36-45
8
5
1
57.1
35.7
7.1
Educational status
Junior high school
High school
Higher education/university
3
6
5
21.4
42.9
35.7
Monthly income
<Rp.1.000.000
Rp.1.000.000-Rp.3.000.000
>Rp.3.000.000
7
4
3
50.0
28.6
21.4
Sexual intercourse in the last 2
weeks
Yes
No
9
5
64.3
35.7
Parity
Nullipara
Primipara
Multipara
10
2
2
71.4
14.3
14.3
Trimester
Trimester 1
Trimester 2
Trimester 3
2
7
5
14.3
40.0
35.7
Based on table 4, gram-negative isolates were found
sensitive to meropenem (100%), ceftazidime
(88,8%), piperacillin-tazobactam (77,7%),
ampicillin-sulbactam, cefotaxime, chloramphenicol,
nitrofurantoin (55,5%). And gentamycin (44,4%).
On the other hand, all gram-positive isolates were
found sensitive nitrofurantoin and meropenem
(100%), followed by gentamycin (40%) and
chloramphenicol (20%).
Table 4: Antimicrobial susceptibility pattern of bacterial isolates
Gram (-)
isolates
Profile Antimicrobial sensitivity, n (%)
SAM CTX CAZ C CN MEM F TZP
E. coli (4)
S 2 (50) 3 (75) 3 (75) 3 (75) 3 (75) 4 (100) 3 (75) 3 (75)
I 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
R 2 (50) 1 (25) 1 (25) 1 (25) 1 (25) 0 (0) 1 (25) 1 (25)
Klebsiella
pneumoniae
(2)
S 1 (50) 1 (50)
2
(100)
1 (50) 1 (50) 2 (100) 1 (50) 2 (100)
I 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
R 1 (50) 1 (50) 0 (0) 1 (50) 1 (50) 0 (0) 1 (50) 0 (0)
The Proportion of Asymptomatic Bacteriuria among Pregnant Women in a Primary Health Centre Medan, Indonesia
249
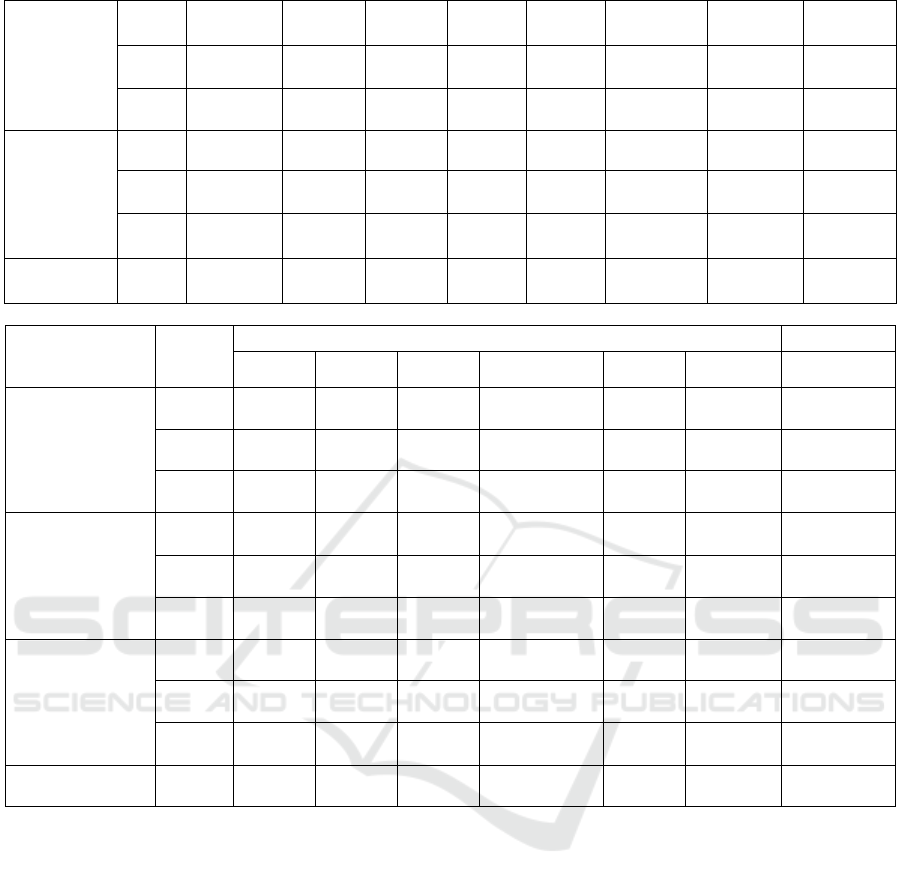
Pseudoman
as
aeruginosa
(2)
S
2
(100)
1 (50) 2 (100) 0 (0) 0 (0) 2 (100) 1 (50) 1 (50)
I 0 (0) 1 (50) 0 (0) 1 (50) 1 (50) 0 (0) 0 (0) 0 (0)
R 0 (0) 0 (0) 0 (0) 1 (50) 1 (50) 0 (0) 1 (50) 1 (50)
Klebsiella
oxytica (1)
S 0 (0) 0 (0) 1 (100) 1 (100) 0 (0) 1 (100) 0 (0) 1 (100)
I 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
R
1
(100)
1 (100) 0 (0) 0 (0) 1 (100) 0 (0) 1 (100) 0 (0)
Total
(9)
5 (55,5) 5 (55,5) 8 (88,8) 5 (55,5) 4 (44,4) 9 (100) 5 (55,5) 7 (77,7)
Gram (+)
isolates
Profile Antimicrobial sensitivity, n (%)
AK MEM F C E CN DA
Staphylococcus
coagulase (-) (3)
S 0 (0) 3 (100) 3 (100) 1 (33.3) 0 (0) 2 (66.6) 0 (0)
I 0 (0) 0 (0) 0 (0) 1 (33.3) 0 (0) 0 (0) 0 (0)
R 3 (100) 0 (0) 0 (0) 1 (33.3) 3 (100) 1 (33.3) 3 (100)
Staphylococcus
aureus (1)
S 0 (0) 1 (100) 1 (100) 0 (0) 0 (0) 0 (0) 0 (0)
I 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
R 1 (100) 0 (0) 0 (0) 1 (100) 1 (100) 1 (100) 1 (100)
Staphylococcus
epidermidis (1)
S 0 (0) 1 (100) 1 (100) 0 (0) 0 (0) 0 (0) 0 (0)
I 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
R 1 (100) 0 (0) 0 (0) 1 (100) 1 (100) 1 (100) 1 (100)
Total (5) 0 (0) 5 (100) 5 (100) 1 (20) 0 (0) 2 (40) 0 (0)
4 DISCUSSION
This study is a cross-sectional study to see the
proportion of asymptomatic bacteriuria among
pregnant women in Padang Bulan Primary Health
Center, Medan.
The result In this study found the proportion
was 28%. This proportion is higher than the study in
Sundari Hospital Medan with the proportion of
21.8% (Novita, 2016), but lower than the 30.2%
reported in Janti Primary Health Center, Malang
(Zahroh, 2014).
The most common bacterial isolated were E.
coli. This result is consistent with Tosin et al.
(2014), Enayat et al. (2008), and Tadesse et al
(2018)., that E. coli is the dominant organism
causing asymptomatic bacteriuria. Escherichia coli
is a normal flora in the vaginal and rectal area (Tosin
et al., 2014), and because the female urethra is
shorter compared to men therefore the chance of
bacteria ascends into the bladder is higher and may
cause an infection (Curtiss et al., 2017). This
bacteria also has a unique structure (pilus adhesions)
which help the bacteria for attachment to the
uroepithelium lining and prevent them from urinary
lavage, which allows them for multiplication and
tissue invasion resulting in invasive infections in
pregnancy (Tadesse et al., 2018).
In this study, according to age the highest
frequency of asymptomatic bacteriuria in pregnant
women was in the age group 16-25 years old. This
result is in accordance with the research of Tadesse
et al. (2018) with the most bacteriuria was in the age
ICTROMI 2019 - The 2nd International Conference on Tropical Medicine and Infectious Disease
250

group 18-25 years old. This might due to that early
and intensive sexual intercourse which may cause
minor urethral trauma and transfer bacteria from the
perineum into the bladder. In contrast to findings by
Tosin et al. (2014) with the highest prevalence of
asymptomatic bacteriuria in the age group 25-34
years old.
According to educational status, we found a
higher frequency of asymptomatic patients in the
high school group. A similar result was reported by
Laily in Kenangan Primary Health Center
Puskesmas Kenangan, Kabupaten Deli Serdang
(Laily, 2017). Most asymptomatic pregnant women
also had monthly income <1.000.000 rupiah, as
found by Tadesse et al. (2018). Reported pregnant
women with low family income were found 7 times
more likely to be positive for asymptomatic
bacteriuria (Tadesse et al., 2018). This could be due
to the relation of low socioeconomic status with
nutrition and immunity (Emiru et al., 2013).
In this study, we also found that asymptomatic
bacteriuria was more common in pregnant women
who had sexual intercourse in the last 2 weeks. A
similar finding was reported by Zahroh et al where
61.5% of pregnant women with high sexual activity
had bacteriuria. Pregnant women who had sexual
intercourse >3 per week were more likely have UTI
than women who had sexual intercourse <3 per
week, with the theory that sexual intercourse can
potentially cause skin irritation which increases the
occurrence of urethra infection (Zahroh et al., 2014).
Another theory that is sexual intercourse can
encourage bacterial ascending (Curtiss et al., 2017).
According to parity, the highest frequency of
asymptomatic bacteriuria was in pregnant women
with nullipara, this finding is in line with studies by
Zahroh et al. (76,9%) (Zahroh et al., 2014).
Different finding reported by Turpin et al. with
multiparity had the highest percentage of
asymptomatic bacteriuria (Turpin et al., 2007).
In this study, pregnant women in the second
trimester of pregnancy had the highest percentage of
asymptomatic bacteriuria followed by pregnant
women in the third trimester of pregnancy, similar
finding by Tosin et al. was also reported in Lagos,
Nigeria (45,3%) (Tosin et al., 2014). Different
findings reported by Turpin et al. with most of the
infected subjects were in their first and early second
trimesters. This could be because most pregnant
women report at the antenatal clinic for booking
during these periods (Turpin et al., 2007) it also
indicated that the gold standard for screening
asymptomatic bacteriuria is in early pregnancy of
12-16 weeks (Tadesse et al., 2018).
The dominant organism in this study was E.
coli which was sensitive to meropenem (100%),
nitrofurantoin, piperacillin-tazobactam, gentamycin,
chloramphenicol, ceftazidime, and cefotaxime
(75%). A similar finding was reported by Tosin et
al. where E. coli was observed to be sensitive to
nitrofurantoin and gentamycin (Tosin et al., 2014).
5 CONCLUSIONS
The proportion of asymptomatic bacteriuria in
pregnant women in Padang Bulan Primary Health
Center was 28.0%, and the most frequent isolates
were Escherichia coli followed by Staphylococcus
coagulase negative. Most pregnant women with
asymptomatic bacteriuria were in the age group of
16-25 years, with educational status in high school,
low socioeconomic status, had sexual intercourse in
the last 2 weeks, at trimester II, and a nullipara.
The antibiotic sensitivity from this study
showed all gram-negative and gram-positive were
sensitive to meropenem (100%), and nitrofurantoin
was sensitive to gram-negative (100%).
ACKNOWLEDGMENTS
We thank the staff of Padang Bulan Primary Health
center for their assistance and the staff of USU
Microbiology Laboratory for their help in the
specimen processing.
REFERENCES
Azkia, H.P. & Berawi, K. 2015, ,,Bakteriuria
Asimptomatik pada Kehamilan’’, J Agromed Unila,
vol. 2, no. 4, pp. 434-439.
Bukitwetan, P., Salim, O, Ch., Surjawidjaja, J, E., Aidilfit,
M., & Lesmana, M. 2004, ,,Prevalensi bakteriuria
asimtomatik pada ibu hamil”. Bakteriuria pada
kehamilan, vol. 23, no. 4, pp. 127-133.
Curtiss, N., Meththananda, I., Duckett, J. 2017,,,Urinary
tract infection in obstetrics and gynaecology‟,
Obstetrics, gynaecology and Reproductive Medicine,
vol. 27, no. 9, pp. 261-265.
Emiru, T., Beyene, G., Tsegaye, W., & Melaku, S. 2013,
,,Associated risk factors of urinary tract infection
among pregnant women at Felage Hiwot Referral
Hospital, Bahir Dar, North West Ethiopia”, BioMed
Central Research Notes, [Online], accessed 25
December 2018, Available at:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3750516/
The Proportion of Asymptomatic Bacteriuria among Pregnant Women in a Primary Health Centre Medan, Indonesia
251

Enayat, K., Fariba, F., & Bahram, N.
2008,,,Asymptomatic Bacteriuria among Pregnant
Women Reffered to Outpatien Clinics in Sanandaj,
Iran”, International Braz J Urol, vol. 34, no. 6, pp.
699-704.
Glaser, A, P., & Schaeffer, A, J. 2015, Urinary tract
infection and bacteriuria in pregnancy‟, Urologics
Clinics of North America, vol. 42, no. 4, pp. 547-560.
Laily, F. 2017, Hubungan Faktor Resiko pada Wanita
Hamil dengan Kejadian Infeksi Saluran Kemih pada
Masa Kehamilan di Wilayah Kerja Puskesmas
Kenangan, Kecamatan Percut Sei Tuan, Kabupaten
Deli Serdang”, USU Institutional Repository, [Online],
accessed 22 January 2019, Available at:
http://repository.usu.ac.id/handle/123456789/67213
Macejko, A, M., Schaeffer A, J. 2006, Asymptomatic
bacteriuria and symptomatic urinary tract infection
during pregnancy‟, Urologic Clinics of North
America, vol. 34, no. 1, pp. 35-42.
Novita, S, H. 2016, ,, Insiden Infeksi Saluran Kemih
berdasarkanhitungan leukosit pada wanita hamil di
trimester III Periode September-Oktober 2015 di
Rumah Sakit Sundari Medan”, USU Institutional
Repository, [Online], accessed 18 January 2019,
available at:
http://repository.usu.ac.id/handle/123456789/56345
Pais, Jr., V.M & Reinstatler, L. 2018, Urologic Surgery in
the Pregnant Patient, Elsevier, Edinburgh.
Schaeffer, A, J., Matulewicz., R, S., & Klump, D, J. 2016,
Infections of the Urinary tract," in Campbell-Walsh
UROLOGY, ed. Elsevier.
Smaill, F. 2007, Asymptomatic bacteriuria in pregnancy‟,
Best Practice and Research: Clinical Obstetric and
Gynaecology, vol. 21, no. 3, pp. 439-450.
Tadesse, S., Kahsey, T., Adhanom, G., Kahsu, G., Legese,
H., G/wahid, A., & Derbie, A. 2018, ,,Prevelence,
antimicrobial susceptibility profile and predictors of
asymptomatic bacteriuria among pregnant women in
Adigrat General Hospital”, BioMed Central Research
Notes, [Online], accessed 12 October 2018, Available
at: https://www.ncbi.nlm.nih.gov/pmc/articles/
PMC6194591/
Tosin, O, J.A., Mathew, A, O., Bello, F, J., Oludare, I, T.,
Dolapo., A, L., Abosede, A, F. 2014, ,,Asymptomatic
Bacteriuria among antenatal Woman Attending private
Hospital in Lagos, Nigeria”, Scholars Journal of
Applied Medical Sciences, vol. 2, no. 6D, pp. 3076-
3080.
Turpin, CA., Minkah, B., Danso, KA., & Frimpong, EH.
2007, Asymptomatic Bacteriuria in Pregnant Women
Attending Antenatal Clinic at Komfo Anokye
Teaching hospital, Kumasi, Ghana” Ghana Medical
Journal, vol. 41, no.1, pp. 26-29.
Zahroh, F., Roebijoso, J., samsu., N. 2014, ,,Profil
Kejadian Bakteriuria Asimtomatik serta Faktor-Faktor
yang Terkait dengan Kejadian Bakteriuria
Asimtomatik pada Ibu Hamil di Puskesmas Janti Kota
Malang”, Majalah kesehatan FKUB, vol. 1, no. 4, pp.
228-234.
ICTROMI 2019 - The 2nd International Conference on Tropical Medicine and Infectious Disease
252
