
Comparison of C-Reactive Protein Levels and Erythrocyte
Sedimentation Rates to Osteoarthritis Patients with Sidaguri Extract
Treatment within 1 Month and 2 Month
Blondina Marpaung
1*
, J. Siregar
2
1
Division of Rheumatology, Department of Internal Medicine, Universitas Sumatera Utara/ Adam Malik Hospital, Jl.Bunga
Lau, Medan, Indonesia
2
Clinical Pathology Department, Universitas Sumatera Utara/ Adam Malik Hospital, Jl.Bunga Lau Medan Indonesia
Keywords: Sidaguri, CRP, ESR
Abstract: Osteoarthritis (OA) is defined as a heterogeneous condition that leads to joint sign and symptoms caused by
defective integrity of articular cartilage and inflammation. CRP is a sensitive acute phase reactant with
levels rapidly rising in many inflammation conditions. ESR is an indirect measure of the level of
inflammation in the body. The management of OA limited in the pain and inflammation control with any
NSAID. Meloxicam is one of NSAID that inhibits the synthesis of prostaglandins by inhibiting at least 2
cyclo-oxygenases (COX) isoenzymes. Sidaguri plant (Sida rhombifolia L.) is one of the most important
species of the medicinal part in Indonesia as anti-inflammation, by inhibition of nitric oxide and protein
denaturation inhibitions. Our study recruited 50 patients with OA divided into two groups, patients who get
Meloxicam and Sidaguri (n = 25) and patients with Meloxicam and placebo (n = 25). There were significant
differences before, one month, and two months after therapy with p-value <0.001, and the Sidaguri
combination with meloxicam is better in reducing CRP and ESR levels.
1 INTRODUCTION
According to the American College of
Rheumatology (ACR), osteoarthritis (OA) is defined
as a heterogeneous condition that leads to joint sign
and symptoms which are caused by defective
integrity of articular cartilage. (Sarzi-Puttini et al.,
2005)
OA is one of the most common chronic disorder
among the elderly. WHO Scientific Group on
Rheumatic Diseases data found that approximately
40% of people over the age of 70 years developed
this disease. More than 65 years of age are at risk of
having OA. The prevalence of OA was 80% and
have some degree of limitation of movement.
(Organization, 2003) The disease is characterized by
degenerative process and mechanical disturbance
with the gradual erosion of joint cartilage.
Prevalence of OA was found to increase with age
and enzymatic sequence that triggers a response
which ended in the destruction of joints.
(Dahaghin
et al., 2005)
Assessment of pain usually used in OA is the
visual analog scale (VAS). The pain VAS is self-
completed by the respondent. The score is classified
as 1 to 4 (on a 0-10 scale). The mild pain is treated
with non-opioid analgesics with or without adjuvant
therapy, 5 to 6 scale as moderate pain treated with
non-opioid analgesics, weak opioid analgesics with
or without adjuvant therapy, and 7 to 10 as severe
pain treated with strong opioids analgesics with or
without adjuvant therapy. (Jensen et al., 2003)
The ACR use non-steroidal anti inflammatory
drugs (NSAIDs) as the main drug of OA. The
Agency for Healthcare Research and Quality
(AHRQ) reported the use of non-opioid analgesics
for OA as primary and secondary treatment. The
European League Against Rheumatism (EULAR)
recommendations for the management of OA
recommend paracetamol as the first line treatment,
with topical agents such as topical NSAID and
capsaicin. The American Heart Association
Scientific Statement on the use of NSAIDs and the
American College of Cardiology Foundation
consensus recommend reducing the risk of
gastrointestinal (GI) adverse events in patients using
antiplatelet and NSAID therapy. (Hochberg et al.,
2012)
Marpaung, B. and Siregar, J.
Comparison of C-Reactive Protein Levels and Erythrocyte Sedimentation Rates to Osteoarthritis Patients with Sidaguri Extract Treatment within 1 Month and 2 Month.
DOI: 10.5220/0009855600330037
In Proceedings of the 2nd International Conference on Tropical Medicine and Infectious Disease (ICTROMI 2019), pages 33-37
ISBN: 978-989-758-469-5
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
33

Meloxicam is one of NSAID member of oxicam
class that inhibits the synthesis of prostaglandins in
cells settle in a specially designated tube of
anticoagulated blood, an effect that is altered by
proteins associated with an inflammatory response
(Assasi et al., 2015)
CRP is merely an indicator or biomarker of a
disease process that is caused by cell death due to
inflammation. C-reactive protein (CRP) is a protein
produced by the liver as a response of inflammation
and infection. It is an extremely sensitive acute
phase reactant with levels rapidly rising 1000 times
or more in many disease condition. ESR is an
indirect measure of the level of inflammation in the
body. ESR measures the rate at which red blood
body tissue by inhibiting at least 2 cyclo-oxygenases
(COX) isoenzymes. (Davies and Skjodt, 1999) From
an international perspective, WHO has agreed to
promote the use of traditional medicine,
complementary medicine for health that focuses on
people centered on health services and encourages
the use of security and the efficacy of the traditional
medicines related to licensing and products, training
and practitioners. (Aditama, 2014)
Sidaguri plant (Sida rhombifolia L.) is one of the
most important species of the medicinal part in
Indonesia as anti-inflammation. The anti-
inflammatory activity effects by inhibition of nitric
oxide and protein denaturation inhibitions. Potent
anti-inflammatory effect of root of Sidaguri on rat
periapical lesion model caused by β-sitosterol, a
sterol isolated of different species of Sidaguri, which
is reported to have anti-inflammatory properties,
similar to hydrocortisone and oxyphenbutazone.
(Khalil et al., 2006)
2 METHODS
2.1 Patient Selection
This randomized, independently and a double-blind
controlled clinical trial was performed from April
2017 until November 2017 in Haji Adam Malik
Hospital and Prof. Dr. Boloni Hospital in Medan.
This Study enrolled patients diagnosed with
osteoarthritis. CRP, ESR, RFT, LFT levels were
measured from blood samples collected from the
cubital fossa area at one day before treatment, 30
days and 60 days later. The patients were randomly
divided into two groups: one group with sidaguri
extract and meloxicam and the other group with
meloxicam and placebo, in simple random sampling
with some sealed envelope that was not transparent
and given odd and even numbers on the rolled of
paper in it.
2.2 Inclusion and Exclusion Criteria
In inclusion criteria, all the subjects aged over 40
years of both men and women with OA, with VAS ≥
4, no impaired liver and kidney function and other
causes of inflammatory reaction.
2.3 Statistical Methods
To display epidemiological data of the subject of the
research, we used tabulation to show the descriptive
picture. Data were processed and analyzed using
SPSS Version-24 program with p <0.05
significance.
3 RESULT
This study involved 50 patients who fulfilled the
inclusion criteria, the patients were equally divided
into two groups: patients who received Meloxicam
with Sidaguri ( n=25) and the other group who
received Meloxicam with placebo (n=25). The
patients were monitored before treatment, one month
and two months after treatment. Nine patients
(69,2%) who received Meloxicam therapy and
placebo were male. Meanwhile, 21 patients (56,8%)
who received meloxicam and sidaguri were female.
The baseline characteristics showed no significant
differences between the two groups (p-value =0,017)
Table 1. Basic characteristics
Characteristics
Therapy
P-Value
Meloxicam&
Placebo (MP)
Meloxicam&Sidaguri (MS)
Gender Male 9 (69.2%) 4 (30.8%) 0.107
Female 16 (43.2%) 21 (56.8%)
Age
58.92 േ10.43 59.64 േ 11.39
0.817
ICTROMI 2019 - The 2nd International Conference on Tropical Medicine and Infectious Disease
34
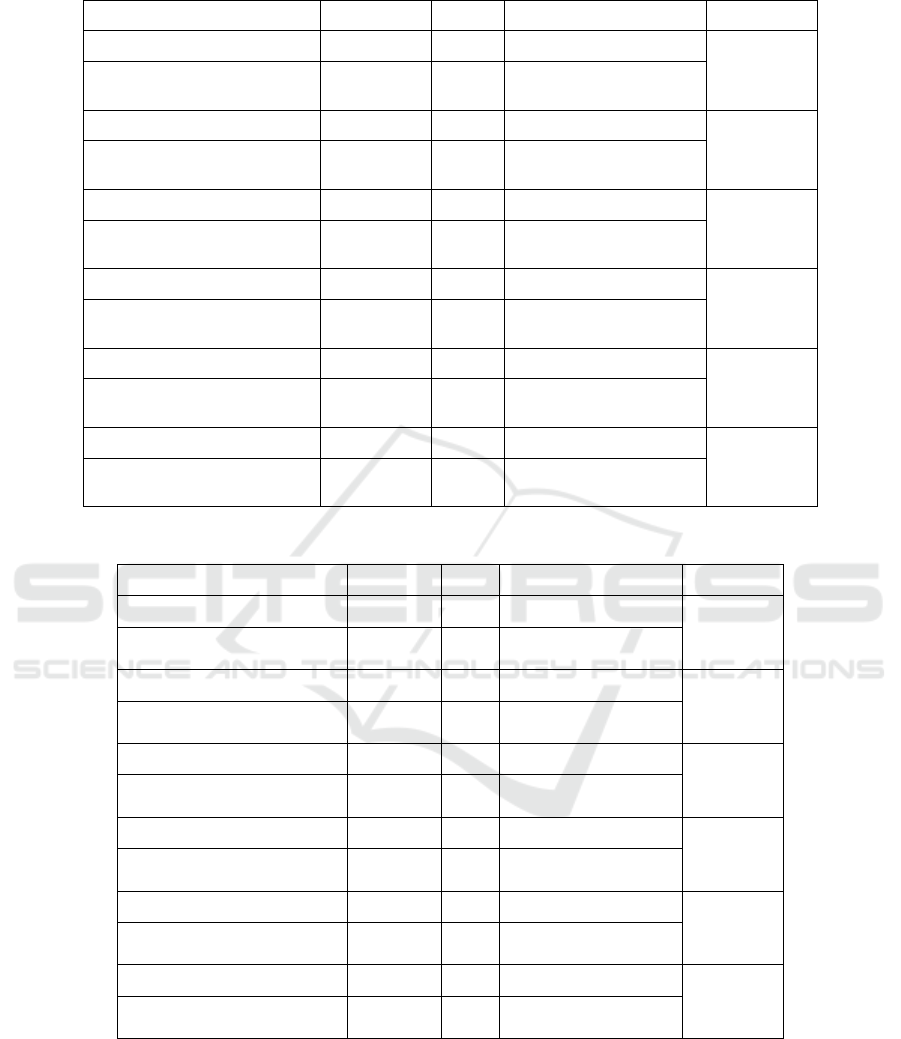
Table 2: Significance Test Differences in laboratory results based on Meloxicam and Placebo Therapy
Variable Mean n Standard Deviation P-Value
ESR-PRE 22.88 25 2.205
<0.001
ESR-1 month
ESR- 2 months
22.40
21.44
25
25
2.217
1.873
CRP-PRE 0.876 25 0.2437
<0.001
CRP-1 month
CRP- 2 months
0.836
0.764
25
25
0.2515
0.2079
SGOT-PRE 19.45 25 4.342
<0.001
SGOT-1 month
SGOT-2 months
22.76
23.67
25
25
4.560
4.628
SGPT-PRE 21.05 25 7.239
<0.001
SGPT-1 month
SGPT- 2 months
23.87
22.96
25
25
7.538
7.760
UREUM-PRE 30.786 25 17.875
<0.001
UREUM-1 month
UREUM-2 months
36.709
38.912
25
25
18.786
19.074
CREATININ-PRE 0.876 25 0.265
<0.001
CREATININ-1 month
CREATININ-2 months
1.120
1.368
25
25
0.298
0.321
Table 3: Significance Test Differences in laboratory results based on Meloxicam and Sidaguri Therapy
Variable Mean n Standard Deviation P-Value
ESR-PRE 23.89 25 1.689
<0.001
ESR-1 month
ESR- 2 months
12.98
11.32
25
25
3.309
3.867
CRP-PRE 1.309 25 0.245
<0.001
CRP-1 month
CRP- 2 months
0.762
0.639
25
25
0.158
0.142
SGOT-PRE 19.59 25 7.987
<0.001
SGOT-1 month
SGOT-2 months
25.68
27.52
25
25
8.142
9.043
SGPT-PRE 22.81 25 14.986
<0.001
SGPT-1 month
SGPT- 2 months
27.47
29.56
25
25
13.782
12.908
UREUM-PRE 23.90 25 11.703
<0.001
UREUM-1 month
UREUM-2 months
27.51
30.91
25
25
10.678
10.002
CREATININ-PRE 0.79 25 0.156
<0.001
CREATININ-1 month
CREATININ-2 months
0.83
0.98
25
25
0.179
0.190
Our study revealed a statistically significant
improvement based on laboratory results include
CRP, liver function, renal function, and ESR
before, after 1 month and 2-month Meloxicam and
placebo treatment with p-value <0.001. (Table 2 )
A statistically significant improvement
laboratory results include CRP, liver function,
renal function, and ESR before, after 1 month and
2 months after Meloxicam and Sidaguri treatment
also revealed p-value < 0.001. (Table 3)
The mean ESR after 2 months Meloxicam and
Placebo therapy was 66.72, while the mean ESR
after 2 months Meloxicam and Sidaguri therapy
were 16.06. There is a statistically significant
Comparison of C-Reactive Protein Levels and Erythrocyte Sedimentation Rates to Osteoarthritis Patients with Sidaguri Extract Treatment
within 1 Month and 2 Month
35
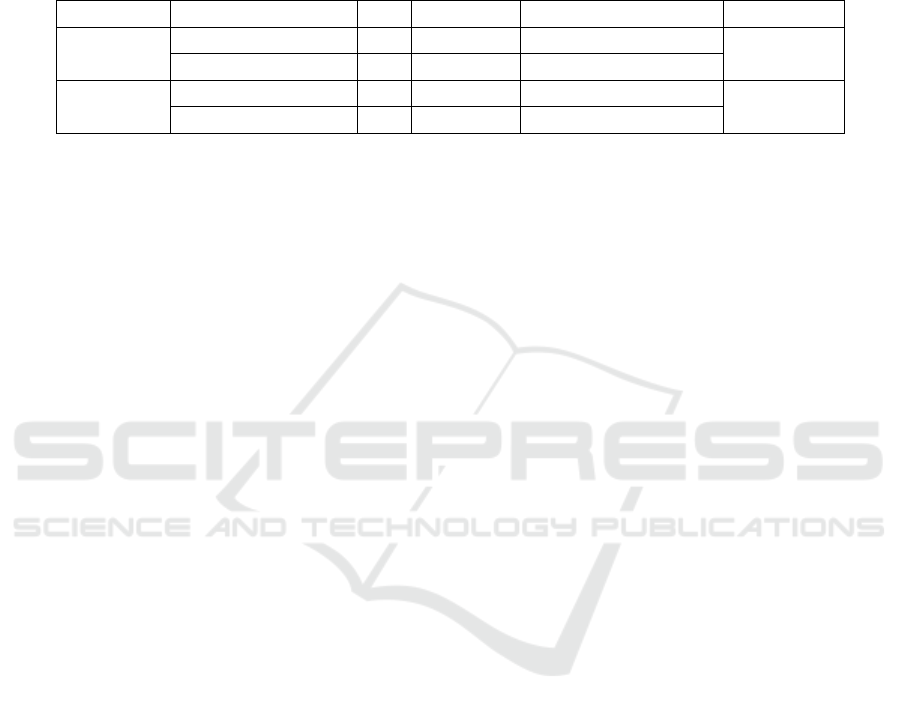
difference between ESR-2 months treatment with
MP and ESR-2 months treatment with MS with p-
value <0.001.
The mean CRP after 2 months with MP
therapy was 0.825, while the mean CRP after 2
months with MS therapy was 0.903. There is a
statistically significant difference between CRP-2
months treatment with MP and CRP-2 months
treatment with MS with p-value 0.003.
Table 4: Significance Test of difference between post-therapy ESR and post-therapy CRP in both groups and VAS score
Variable Therapy N Mean Standard Deviation P-Value
ESR
Meloxicam& Placebo 25 66.72 2.098
˂0.0001
Meloxicam&Sidaguri 25 16.06 2.855
CRP
Meloxicam& Placebo 25 0.825 0.234
0.003
Meloxicam&Sidaguri 25 0.903 0.182
4 DISCUSSION
This study included 50 samples, divided into two
groups. It was found that OA was predominantly in
women (43.2% and 56.8%). Subject’s age in both
groups were not significantly different (58.92 ±
10.43 and 59.64 ± 11.39) with p-value 0.817. The
prevalence of OA is rising along with the age due to
its irreversibility. Therefore, age has a major role as
an important risk factor in osteoarthritis and it is
much more common in women than men. (Glyn-
Jones et al., 2015)
Increased level of CRP and ESR was found in
both groups before therapy with either meloxicam
and Sidaguri or meloxicam with placebo. On the
other hand, CRP and ESR levels after 30 days and
60 days are lower, and statistically significant with
p-value <.0.001. According to Mishra et al. there is a
significantly increased CRP level in patients with
OA (Mishra et al., 2012).
A significant improvement was found in the
meloxicam group compared to placebo while
comparing meloxicam with placebo and meloxicam
with Sidaguri resulted in a statistically different
outcome in CRP and ESR. Systemic inflammation is
reflected by CRP, even it is not specific for OA. Its
level can reach up to 100 times of normal range.
CRP levels will diminish rapidly when tissue
damage and inflammation recede and return to
baseline in 24-48 hours. CRP levels are steady in
plasma and are not influenced by diurnal variation.
(Kandy, 2016)
Meanwhile, ESR could rise in the following
condition: acute inflammatory processes, acute and
chronic infections, tissue damage (necrosis),
rheumatoid, collagen disease, malignancy and
physiological stress conditions (e.g. pregnancy), thus
it is not a specific indicator. ( Kee, 2008)
From the study results, it can be concluded that
mean ESR in patients receiving meloxicam and
placebo treatment group was 66,72 while in
meloxicam and sidaguri-treated patient, the mean
ESR was 16.06 with p-value ˂0.0001. This implied
that meloxicam and sidaguri treatment was
preferable in decreasing ESR over meloxicam and
placebo treatment. Moreover, mean CRP levels
found in meloxicam and placebo group was 0.825
while in meloxicam and the sidaguri group was
0.903 with p-value 0.003, succeeded by clinical
improvement observed from decreasing VAS (p
=0,003).
Several studies found the anti-inflammatory
effect in Sidaguri. It contains an alkaloid,
ecdysteroid, flavonoids, and saponins, which is
believed can inhibit the production of prostaglandin
(as cyclooxygenase blockers). Moreover, it is also
found that β-sitosterol in the Sidaguri also has anti-
inflammatory properties. (Mah et al., 2017)
The author acknowledges the limitation of this
study. The study had a smaller sample size. We
recommend further study with larger samples to
confirm this finding.
5 CONCLUSIONS
There were significant differences before, one
month, and two months after therapy with p-value
<0.001 in both group and the Sidaguri combination
with meloxicam is better in reducing CRP and ESR
levels.
ICTROMI 2019 - The 2nd International Conference on Tropical Medicine and Infectious Disease
36

REFERENCES
Aditama, T. Y. 2014. Jamu dan kesehatan. Badan
Penelitian dan Pengembangan Kesehatan.
Assasi, N., Blackhouse, G., Campbell, K., Hopkins, R. B.,
Levine, M., Richter, T. & Budden, A. 2015.
Comparative Value of Erythrocyte Sedimentation Rate
(ESR) and C-Reactive Protein (CRP) Testing in
Combination Versus Individually for the Diagnosis of
Undifferentiated Patients With Suspected
Inflammatory Disease or Serious Infection: A
Systematic Review and Economic Analysis. Ottawa
(ON).
DAHAGHIN, S., BIERMA-ZEINSTRA, S., REIJMAN,
M., POLS, H., HAZES, J. & KOES, B. J. A. O. T. R.
D. 2005. Prevalence and determinants of one-month
hand pain and hand related disability in the elderly
(Rotterdam study). 64, 99-104.
DAVIES, N. M. & SKJODT, N. M. J. C. P. 1999. Clinical
pharmacokinetics of meloxicam. 36, 115-126.
GLYN-JONES, S., PALMER, A., AGRICOLA, R.,
PRICE, A., VINCENT, T., WEINANS, H. & CARR,
A. J. T. L. 2015. Osteoarthritis. 386, 376-387.
HOCHBERG, M. C., ALTMAN, R. D., APRIL, K. T.,
BENKHALTI, M., GUYATT, G., MCGOWAN, J.,
TOWHEED, T., WELCH, V., WELLS, G.,
TUGWELL, P. J. A. C. & RESEARCH 2012.
American College of Rheumatology 2012
recommendations for the use of nonpharmacologic and
pharmacologic therapies in osteoarthritis of the hand,
hip, and knee. 64, 465-474.
JENSEN, M. P., CHEN, C. & BRUGGER, A. M. 2003.
Interpretation of visual analog scale ratings and
change scores: a reanalysis of two clinical trials of
postoperative pain. J Pain, 4, 407-14.
KANDY, A. P. 2016. Uji Aktivitas antiinflamasi
kombinasi ekstrak etanol jahe merah (Zingiber
officinale var. rubrum) dan daun sidaguri (Sida
rhombifolia L.) terhadap jumlah neutrofil tikus yang
diinduksi karagenin.
KHALIL, N. M., SPEROTTO, J. S. & MANFRON, M. P.
J. A. F. B. 2006. Anti-inflammatory activity of the
hydroalcoholic extract of leaves of Sida rhombifolia
L.(Malvaceae). 25, 260.
MAH, S. H., TEH, S. S. & EE, G. C. L. J. P. B. 2017.
Anti-inflammatory, anticholinergic and cytotoxic
effects of Sida rhombifolia. 55, 920-928.
MISHRA, R., SINGH, A., CHANDRA, V., NEGI, M. P.,
TRIPATHY, B. C., PRAKASH, J. & GUPTA, V. J. R.
I. 2012. A comparative analysis of serological
parameters and oxidative stress in osteoarthritis and
rheumatoid arthritis. 32, 2377-2382.
ORGANIZATION, W. H. 2003. The burden of
musculoskeletal conditions at the start of the new
millennium. 919, i.
SARZI-PUTTINI, P., CIMMINO, M. A., SCARPA, R.,
CAPORALI, R., PARAZZINI, F., ZANINELLI, A.,
ATZENI, F. & CANESI, B. 2005. Osteoarthritis: an
overview of the disease and its treatment strategies.
Semin Arthritis Rheum, 35, 1-10.
Comparison of C-Reactive Protein Levels and Erythrocyte Sedimentation Rates to Osteoarthritis Patients with Sidaguri Extract Treatment
within 1 Month and 2 Month
37
